



Books and Documents > The Army Medical Department 1818-1865
CHAPTER 12
The End
From January to early April 1865, the Civil War continued in full fury, but on 9 April, after pushing his men close to the limits of their endurance, Grant forced the surrender of Lee`s Army of Northern Virginia at Appomattox. Further south, Union armies took Mobile and swept through Alabama and southwestern Georgia. Sherman led his army north from Savannah through the Carolinas, forcing Confederate General Joseph Johnston to abandon the struggle a few days after Lincoln`s assassination on 14 April. Weeks before the last Confederate army formally surrendered on 26 May, the bloodiest conflict the nation had ever known had essentially come to an end.
The Union`s sick and wounded from recent campaigns had never been the only patients for whom the Medical Department was responsible. Thousands of Confederate soldiers in Northern prisons as well as a trickle of sick and wounded Union soldiers released from captivity in the South during the course of the war looked to Union medical officers for help. The campaigns of 1865 began to release Union prisoners of war in the thousands, and the health of many was shattered. Thus, even as it prepared to cut back its operations to a peacetime level, the Medical Department was taking on increased wartime obligations.
Administration
Other than the collection of routine reports and the coordination of the work of the various branches of the Medical Department, much of the administrative work of the Surgeon General`s Office in the first half of 1865 continued to involve the reduction of the department`s size and expenses to a peacetime level. In January 1865 the number of general hospitals still operating was already three less than the 204 that marked its peak. These installations had treated more than a million white troops during the conflict, but by the end of June, after the Army began mustering patients out directly from hospitals, 170 were closed. The War Department`s order of 28 April to cut back on expenses was followed by the reduction of the department`s small fleet of ocean-going hospital transports from four to one, the return of all its river transports to the Quartermaster`s Department, the elimination of all hospital trains but one in the West, and the collection of excess medicines and hospital supplies for sale at public auction. Barnes dismissed the medical boards that had been examining surgeons for the wartime Army and ordered his purveyors to stop buying until all surpluses had been consumed. He began closing purveying depots, keeping open only seven distributing sites
252
and the main depots at New York, Philadelphia, and Louisville. He started reducing the size of the department`s laboratories. His medical directors intensified the process of consolidating patients, both Union soldiers and Confederate prisoners of war, and of converting large hospitals to post facilities, while Barnes began discharging contract doctors and hospital attendants. The surgeon general also decided that the department could loan its excess bedsteads, bedding, and blankets to soldiers` homes. All the while, the Department was processing requests for confirmation of death from the Pension Bureau, averaging 5,500 a month in May.1
Among the expenses the Medical Department could not reduce in the spring of 1865 were those involving sick and injured freedmen and refugees, for although Congress voted aid to these men in March, the law was apparently not quickly implemented. Thus for several more months in 1865, much of the cost of the care of such patients, including that incurred in hiring contract surgeons and nurses, continued to be borne by the Medical Department, with the understanding that it would be reimbursed, and the War Department continued to detail medical officers to assist in the care of the unfortunate new citizens.2
Even with the end of the war in sight and much to occupy his mind, Barnes continued the department`s efforts to improve the status of its most burdened medical officers. Less than two months before Lee`s surrender, the War Department finally ordered the pay of medical directors increased. Medical directors of armies in the field composed of two or more corps and medical directors of military departments whose general hospitals housed 4,000 or more patients were given the rank and pay of colonels, and those with lesser responsibilities were given the rank and pay of lieutenant colonels. These increases, however, were to be effective only while these officers bore exceptional responsibilities, and at least two-thirds of these positions were reserved for surgeons and assistant surgeons of the volunteers. Thus, with the end of the war, very few regular officers in the Medical Department would be entitled to retain ranks above major.3
Although the surgeon general`s support and influence in Washington was invaluable, by 1865 medical directors were experienced enough to need little guidance from Barnes. While the surgeon general coordinated the efforts of his various subordinates, prepared the Department for a return to peacetime duties, and supervised the collection of records and specimens that would be used for the Medical Department`s history and museum, his subordinates followed familiar routines, caring for their patients on the battlefield and in the various hospitals that sheltered the sick and wounded.
1War Department, SGO, Annual Report, 1865, pp. 2-5; MSH 1, app.:205; Brown, Medical Department pp. 244-45; Ltrs, William J. Sloan to SG (28 and 31 Mar and 8 Apr 1865),A. K. Smith to McDougall (2 May 1865), R. Crowell to SG (17 May 1865), Magruder to SG and Clymer to SG (both 25 May 1865), A. J. Phelps to Wood, Sloan to SG, and Sloan to Alfred Henry Thurston (all 31 May 1865), Abadie to SG (15 Jun 1865), and C. W. Ballard to SG (27 Jun 1865), all in RG 112, entry 12; Ltr, Alexander N. Dougherty to Lincoln R. Stone (4 May 1865)and Circ Ltrs (2 and 5 May 1865), U.S. Army, General Hospital, Gallipolis, Ohio- Correspondence, orders, internal regulation, all in Ms C24, NLM.
2GO, AG (no. 1, 1 Jan 1865); filed with Ltr, Hennell Stevens to SG (10 Jan 1865), and Ltrs, McCord to Lee (10 Jan 1865), Stevens to SG (10Jan 1865), and Cooper to SG (27 Feb 1865), all in RG 112, entry 12;WOR, ser. 1, 47, pt. 1:492, 704 and pt. 2:80, 477; Commission of the Bureau of Refugees, Freedmen, and Abandoned Lands, Circulars, etc.,. . . With Copies of Acts and Joint Resolutions of Congress, and Proclamations by the President ... (Washington, 1867), pp. 1-3, in Freedmen`s Bureau Papers, RG 105.
3Grace, Manual, p. 105.
253
Grant`s Campaign in Northern Virginia
In January 1865 the battlefield for the Army of the Potomac lay around Lee`s besieged force at Petersburg. More than 500 medical officers and40 hospital stewards served 4 army corps, a cavalry division, and several independent commands, including artillery and Signal Corps units. More than 1,900 men and 43 officers formed the ambulance corps, although the former figure dropped to 1,600 as the campaign continued. Field hospitals housed 2,500 patients, another 2,900 occupied the City Point depot hospital, and almost 8,000 had been sent to general hospitals in the North. Slightly more than 22 percent of the soldiers of this army were sick in January, many of them with bowel ailments or fevers, usually typhoid or malaria. Respiratory problems and rheumatism were not uncommon. Scurvy was specifically diagnosed in only 52 patients in January, but at least 1 medical inspector blamed the severity of the diarrhea that prevailed on a lack of fresh vegetables caused by a shortage of transportation. It is highly likely that many men were suffering from a subclinical form of scurvy.4
In addition to the diseases that almost invariably afflicted armies in the Civil War, surgeons in the field with Union troops around Petersburg contended with diseases associated with poorly located camps and inadequate shelter or contracted by men on furlough. Around Petersburg the campsite that military requirements dictated might be poorly drained, and shallow wells were easily contaminated by surface water. The health of two V Corps divisions camped in a particularly marshy area did not improve until these units moved elsewhere. Circumstances also forced the men of one division to live several days without adequate shelter or blankets, and their health suffered accordingly. In mid-January men returning from leave added to these difficulties when they brought smallpox back with them. The mass vaccination program ordered as a result was not completed until mid-February, but surgeons established a smallpox hospital where they could isolate victims of that highly contagious disease.
Most of the 3,000 wounded and 6,400 who fell ill while in camp or field in January and February 1865 were initially sheltered in division hospitals. Surgeons sent those whose recovery was not likely, as well as all those sick when the division was about to march, back to City Point. Should the number in a division hospital exceed its capacity, which in at least one instance was 100, the excess was also sent to the depot facility. The twenty-bed brigade artillery hospital, unlike other field hospitals, remained at Petersburg until the end of March; artillery men falling ill or suffering wounds elsewhere entered the hospital of the division with which they were serving. The cavalry division had its own 120-bed hospital and ambulance corps with 26 ambulances, 3 medical wagons, and 15 army wagons.
Sick and wounded officers, however, did not have their own facility. Disabled officers in the field often took shelter outside hospitals, a practice McParlin wished to discourage, but no rules existed to dictate how their expenses should be handled if they were hospitalized. In March McParlin finally sent out a circular calling for officers to meet the cost of feeding themselves and any servant who attended them in the hos-
4Unless otherwise indicated, all information concerning the Armies of the Potomac and the James is based on MSH1:491-92, 495, and app.:202-23.
254
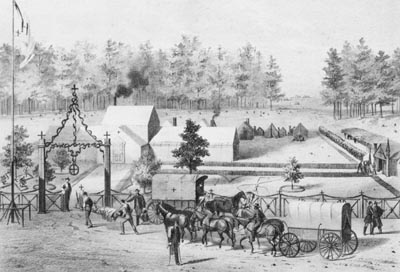
FIELD HOSPITAL NEAR PETERSBURG, VIRGINIA. (Courtesy of Library of Congress)
{kind=link}
pital, but forbidding the levying of any other charges.5
McParlin`s order meant that the depot hospital at City Point would shelter officers from both the Army of the James and the Army of the Potomac, since patients from Butler`s army outside Richmond had been using the City Point depot as a way station, whence they were soon sent to the Army of the James hospital at Point of Rocks. City Point`s popularity resulted in large measure from its easy accessibility by both water and rail, in the latter instance either directly or by means of a single change of trains at an intermediate station. Although there were some complaints of inadequate care, neither gangrene nor any form of epidemic appeared at City Point, and those familiar with the conditions under which it had to operate regarded it highly.6
City Point experienced staffing problems, however, once Grant`s force began to prepare for the final stages of the campaign in northern Virginia, nd McParlin had to order regimental medical officers on duty at the depot hospital to join their units. To replace them the surgeon general sent in contract surgeons, some recent graduates of the Harvard Medical School, committed to serve three months. The fact that contract nurses worked only in general hospitals left City Point short of attendants when commanding officers ordered the
5WOR, ser. 1, 46, pt. 2:609, 616.
6Rpt, Proceedings of Board of Inquiry (26 Jan 1865), RG 112,entry 12.
255
musicians serving as nurses to prepare to march. Veterans in the Reserve Corps who could serve in hospitals were few, and the need for a hospital corps was particularly evident. Despite the shortage of attendants, McParlin ordered the capacity of the City Point hospital, then variously estimated as between 5,400 and 6,000, expanded by 1,000 beds or more; one surgeon reported that tents were to be pitched to increase its overall capacity to 8,800. McParlin also ordered hospital transports readied to remove all patients destined for general hospitals.7
Union troops suffered more than 1,200 wounded in the enemy`s unsuccessful attack on Fort Stedman, outside Petersburg, on 25 March and captured large numbers of Confederate casualties as well, all of whom were sent to Union facilities. In the hospital of a Union division not involved in the defense of Union lines, Confederate wounded were cared for "as promptly and as kindly ... as our own men." These patients, quickly sent back to City Point to free the division hospitals to take newer casualties, were the first of a flood that would fill Union hospitals from this point on until Lee`s surrender.8
Realizing that the last stage of the campaign would require the transport of many casualties over increasing distances back to City Point, McParlin had hospital cars placed on the military railroad. His effort to have the quartermaster keep a reserve train of ambulances available for his use failed, forcing him to rely entirely on vehicles that were old and much repaired and wagons whose number had been substantially reduced. In order that unexpected demands could be met, a 36-wagon train loaded by the medical purveyor accompanied the army as it moved, and McParlin ordered supplies for 10,000 to 12,000 men kept at City Point to meet any emergency.9
It had been raining heavily before Grant began his attack on Lee on 31 March, and the downpour had turned the Virginia clay into a treacherous quagmire that rendered roads virtually impassable. Supplies were left behind to lighten wagons. Although stretcher-bearers moved with their commands, ambulance drivers pitched in to help those trying to improve the roads. Enemy action had wounded more than 1,500 from 29 to 31 March, and delays in evacuation necessitated keeping field hospitals in operation even after the troops moved on, requiring the establishment of new facilities as the army advanced even while the old ones remained open in the rear. Surgeons had to use tents to supplement available buildings along the way.10
As Union troops moved forward after Lee evacuated both Richmond and Peters-burg in the first days of April, McParlin ordered the chief medical officer of the City Point depot hospital to establish a sub depot facility as far forward as the railroad was open. He hoped, apparently, that this hospital could be set up at Burkeville, or Burke`s Station, fifty miles from Petersburg where the rail line to Lynchburg crossed that from Richmond to Danville. Twenty-five medical officers, 3 hospital stewards, and 100 attendants started out for the new depot with tents and food for 2,500 wounded, but when they arrived at Wilson`s Station on 7 April, they found they could go no further by rail. While
7Ltrs, Adam Neill McLaren to SG (6 Feb 1865),Charles Page to SG (10 Mar 1865), John Campbell to SG (17 and 30 Mar and7 Apr 1865), and McParlin to SG (25 May 1865), all in RG 112, entry 12;WOR, ser. 1, 46, pt. 2:609.
8Grant, Memoirs 2:619; quote from MSH 1, app.:220.
9WOR, ser. 1, 46, pt. 1:609.
10WOR, ser. 1, 46, pt. 1:707, 843-45.
256
awaiting the completion of repairs to the track and its conversion to a uniform gauge, they set up a facility at that intermediate point. Patients from Sheridan`s command received care at Wilson`s Station, and surgeons of the IX Corps, assigned to guard the Burkeville junction, set up their division hospitals to accommodate all the wounded from units that had pushed beyond Burkeville in their pursuit of the enemy. Confederate wounded had crowded the Burkeville hotel, so the division hospitals were housed in private homes, warehouses, tents, and makeshift shelters. Foragers were sent out to find food, while the medical purveyor`s wagons continued beyond Burkeville in the wake of the troops.11
As Grant drove his men in a relentless pursuit of the enemy, the strain took its toll. Hospital wagons and ambulances experienced difficulty keeping up with the troops, who were covering twenty to thirty miles a day. Some of the ambulance horses were "completely used up." As ambulances from the IX Corps at Burkeville shuttled to and from the front, stretcher-bearers were hard pressed because of the shortage of vehicles in which to remove the casualties. By the time the two armies reached the vicinity of Appomattox, even General Meade was among the sick, "hardly able to get out of bed," as Grant recalled, although Meade continued to obey Grant`s orders "with great energy." Under the stress, Grant himself was suffering from a persistent headache that responded neither to mustard plasters on his wrists and neck nor to mustard and hot water baths for his feet. Grant wrote later, however, that "the instant" he heard of Lee`s readiness to surrender, he was "cured."12
The end of the war in Virginia led to a gradual closing of the field and depot hospitals that had served Grant`s men, including, finally, the main depot hospital at City Point. McParlin estimated that this facility had admitted more than 11,000 wounded from units under Grant from 1 January through 31 May 1865. Including the sick, in the first six months of 1865, over 26,000 patients passed through City Point. Of these, more than 12,000 were returned directly to duty. McParlin sent those wounded in the last days of the campaign back to City Point as promptly as possible and after Lee`s surrender continued to empty his field hospitals by sending 2,000 more back. On 30 April, he ordered the capacity of the City Point hospital reduced to 2,500 beds. On 4 May the Medical Department moved the facility to Alexandria, and destitute former slaves apparently took shelter in the vacant buildings. Three weeks after its final move, the hospital closed and its remaining patients were transferred to general hospitals, whence they were eventually discharged from the Army.13
The Burkeville sub depot of the City Point hospital took in 660 sick and 192 wounded during its existence, from 9 to 30 April, 838 of whom went on to City Point. For part of this period, both the Army of the Potomac and the Army of the James camped at Burkeville, and Confederate wounded still occupied a hotel there, but many of the wounded at the facility also came from Farmville, where after occupying the town, Union forces had shared a large Confederate hospital. By 11 April, railroad cars supplied with straw for bedding were available to move 1,450 of the 2,200 patients in the various facilities in
11Reed, Hospital Life, pp. 160, 168.
12Quotes from Grant, Memoirs 2:466, 482-83, 485.
13A. W. Smith, Reminiscences, p. 47; Ltr, McParlin to SG (12 Apr 1865), RG 112, entry 12.
257
the Burkeville area. Two attendants accompanied each car, and medical officers rode every train to City Point. Another 600 patients started back on 12 April, but because of a transportation shortage, 150 Confederate patients remained at Burkeville. Ambulances continued arriving at this sub depot from field hospitals, however, so by the 13th, another 450 awaited transportation. On 29 April ambulances began moving Confederate patients from Farmville to the sub depot on the first leg of their journey to hospitals set up for them within the city of Petersburg. Small numbers of sick and wounded continued to arrive at Burkeville even after McParlin closed the facility and sent its supplies and hospital train on to City Point.14
In mid-April, with the war all but over, a surgeon with the Army of the Potomac noted that disease had become a greater problem than it had been when the troops were in action. Perhaps it was easier for disease to spread when the men remained longer in one spot and water sources were more likely to become contaminated with the organisms that cause diarrhea. The cases of diarrhea that McParlin was encountering, however, were markedly more severe than they had been. The surgeon blamed not only bad water but fatigue and, above all, the lack of vegetables. No obvious cases of scurvy confronted him except for a few in men newly returned from southern prisons, but these returnees, wherever they were, caused much anxiety among Army physicians, since their deprivations in the South had severely undermined their health.
Nevertheless, the fighting was over for the Army of the Potomac. For the medical officers who accompanied it, the months of struggle to keep pace with an aggressive, at times very fast-moving campaign that often left them without an adequate number of ambulances and sometimes without adequate field facilities as well, were behind them. The war was not yet over, however, for further south the army of Confederate General Joseph Johnston still struggled on.
Sherman`s Campaign
For the four Army corps of the Military Division of the Mississippi that would defeat Johnston, the first months of 1865 brought a march from Savannah, Georgia, to Raleigh, North Carolina, during which the men once again lived largely off the land. Sherman had great confidence in the "quiet, industrious, and most skillful" surgeons who accompanied him, but the nature of his campaign placed a considerable burden upon them from the outset by once again requiring that what they took with them be strictly limited. Sherman did not on this occasion, however, plan to keep his sick with him, and by having them promptly evacuated east to ports whence transports could move them north, he also limited the number of patients who would draw upon the supplies he brought with him.15
In Savannah, preparing for the campaign to come early in 1865, John Moore, medical director under Sherman, set up hospitals, staffed for the most part with contract surgeons, where he could leave those unable to march. He drew one month`s supplies from the resources accumulated for his use by the medical purveyor at Hilton Head, South Carolina, apparently planning to rely heavily upon
14Grant, Memoirs 2:513.
15WOR, ser. 1, 47, pt. 1:17, 119; quote from 1:46. Unless otherwise indicated, all material on Sherman`s campaign is based on MSH1, app.:321-23, 327-29, 337-39.
258
what his foragers could find along the way. He attempted in vain, however, to acquire new ambulances to replace the aged and worn vehicles that were all he had. In mid-January Sherman and 60,000 men started out, but the rains that had flooded swamps and rivers forced the temporary abandonment of the move. While they awaited a change in the weather, surgeons sent those who fell ill back to the hospitals in Savannah and contained an incipient epidemic of smallpox by isolating the twenty-five cases that appeared in a three-day period.16
Sherman`s men were able to advance again early in February, and on the 17th the right wing entered Columbia, South Carolina, which had been virtually abandoned by its defenders. As Confederate garrisons along the coast began to surrender, Union soldiers also occupied such cities as Charleston and Wilmington, North Carolina. Medical Director Moore noted that, despite the weather, an average of only 2 percent of the army was sick. He concluded that the variety and abundance of food gained by foraging and the absence of opportunities for drunkenness, as well as the high spirits of the men, contributed to the army`s health.17
The Union force paused for a few days when it reached Fayetteville in North Carolina on 11 March. Surgeons then shipped 200 to 300 of the approximately 1,500 disabled, most of whom were sick rather than wounded, by river east to Wilmington, where the surgeon general ordered five contract surgeons sent to assist in their care. The men remaining with Sherman were at this time still in good condition, according to that general. Relatively few had been wounded, and although their wounds tended to be severe, causing more deaths than might otherwise have been expected, amputees did surprisingly well after surgery, presumably because of a low rate of infection. When Sherman arrived at Goldsboro, however, the disease rate had doubled. Over 3,000 of his men were ill and more than 1,100 wounded as a result of encounters with Confederate forces. Surgeons once again sent the seriously disabled east to the coast, on this particular occasion to New Bern, North Carolina, where Barnes sent five more contract surgeons to assist in their care.18
Despite the difficulties he encountered as Sherman`s force moved north, Moore believed that his care of the sick and wounded was adequate. Letterman`s system for managing evacuation and field hospitals was proving successful. The 100 new ambulances that arrived during the course of the campaign were, however, but one-fifth of what Moore needed, and since these vehicles were still scarce, surgeons once again had to rely on army wagons to evacuate their patients. Moore reported during March that he was experiencing no shortage of items necessary to the care and comfort of his patients, and after the occupation of Goldsboro at the end of the month, the supplies that had been awaiting them arrived from New Bern. He noted that by the 26th all the sick and wounded were comfortable in bunks set up in tents or private homes and that all patients did well, partly because their health was excellent when they were wounded.19
16Sherman, Memoirs 2:260; WOR, ser. 1, 47, pt. 1:439-41; Ltrs, Moore to SG (30 Jan and 30 Mar 1865), Campbell to SG (13 Jan 1865), and Clymer to SG (4 Feb 1865), all in RG 112, entry12.
17WOR, ser. 1, 47, pt. 1:440.
18WOR, ser. 1, 47, pt. 1: 188, 440; Sherman, Memoirs2:296, 298, 305; Ltrs, Campbell to SG (13 Mar 1865) and Moore to SG (14Mar 1865), both in RG 112, entry 12.
19WOR, ser. 1, 47, pt. 1:441; Ltrs, Clymer to SG (14Mar 1865) and Moore to SG (30 Mar 1865), both in RG 112, entry 12.
259
Although Moore was happy about the condition of the men and Sherman himself described them as "saucy" despite their "dirty, ragged" state, the Sanitary Commission had received a contrary impression of the state of affairs. Not allowed by the general to come near troops in the field because he believed that the commission members favored men from their own communities, they nevertheless concluded that the men must be in poor physical shape. Since, by his own admission, Sherman had "gained the ill-will of the agents of the Sanitary Commission," some commission officials may have been eager to conclude the worst.20
While Sherman was leading one army north from Savannah, Maj. Gen. John M. Schofield was leading another in a successful campaign to take Wilmington, through which Sherman could then receive supplies and evacuate his sick and wounded by hospital transport. Apparently unaware of the secretary of war`s firm instructions to General Butler late in 1864 and of the issuance of general orders forbidding the removal of hospital vessels from Medical Department control early in 1865, Schofield appropriated the S. R. Spaulding for use as his headquarters. He pointed out, when taken to task, that the vessel had been merely "lying idle without a single sick or wounded man on board.... of no use but to furnishing quarters to three assistant surgeons, who had nothing to do but lounge in the steamer`s cabin. "He added that the Spaulding could still be used as a hospital ship when he was aboard, and, indeed, was all the better suited for that purpose, since as his headquarters, she moved up and down the river, following the action and thus close to the largest number of wounded.21
Schofield and troops from New Berri and Wilmington joined Sherman`s troops before they left Goldsboro on 10 April. The Confederates retreated before this enlarged force, which was still pursuing Johnston toward Raleigh when the news of Lee`s surrender arrived. The main body of Johnston`s army no longer formed a real threat to Sherman`s men, and in his haste Sherman moved ahead of a group of convalescents accompanied by twenty-three hospital attendants, leaving them vulnerable to an attack by guerrillas on 11 April, when all but two were captured. Sherman continued north despite the attempts of Confederate cavalry to slow him, and entered Raleigh on 13 April, where the next day he received a Confederate request for a truce. The process of finding an acceptable formula for Johnston`s surrender proved surprisingly tedious, but word of the truce was sent to other units fighting under Sherman, and fighting in the Deep South came to an end.22
While Moore moved north with Sherman to manage the care of those wounded or falling ill with the army, members of the medical staff of the Department of the South struggled to care for the men left behind. Those who could no longer fight presented a considerable problem for the medical director, surgeon of the volunteers Meredith Clymer. The release or exchange of many former prisoners of war only added to his difficulties. In March, anticipating that disease might create a need for a temporary general hospital in Charleston, Clymer prepared to open one on short no-
20Sherman, Memoirs 2:306, 392, quotes from both; Maxwell, Sanitary Commission, pp. 280-81; WOR, ser. 1, 47, pt. 1:190; "Report of M. C. Read" and "Letter From Mr. Seymour," both in Sanitary Reporter 2 (1864):165 and 191, respectively.
21WOR, ser. 1, 47, pt. 2:342-43, 545, 832-33, quote from 2:833; WOR, ser. 3, 4:1156.
22Sherman, Memoirs 2:342-44, 346-63.
260
MEREDITH CLYMER.(Courtesy of National Library of Medicine.)
{kind=link}
tice, a step he apparently was never actually required to take. Clymer tried to prevent overcrowding in his department by moving patients retained at Savannah north as soon as they could tolerate the voyage and transports could be obtained. He lowered his patient load there from 2,800 in late February to 800 a month later. He hoped that by continuing to send patients north he could reduce any facilities he might have to establish in Charleston and Savannah to post hospitals and concentrate future casualties at port cities further up the coast.23
Contract surgeons staffed many of the facilities serving returning prisoners of war as well as the men Sherman left behind. Clymer distrusted these physicians, however, and rejoiced in May when he discovered that the sick rate was lower than he had anticipated among the 4,000 who returned to Union control in Florida and that his earlier request for six contract surgeons had become unnecessary. Permitted to terminate their contracts after three months, acting assistant surgeons tended to head north when the sickly season began. Having repeatedly but apparently vainly urged that they be signed for six-month terms, Clymer could only hope to function without them. After the war ended, several assistant surgeons of the volunteers were assigned to the quarantine stations at such yellow fever-threatened ports as Charleston, Savannah, and Fernandina, Florida, reducing the number of physicians available to care for the new, unacclimated troops that were arriving in the South to man new posts. Although recovering patients were being discharged from the Army directly from hospitals, Clymer was forced to call again and again for contract surgeons to replace those who went north for the summer.24
Adding to Clymer`s woes in the Department of the South was the fact that authorities there did not initially honor the law of March 1864 concerning ambulances and their use. For more than two months Clymer agitated and appealed, pointing out that, contrary to law and custom, the Medical Department in his area exercised no control over the use of ambulances. He cited stories of pleasure jaunts from which neither the line officers appropriating the vehicles nor the ambulances always returned safely. Only on 5 May did Maj. Gen. Quincy A. Gillmore, commanding in the Department of the South, order that all
23Ltrs, Cuyler to SG (17 and 23 Mar 1865) and Clymer to SG (22 Mar and 22 Apr 1865), all in RG 112, entry 12.
24Ltrs, Clymer to SG (29 and 30 Apr, 6 and 19 May, and 8 and 24 Jun 1865), all in RG 112, entry 12.
261
ambulances, medicine wagons, and similar vehicles be placed under the control of his medical director.25
Units under Sherman`s command were not limited to service on the coast. Men led by Maj. Gen. James H. Wilson crushed the last significant Confederate resistance in Alabama and western Georgia. Fifty medical officers accompanied Wilson and his 13,500 men through Alabama from west to southeast, beginning in late March. Despite daily marches that sometimes covered more than twenty-five miles, neither wounds nor diseases caused major losses. On 2 April Wilson`s surgeons established a hospital in a church at Plantersville, where 2 doctors and attendants remained to care for 40 wounded and 18 sick while the command continued on to Selma. After Wilson launched a night assault, Confederate Lt. Gen. Nathan B. Forrest retreated from Selma back to Plantersville and captured the unguarded Union hospital. Forrest required the attendants and those patients who were only slightly wounded to swear not to participate further in the war before paroling them, but he let the surgeons care for the seriously injured without interference. When Forrest left Plantersville, Union medical officers brought the patients there south to Selma, where they had established corps hospitals to care for the 24 officers and 212 men wounded in taking the town. When the command resumed its march, 2 surgeons remained at Selma with the 68 patients who could not be moved, keeping with them forty days worth of rations and other supplies. All who could endure travel, however, were loaded into ambulances and wagons for the journey to Montgomery.26
When Montgomery surrendered to Union forces on 12 April, medical officers entering the city were alarmed to discover that a smallpox epidemic was" raging furiously." Fortunately, vaccination proved effective for Wilson`s men, and the epidemic did not spread among them. Doctors unloaded the wounded and placed them in a local hospital. Because the disabled had proved a serious encumbrance when moved with the army, Wilson now decided to leave 144 of them in Montgomery with an assistant surgeon when he continued east on 14 April. The division that went on to Columbus, Georgia, sustained an additional 28 wounded in capturing that city four days later. The taking of West Point the same day produced 30 more Union wounded. Leaving 35 patients at Columbus, Wilson moved on to take Thomaston on the 19th and Macon on the 20th before word of Sherman`s armistice agreement with Johnson ended his campaign.27
Wilson`s medical director, Surgeon Francis Salter, was quite pleased with the way his branch of the Medical Department had functioned during this campaign. Despite the speed with which the army moved, no patients were left by the roadside or cared for in makeshift shelters. "Regularly furnished hospitals" received all casualties. Although Salter had apparently been concerned about whether an ambulance corps could function effectively for cavalry units, his experience in this campaign led him to conclude that such an
25Ltrs, Clymer to W. S. M. Burger (copies, 23 Feb and 29 Apr 1865) and to SG (29 Apr 1865) and GO, Gillmore (no. 56,5 May 1865), all in RG 112, entry 12.
26Unless otherwise indicated, all material on Wilson`s march is based on MSH 1, app.:327-29. A report of 22 rather than 212 men wounded is probably a typographical error, since 35 were killed in taking Selma: WOR, ser. 1, 49, pt. 1:406.
27Quote from MSH 1, app.:328-29.
262
organization could be as effective for cavalry units as for infantry.28
The medical officers caring for the sick and wounded of the two corps that took Mobile on 11 April encountered few significant problems, despite the fact that Maj. Gen. Edward R. S. Canby allowed only a single ambulance for every 400 men (under the law of March 1864, a regiment of 500 men should have had two ambulances). He had an additional ambulance permanently attached to each artillery battalion, and two more for each army headquarters and each corps headquarters. Three wagons were to accompany each division hospital train to carry hospital tents and other equipment. Predictably, the number of ambulances available during the siege of Spanish Fort and Blakely, Alabama, guarding Mobile, proved inadequate, and once again wagons had to be used to carry some of the wounded.29
No deficiencies appear to have marked the work of Canby`s ambulance corps or the organization and management of division hospitals, to which were allotted one hospital tent for every 600 men in the division. At Spanish Fort enemy fire delayed the removal of casualties from the field until dark each day. Their able-bodied comrades covered the wounded with rubber blankets, thus limiting their sufferings in the heavy rain. At Blakely, shells from the enemy gunboats forced surgeons to move division hospitals several times. Boats removed casualties from field hospitals at both Spanish Fort and Blakely to general facilities in New Orleans within two or fourdays.30
The ordeal that Mobile was to endure at the hands of the Union Army was not yet over. Late in May ammunition stored in a warehouse there exploded, causing what a witness described as "a terrible calamity- beyond description. Acres of ground were covered with flames.... The loss of life [was] terrible... several steamers were torn to pieces." The hospital serving Army engineer units was totally destroyed, and the interior of the building used as a freedman`s hospital was gutted. All the injured were initially taken into the city`s hospital for merchant seamen, where white victims remained while blacks were quickly moved to another facility. Because the accident occurred just as regimental medical officers were leaving the city with their units, the surgeon in charge of the general hospital at Mobile sent out a frantic call for more physicians, and Canby ordered that all medical officers in the area come to the aid of the injured.31
Except for those areas in which Union troops commanded by Grant or Sherman were fighting the last major battles of the war, Army surgeons were already beginning to return to their peacetime occupations. In Arkansas the surgeon at Helena converted the 250-bed general hospital into a post facility in March. At Fort Smith, newly reoccupied after its evacuation in 1864, the chief health problem was apparently scurvy. The countryside had been so devastated that no vegetables were available locally, and guerrillas continued to threaten shipments coming in. A Sanitary Commission agent offered seeds to start a post garden, the Western Sanitary Commission furnished some vegetables, and the department`s commanding officer ordered a special issue of vegetables to control the
28Quote from MSH 1, app.:329.
29WOR, ser. 1, 49, pt. 1:791; MSH 1, app.:337-39.
30MSH 1, app.:337-39.
31WOR, ser. 1, 49, pt. 2:741, 911-14, quote from pp 912-13;Ltr, Samuel Kneeland to Abadie (26 May 1865), RG 112, entry 12.
263
inroads of scurvy until local crops could mature.32
It was also west of the Mississippi, at Brownsville, Texas, that on 13 May 1865 a small number of Union and Confederate soldiers fought the last battle of the Civil War. Although the 26 May surrender of this last Confederate army formally ended the war, for the Medical Department a considerable challenge remained. The end of the conflict brought with it the release of the last prisoners remaining in captivity in the South and the beginning of the return of Confederate prisoners to their homes, with Union surgeons being responsible for the care of the sick and wounded in both groups. The apparatus of war also had to be dismantled, and the transformation of the Medical Department to a peacetime organization would not be complete for many months.
Prisoners of War
Although the difficulties involved in maintaining or restoring the health of prisoners of war peaked in 1865, the challenge was not new. From the outset, the Medical Department of the Union Army had been responsible for the prevention of disease in Northern prisons, for the health of Confederate captives, and for the care of sick and wounded Union soldiers returned through exchange or released by successful Union armies. Union surgeons had little to do, however, with the care of Northern men while they were in Southern prisons, since during most of the war, medical officers were not held captive, and when they were imprisoned, they were apparently concentrated at Richmond rather than distributed among the various prisons throughout the South.33
In the earliest months of the war, the governments of the Union and Confederacy had not agreed upon the status of physicians. Medical officers taken in April 1861 in Texas were paroled and allowed to return home after swearing not to care for combatants until formally exchanged. Surgeons on both sides were held captive for varying periods of time until the spring of 1862, when the Union War Department ordered all medical officers "unconditionally released." This order was not invariably obeyed, as there were apparently some misunderstandings about it, but generally for a time thereafter both sides released surgeons unconditionally, allowing medical officers to stay with the captive wounded of their own armies until their captors could provide adequate medical attendance.34
In 1863, however, the state of Virginia claimed that a certain captured Union medical officer had committed crimes punishable under state law. He was, therefore, ineligible for return under any circumstances until he had been tried. Union authorities reacted by claiming the right to hold Confederate physician hostage against the safe return of the Union surgeon. The agreement to return medical officers unconditionally collapsed completely in July when Confederate authorities refused to recognize the Union`s right to hold a hostage. As a result, although it was still possible to be released by means of exchange, many medical officers apparently concluded that the possibility of long impris-
32"Report of Mr. Carpenter," Sanitary Reporter 2 (1864):166; SGO, Sanitary Report of the Army of Arkansas,1865-66, Ms C 126, NLM; U.S. Army, Medical Department, U.S.A. General Hospitals in Existence, January 1865, Ms B125, NLM.
33WOR, ser. 2, 5:953 and 6:619.
34WOR, ser. 2, 1:62, 73-75, 4:27, 33, 37, 39, 44, 101-02,268-69, 272, and 5:164, 262, quote from 5:262.
264
onment dictated that they take fewer chances of being captured.35
The impasse ended late in 1863, when finally Confederate authorities returned the Union surgeon whose plight caused the problem, apparently still untried-his guilt appears highly questionable-and both sides ordered the release of all medical officers. Captives were by then in prisons far from the front, however, and their return proved tedious. Word that physicians were to be released did not always reach prisons in a timely fashion. In one instance, Confederate refusal to allow a flag-of-truce boat to carry Confederate physicians on the final leg of their journey home led to additional difficulties when General Butler concluded that the alternative of letting, these doctors through his lines in Virginia would be unsafe because they would then "know too much." The status of hospital stewards caused further confusion, but in March 1864 the War Department ruled that these men were to be treated in the same manner as surgeons.36
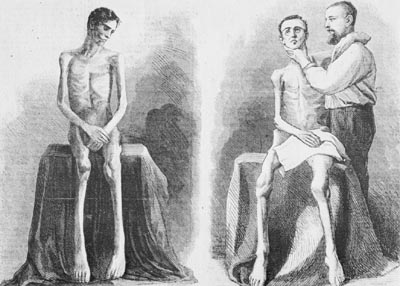
Although they rarely cared for men held in Confederate prisons, Union surgeons assumed responsibility for their health when they returned from the South. Until Union armies began to occupy large areas of the Confederacy, only limited numbers of captives returned home, but as the war went on, these men presented a growing challenge to the Medical Department because of their numbers and their condition. Many were sick before they started north, and those who remained in captivity until the last months of the conflict suffered increasingly from the effects of an inadequate diet and often from the effects of exposure and poor sanitation as well.
Despite a formal agreement in 1862 calling for the parole of all prisoners within ten days of their capture, actual exchanges were erratic because of squabbles concerning interpretation. Some difficulties apparently arose from the Union`s lack of enthusiasm for a step that would renew the Confederacy`s dwindling manpower supply by returning healthy prisoners. The Union seems to have been less reluctant to take part in exchanges of those "who will not soon be fit for service." The cartel of 1862 called for most exchanges, whether of healthy or disabled men, to take place through the City Point area or Vicksburg, but wounded prisoners could also be re-turned directly to their units shortly after battle on the initiative of individual commanders involved.37
By the fall of 1863, the effects of malnutrition upon invalids returning from the Richmond area via City Point were pronounced. As often happened, a few of the disabled men sent from City Point to Annapolis hospitals died before reaching Maryland. Many returnees had diarrhea, and chronic diarrhea was the most common cause of deaths occurring soon after exchange, although pneumonia and debility added to the toll. Some taken at Gettysburg maintained that their wounds had never received medical attention. With sick prisoners returning in such precarious health, Union authorities soon realized that extraordinary measures would be necessary to limit suffering and the number of deaths. Medical officers began to accompany the vessels that picked up the returnees at City Point, and at the end of
35WOR, ser. 2, 5:212 and 6:13, 18, 26-27,35-36, 81, 85, 88-89, 157-58, 208-09, 250, 283, 335-36, 473-74, 762; Solon Hyde, A Captive of War (New York: McClure, Phillips & Co., 1900),p. 54.
36WOR, ser. 2, 6:1078, 7:127-28, 141, 481,491, 710, 853, 860-62, and 8:156, quote from 7:412-13.
37WOR, ser. 2, 1:518, 4:266-68, 6:124, 129, 134, 512, 523, 599, 615, 629, 995, and 7:76, 108, 215, quote from 7:75; Hyde, Captive, p. 51.
265
CONDITION OF RETURNEES FROM SOUTHERN PRISONS. (Courtesy of Library of Congress.)
{kind=link}
266
November 1863 the surgeon who acted as medical inspector of prisoners of war, Augustus M. Clark, reported that a contract surgeon, a contract hospital corpsman, and two nurses were serving on the truce ship.38
On an average run, the truce ship carried 600 men, only 5 percent of whom needed immediate care during the 16 to 20-hour voyage to Annapolis, and no addition to her fifty-six hospital bunks was necessary. But when the ship carried exclusively sick returnees, facilities on board were inadequate, even when an additional ten bunks were set up on deck. By early 1864, however, the Medical Department had succeeded in obtaining hospital transports to move the sick and wounded. Sometimes, if the patients` condition permitted, these vessels took them beyond Annapolis to hospitals in Baltimore and Philadelphia, since even before the start of 1865, thousands of sick and wounded returnees whose condition was "indescribable" were almost overwhelming Annapolis facilities.39
In 1865, as Sherman drove north through the Carolinas, newly released prisoners, many in need of medical care, began gathering in Wilmington for transportation to hospitals farther north. By March 1865, 3,700 sick former captives were crowding facilities in North Carolina. The surgeon general diverted medical supplies and officers intended for Sherman and Schofield to the care of the newly released prisoners. Quick attention and prompt transfer north interrupted a typhoid fever epidemic, but a shortage of clothing and bedding rendered the voyage arduous, and the "wretched condition" of many made it advisable in some instances to terminate it at Fort Monroe. A contract physician at Annapolis, where many returnees from Wilmington arrived in the spring of 1865, maintained that they were being shipped without medical attendance, crowded, and "in a most horrible plight." The most desperately sick or wounded were packed in the hold, where the ventilation was entirely inadequate. The medical officer responsible for loading the ships at Wilmington, however, pointed out that it was impossible to spare a physician to accompany each ship and insisted that only those who appeared able to withstand the voyage were sent north. Prisoners had started arriving at Wilmington only five days after Union forces took the city, he said, but he insisted that, although the quartermaster general was initially unable to supply enough blankets and bedding for all returnees, those sent to Annapolis were adequately provided for.40
The situation in which sick and wounded prisoners returning through Vicksburg found themselves was similar to that in the East, and many patients died before they had been long in Union hands. Prisoners released from Andersonville were in particularly deplorable shape, almost all needing medical care. Exchanges were cut off during several months of 1863 while Grant was closing in on Vicksburg, but in 1865 so many prisoners were returning that the city`s hospitals had to be emptied of other patients. Surgeons sent many north to St. Louis and even beyond, but hospital steamers could not keep up with the demand. In April, the explosion of the steamer Sultana after it left Vicksburg killed 1,100 returnees
38WOR, ser. 2, 6:446, 474-75, 494, 593,and 1089.
39WOR, ser. 2, 6:535, 593, and 7:69, 101, 1161, quote from 7:1160; Ltr, McCormick to SG (17 Apr 1864), RG 112, entry 12.
40First quote, Ltr, Cuyler to SG (23 Mar 1865), and second quote, Ltr, J. Simpson to SG (12 Mar 1865), both in RG 112, entry 12; Ltrs, Cuyler to SG (25 Mar 1865) and Shippen to SG (23 Feb and 26 Mar 1865), all in RG 112, entry 12; WOR, ser. 2, 8:464-65; War Department, SGO, Annual Report, 1865, p. 7.
267
and added still further to the strain on the evacuation system, although surgeons were able to send the 500 injured survivors on to Memphis.41
When caring for enemy prisoners rather than their own returnees, authorities in the North and South alike occasionally exhibited a certain vengefulness. The "Instructions for the government of armies of the United States in the field" issued by the Union in April 1863 maintained that the Confederate prisoner was a "public enemy," who should be "penitent" and should not be coddled. Prisoners should not receive clothing beyond that absolutely necessary, regardless of whether the clothing came from the federal government or from friends. In 1864 Union authorities, including Surgeon General Barnes, General Halleck, and Secretary of War Stanton, agreed not to furnish able-bodied captives a diet any better than the one Confederate soldiers were receiving from their own army in the field. A Southern medical officer fulminated against what he took to be "the indifference and brutality" of the federal government, as typified by the inadequate diet, shelter, and hospital facilities made available to Southern prisoners of war.42
Union authorities were kinder to the sick and wounded among their captives than to the able-bodied. After the battle of Gettysburg, they ordered medical officers to ensure that Confederate patients were treated with all the care granted Union casualties, but that they should be confined in separate facilities from those sheltering Union soldiers and receive "only such [clothing] as is absolutely necessary." The hospitals themselves, according to advice given by an officer responsible for prisoners of war, were not to be "fitted up with all the conveniences which are provided in hospitals for Federal soldiers," but only to be adequate "to meet all necessary wants of the sick." Ideally, furthermore, prisoners should not be hospitalized south of Nashville.43
In spite of the restrictions placed on the care given Confederate prisoners and the accusations made by each side concerning the treatment of prisoners of war, some observers, both North and South, excluded medical officers from their diatribes. The same Southern physicians who wrote of Northern indifference and brutality noted that Union surgeons were compassionate. Speaking for the Union, General Butler informed Secretary of War Stanton in February 1864 that he had "received less complaint of the treatment by rebels of our prisoners in hospitals than elsewhere." He added that he had had "occasion to know, the treatment in the hospitals by rebels of our soldiers prisoners in their hands [has] been reasonably proper and sufficient."44
Although the death rate among Confederate soldiers in Union hands was less than that of Northern soldiers in Southern institutions, more than 26,000 of 220,000 rebel captives died during the course of the war. This rate of 12 percent compared favorably with the almost 18 percent characteristic of Confederate prisons, where 22,576 of approximately 126,950 Union
41WOR, ser. 1, 48, pt. 1:217 and ser.2, 8:477-78, 492-93; Benjamin Woodward, "Among the Prisoners" and "Letters From Mr. Tone," both in Sanitary Reporter 2 (1864):188 and 190, respectively; Ltr, Azpell to Wood (8 Apr 1865), RG112, entry 12.
42WOR, ser. 2, 6:602, 7:151, and 8:161, first and second quotes from 5:674 and third quote from 6:102; J. A. Wyeth, With Sabre and Scalpel, the Autobiography of a Soldier and Surgeon (New York: Harpers, 1914), pp. 286-92, fourth quote from p. 286; MSH 1, app.:324-25.
43WOR, ser. 2, 5:676, 6:98, 106, and 8:5, first quote from 6:149 and second and third quotes from 7:468; A. W. Smith, Reminiscences, p. 133.
44Wyeth, With Sabre and Scalpel, p. 287; WOR, ser. 2, 6:601, quotes from 956.
268
prisoners died, despite the fact that from the outset many Confederate prisoners suffered from the effects of an inadequate diet. Although they were sick as often and suffered from the same diseases as Confederate soldiers in the field, twice as many Confederate captives died. One authority suggested that it was possible that the least healthy were the most likely to betaken prisoner. Almost 6,000 deaths in Union prisons resulted from diarrhea and dysentery, over 5,000 from respiratory diseases, and just under 3,500from smallpox, measles, erysipelas, scarlet fever, and similar rash-producingdiseases.45
Setting the policies that governed the management of prisons and the hospitals that served them was a relatively simple matter, but the attitudes that lay behind these policies may well have contributed to the relatively high death rate in many of these institutions. Northern camps were hastily established at a time when large numbers of prisoners, many in poor health, were coming in. As a result, these camps often acquired unenviable reputations that challenged Army physicians, but improvements were not always immediately forthcoming.
Medical inspectors and prison doctors attempted to prevent diseases at these prison camps as well as to cure them, inspecting sanitation and living conditions in the prisons and their hospitals and making recommendations for improvements. Worst among the institutions for which they were responsible was Elmira, New York, "a perfect pest hole" established in 1864,where 241 of every 1,000 prisoners died each year it was in operation. Diarrhea and dysentery killed almost 1,400 of the 12,000 men who were atone time or another imprisoned at Elmira. One factor contributing to the high disease rate was the drainage of effluent from the sinks into a pond within the camp`s boundaries. Another was the paucity of fresh vegetables available in the diet. Since the vitamin C reserves of most of the men confined there were undoubtedly low, scurvy afflicted a large number, atone point as many as 2,000 at a time.46
Conflict between the camp commander at Elmira, Benjamin Franklin Tracy, future secretary of the Navy, and the chief medical officer, a surgeon of the volunteers, contributed to the difficulties in both the camp and the hospital attached to it. The entire medical staff, which in addition to the chief surgeon included seven contract surgeons, an assistant surgeon to a militia unit, and a New York State National Guard assistant surgeon, accused Tracy of interfering in the management of the hospital and thereby making their work more difficult. Although the Medical Department`s investigation of the prison hospital confirmed the surgeons` complaints, Commissioner General of Prisoners William Hoffman concluded that all concerned, medical staff and camp commander alike, were incompetent. Under Hoffman`s prodding, however, Tracy improved camp drainage and pushed the building of better accommodations for the prisoners.47
So much illness among so many men at Elmira initially threatened to overwhelm hospital facilities regardless of what anyone could do. The hospital was still under con-
45MSH 1, pt. 3:47; WOR, ser.2, 8:948; USSC, Documents 1, no. 55:22.
46MSH 1, pt. 3:63, quote from p. 56; WOR, ser.2, 7:465, 1093.
47Benjamin Franklin Cooling, Benjamin Franklin Tracy, Father of the Modem American Fighting Navy (Hamden, Conn.: Shoe String Press, Archon Book, 1973), pp. 22, 28-33; WOR, ser. 2, 7:878, 892, 918-19, 989-90, 997, 1025, 1042-43, 1050, 1092, 1093-94, 1124, 1133-34, 1135.
269
struction when the first Confederate soldiers began arriving, and the sick among them had to lie on bare bunks. Straw for bedding and medical supplies arrived only after several weeks, but by October the hospital contained six new wards with an average of sixty-two beds each. The completion of yet another ward in November allowed the abandonment of an old one. Construction continued until, by the end of the year, four more hospital buildings were approaching completion.48
Sickness was on the increase, however. Smallpox had broken out and, since a delay in the arrival of vaccine made the immediate immunization of the entire camp impossible, new cases continued to appear. By 24 January 1865, 397 men had been sent to the tents hastily pitched to isolate smallpox patients, and hospital accommodations remained inadequate. Perhaps motivated by the need to reduce the population at Elmira, the surgeon in charge was less discriminating than he should have been in selecting patients for the 41-hour voyage to the exchange point, and some men broke down under the strain. Even so, the hospital remained crowded, and in February 1865a medical inspector found 200 patients being cared for in their quarters when in his opinion they should have been hospitalized. In mid-March the excess hospital patient load was still being cared for in quarters, and more than 1,700 of 6,000 prisoners were sick. An inspector reported their condition as "pitiable." Only the end of the war and the return of warm weather led to significant improvement in conditions at Elmira shortly before its closing late in June.49
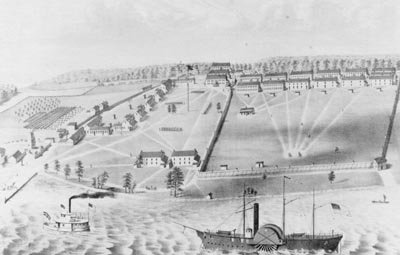
The Medical Department regarded Johnson`s Island, on the other hand, as one of the healthiest prisons. It opened early in 1862 on a 360-acreisland near Sandusky, Ohio. Drainage was excellent, the water good, and the diet almost ideal. Most of the prisoners were officers, however, and thus may have been in better health at the time of their capture than the enlisted men who formed the majority of prisoners at camps like Elmira. The regimental surgeon in charge at Johnson`s Island for much of the time it was in operation was a Union physician, but he was assisted by Confederate surgeons, doctors who had been serving in the Confederate Army as line officers and therefore were not released. The surgeon in charge was authorized to hire contract surgeons when he needed them, but the isolation of the prison made finding civilians willing to serve for $80 a month difficult.50
Medical Inspector Clark found much to criticize at Johnson`s Island in spite of its wholesome location and the health record of its inmates. In the fall of 1863, the hospital was in need of repair and improved ventilation, the wards were crowded and badly kept, more physicians were needed 9 and the nursing, which was probably done by prisoners, was careless. The latrines were badly maintained, and some of the beds "in a horribly filthy condition." Even when improvements were made at the hospital, the camp kitchens and latrines remained filthy, policy in such matters having been "left to the caprice of the prisoners themselves," and the patients` clothing was inadequate for cold weather. By late July 1864, although the hospital was well-policed and the patients were receiving good care, the prison itself had not improved. The number of sick was growing rapidly, principally because of diarrhea
48MSH 1, pt. 3:56; WOR, ser.2, 7:1173, 1272.
49MSH 1, pt. 3:57, quote from p. 57; WOR, ser.2, 8:181, 232.
50WOR, ser. 2,3:196 and 6:827-28; MSH 1, pt. 3:54.
270
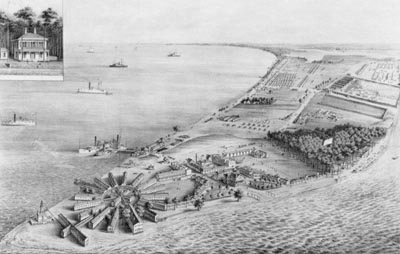
UNION ARMY PRISONER OF WAR CAMP, Johnson`s Island, Ohio. (Courtesy of Library of Congress.)
{kind=link}
and dysentery. Under the stress of imprisonment and disease, some prisoners developed scurvy, and the surgeon increased the allotment of onions to sixty pounds for every 100 men twice a week. Nevertheless, the annual sick rate of 811 per 1,000 and the death rate from all causes of 35.4 per 1,000were less than a fifth that of the second most healthy prison.51
The health problems experienced at many of the prisons were similar-diarrhea, dysentery, fevers, respiratory diseases, and occasionally scurvy. At many prisons, smallpox, classified as an eruptive fever, was a minor problem, but at Alton, Illinois, it was responsible for greatly increased disease and death rates. The fact that from Alton healthy prisoners were usually sent quickly to other prisons, leaving their sick comrades behind, contributed to misleading statistics, but the long-lasting epidemic a Alton raised the annual sick rate to 10,000 per 1,000, compared to 1,544 at Elmira. The death rate at Alton was also higher than that at Elmira, although dysentery and diarrhea took a higher toll at the New York hospital. The prison surgeon at Alton had believed that he could successfully isolate his smallpox patients within the prison, and by the time he realized he was wrong, smallpox was afflicting guards as well as inmates and was threatening the civilian population of the area as well. Despite a policy of vaccinating every new prisoner on arrival, the disease flared anew as each new group of prisoners
51WOR, ser. 2, 6:364-66, 826-28 and7:484-85 ` first and second quotes from 6:365 and 827, respectively; MSH1, pt. 3:61.
271
arrived, and the surgeon in charge finally concluded that the vaccine he was receiving from St. Louis was worthless. The medical inspector who came to the prison at the end of July at the request of the desperate medical officer recommended that a smallpox hospital be established outside the confines of the prison. In August, despite opposition from property owners, and was finally obtained two miles from the town and the surgeon general ordered the erection of a tent hospital. By March 1864 Alton had only five patients with smallpox, and these were all convalescent.52
When a contagious disease appeared at a prison, the threat of its spread was not always limited to the immediate vicinity. Apparently unaffected prisoners were sometimes moved from a fort where smallpox had appeared to another or sent south for exchange. If they fell ill in transit with this highly contagious disease, they endangered the populations of the areas through which they moved as well as those at their destinations. In October 1863 the appearance of smallpox in prisoners moving toward City Point from Fort Delaware caused so much anxiety that delaying future exchanges from the fort seemed advisable. The disease at Fort Delaware apparently arrived with a prisoner from Camp Chase. Although no surgeon would permit a man obviously suffering from smallpox to travel, men known to be suffering from chronic diarrhea did make the journey south for exchange. Some had to be hospitalized along the route, and others died.53
As the end of the war drew nearer, the challenge to prison physicians grew. New prisoners poured in, especially to facilities in the more southern locations. The population at Ship Island in the Mississippi River was 4,000 in April, and during the same month that at Point Lookout, between the Potomac River and the Chesapeake Bay, rose from less than 8,000 to almost 12,000. The sick and dead at Point Lookout were particularly numerous-203 died in April, when more than 1,700 were sick. By May, when nearly 1,600 left Point Lookout, prisoners were heading home in great numbers. Sick rates remained high at Point Lookout, however, where another 1,800 were ill during May. Almost all detainees at Ship Island left before June, and prisoners departed from other camps so rapidly that by the end of the month relatively few remained except for those too sick or too weak to be moved.54
Men in blue or gray were not the only patients for whom Medical Department physicians were responsible during 1865. The chief elected officers of both Union and Confederacy, the one an assassin`s victim, the other a defeated, harrassed, and ailing prisoner at Fort Monroe, received medical care at the hands of Army surgeons. The first doctor to come to the aid of Abraham Lincoln in his box at Ford`s Theater on 14 April 1865 was 23-year-old Charles Leale, assistant surgeon of the volunteers. It was Leale, an ardent Lincoln admirer who apparently came to the theater that night only because he knew the President would be there, who determined the nature of Lincoln`s wound. Leale directed the efforts of two other physicians, one an Army contract surgeon, Charles Taft. Taft joined him in the President`s box, attempting to revive the victim by pumping his arms up and down, clearing his throat, and blowing into his mouth. The physicians repeatedly removed the clot that clogged the
52MSH 1, pt. 3:50-51, 61-62, 67; WOR, ser. 2, 6:96-97, 104-05, 157, 160, 179, 476, 1123, and 7:535.
53WOR, ser. 2, 6:96, 422, 477 and 8:231.
54WOR, ser. 2, 8:173, 259, 480, 482, 493, 1001-02.
272
HOSPITAL AND PRISONER OF WAR DEPOT at Point Lookout, Maryland. (Courtesy of Library of Congress.)
{kind=link}
wound, after having noticed that their patient`s breathing and heartrate improved when they did so. Although they were certain almost from the outset that the injury would prove fatal, one of the physicians administered a few drops of brandy. They ordered that a room nearby be procured where the President`s last hours could be spent and helped carry Lincoln to a nearby house. Leale then sent for his patient`s regular physician and for Surgeon General Barnes. Until Barnes and Surgeon Charles Henry Crane, who would be Barnes` successor as surgeon general in 1882, arrived a short while later, Leale continued to direct the patient`s care, which included the application of mustard plasters the length of his body. Barnes probed the wound deeply and repeatedly without encountering the bullet, and agreed with the other physicians gathered around the bedside that Lincoln could not survive his injury. Crane and Taft alternated holding Lincoln`s head as they waited, and Leale was holding his patient`s hand when Barnes pronounced him dead shortly after seven in the morning of 15 April.55
The physicians responsible for the health of Jefferson Davis after his capture were also military surgeons. When Davis first arrived at Fort Monroe on 19 May, John J. Craven, surgeon of the volunteers, reported on his health. By the time Surgeon George Cooper, former medical director for the Army of the Cumberland, assumed the
55Jim Bishop, The Day Lincoln Was Shot (New York: Bantam Books, Bantam Pathfinders, 1955), pp.208-14, 230, 256, 263-64;Charles Sabin Taft, Notes on Abraham Lincoln, Ms C 108, NLM; MSH2, pt. 1:305-06.
273
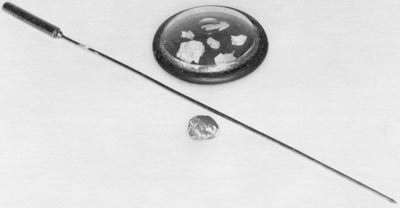
PROBE AND BULLET FRAGMENTS FROM LINCOLN`S BRAIN. (Courtesy of Armed Forces Institute of Pathology.)
{kind=link}
responsibilities initially handled by Craven, Davis` health or lack of it was beginning to become a cause of controversy. During the two years he remained a prisoner, the former president of the Confederacy suffered from a variety of conditions, including neuralgia, boils, erysipelas, "dyspeptic symptoms," and "severe hemorrhoids." Cooper`s concern for his patient`s health and the effect of imprisonment upon it led the officer in charge of the prison to accuse the surgeon of being "entirely under the influence of Mr. and Mrs. Davis" and to refer disparagingly to Mrs. Cooper`s Southern connections. In making this last comment, the commandant may not have realized that Surgeon General Barnes himself, despite his birth in Philadelphia and education in New England, also had ties with the Confederacy, for his brother had worked actively for the Southern cause.56
Conclusion
In mid-1865, only Davis and a relatively few seriously ill soldiers and prisoners of war still remained to remind Medical Department surgeons of the great conflict that
56WOR, ser. 1, 52:171 and ser. 2, 8:56,558, 571, 577, 711, 720, 740, 754-55, 775, 846, 871, 875, 883, 919, first, second, and third quotes from 8:846, 919, and 976, respectively; James M. Phalen, Chiefs, p. 47.
274
had just ended. Surgeon General Barnes was occupied principally in preparing his organization for a return to peacetime status. The quiet was welcome after the tumultuous last months of the war. Returning prisoners in fragile health had poured in. Grant`s army in its final drive had moved so rapidly that the countryside between Petersburg and Appomattox had been strewn with wounded, Union and Confederate. Sherman had once again covered great distances with a minimum of medical supplies. Ambulances had been in short supply and many vehicles in poor repair. Although prisons were not managed with the health of their occupants as the main consideration, nor campaigns planned with the care of the wounded as the prime concern, the Medical Department had functioned as effectively in prisons as it had in the field under conditions it could not control. But now the war was over; it continued to exist only in the memory of survivors and in an enormous volume of records that would as the years went by be compiled, published, and studied, so that from this hideous conflict, something worthwhile might still emerge.57
57SGO, Annual Report, 1865, p. 6; MSH1, app.:205; Brown, Medical Department, pp. 244-45.
![]()