



Books and Documents > The Army Medical Department 1818-1865
CHAPTER 13
Achievements and Failures During the Civil War
The Medical Department had intended that its detailed and copious records concerning the Union`s sick and wounded guarantee the emergence of something of value to medical science as well as to the Army from the most frightful conflict that the nation had ever faced. During the struggle and the months immediately following it, more than 12,000 medical officers- regulars, volunteers, and contract- examined over 250,000 wounds and treated more than 7 million cases of disease. In the course of their duties, more than300 Army surgeons died from wounds, disease, or accidents.1
In spite of their heavy case loads, many were able to record what they saw for posterity. The value of their observations, however, was to some degree negated by the fact that they, like their civilian counterparts, knew little of bacteria and the methods by which one microscopic creature could be clearly distinguished from another. Furthermore, the heavy demands placed on Army surgeons left little time for the careful consideration of the significance of what they saw. As a result, their observations were haphazard and often of little value. Since surgery was usually performed in great haste and under difficult circumstances, there was also little time available for trying new or intricate techniques. The frightening mortality that resulted from infection obscured the possible achievements of new approaches to surgery. The most important progress made by the Medical Department during the Civil War involved practical matters of organization and administration and resulted in the creation of an effective and efficient medical department for the large and active Union Army.2
Disease
In the nineteenth century, disease exacted a heavy toll when large groups of men were gathered closely together under conditions of stress and poor sanitation. In the Civil War, it killed twice as many men as battle. The conflict thus provided millions of cases of various diseases for study, but Union surgeons, like their counterparts everywhere, were still unable to distinguish harmless organisms from those causing disease-the developments that would make this possible were yet to come.3
1Brown, Medical Department, pp. 245-46; MSH 2, pt. 3:1, 3-4, 910.
2MSH 2, pt. 3:1, 3-4,910; Phyllis Allen, "Etiological Theory in America Prior to the Civil War," Journal of the History of Medicine and Allied Sciences 2 (1947):514.
3MSH 1, pt. 3: 1; Bayne-Jones, Preventive Medicine, p. 99.
276
The book devoted by the editors of the Medical and Surgical History of the War of the Rebellion exclusively to the greatest scourge of nineteenth century armies, dysentery, illustrates both the intensity with which the Medical Department conducted its attempts to learn more about this problem and the reasons why these efforts were unavailing. More than 1.6 million cases of diarrhea and dysentery were diagnosed in the Union Army, and an average of 14.31 per 1,000 mean strength died from it. A Union medical officer found "the prevalence of diarrhea as among the rebel prisoners ... absolutely astonishing." But the gradual realization that living organisms might be causing this and other major problems would gain impetus only after the Civil War. Lacking the staining and culturing techniques available a few decades later, physicians were also unable to compile records that would enable the modern scientist to identify positively the organisms responsible for the Union Army`s epidemics of dysentery. It seems probable that Entamoeba histolytica, Shigella, Giardia, Salmonella, and Campylobacter were afflicting the soldiers of 1861-1865. Nevertheless, fourteen years after the end of the war, Joseph Janvier Woodward, editor of the volume on dysentery and since 1864 a pioneer in the art of staining specimens, was still skeptical about the possibility that minuscule forms of life could be causing diarrhea and dysentery. He, like others of his contemporaries, refused to take seriously an 1876 publication maintaining that an ameba might be capable of causing this disease.4
Since they did not know what was really causing diarrhea and dysentery, medical officers had little chance of devising a cure. Shrewd observation based on trial and error was the only hope for progress, but they were also handicapped by their apparent assumption that dysentery was a single disease. Although occasional success was reported with the use of ipecacuanha, which is effective against amebiasis, when trials at a Washington hospital proved disappointing, this drug was rarely used. Among other medicines used to treat diarrhea, opium was often mistrusted, especially after medical officers began to realize it was only a palliative and not a cure. Bismuth subnitrate, also somewhat effective in easing the symptoms of dysentery, was used with caution because the presence of arsenic as an impurity was "exceedingly common." Strychnine, oil of turpentine, and cathartics, including mercurials and castor oil, were among other remedies tried without success. A few surgeons used lead acetate, but the very genuine risk of lead poisoning made many others reluctant to try it. Since malaria could cause diarrhea, quinine was "extensively employed," and "with a liberal hand." Although they had little control over the purity of the water the men drank in the field, doctors took great care to ensure the purity of the water their dysentery patients consumed, preferring rainwater, distilled water, or boiled water, or, as a last resort, the addition of a little claret to whatever was available. Their efforts to treat dysentery and diarrhea were to no avail, however. Although only 1 in 178 dysentery patients died in the first year of the war,
4Quote from "Chronic Diarrhea at Camp Douglass," Boston Medical and Surgical Journal 67 (1863):266; MSH 1, pt. 2; USSC, Sanitary Memoirs, p. 291; Henry, Armed Forces Institute, pp. 34-36; Joseph Janvier Woodward, "On the Use of Aniline in Histological Researches. . . "American Journal of the Medical Sciences 49 (1865):106-13. Unless otherwise indicated, all material on dysentery and diarrhea in the Union Army is based on MSH1, pt. 2. Campylobacter has only recently been identified as a cause of dysentery: Jack E. Welsh and R. Clark Gillett, telephone conversation with author.
277
by June 1865, when long campaigns, disease, and deprivation had weakened many soldiers, 1 in 29 was failing to survive.5
The most effective steps taken against the diarrheal diseases involved sanitation. Without knowing precisely why, military experts had long realized that filth, especially when large numbers of men were grouped together, was associated with disease. But in an army composed largely of amateurs, enforcing strict standards of sanitation and hygiene posed great problems. When many were afflicted with diarrhea, these problems became even more urgent, both in hospitals and in camps. Officers often ignored regulations requiring the digging of sinks for every camp. Men ignored trenches that were dug for this purpose, which were "often so badly managed that it was disgusting to use them." When drinking water came from shallow wells, pollution was inevitable, and typhoid as well as diarrhea and dysentery resulted. The need for improved camp sanitation inspired sanitary commissions from the beginning of hostilities, and with time, and perhaps as the men themselves began to understand the importance of sanitation, the number of diarrheal cases per 1,000 men began to drop, from 770 in the year ending June 1862 to 686 three years later, and this despite the rising death rate.6
Unlike dysentery, malaria no longer formed a serious threat to the Union Army as long as adequate supplies of quinine could be obtained. Wishing to reduce the amount of even temporary disability caused by malaria, Union surgeons continued to experiment with the prophylactic use of quinine, mixing the dose with whiskey to increase its attractions. It was not always possible, however, to obtain enough of both ingredients, and even when several times the normal dose of three to eight grains was administered daily, fever paroxysms might still occur. The disease was reported to return with even greater severity if the prophylactic doses were stopped once started, and prophylactic quinine never became routine.7
The Medical Department`s interest in malaria extended to the question of the relative susceptibility of blacks and whites. Perhaps on the assumption that blacks were less likely to be disabled by this disease, the Army tended to send black regiments to areas with higher malaria rates. Although department statistics suggested that blacks contracted and died from malaria more frequently than whites, Charles Smart, editor of part three of the Medical
5MSH 1, pt. 2, first quote from p. 793,remaining quotes from p. 800; Woodward, Outlines, pp. 216-17, 222,229; Charles Beneulyn Johnson, Muskets and Medicine, or Army Life in the Sixties (Philadelphia: F. A. Davis Co., 1917), p. 162; "Subnitrate of Bismuth . . . " American Journal of the Medical Sciences 44 (1862):213-32; USSC, Surgical Memoirs 1:304-05; Thomas T. Smiley, "Medical and Surgical Cases at Port Royal, S.C.," Boston Medical and Surgical Journal 67 (1863):271
6Quote from MSH 1, pt. 2:617; Woodward, Outlines, p.50; Maxwell, Sanitary Commission, pp. 33-34, 38; Steiner, Disease, p. 26; Reed, Hospital Life, p. 68; Howard D. Kramer, "Effect of the Civil War on the Public Health Movement," Mississippi Valley Historical Review 35 (1948):46 1; USSC, Documents 1, no. 1:7,11 and no. 5:7 and no. 46:41-42; William A. Hammond, A Treatise on Hygiene With Special Reference to the Military Service (Philadelphia: J. B. Lippincott Co., 1863), p. vii.
7MSH 1, pt. 3:77-78, 154, 167, 170-71, 180; Bispham, Malaria, p. 136; Ltr, Moore to SG (4 Aug 1863), RG 112, entry 12;William H. Van Buren, "Quinine as a Prophylactic Against Malarial Disease," Military Medical and Surgical Essays Prepared for the U.S. Sanitary Commission, ed. W. A. Hammond (Philadelphia: J. B. Lippincott Co., 1864), pp. 96-97; "Quinine as a Prophylactic, American Medical Times 3 (1861):262; USSC, Documents 1, no. 8:248; USSC, Surgical Memoirs 1:135-36. It might be noted that during World War II, the Medical Department found daily doses of 0.3 g (4.6 gr.) of quinine relatively ineffective in preventing vivax malaria in both New Guinea and West Africa: Havens, Jr., Infectious Diseases, p. 532.
278
volume of the Medical and Surgical History, blamed this situation on the greater exposure of blacks to the disease. The death rate for blacks with malaria was twice that of whites suffering from that disease, but he remained convinced that blacks had a lesser susceptibility to malaria than whites, a belief that modern research has to some extent confirmed.8
Typhoid was yet another disease about which medical officers discovered little that was new during the Civil War, despite devastating epidemics. Although many soldiers coming from the North were exposed to both typhoid and malaria at essentially the same time, the announcement that the resultant collection of symptoms constituted typhomalarial fever merely added to the confusion. Medical officers, though aware of the connection between poor sanitation and typhoid, remained as much mystified by the disease in 1865 as in 1861. The data collected in the Medical and Surgical History did, however, help Army physicians after the war to realize that water was indeed one source of typhoid infections.9
Smallpox was no longer the formidable threat it had been during the American Revolution, but medical officers still had to treat many cases, since an average of 5.5 per 1,000 mean strength among whites and 36.6 among blacks contracted the disease. It was not always possible to immunize immediately the thousands of volunteer troops who came pouring in, and doctors were already aware that periodic revaccination was necessary if the spread of smallpox was to be prevented. Surgeons learned that possible complications made it advisable, however, not to immunize those suffering from scurvy. They also discovered that vaccine could be safely preserved and shipped in narrow glass tubes, three inches or less in length, for each dose so stored. Because of the efforts of the Medical Department, during the autumn of 1863 and the winter of 1864 more people were vaccinated than had ever been immunized before in a comparable period of time.10
The inroads of other diseases, including the very prevalent respiratory infections that also afflicted Union soldiers, were relatively easy to appreciate, but the effects of a deficient diet were not. Medical officers, helpless to solve the transportation problems that led to the deficiency, were well aware that the standard ration of the soldier in the field was likely to lead to scurvy, although they were not aware that the soldier who refused to eat desiccated vegetables was also in danger of suffering from a lack of vitamin A. Surgeons usually recognized cases of scurvy at its worst, but the less obvious effects of subclinical scurvy were hard to pinpoint. As a result, one can only conjecture about precisely how much the vigor and effectiveness of troops in the field were affected by the depression and lethargy that accompanied the earliest stages of a vitamin C deficiency, since they could have resulted from or been reinforced by other health problems as well. It is difficult, too, to estimate to what extent a deficient diet, sometimes low in protein and calorie content as well as in vitamins, contributed to the prolongation of other ills, to the failure of injuries to heal, and to devastation wrought by
8Bispham, Malaria, pp. 34,119; MSH1, pt. 3:12-13, 80, 85, 89, 92, 107, 109, 110-11.
9MSH 1, pt. 3:372-73, 375, 494; Kenneth F. Maxcy, Preventive Medicine and Public Health, 8th ed. (New York: Appleton-Century-Crofts,1956), pp. 180-81.
10MSH 1, pt. 3:625-27, 635, 638; F. G. Smith and Alfred Stille, "Vaccination in Armies," Military Medical and Surgical Essays, ed. W. A. Hammond, pp. 148-49, 151-52; USSC, Surgical Memoirs1:137-38, 142-50, 162-63, 165; USSC, Documents, no. 9:15, 25.
279
open wound infections. A Sanitary Com-mission official familiar with the problems caused by scurvy commented, however, that "The pecuniary loss to the nation, by badly regulated and insufficient army ration, constitutes one of the great burdens of taxation now pressing upon the people."11
Although the Army did what it could to treat the sick, many soldiers returned to their homes and to civilian life with their health permanently impaired by chronic disease. Usually the lingering illness involved diarrhea that, even when inactive, hung like the sword of Damocles over the veteran`s head, likely to fall when his body was overstressed. Many deaths from dysentery acquired during the war occurred in peacetime in soldiers whose health declined slowly even after they returned to their families. Veterans suffering from malaria acquired when they were far from their northern homes became a potential source of infection for local Anopheles mosquitoes. A study of former soldiers in Massachusetts made in the 1890s showed that they also suffered from such diseases as tuberculosis and rheumatism at a rate far greater than that of the general population of that state. The rate of diarrhea and dysentery among veterans was almost fifty-six times that among the rest of the population, that of rheumatism five times, that of heart and circulatory problems six times (possibly as a legacy of streptococcal infections), and that of consumption twice. There was no indication, however, whether returning soldiers spread dysentery and diarrhea among those who had remained at home.12
Except for offering supportive care, doctors could do little during the Civil War to help those stricken with diseases other than malaria. Except for improved sanitation, they could do little to prevent diseases other than smallpox, but their renewed appreciation for sanitation undoubtedly contributed to a marked drop in the disease rate in the postwar Army as compared with the prewar force. Despite voluminous records, medical officers made no significant progress during the Civil War toward finding ways in which to prevent or cure the diseases that ravaged the Union Army.13
Infection and Wounds
Although aware that scurvy or even a scorbutic taint delayed healing, medical officers were ignorant of how infections spread from wound to wound. As a result, they were initially unable - to combat the horrors of what now appear often to have been streptococcal infections. These bacteria spread through hospital wards, turning even small wounds into gaping, oozing pits of hospital gangrene, poisoning the bloodstream, and spreading the rash of erysipelas among wounded and unwounded alike. On the basis of the many cases they saw during the war, some surgeons did begin to suspect that these infections as well as scarlet fever, rheumatism, and some forms of heart disease might all be related,
11USSC, Surgical Memoirs 1:51, 88, 274,276, 278, quote from 278; USSC, Documents 1, no. 17:11-12; MSH1, pt. 3:68-70, 684, 705-07, 713. Desiccated vegetables were prepared by cleaning and slicing, drying in hot air, pressing, and then sealing in cans, a process likely to destroy vitamin C: E. N. Horsford, The Army Ration, 2d ed., rev. (New York: D. Van Nostrand, 1864), p. 11.
12MSH 1, pt. 2:651 and pt. 3:77-78, 82; Johnson, Muskets and Medicine, p. 170; John S. Billings, "The Health of the Survivors of the War," Forum, Jan 1892, p. 656.
13Kramer, "Effect of the Civil War," p. 456, 462; Steiner, Disease, p. 5.
280
but they blamed them on miasmas or the poisons produced by decaying flesh.14
Medical officers could not afford to take these infections lightly. Some had a very high mortality; of 2,812 cases diagnosed as pyemia, a systemic infection, 2,747 were fatal. Surgeons recorded surprisingly few cases of tetanus, but much gangrene, which killed 45 percent of its victims and necessitated surgery that would not otherwise have been performed. Of the wounded afflicted with erysipelas with its spreading areas of swollen, empurpled skin, 41 percent died. Surgeons observed once again that patients in tent hospitals suffered less from infection than those housed indoors and that good ventilation reduced the infection rate. Although some theorized that erysipelas spread through the blood, many were convinced that it moved through the air, noting that it seemed to spread in the direction the wind was blowing. Case histories revealed patients who suffered first from one form of infection, then another, gangrenous wounds that healed only to be followed by erysipelas and then even pyemia.15
Hospital gangrene, probably caused by Streptococcus pyogenes, had such a rapid and horrible effect on wounds that it inspired both dread and strong efforts to find a cure. The skin around gangrenous wounds sloughed off, revealing flesh that slowly turned "reddish, greenish, purplish, or black," while the gray edges of the opening grew wider at the rate of half an inch an hour. Arteries and even bones were rapidly exposed and the stench of rotten meat filled the air. As his skin turned gray the patient`s breath became sickly sweet, his body alternated between chills and sweats, and his pulse grew ever faster, ever feebler. So great was the fear of the spread of this infection that in several areas medical officers established special facilities to isolate its victims.16
Gas gangrene was not the infection that caused so much alarm in the military hospitals of the Civil War. Civil War records reveal that one of the most terrifying aspects of hospital gangrene was the rapidity with which it spread from patient to patient, but gas gangrene is not contagious. The presence of a clostridial infection cannot be ruled out, however, especially since the occasional mention of a sweetish odor from the wounds strongly suggests its presence. We know, however, that less than a third of all wounds become infected with clostridia, and only 5 percent of these actually develop gas gangrene. Gas gangrene, moreover, tends to appear in deep wounds, especially when damage to major blood vessels has reduced the oxygen supply to the muscles, a type of injury that during the Civil War usually led to relatively prompt amputation before gas gangrene
14USSC, Surgical Memoirs 1:274; C. H. Cleaveland, "Hospital Gangrene in the U.S. Military Hospital at Memphis, Tenn.," Chicago Medical Journal 21 (1864):15-16; M. Goldsmith, A Report on Hospital Gangrene, Erysipelas and Pyaemia, as Observed in the Departments of the Ohio and the Cumberland, With Cases Appended(Louisville: Bradley & Gilbert, 1863), pp. 7-8 n. 7-8, pp. 14-15, 20-21;E. Andrews, "Diathesis: Their Surgical Relations and Effects, "Transactions of the American Medical Association 14 (1863):125;Alfred North, "Report of Sixty Cases of Hospital Gangrene," American Medical Times 6 (1863):258.
15MSH 1, pt. 3:663, 673; 854; MSH 2, pt. 3:32,34, 37, 818; Goldsmith, Gangrene, pp. 13-14; Keen, "Reminiscences," pp. 104-05; Mitchell, "Medical Department," p. 1446; Frank Hastings Hamilton, ed., Surgical Memoirs of the War of the Rebellion, 2 vols.(New York: Hurd & Houghton, 1870),1:509-10; William Thomson, "Report of Cases of Hospital Gangrene," Chicago Medical Examiner 5(1864):675, 689-90; Stewart Brooks, Civil War Medicine (Springfield, Ill.: Charles C Thomas, 1966), p. 83.
16Quote from Cleaveland, "Gangrene," p. 5; MSH2, pt. 3:823, 825-30, 843; Brinton, Memoirs, pp. 225-26; Hamilton, Treatise, pp. 570-71, 573; Wangensteen and Wangensteen, Rise of Surgery, pp. 63, 394; Goldsmith, Gangrene, pp. 25, 27.
281
HOSPITAL GANGRENE as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
could develop in the wound. Hospital gangrene, on the other hand, actually caused a higher death rate when it originated in flesh wounds than it did in wounds accompanied by fractures.17
The horror of hospital gangrene inspired urgent efforts during the Civil War to find both a preventive and a cure. Among the remedies used, the halogens- iodine, chlorine, and bromine-proved to be more useful against hospital gangrene than nitric acid, which was also tried but with less widespread enthusiasm. Apparently finding bromine the easiest to use, surgeons began applying it to wounds and the rash of erysipelas, vaporizing it to disinfect the air,
17MSH 2, pt. 3:31, 824; Wesley W. Spink, Infectious Diseases: Prevention and Treatment in the Nineteenth and Twentieth Centuries (Minneapolis: University of Minnesota Press, 1978),pp. 302-03; James F. Coupal, "Pathology of Gas Gangrene Following War Wounds," sec. 2 in Pathology of the Acute Respiratory Diseases, and of Gas Gangrene Following War Wounds, vol. 12 of The Medical Department of the United States Army in the World War (Washington: Government Printing Office, 1929), pp. 412-14, 419; Rene J. Dubos and James G. Hirsh, Bacterial and Mycotic Infections of Man, 4th ed. (Philadelphia: J. B. Lippincott Co., 1965), pp. 553, 555; Wintrobe et al., Harrison`s Principles, pp. 783, 852-53.
282
HOSPITAL GANGRENE as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
and mixing it with glycerine for internal use, not thinking, however, to use it to sterilize instruments. One successful technique involved inserting bromine on wooden sticks into diseased tissue; another called for injecting bromine by hypodermic into healthy tissue bordering the infected area. These procedures could cause so much pain as to require the use of anesthesia. Used in adequate strength and quantity, bromine prevented the spread of gangrene both in the individual patient and among patients. Although some surgeons using bromine reported that deaths from hospital gangrene had been entirely eliminated, others remained skeptical and apparently regarded the approach as something of a fad.18
Attempts to find the cause of hospital gangrene and other infections met with less success than efforts to find a cure. Microscopic studies revealed an elevated white blood cell count in the victims of hospital gangrene, but beyond that "only the ordinary bacteria which are to be observed in every decomposing animal substance." This last comment, although strange to modern ears, was the natural result of ignorance about the range and variety of disease-causing organisms and the absence of stains and other techniques that would emphasize the characteristics of cells seen under the microscope.19
The injuries that were the sites of such grim infections usually resulted not from bayonet or saber but from the slow-moving minie ball, which shattered bone and crushed soft tissues, carrying into the body bacteria-laden bits of clothing and other debris. A few minie balls were actually explosive and, while shattering bone still further, embedded bits of copper, lead, and pewter in the shredded flesh. Many victims bled to death on the battlefield. Even without infection, the fractures caused by the minie ball would challenge a twentieth century orthopedist. When streptococci filled the wound and spread ever more widely beyond the injury, even amputation often failed to save the victim. Thus the death
18Wangensteen and Wangensteen, Rise of Surgery, pp. 318-20, 323-25, 507; John Brinton, "Bromide in Hospital Gangrene, "American Medical Times 6 (1863):250; MSH 2, pt. 3:837, 845;Goldsmith, Gangrene, pp. 29, 31, 32, 35, 81-84; Cleaveland, "Gangrene," pp. 6-7, 10; Mitchell, "Medical Department," pp. 1446; Thomson, "Gangrene" 5:676, 677-78, 692; North, "Gangrene" 6:255;Roberts Bartholow, The Principles and Practice of Disinfection (Cincinnati: R. W. Carroll & Co., 1867), pp. 44-47.
19MSH 2, pt. 3:827, 832, 848-49, 862-65, quote from p.832; Wangensteen and Wangensteen, Rise of Surgery, pp. 508-09; Reed, Hospital Life, pp. 35-36; Keen, "Reminiscences," pp. 103-04;Willis G. Diffenbaugh, "Military Surgery in the Civil War," Military Medicine 130 (1965):491.
283
rate was high. Sixty-two percent of those with chest wounds died, as did more than 87 percent with abdominal wounds, usually within two days of the moment when the bacteria-filled contents of the injured intestines spilled into the peritoneal cavity. Few surgeons would open the abdomen unless fecal material was actually oozing from the wound. Of the 253,142 wounds recorded in the Surgeon General`s Office, however, most involved the extremities, more than 35 percent the legs and feet, and another 33percent the arms and hands.20
Confronted with so many injuries and imbued with the pragmatism characteristic of their profession, surgeons tried to test the effectiveness of both old methods and newly proposed approaches. One area of experimentation involved the hermetic sealing of chest wounds. Although this procedure gave instant relief for breathing difficulties and bleeding, it also eliminated the possibility of external drainage and thus provided no improvement in the management of infection. Many surgeons vigorously opposed its use. Another area of relatively intense study involved nerve injuries. Medical officers tried various forms of stimulation upon paralyzed patients, including electrical currents and alternating applications of cold and heat. Although 55.5 percent of those with spinal injuries died of their wounds, in at least one instance doctors were able to keep a "nearly complete paraplegic" whose bladder could be emptied only by catheter alive for at least seventeenyears.21
So great was Surgeon General Hammond`s interest in nerve injuries that he turned an entire hospital over to S. Weir Mitchell, a pioneering neurologist, for the exclusive use of patients with nerve injuries and nervous diseases. Here Mitchell, George R. Morehouse, and William W. Keen, Jr., studied the victims of phantom limb and nerve damage, epileptics, malingerers, and shell-shock victims (although "shell shock" is a term of more recent origin), men whose ills were psychological in origin and who usually received little attention from physicians. In one year alone Mitchell used 40,000 injections of morphine in his attempts to relieve the torments of his patients. He experimented also with hypodermic injections of atropine to ease muscle spasms. In this facility he took thousands of pages of notes in preparation for later publication.22
Since such a large proportion of wounds involved the extremities, much of the data collected on wartime surgery dealt with amputation, excision(the removal of a major portion of bone), and attempts to preserve bone essentially intact. Surgeons
20MSH 2, pt. 2:434 and pt. 3:2, 685,702, 723; John Hill Brinton, "Address: Closing Exercises of the Session 1895-96, Army Medical School," Journal of the American Medical Association 26 (1896):603; Duinell Medical Report; Frank H. Hamilton, "Lecture on Gunshot Wounds of the Abdomen," American Medical Times 8 (1864):230; Johnson, Muskets and Medicine, pp. 131-32;"Scenes in Hospitals," Sanitary Reporter 1 (1863):162;"Military Medicine," MD 12, no. 6 (1968):130; Keen, "Reminiscences," p. 107; Robert L. Reid, "The British Crimean Medical Disaster- Ineptnessor Inevitability," Military Medicine 140 (1975):425; Dean Thomas, "The Gardiner Explosive Shell," North South Trader 2 (Jul-Aug 1976):23-24; Robert Reyburn, Fifty Years in the Practice of Medicine and Surgery, 1856 to 1906 (n.p., 1907), p. 9; Diffenbaugh, "Military Surgery," p. 492.
21MSH 2, pt. 1:424, 452, 497-98, 500n, 509-11, 618, 634, and pt. 1, app.:200, and pt. 3:725, 727-28, quote from 3:727.
22 Anna Robeson Burr, Weir Mitchell: His Life and Letters(New York: Duffield & Co., 1929), pp. 104-06, 122; Mitchell, "Recollections," pp. 91-93; Ernest Earnest, S. Weir Mitchell: Novelist and Physician(Philadelphia: University of Pennsylvania Press, 1950), p. 52; S. Weir Mitchell, George R. Morehouse, and W. W. Keen, Jr., Reflex Paralysis, Cir no. 6 (SGO, 10 Mar 1864; New Haven, Conn.: Yale University School of Medicine, 1941), pp. iii-vi; S. Weir Mitchell, Injuries of Nerves and Their Consequences (New York: Dover Publications, 1965), pp. v, xviii-xix.
284
seeking to preserve a limb tried many devices to immobilize it, but apparently distrusted casts, fearing impaired circulation. Sandbags and elongated box splints limited motion during transportation, and several different kinds of splint were used in the hospital, including one designed by an Army surgeon. In cases where the femur, or thigh bone, was fractured, extension or traction devices were rarely used. Such treatment might prevent solid contact between the broken ends and thus inhibit or preclude healing, but without it, a leg tended to mend inches shorter than it had been and at times could be badly deformed as well. Other complications included abscesses and sinuses or abnormal channels that lasted for years and drained the patient`s strength, and splinters of shattered bone left in the wound that continued to work their way to the surface, adding to the patient`s lingering anguish. Some of the wounded thus died after years of suffering and slow decline. Medical officers attributed most deaths in those whose limbs they had tried to save to pyemia or other forms of systemic infection.23
21MSH 2, pt. 2:811, 814, 841, and pt.3:179-83, 190, 193, 198, 346n, 350, 428-29, 568; "The Week," American Medical Times 4 (1861):268; Tripler and Blackburn, Handbook, p. 56.
285
Since the treatment to be accorded fracture cases was chosen on the basis of the patient`s condition rather than at random, the death rates do not necessarily reflect the merits of the various forms of treatment. Although there was much disagreement on the value of a conservative approach to the management of shot fractures, the mortality of patients chosen for conservative treatment proved less than that of those treated with excision or amputation. In a series of 386 men with shot fractures of the hip, for example, 249 of 304, or 82 percent, treated conservatively died, but 53 of 55, or 96 percent, undergoing excision failed to survive, and 25 of 27, or almost 93 percent, enduring amputation died. Of 2,369 victims of shot fractures of the shoulder, only 25.1 percent treated conservatively died, while 36.6 percent of excision patients died, as did 29.1 percent of the amputees.24
WILLIAM W. KEEN. (Courtesy of National Library of Medicine.)
{kind=link}
The chief value of excision, with its high death rate, lay in the fact that it could preserve some function of the arm and, when the periosteum(the bone-forming connective tissue covering all bones) was preserved, doctors could hope for some bone regeneration. One surgeon maintained that he had seen the entire shaft of the tibia (the principal bone of the lower leg) regenerated. Even without regeneration, however, an arm could be surprisingly useful despite the removal of a large amount of bone, and doctors regarded any function as better than none. Such removal might mean, however, that the limb would dangle loosely from the shoulder. Unfortunately, time might cause such an arm to deteriorate and to swell because it was dangling unsupported. In one such case, although Army doctors considered the result to be satisfactory, a pension examiner recommended amputation in 1867. Excision became less popular as the war went on- the chances for infection were great, the period of healing was long, and the results, except in the instances when the usefulness of a hand was retained, were questionable, if not actually disastrous. The death rate, furthermore, was comparable to or greater than that in amputations, with pyemia the chief danger and hemorrhage a significantproblem.25
Although occasional reports of excessive enthusiasm for amputations did surface during the Civil War, this form of surgery
24MSH 1, pt. 1, app.:311; MSH2, pt. 2:660 and pt. 3:65; Hamilton, Treatise, pp. 13-14; WOR, ser. 1, 38, pt. 2:526.
25MSH 2, pt. 2:518, 548, 563, 611-12, 670, 966, 992 and pt. 3:874-76; USSC, Papers 1:5-7; "Conservative Surgery, "American Medical Times 3 (1861):295.
286
was apparently often undertaken only after careful consideration of the alternatives. Excision was generally viewed as the least desirable choice, however, in cases where there was damage to the upper leg, and damage to a joint was often regarded as necessitating amputation. The records concerning the number of amputations performed are not complete, but the figure was at least 30,000. The most common amputation was that of the hand or fingers, while the highest fatality rate, of 83.3 percent, occurred after amputation at the hip joint. Surgeons discovered that amputation at the knee took a surprisingly high toll of 57.2 percent, and even amputation of the lower arm was followed by the deaths of 20.7 percent of those operated on. Considerable difference of opinion existed as to how the amputation was to be performed in any event, with many favoring a flap procedure that could be quickly done on the field and involved less danger from bleeding than the circular form of the operation. Some surgeons favored immediate operation, others a very brief wait until the first shock had worn off. The surgery itself was apparently a rapid procedure even though anesthesia was generally used. A hip amputation reportedly took two minutes, including the time needed to tie off the femoral artery.26
Some surgeons were still a little wary of anesthesia, however, and avoided its use when the patient`s condition was very poor. Few deaths were actually blamed on these agents, but surgeons noted the adverse effects on appetite and the nausea and vomiting that followed their use. Some continued to believe that anesthesia prevented quick healing and therefore led indirectly to increased rates of infection and hemorrhage. Nevertheless, by the time of the Civil War, most Army surgeons, even conservative Surgeon General Thomas Lawson, had accepted its use.27
Anesthetics were used in at least 80,000 cases during the Civil War. More than 76 percent of the time the agent used was chloroform, but ether was popular in general hospitals, and a combination of ether and chloroform was used in 9.1 percent of the cases. A failure to use any form of anesthesia was recorded only 254 times. The debate over which anesthetic to use centered around the difficulties and dangers involved. Deaths from chloroform averaged 5.4 per 1,000 cases, those from ether 3 per 1,000. Ether was flammable and particularly hazardous when operations were performed by candlelight, while chloroform caused some inexplicable deaths, although it was easy to take and even a small amount acted with considerable speed. Surgeons well aware of its dangers and its reputation still preferred to use this anesthetic, although they did so with care, attempting to limit the length of time it was administered and to ensure that an adequate amount of air was inhaled with it.28
An anesthetic, whether ether, chloroform, or a mixture of the two, was appar-
26MSH 2, pt. 2:746 and pt. 3:20,134,339-40, 411, 877, 879; Hamilton, Treatise, pp. 420-23, 426-28, 431,436; Charles H. Rawson, "Visit to the Hospital at Springfield, Mo., "American Medical Times 3 (1861):364.
27Hamilton, Treatise, pp. 612, 621-22; MSH 2,pt. 3:134-35; Ms C24, p. 26, NLM; G. W. H. Kemper, "The Surgeons of the Civil War," Journal of the Indiana Medical Association11 (1918):368; "Anesthetics in Military Surgery," American National Times 3 (1861):151; Gross, Manual, p. 81.
28MSH 1, pt. 1, app.:200; MSH 2, pt. 3:887-89;"Anesthetics," p. 151; Keen, Reminiscences, p. 109; William Williamson Wellington, "Modern Medicine: Its Need and Its Tendency, "Medical Communications of the Massachusetts Medical Society, ser.2, 11, no. 7 (1874):163; Jones, "Medical History," p. 188n; J. Mason Warren, "Recent Progress in Surgery," Medical Communications of the Massachusetts Medical Society, ser. 2, 10, no. 6 (1866):273.
287
ently usually administered by means of an impregnated cloth, which might have been rolled into a cone with an anesthetic-soaked sponge at its apex, held over the mouth and nose. Experience taught medical officers that in the open air where so many amputations were performed, merely pouring an anesthetic on a cloth was not effective. Premedication, if given, might take the form of a dose of whiskey. As a rule no ill effects resulted from the inhalation of an anesthetic. On occasion, however, a patient inhaling chloroform would begin to make convulsive movements, and the veins in his neck would start to swell. The physician would often note that his patient`s heart was either at the point of arrest or had already stopped beating. In such cases, respiration soon also ceased, and all the efforts of doctors and nurses were often to no avail. It was only in March 1865, however, that the surgeon general was sufficiently disturbed over the problem of anesthesia deaths to order his surgeons to report on their experiences with these agents.29
In addition to anesthetics, medical officers used analgesics, including both alcohol and opiates, in their battle against pain. Alcohol was used not only to relax a patient before the administration of anesthetics, but also to serve as a vehicle for quinine. Some physicians, including Letterman feared that this free use of alcohol could induce addiction or mask symptoms, but alcoholism did not become a significant problem during the Civil War. Authorities should perhaps have been more concerned about the possible overuse of opiates, since many cases of addiction after the war were blamed on the free prescribing of such drugs during the conflict. Opium itself had long been prescribed for diarrhea, but during the Civil War morphine was also dusted in wounds or administered by hypodermic. Occasional mention was also made during this period of the use of cannabis for patients with tetanus or head injuries.30
The hypodermic, apparently used chiefly to inject morphine, was one of a few new devices slowly gaining in popularity in the Army during the Civil War. It was regarded to some extent as experimental. Although the Medical Department did have clinical thermometers, they were not in common use, and the model available was very long, intended for use in the armpit. Such instruments as hemostatic forceps, retractors, and dilators were not available, and few doctors knew how to use an ophthalmoscope or laryngoscope. Microscopes were few and far between. Real progress, however, was being made in the design of artificial limbs, enabling crippled soldiers to walk with only a limp or, with the aid of gloves, to conduct their lives with few aware that they had lost a hand or an arm. A relatively new development was mobility in the ankle of an artificial leg. A device developed by one firm for patients with resections of the elbow or shoulder was so effective that it permitted a greater reliance on this form of surgery as opposed to am-
29Frederick E. Lente, "Sulphuric Ether as an Anesthetic in Military Surgery," American Medical Times4 (1862):365; MSH 2, pt. 3:888; 890-9 1, J. H. Thompson, "Report of the Wounded at the Battle of Newbern, N.C.," American Medical Times 5 (1862):6; Cir, SG (Cir no. 2, 15 Mar 1865), Ms C24, NLM.
30Woodward, Outlines, p. 170; Hall, Researches, p. 173; MSH 1, pt. 1, app.:232-33, and pt. 3:171, 890; MSH2, pt. 1:646 and pt. 3:818; A. W. Smith, Reminiscences, p. 129;R. N. Barr, "Army Diseases," Ohio Medical and Surgical Journal14 (1862):107-08; Letterman, Recollections, p. 183; USSC, Surgical Memoirs 1: 13; Brooks, Civil War Medicine, p. 103; "Blue Velvet: The New Look in Drug Addiction," The Sciences 4 (1964-65):8;Barry M. Parsinen and Karen Kerner, "The Development of the Disease Model of Drug Addiction in Britain, 1870-1926," Medical History24 (Jul 1980):275-77.
288
putation. Medical officers also developed considerable ingenuity in devising for those whose lower jaws had been torn away prostheses that limited drooling and made taking liquids possible. The actual selections of the firms to make prostheses and of the designs to be used was apparently significantly influenced by a committee of distinguished doctors appointed by Surgeon General Hammond. The soldier whose artificial limb was approved by the Medical Department could choose any limb costing $50 or less from one of several authorized manufacturers.31
The benefits to medical science arising from the Civil War are not easily established, but undoubtedly the civilian population profited from the presence of surgeons like S. Weir Mitchell and his colleagues who had received more training and experience during that conflict than they would otherwise have had in a lifetime. Although the records and specimens that would form the Medical and Surgical History, and the Army Medical Museum were of little help in improving the care of the sick or wounded during the struggle, both would be of value to future generations, just as would be the techniques in staining specimens for the microscope and in photomicrography pioneered in the museum late in the war.32
Organization and Administration
The effect of Civil War experiences on the size, organization, and administration of the Medical Department was more pronounced than the Civil War experiences` effect on medical science. A more effective use of the department`s newly huge medical staff was but one of its achievements. Great flexibility proved necessary to care for the enormous numbers of sick and wounded that poured in from battlefields and camps, both east and west. No ratio of surgeons to men that would be adequate under all circumstances could be efficiently established for a given unit. To deal with this situation, the Department departed from the Mexican War pattern to create positions for surgeons and assistant surgeons of the volunteers, who could be assigned as needed and whose qualifications were determined by the Medical Department. More than 500 of these physicians worked with a Regular Army staff numbering less than half that figure. Almost 6,000 regimental medical officers, whose qualifications were initially ascertained at the state level, also served at one time or another in the Union Army. An equivalent number of civilian doctors unwilling or unable to join the Army worked as contract surgeons, either for short periods when necessity dictated or in general hospitals in the cities where they lived. Although a few Army doctors, especially in the early months of the war, earned unenviable reputations, the Department was apparently
31MSH 1, pt. 3:965; MSH 2, pt.1:398; Ltrs, Brinton to Barnes (8 Dec 1864), RG 112, entry 12. Byrne to Reed and Barton (9 Apr 1863) and Edward S. Dunster to James W. Queen (10Jun 1863), both in RG 112, entry 2, 34:497 and 35:187, respectively; Keen, "Reminiscences," p. 109; W. W. Keen, "Military Surgery in1861 and in 1918," Annals of the American Academy of Political and Social Science 80 (1918):20; Charles R. Greenleaf, A Manual for the Medical Officers of the United States Army (Philadelphia: J.B. Lippincott Co., 1864), p. 25; A. W. Smith, Reminiscences, p.189; Samuel D. Gross, Autobiography of Samuel D. Gross, M.D., With Sketches by His Contemporaries, ed. by his sons, 1 (Philadelphia: George Barrie,1887):133-34; Andrews, Surgery, pp. 414-15; James M. Minor, "Report on Artificial Limbs," Bulletin of the New York Academy of Medicine1 (1860-62):177; Henry, Armed Forces Institute, p. 8.
32Henry, Armed Forces Institute, pp. 34-39; Anderson Hunter Dupree, Science in the Federal Government (Cambridge, Mass.: Belknap Press of Harvard University, 1957), p. 129.
289
able to gather a medical staff that was on the whole highly regarded. The new type of organization, where regular medical officers shared their responsibilities at all levels with a large volunteer staff, was needed more in war than in peace, but it blazed a trail that would not be forgotten.33
The war also served to emphasize the necessity for abandoning the customary haphazard approach to the problem of providing an adequate number of hospital attendants, nurses, clerks, and guards. Expecting to find a sufficient number of able and disciplined men and women to work in hospitals on short notice proved unreasonable. Complaints about the caliber of the nurses rounded up to care for military patients were numerous, yet by the end of the war, the problem remained only partially resolved. Line officers understandably resented having to leave healthy and competent men behind to care for the sick. As the war progressed and the number of invalids grew, the Invalid Corps significantly eased the staffing shortage, but few were available early in the war. Since these men had no training in the care of the sick, their usefulness was limited. Moreover, few women had any formal training in nursing, although their practical experience in caring for their families stood many in good stead. The obvious need for professional training of nurses influenced those responsible for staffing civilian hospitals after the war, not only to give nurses the expertise needed but also to separate the dedicated from the dilettante. Of the latter, many had found their way to the hospitals in the guise of nurses during the war.34
The Medical Department also introduced greater system into the management of field hospitals. Early in the war, surgeons started organizing these facilities principally on a division basis rather than a regimental one. Medical officers also established small stations near the battlefield and evacuation hospitals at rail depots or near wharves along waterways. Tents, marked as hospitals by yellow flags with green numerals, became an increasingly common sight in the field, since they offered many advantages over the buildings that might be available near a battlefield. They could be pitched in an hour by someone familiar with them, and although those designed for hospital use could accommodate only eight patients comfortably, their design permitted two or more to be joined to serve larger numbers of wounded. Smaller tents could be used to shelter medical officers and medical and kitchen supplies. Surgeons found that there was less infection among patients sheltered in tents, where in good weather the walls could be raised to achieve perfect ventilation. An experienced Army surgeon concluded, "One of the most valuable lessons taught by the experience of the American War of 1861-65 was the demonstration of the inestimable value of the tent as a hospital.35
Unlike field hospitals, base or general hospitals were located almost entirely in buildings, although tents were occasionally
33Hamilton, Treatise, pp. 34-35, 38-39;USSC, Surgical Memoirs 1:40; Walt Whitman, The Wound Dresser... (Boston: Small, Maynard & Co., 1898), p. 44; Mitchell, "Medical Department," p. 1448.
34Jane Stuart Woolsey, Hospital Days (New York: D. Van Nostrand, 1868), pp. 41, 123; MSH 1, pt. 3:958; Whitman, The Wound Dresser, pp. 42-43; Charles S. Tripler and Chris C. Cox, "Report of the Committee Appointed to Memorialize Congress in Regard to the Medical Department of the Army," Transactions of the American Medical Association16 (1865):578; Hall, "Lessons," p. 93.
35Irwin, "Notes," p. 122, quote from p. 128; MSH2, pt. 3:909-12; Hamilton, Treatise, pp. 134, 136-37; Johnson, Muskets and Medicine, p. 129; Mitchell, "Medical Department," p.1446; Woodward, Outlines, p. 117; "Army Medical Intelligence, "Cincinnati Lancet and Observer 7 (1864):129.
290
MOWER GENERAL HOSPITAL in West Philadelphia, Pennsylvania. (Courtesy of National Library of Medicine.)
{kind=link}
used to increase their capacity. Authorities soon discovered that structures erected for some other purpose did not usually make good base hospitals. In a former hotel or barracks, no amount of purification, cleaning, and disinfecting could disguise the odors that spoke of inadequate ventilation. Maximum efficiency by a large staff, furthermore, was impossible in a badly designed building; every 1,000 patients required a staff of 20 wardmasters, 100 nurses, 5 or 6 cooks, 8 to 10 assistant cooks, 4 or 5 launderers with occasional assistants, 3 or 4 bakers, 10 to 15 men to run the stables and shops, 3 or 4 more men to manage the morgue and cemetery, 10 in the headquarters and library, about 15 physicians, and an undetermined number of medical cadets, all under the command of a regular or volunteer medical officer.36
As a result of the inconvenience and the sanitation problems involved in using existing buildings to house general hospitals, the Army began to design and erect structures intended from the outset for this purpose. Small post facilities had been designed and built specifically to house sick and wounded soldiers ever since the days of Lovell, but the Medical Department had never before encountered such a pressing need to design very large hospitals. Experiments undertaken in its drive to create them contributed considerably to civilian medicine too. The concept of the pavilion hospital was later adopted by such famous institutions as the Johns Hopkin Hospital, for which John Shaw Billings, who as a
36MSH 1, pt. 3:956-57; MSH 2,pt. 3:902, 908; Woodward, Outlines, p. 120; Northern Monthly(no. 2, Dec 1864), in U.S. Armory Square General Hospital, Washington, D.C., Orders, Correspondence, and Printed Matter, 1862-1869, Ms C60, p.191, NLM.
291
FLOOR PLAN OF MOWER GENERAL HOSPITAL as illustrated in the Medical and Surgical History of the War of the Rebellion.
292
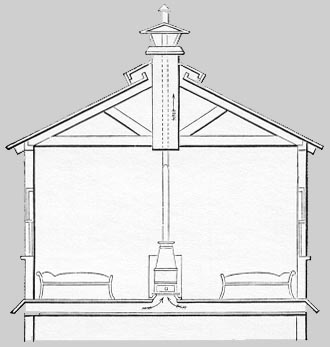
DESIGN FOR VENTILATION OF HOSPITAL STOVE as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
young medical officer worked on the design of the Army`s new general hospitals, drew the plans.37
In the pavilion hospital, thousand of patients could be sheltered and the spread of infection and contaminated air limited by the division of patients into relatively small groups, each kept separate from the others. Since the separation could result in administrative problems, various arrangements of the pavilions were tried to achieve the best combination of good ventilation and efficiency. On occasion, a hybrid hospital design was created by adding pavilions to a preexisting structure, which was used as the administration and storage building. Some of the earliest facilities, hastily erected, were of frail construction as well as poor design, and their walls eventually required buttressing to prevent their collapse. One design that proved satisfactory called for pavilions 24 to 25 feet wide and 12 to 14 feet high, which represented a 7-foot increase in width and a 4-to 6-foot increase in height over the earliest models, with the length cut from 200 feet to 150 feet. This plan also called for ridge ventilation on well-spacedbuildings.38
Hospital designers believed that the ideal facility would consist of one-story buildings set 3 to 4 feet above ground level where each patient had 1,000 cubic feet of air. In warm weather, ventilators at the ridge of the roof, sheltered from the rain by a small roof of their own, would keep the air circulating, and open corridors would add to the fresh air available. Cold weather ventilation would be achieved by closing shutters in the ridges and using a system of shafts that minimized the loss of the heat generated by stoves.39
Although city water and city sewers were available to some general hospitals, the problems involved in achieving sanitation goals, already difficult when so many patients suffered from diarrhea, were in some instances exacerbated by water shortages and the need to dispose of patient waste without city plumbing. The Medical Department was forced to experiment with solutions to such difficulties. In a Wilmington, Delaware, hospital, where city water was available but city sewers were not, a long trough under the seats of
37Mitchell, "Medical Department," p. 1446; MSH 1, pt. 3:896-98; Fielding H. Garrison, An Introduction to the History of Medicine, 4th ed. (Philadelphia: W. B. Saunders Co.,1929), p. 669.
38Quote from Hamilton, Treatise, p. 124; MSH 1,3:920, 922, 930, 394-95; Diffenbaugh, "Military Surgery," p.494.
39Woodward, Outlines, pp. 115-16, 118; MSH 1,pt. 3:935, 943-45, 952-53; Hamilton, Treatise, pp. 127-29; Hammond, Treatise, pp. 324-25.
293
the latrine was flushed two or three times a day and emptied by pipe into a deep covered pit some distance from the buildings. When hospital effluvia was discharged near the building or retained any length of time within it, odor became a problem, a particularly alarming one because doctors assumed that with odor came infection.40
As a rule, base hospitals sheltered patients suffering from every kind of disease, wound, and infection, but a few specialized facilities were beginning to appear. One such facility was the hospital in Philadelphia, where Mitchell, Moorehouse, and Keen studied patients with neurological and nervous problems. In 1863 the Army also established an eye and ear hospital in St. Louis, while in Nashville patients with erysipelas had their own facility. At Wilmington, Delaware, patients who had lost feet or toes to frostbite were hospitalized together, and in the fall of 1862 Surgeon General Hammond ordered the establishment of a facility for "mutilated soldiers" in New York City.41
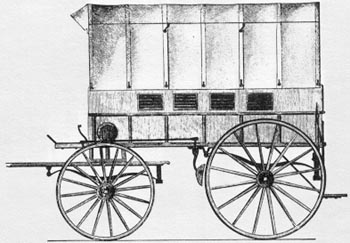
Innovative thought was as necessary in dealing with evacuation as it was with hospitalization. The enormity of the conflict made it plain early in the war that the casual approach of peacetime would not be adequate for the wounded and sick of 1861-1865. The two-wheeled ambulance proved too fragile and too uncomfortable for wide use on the battlefield. The Army was forced to experiment to find a conveyance that could move the wounded quickly from the battlefield to the nearest aid station and sturdier models to move them thence the longer distance to a hospital, hospital train, or hospital transport. Ironically, although many ambulance designs were tried, some of which were presented for approval by such Army surgeons as Finley and Tripler, the most useful one was the work not of a medical officer but of Brig. Gen. Daniel H. Rucker, a Quartermaster`s Department officer. Mule litters of varying design were also tried, but without significant success. The best stretcher proved to be one weighing less than twenty-four pounds and designed to be carried by man rather than beast.42
RUCKER AMBULANCE as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
The Medical Department also discovered that it was highly desirable to have trains and ships equipped specifically for the evacuation of the wounded. Early in the war, the wounded who traveled by train lay on straw in boxcars or, if they could manage it, sat up in passenger cars. Gradually, however, with the help of charitable organi-
40MSH 1, pt. 3:919-20, 922, 924, 928,953.
41Andrews, Surgery, pp. 413-14, quote from p. 413; MSH1, pt. 3:50, 665; USSC, Documents 2, no. 87:14; Ltr, McDougall to Hammond (25 Oct 1862), RG 112, entry 12; Western Sanitary Commission, Report, p. 11.
42MSH 2, pt. 3:866-67, 923-31, 944-57; Hamilton, Treatise, pp. 158, 166-67; "Flying Hospitals," American Medical Times5 (1862):263; Otis, A Report to the Surgeon-General, p. 11n; Thomas Longmore, A Treatise on the Transport of the Sick and Troops(London, 1869), pp. 357-58; War Department, SGO, Report on the Extent and Nature of the Materials Available for the Preparation of a Medical and Surgical History of the Rebellion (Philadelphia: J. B. Lippincott Co., 1865), p. 84.
294
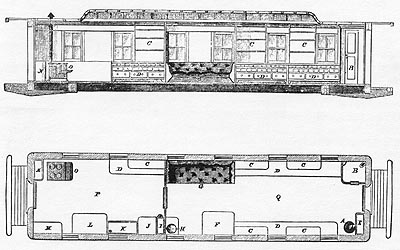
KITCHEN AND DISPENSARY CAR FOR HOSPITAL TRAIN, longitudinal view (top), and horizontal view (bottom), Army of the Potomac, as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
zations, more and more hospital cars of varying design and offering greater comfort began to appear, and in time these were combined into hospital trains that might include cars used specifically for cooking, dining, storage, or sleeping quarters for the medical staff. In Sherman`s army, civilians hired by the Quartermaster`s Department served as conductors and traincrew, while enlisted men served as cooks and nurses. The Medical Department staff present on such a train usually consisted of a surgeon in charge, an assistant surgeon, and a hospital steward. Clearly identified by its bright red smokestack, engine, and tender, and its three red lanterns at night, the hospital train was apparently never molested by the enemy. The various sanitary commissions also helped outfit specially equipped hospital ships and provided more vessels of their own when necessary.41
Although the most important obstacle had been surmounted when the Medical Department recognized the simple fact that a formal organization, careful planning, and trained and disciplined personnel
43MSH 2, pt. 3:959, 961, 964, 970-73, 977-98; John E . Ransom, "The Development of Ambulance Service in the Armies of Great Britain, the United States and Other Countries, "Ciba Symposia 8 (1946):554-59; Linus Pierpont Brockett and Mary C. Vaughn, Women`s Work in the Civil War: A Record of Heroism, Patriotism and Patience (Philadelphia: Ziegler, McCurdy & Co., 1867), pp.151-52; "Hospital Care- Report of Dr. Barnum," Sanitary Reporter1 (1863):147; Longmore, Treatise, p. 474; Turner, Victory Rode the Rails, pp. 300-301.
295
U.S. ARMY HOSPITAL STEAMER, D. A. JANUARY, as illustrated in the Medical and Surgical History of the War of the Rebellion.
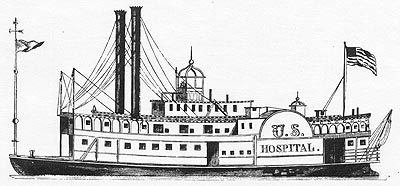{kind=link}
were necessary to successful evacuation, not everyone within the Army was willing to grant the department the control necessary to ensure its efficient operation. Letterman`s struggle to have the ambulance corps placed under the command of medical officers succeeded in the Army of the Potomac only with General McClellan`s support, and his approach was officially adopted throughout the Army late in the war. Medical Department control over hospital transports was not generally conceded until early 1865.
The improvements in the management of hospitalization and evacuation achieved during the course of the Civil War were considerable. By the end of the war, evacuation tended to be as prompt and as systematic as the military situation permitted. As a result, the number of regimental medical officers and attendants drawn away from the battlefield was minimal, and the need for tents and equipment for field and depot hospitals was limited. Although many patients still had to endure the heavy ride of Army wagons for short distances, increasing numbers made the major portion of their journey north or east in the comfort of well-appointed hospital ships or trains. The hospitals they stayed in along the way were more likely to be efficiently organized, and there was a better chance that the hospitals they reached at the end of their trip would be carefully designed and ventilated institutions where the staff was able to work with maximum efficiency.
In 1965 Army surgeons remained to a large degree helpless in the face of disease, and because of the devastating infections they, confronted, they made little progress in their handling of wounds. The Medical Department did, however, reestablish order after a chaotic beginning and create an organization competent to meet the de-
296
LOWER BOILER DECK OF D.A. JANUARY, as illustrated in the Medical and Surgical History of the War of the Rebellion.
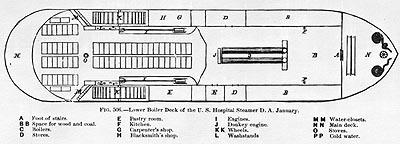{kind=link}
MIDDLE DECK OF D.A. JANUARY, as illustrated in the Medical and Surgical History of the War of the Rebellion.
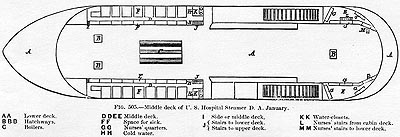{kind=link}
297
UPPER DECK OF D.A. JANUARY, as illustrated in the Medical and Surgical History of the War of the Rebellion.
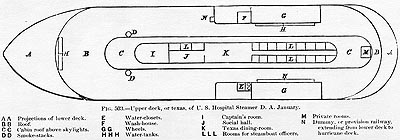{kind=link}
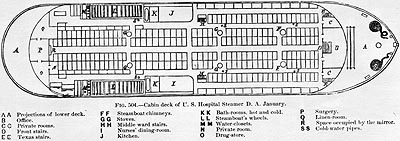
CABIN DECK OF D.A. JANUARY, as illustrated in the Medical and Surgical History of the War of the Rebellion.
{kind=link}
298
mands of a war that was waged on a scale never before encountered. These accomplishments were initially impossible, however, because those who shaped the Medical Department policies understood neither the unprecedented nature of the conflict nor the demands it was placing upon them. After William Hammond inspired the department`s overwhelmed medical officers to withstand frustration and adversity while he initiated new and determined approaches to their problems, there was no turning back to the old ways. By cooperating closely with one another, the very men who had been Hammond`s undoing were able to continue successfully along the path he had laid out.
Epilogue
The creation of the Medical Department on a permanent basis in 1818 had far-reaching consequences both for the U.S. Army and for medical science. Endowed by Congress with the responsibility for a permanent organization rather than a temporary wartime expedient, the surgeon general was in a position from this time onward to make long-range plans for the care of the Army`s sick and wounded in war and peace and to direct continuing efforts to contribute to the sum of medical knowledge. Much depended, however, on the ability of the physician who served as surgeon general.
The first man to head the Medical Department was the young and brilliant Joseph Lovell, who quickly moved to improve the caliber of his staff and to begin collecting information on factors that might be affecting the Army`s health. Because of Lovell`s efforts, the highly trained and disciplined physicians who gradually replaced the motley crew that formed the department in 1818 began to regard themselves as members of a proud profession. The beneficial effects of this change in attitude were soon evident, for, on the whole, the first career military surgeons in the nation`s history worked diligently to meet the responsibilities placed upon them.
The appointment of the most senior surgeons in the department rather than the most able as Lovell`s two immediate successors did not augur well for further progress in the Medical Department. Nevertheless, Thomas Lawson`s enthusiasm for the department and its work led to the winning of rank for Army surgeons. He also obtained the right to enlist hospital stewards, continued the collection of data started by Lovell, and worked to develop an effective ambulance. Lawson grew old and ill in office, however, and when he died, the department was still unprepared for war. Lawson`s successor, Clement Finley, while healthier than his predecessor was probably less competent and came to office entirely because of his seniority.
As a result, the Medical Department began to meet the challenge of the Civil War only when Finley was succeeded by a physician who was, like Lovell, both young and talented. Appointed surgeon general despite his lack of seniority, William Hammond built upon the small but sturdy foundation laid and maintained by his predecessors. Forcing through the changes in the department`s organization and administration that were necessary to meet the needs of vast numbers of sick and wounded, with the assistance of the Department`s small nucleus of Regular Army surgeons, Hammond, like his successor, initiated thousands of civilian physicians into the mysteries of their wartime duties.
Unlike his predecessors during the Civil War, Joseph Barnes, who took over as surgeon general upon Hammond`s disgrace, was regarded with great favor by Secretary
299
of War Stanton. He was, therefore, able to continue along the lines set out by Hammond with far greater ease than Hammond himself. During Barnes` tenure, Congress finally created the ambulance corps for which Hammond and his supporters had fought. In the last months of the war, Barnes finally gained for the Medical Department complete control of evacuation and the management of hospitals. The last Civil War surgeon general so pleased his superiors that he was brevetted major general in March 1865.
Although five surgeons general directed the Medical Department from 1818 through 1865, two of them were principally responsible for the shaping of the department`s character to meet the demands placed upon it. Lovell professionalized the care that the Army`s sick and wounded would in the future receive and, in insisting on regular and detailed reports on all matters that might relate to the soldier`s health, let it be known that the Medical Department planned to play a major role in the world of medicine. Circumstances required that Hammond create the department anew, but even as he worked to reorder the structure under which the sick and wounded received care, he demonstrated his agreement with Lovell`s ambition for the department by calling for the gathering of case histories and specimens from his surgeons. As they strove to adapt the Medical Department`s structure and operations to the needs of their times, both Lovell and Hammond blazed clear paths that their less talented successors could follow.
Nevertheless, the willingness of the first surgeons general to take advantage of the department`s potential for contribution to science and their determination to improve the medical care offered to the nation`s soldiers did not result in major scientific discoveries. The era when clinical observations and statistical compilations were the principal approach to the mysteries of human health was rapidly passing. As the tribulations of William Beaumont proved, even in peacetime the Medical Department of the 1818-1865 period was not in a position to foster experimental research.
The department was able during this period to contribute to medical science in lesser, practical ways because the use of any remedy or treatment in relatively large numbers of patients by physicians working under the discipline of a single organization inevitably constitutes a trial of its worth. It was the Army`s experience since 1800 that clearly demonstrated the benefits of mass vaccination against smallpox. Army surgeons established both the advisability and safety of using higher doses of quinine than those customary outside the South and the powers of bromine against infection. The Army`s Civil War use of anesthetics demonstrated on a large scale the benefits and the relative safety of these agents when carefully used.
With the acceptance of the germ theory, however, would come the discovery of the causes of typhoid, malaria, dysentery, and other major diseases, and the resultant development of better ways in which to prevent and treat these scourges. In comparison to these dramatic events, the Army`s informal testing appears insignificant. As the end of the century approached, however, and medical science moved forward with great rapidity, medical officers of the U.S. Army would be in the forefront of many great advances. Army surgeons would be increasingly able to prevent and cure disease and infection. With new and better weapons, post-Civil War physicians would wage a more successful struggle against disease and infection, but they would never conduct a more gallant fight than the Army surgeons of 1818-1865.
![]()