



Books and Documents > The Army Medical Department 1818-1865
CHAPTER 4
Lawson`s First Years as Surgeon General, 1836-1845
Although the Second Seminole War in Florida was Lawson`s greatest concern during most of his first decade as surgeon general, he could not ignore the needs of the men stationed at the posts scattered about the rest of the nation. As increasing numbers of Indians from the Southeast as well as white settlers moved west of the Mississippi, the Army`s responsibilities in that part of the country grew. The need to protect white traders and settlers and Indians from one another and the newly arrived Indians from those indigenous to the area dictated the maintenance of distant posts, even in the most unhealthy areas of Arkansas and the Oklahoma Territory.
Administration in Washington
In the early years of Lawson`s service as surgeon general, the need for surgeons was great west of the Mississippi, and until 1842 the demands of the Second Seminole War were even greater. Under these circumstances, the Army Medical Department more than ever needed a strong central administration to assign its small staff as effectively as possible, to manage the purchase and distribution of medicines and other supplies to posts from the Atlantic to Oklahoma, and to anticipate future needs.
Lawson, however, was not enthusiastic about office work. In 1839 he complained:
I am continuously engaged in answering calls from Congress and the Secretary of War, and in disposing of references made to the department, by any body and every body and so incessantly annoyed with the trumped up accounts coming in upon the office from every section of the Country and every division of the Army that I cannot bestow that attention upon the general interests of the Medical department which I desire to do and ought to do.
He had one or more surgeons assisting him in his office at various times, and on occasion, despite his usual resentment for those who might seem to be encroaching upon his prerogatives, he willingly delegated his authority in the central office to such men as Benjamin King, Richard Coolidge, and Henry Heiskell in order to go out into the field or to free himself from the more tedious demands of his position.1
In other ways, however, Lawson made the most of his Washington assignment. He did not let his eagerness for more active life blind him to the sedentary joys of verbal "tilts" or his scorn for "finery and fur-
1Quote from Ltr, Lawson to Mower (21 Mar 1839), RG 112, entry 2, 15:75. Unless otherwise indicated, material in this chapter is based on War Department, SGO, Annual Reports; Brown, Medical Department; Callan, Military Laws; War Department, General Regulations. 1841 and 1847: and Avars. "Notes."
74
BENJAMIN KING. (Courtesy of National Library of Medicine.)
{kind=link}
RICHARD H. COOLIDGE. (Courtesy of National Library of Medicine.)
{kind=link}
belows" inhibit his enjoyment for the refinements of the capital`s society. A young lieutenant whom Lawson had invited to dinner and who shared his bachelor host`s hospitality with, among others, the commander in chief of the Army, Lt. Gen. Winfield Scott, reported that "the Doctor had a dinner of thirteen courses, provided by the prince of restaurant caterers. The wines were old and rare."2
Except for the problems arising directly from the Seminole wars, most of those Lawson faced in his first years at his Washington desk had been faced by Lovell before him: the inadequate size of the department, the need to establish high standards for the staff and to improve its status, the inadequate number and quality of hospitals and attendants, and the difficulties involved in maintaining the health of the Army at a time when recruits were often in poor condition and the art of medicine was almost primitive. Lawson generally followed his predecessor`s approach to these common problems, but his style of management was radically different from that of the quiet-spoken, and unassuming Lovell.
When Lawson became surgeon general, the Medical Department consisted of fifteen surgeons and sixty assistant surgeons, in addition to a clerk who worked in the Washington office. In 1838 the demands of
2First quote, Ltr, Lawson to AG (copy, 17 Aug 1841), RG 112, entry 12; second quote, Ltr, Lawson to Taylor (18 Nov 1839), RG 112, entry 2,11:73;third quote, Samuel Gibbs French, Two Wars, an Autobiography of Gen. Samuel G. French (Nashville, Tenn.: Confederate Veteran, 1901), p. 28; see also invitations to Lawson in Lawson Papers, LC.
75
the Second Seminole War led Congress to allow the appointment of seven more surgeons. In 1841 a second clerk joined the Washington office, but in 1842, despite the fact that the Army then manned seventy-five posts, Congress ordered the dismissal of two surgeons and ten assistant surgeons, reducing the total number of Regular Army physicians to seventy. A wise provision of this law, however, required that each man who left the department be individually selected out on the basis of his value to the Army, regardless of his seniority.3
The shortage of surgeons forced Lawson to restrict the granting of leave, generally to medical officers who were ill. Even then, he granted leave only to those who had long been in the field on active duty. This policy did not condemn a surgeon to remain forever at one post, however. Lawson believed that medical officers should be moved about so as to become familiar with the climate and "diseases of every section of the Country."4
Under the circumstances, the low attrition in the Medical Department might appear surprising. Many graduates of West Point, faced with low salaries, slow promotions, and assignments in primitive locations that were scarcely suited to the raising of a family, resigned their commissions. Most surgeons, however, apparently found the limited opportunities available to them in civilian life, where the ratio of doctors was high, less lucrative than those available to West Point-trained engineers and stayed in the Army. From 1841 through 1842, of seven department vacancies, only three resulted from resignations and the remaining four from disease contracted in Florida. From 1843 through 1845, there were but six vacancies, two of them caused by deaths, in a department of seventy men.5
Ironically, at a time when the shortage of surgeons in the Army was acute, the individual medical officer. was not necessarily overworked, and Lawson permitted his subordinates to concern themselves with matters that did not directly involve sick or injured soldiers. The variety of duties and professional opportunities that continued to be available may, indeed, have been part of the attraction of the hard, isolated Army life for young physicians. During the 1836 to 1845 period, when the Army made it clear that surgeons were not required to care for anyone but soldiers, it was customary for medical officers to offer their services to wives, children, and other civilians at their posts. In addition, three Medical Department doctors were working, apparently full time, on the problem of choosing and buying sites for two hospitals that were to serve disabled merchant seamen, at the direction of the surgeon general in response to a request from the adjutant general.6
The professional and military pride that
3Ltr, Lawson to J. K. Spaulding (15 Apr 1845), RG 112, entry 2, 15:457-58.
4Quote from Ltr, Lawson to D. C. M. Arbuckle (22 Oct 1840), RG 112, entry 2, 12:107; Ltrs, Lawson to Satterlee (27 Mar 1839) and King to Charles McDougal (7 Jun 1839), both in RG 112, entry 2, 10:223 and 337, respectively.
5"The Requirements of the United States Army and Navy Boards of Medical Examiners. Also those of the British Army and Navy," Transactions of the American Medical Association 2 (1849):317; Sprague, Florida War, p. 548; Duffy, The Healers, p. 9.
6Ltrs, King to J. M. Foltz (17 Nov 1836) and Lawson to AG (1 May 1837), both in RG 112, entry 2, 8:112-13 and 328, respectively; King to Sec War (28 Nov 1837 and 5 Jan 1838), both in RG 112, entry 2, 9:65 and 103, respectively; Lawson to E. B. Birdsall (31 Dec 1838), to Burton Randall (2 Feb 1839), to William Maynadier (25 May 1840), to Lyman Foot (27 Jul 1840), to J. Martin (9 Jul 1841), and to R. S. Baker (7 Aug 1841), all in RG 112, entry 2, 10:62 and 133, 11:351 and 429, and 13:7 and 54, respectively; Heiskell to M. E. Tyler and to D. S. Kimball (both 4 Jun 1845), both in RG 112, entry 2, 16:33 and 34, respectively.
76
Lawson inculcated in his subordinates were also inducements to remain in the Army. The surgeon general expected his surgeons, however heavily burdened, to work without complaining and to exhibit great resourcefulness and unfailing energy under all circumstances. He also insisted that they bear themselves proudly and not submit to indignities or encroachments upon their rights and privileges. "Although in the eye of the law and regulations," Lawson maintained, surgeons were "noncombatants," they were obliged to "prove themselves to possess the ambition andthe feelings of the proudest officers & soldiers."7
The surgeons` basic, responsibilities toward the soldier had changed little. In war and in peace, they continued to care for the sick and wounded and attempted to prevent disease by ensuring that a soldier`s water was good and that the food was both good and properly prepared. They also consulted with the commanding officer on the location of posts and camps, and when troops were to be moved by water, inspected the transports.8
The medical officer`s pre induction examination of the Army recruit, involving principally a visual inspection of the disrobed candidate, might appear to have been one of his least demanding duties, but failure to take this responsibility seriously could bring the surgeon to grief. When it could be proved that an unfit man had been accepted as a recruit, those responsible for an injudicious acceptance were apparently required to reimburse the Army for the expense of clothing and equipping him. In one such instance, an assistant surgeon and a recruiting officer were forced to share this cost for each of three recruits who, according to an inspecting board, could not meet the Army`s physical qualifications. The physician`s fine, half the total, was $26.11, more than $23 of which was for clothing. The medical officer defended himself by saying that the supposedly preexisting conditions in all three men could be faked by someone anxious to get out of the Army, that it had not been proved that any of the problems existed at the time of the recruitment, that he had not had the opportunity of cross-examining the men in question, and that he was being deprived of his property without due process. The surgeon general backed his subordinate in an appeal to the secretary of war, but one of the mem-
7Quote from Ltr, Lawson to Foot (17 Dec 1840), RG 112, entry 2, 15:295; Ltrs, Lawson to Wheaton (20 Sep 1841) and to Clement Finley (18 Sep 1844), both in RG 112, entry 2, 12:207 and 13:103, respectively.
8Robinson, An Account 1:41.
77
bers of the board of inspectors investigating the matter was an Army surgeon. Assuming, apparently, that the board`s physician would have been able to detect a faked contraction of the last two fingers on the right hand or a feigned lameness supposedly caused by a leg two inches shorter than its mate, the Army refused to back down. In any case, the protesting surgeon finally abandoned his case and paid up.9
The collection of meteorological data also remained among the duties of the Army surgeon. The observations and reports on weather and similar matters that the surgeon general required of his subordinates was becoming even more complex with time. The physician responsible for reports from Governors Island in New York Harbor, for example, was required to use not only a barometer and thermometer but also a rain gauge, hygrometer, and wet bulb, and to record cloud formations and the direction and force of the winds. All surgeons became responsible for recording sudden changes in the wind and temperature, the moment when the barometer reached its lowest point during a storm, and even the passage of flocks of migratory birds. Although these responsibilities were
9Rpt, Board of Inspectors (21 May 1839) and Ltrs, Treasury to Hawkins (29 Dec 1840), Hawkins to B. Lewis (13 Jan 1841) and to Lawson (10 May 1841), Lawson to Sec War (3 Jun 1841), Asst AG to Sec War (5 Jun 1841), and Hawkins to Lawson (18 Jun 1841), all in RG 112, entry 12.
79
no doubt an unwelcome burden to some medical officers, others apparently came to enjoy this particular aspect of their work..10
The enormous quantity of reports on meteorological observations that poured into the Washington office only added to Lawson`s problems with paperwork. In 1841 he finally decided that he would no longer acknowledge the arrival of each report and that he would instead write a surgeon in the field only when a report failed to arrive on time. Questions apparently also arose concerning these reports because in 1842 Lawson ordered the formation of a medical board to design accurate and uniform instructions.11
The importance of the Medical Department`s information gathering was apparently widely recognized by the 1840s. In 1842 the Army requested that colleges, scientific institutions, and private citizens cooperate in the collection of data. When an earthquake shook parts of the Southwest on 4 January 1843, inquiries came in to the department from private citizens interested in learning the details of the event, asking that information on the quake be obtained from surgeons in the field. The surgeon general appears to have sent such a questionnaire to his surgeons only a few days after receiving the request.12
Locating young doctors with the ability to perform satisfactorily all the many duties required of them by the Army Medical Department was difficult even though physicians were so numerous that establishing a profitable practice was difficult. Doctors with the education necessary to pass the Department`s tests were presumably among those whose chances for establishing a lucrative practice appear to have been the best. An average of 50 percent or more of those examined failed, but the tests were never waived, even when administering them required the temporary removal of an assistant surgeon from duty in Florida during the Second Seminole War. The department was apparently unwilling to take chances in its search for doctors of good background who might find that the excitement and challenge of military life and the possible difficulties of private practice outweighed the danger and isolation that could face the Army surgeon.13
The entrance examinations were apparently given without favor to anyone, and the age limit of twenty-one to twenty-eight for the examinees was never waived. Unsuccessful candidates occasionally lashed out with accusations such as "damned favoritism- because I did not have influential friends to intercede for me." In this particular instance, the young applicant may have tried to conceal the fact that he was not yet of age, but Lawson was able to calm the troubled waters. Less than two months after he had accused Lawson of "damned favoritism," the proud Dr. James L. Peacocke wrote Lawson to express his gratitude "for the kind words and gentlemanly treatment" he had received from the
10Thomas A. Mower, "Meteorological Observations," New York Journal of Medicine and the Collateral Sciences 2 (1844):134,137; Edgar Erkskine Hume, Ornithologists of the United States Army Medical Corps (Baltimore: Johns Hopkins Press, 1942).
11Cir (14 Jul 1841), RG 112, entry 2, 13:15-56.
12Mower, "Meteorological Observations," p. 137; Ltrs, Lawson to Thomas C. Madison (30 May 1843) and to Henry D. Rogers (31 May 1843), both in RG 112, entry 2, 14:207-08 and 210-11, respectively; Rogers to Sec War (27 Mar and 7 Apr 1843), both in RG 112, entry 12.
13Richard H. Shryock, "Public Relations of the Medical Profession in Great Britain and the United States, 1600-1870," Annals of Medical History, n.s., 2 (1930):318-19; Ltr, AG to Taylor (15 Oct 1839), RG 94, M565, roll 11, 15:435-36; John Duffy, The Healers (New York: McGraw-Hill Book Co., 1976), pp. 177-81.
79
surgeon general and his assistant when he visited Washington.14
As a result of the requirements laid down by the Medical Department for entry and promotion, the reputation of Army surgeons improved. A civilian physician, writing in 1848, pointed out that the Medical Department`s entrance examinations had always been strict and that incompetents had never been known to pass them. The department`s system, he stated, "has saved thousands of brave men from the knives and nostrums [dubious remedies] of professional bunglers." Although they did not explain their reasoning, authorities maintained that the age limit was second only to the examinations themselves as a promoter of the efficiency of the medical service.15
Men so rigorously selected deserved, in Lawson`s opinion, more adequate salaries. Some of his surgeons had written in early 1838 to express their belief that their pay did not reflect the importance of their services. That same year, however, Congress finally raised their pay to equal that given those cavalry officers ranking from first lieutenant through major and also granted an extra ration for every five years of service. This step gave assistant surgeons with less than five years of experience $3.33more a month and all other department physicians $10 more a month.16
The rank and status of Army surgeons in the 1836 to 1845 period remained imprecisely defined, however. Despite their pay, they did not have the rank of field officers and were not entitled to the salutes prescribed for such officers even though they received equivalent salaries. In addition, although the surgeon`s right to serve on a court martial was indisputable, some question existed about his eligibility to serve on such purely administrative bodies as the boards that decided on the disposal of serviceable property (boards of survey) or that managed the fiscal affairs of a post (councils of administration). The commanding officer of a fort was not always happy to have the post surgeon on such a board, but by 1840 the adjutant general had made it plain that although Army physicians could not preside over such bodies, they were entitled to serve on them.17
Lawson was concerned with appearances as well as with substance. The impression created by the surgeon`s uniform had long concerned him and he became enraged over proposed modifications that suggested to him that the medical officer was considered in some way to be inferior to his brother of the line. The surgeon general indicated that he personally would rather wear civilian dress than a uniform unadorned by epaulets. He claimed that their presence upon a medical officer`s shoulders would cause him to esteem his commission more highly. As a result of Lawson`s efforts, the new surgeon`s uniform of 1840 was complete with "Epaulettes-Gold, with solid bright crescent" and "a spread eagle of solid silver metal to be worn by the Surgeon General only ... to be placed upon the epaulette strap above the wreath." The
14Quotes from Ltrs, Peacocke to Lawson (5 Oct and 23 Nov 1842), both in RG 112, entry 12; Ltr, G. M. Willing to Lawson (30 Aug 1842), RG 112, entry 12
15Robinson, An Account 1:40-41, quote from p. 43: Ltrs, Lawson to Sec War (29 Apr 1840) and Heiskell to John Bell (13 Apr 1841), both in RG 112, entry 2, 11:310 and 12:376, respectively; "The Requirements," p. 317; "Review of Forry`s Statistical Researches," Western Journal of Medicine and Surgery, 1st ser., 4 (1841):271-72; Croghan, Army Life, p. 23.
16Ltrs, King to Miller (10 Feb 1838), RG 112, entry 2,9:152-53; W. L. Wharton et al. to SG (28 Feb 1838), RG 112, entry 12; Army and Navy Chronicle, p. 346.
17Ltrs, Lawson to Sec War (18 Jul 1838) and to Porter (17 Mar 1840) and Heiskell to Sec War (4 Nov 1841) and to W. Levely (9 Feb 1844), all in RG 112, entry 2, 9:367, 11:247-48, 13:154-57, and 14:43, respectively.
80
epaulets of all were to bear "a laurel wreath embroidered in gold, and the letters `M.S.` in old English characters within the wreath.18
Lawson`s readiness to fight higher authority on behalf of his subordinates undoubtedly made his flaming pen easier to bear, but in some instances he fought with his surgeons as vigorously as he fought for them. As a rule, his deepest anger was directed at those who appeared to be shirking their duties in Florida or using illness as an excuse for avoiding responsibilities. Even a medical officer`s unfortunate choice of words, however, might cause a marked ruffling of the Lawsonian feathers. Although Lawson had been an arrogant and belligerent subordinate of Lovell, he was very sensitive about the attitudes of his subordinates when he became surgeon general. To one surgeon whose language had unwittingly offended, he wrote, "When it suits my purposes to prefer formal charges against you, I shall do it without your dictation; and should you wish to apply through me to a Court of Inquiry, your language must be more respectful to me and towards the Secretary ofWar."19
Among Lawson`s more significant feuds with a subordinate was the one with William Beaumont, a man whose pride appears to have rivaled that of the surgeon general. Lawson began to resent the attentions and special considerations that Lovell showed Beaumont during the period of Beaumont`s work with Alexis St. Martin. By the time Lawson succeeded Lovell as surgeon general, Beaumont had attained international respect and fame. The antagonism between the two men was great. Each appears to have believed himself entitled to a degree of respect that the other was not willing to grant. Finally, in 1839 Beaumont requested a leave of absence with his replacement to be provided by the department at its expense. Since personal business was the stated reason for the request, Lawson denied it. Beaumont, already distressed by rumors that Lawson was planning to move him to a less desirable post, responded to the refusal with a lengthy and condescending letter of the kind that invariably enraged Lawson. The surgeon general not only held his ground on the matter of leave but added fuel to the fire in September of 1839 by ordering Beaumont to Florida to serve on a medical examining board. Because Beaumont was no longer conducting research on St. Martin`s digestion, the assignment appears to have been reasonable, but Beaumont, in an attempt to force Lawson to rescind it, submitted his resignation. To his astonishment, the surgeon general accepted it, commenting that "if an example is not made of some one soon, the army will become more like a mob than a military Body." Beaumont then attempted to withdraw his resignation, but Lawson stood fast. Beaumont`s long and distinguished Army career, one that began in the War of 1812 when both Beaumont and Lawson had first committed themselves to the care of the Army`s sick and wounded, was at an end.20
Lawson`s concerns were not limited to the physicians in his department. He was also interested in the attendants who as-
18Quote from Brown, Medical Department, p. 164; Ltr, Lawson to Lovell (5 Oct 1824), RG 112, entry 2.
19Quote from Ltr, Lawson to Woods (12 Oct 1840), RG 112, entry 2, 12:54; for Lawson`s attitude toward Lovell, see also RG 112, Lawson`s Letterbook, 1821-1825, entry 226, esp. Ltr, 16 Oct 1825.
20Quote from Ltr, Lawson to Sec War (16 Jan 1840), RG 112, entry 2, 11:188; Myer, Beaumont, pp. 241-45, 251-54, 265-67; Ltrs, Lovell to AG (7 Jul 1827) and Lawson to William Beaumont (27 Mar 1839), both in RG 112, entry 2, 4:156 and 10:222, respectively.
81
sisted post surgeons in their hospitals. The problem of obtaining good men to serve as hospital stewards remained from Lovell`s period of administration. A steward was usually selected from the line by a surgeon, with the consent of the post`s commanding officer. The Medical Department apparently continued to operate on the assumption that when it was impossible to find in this way an enlisted man capable of performing in a sober, reliable, and reasonably intelligent manner, the post surgeon could enlist a man specifically to serve in this capacity or even hire a civilian.21
A law enacted in 1838 officially authorized the enlistment of young men as stewards and increased their pay. At posts with more than four companies, stewards were paid as sergeants of ordnance; at smaller posts, they were paid as infantry sergeants. Nevertheless, many surgeons continued to have questions about signing on stewards. Thomas Mower, a surgeon on recruiting duty in 1839, made an arrangement with a young man anxious to serve as a hospital steward, specifying that he was not to serve in any other capacity. Since the enlistee had "rec. a collegiate education" and was both "a student of theology" and "of good character," Mower was eager to have him in the Army but was unsure how to interpret the regulations.22
In 1842 Congress forbade the enlistment or reenlistment of men to serve specifically as stewards, but surgeons continued to be confused. "Is it intended that the assignment of Hospital Stewards be permanent, or only temporary"? a surgeon wrote Lawson in 1844, adding, "Can a citizen who has enlisted solely with a view to perform the duties of Hospl steward be reduced to the ranks and made liable to perform military duty- more especially when the word soldier has been erased and steward substituted in the enlistment?" How Lawson solved this problem is not known.23
The realization of the extent to which a good steward could lighten the medical officer`s burden engendered much of the interest in the character of the men chosen to be hospital attendants. Lawson did not approve of the custom of those surgeons who had their stewards fill out reports and manage accounts, because unnecessary errors resulted. He did not, however, underestimate the worth of stewards to the Medical Department. Wishing to upgrade their position, in early 1840 he established a training school for stewards at one of the New York Harbor posts, apparently Fort Columbus. By mid-1840 twenty young men of upright moral character had been trained by an assistant surgeon, had gone through a four to five-month probationary period, and had been sent out to assist surgeons requesting their aid. In 1844 the adjutant general ruled that new orders issued by the commanding general of the Army, Lt. Gen. Winfield Scott, required that stewards be taken from the line and that they remain attached to their companies. Lawson`s attempts to improve the standards for hospital stewards were thereby negated, and the records of the period never again refer to the school .24
21Ltr, Thomas Mower, Heiskell, and Sylvester Day to Lawson (30 Jul 1840), RG 112, entry 12.
22Quote from Ltr, Mower to Lawson (18 Feb 1839), RG 112, entry 12; Ltr, Mower, Heiskell, and Day to Lawson (30 Jul 1840), RG 112, entry 12.
23Quote from Ltr, Adam M. McLaren to Lawson (14 Apr 1844), RG 112, entry 12; Ltrs, Heiskell to Sec War (8 Dec 1842), RG 112, entry 12; Lawson to John S. Griffin (11 Oct 1843), RG 112, entry 2, 14:439; see also Ltrs, Mills to Lawson (12 Aug 1837), Wheaton to SG (4 Jan 1843), McDougall to Lawson (13 Apr 1843), Lawrence Sprague to Lawson (10 Oct 1843), Stinnecke to Lawson (8 May 1844), and AG to Military Storekeeper (15 Jun 1844), all in RG 112, entry 12; Lawson to Stinnecke (13 May 1844), RG 112, entry 2, 15:143.
24Ltrs, Lawson to Hoxon (24 Apr 1840), to Randall (25 Aug 1840). and to Richard H. Coolidge (1 Oct 1841), all in RG 112, entry 2, 11:302 and 494 and 13:115, respectively; Henderson to Lovell (12 May 1836), Heiskell to Lawson (4 Jan 1839), Russell to Lawson (15 Dec 1839), Randall to Lawson (17 May 1840), Mower, Heiskell, and Day to Lawson (30 Jul 1840), Wheaton to Lawson (23 Oct 1841), Hawkins to Lawson (25 May 1842), Porter to Lawson (11 Jun 1844), E. D. Townsend to C. S. Merchant (copy, 14 Jun 1844), Porter to Lawson (2 Jul 1844), and Steiner to Lawson (20 Jul 1848), all in RG 112, entry 12.
82
THOMAS MOWER. (Courtesy of National Library of Medicine.)
{kind=link}
Surgeons do not appear to have been as enthusiastic about hiring women to help in hospitals as they were about hiring stewards. At least one surgeon suggested replacing matrons with men. Matrons were the only women routinely found working in Army hospitals, but the surgeon at Fort Wood, in New York Harbor, maintained that it was they who caused the greatest problems he ever had to face in his facility. They "either have children when they come, or make out to get them soon after, which adds very materially to the other objections against them." In listing these other objections, he noted that matrons were "lazy, sluttish, and wasteful, and in short . . . , a nuisance."25
Lawson does not appear to have expressed himself on the subject of women in hospitals, but he emphasized his "dislike to any thing like effeminancy, luxury, or too much convenience in a military hospital." He could not "consent to make Gentlemen of common Men as soon as they are brought into the Army." No man, in his opinion, was entitled to find in a military hospital any form of luxury he could not provide for himself at home, and Lawson obviously intended that this policy be a guide to those ordering supplies for these facilities.26
Nevertheless, certain standards had to be maintained at the various post hospitals scattered about the nation, and many facilities needed upgrading. In 1839 Congress voted almost $70,000 for the building of new hospitals, but most of this sum was spent in just two years. In 1843 the surgeon general pointed out that the coastal forts still lacked appropriate hospital facilities. He blamed this situation upon those who believed that structures erected outside the walls of a fort would interfere with its defense. He pointed out that a building located outside the fortifications could be burned down if hostilities ever made it advisable, but that keeping patients in the damp, poorly ventilated quarters within fortifications endangered their recovery and, indeed, threatened the health of all those who lived in them.
25Quotes from Ltr, Monroe to Lawson (11 Aug 1837), RG 112, entry 12; Ltr, Monroe to Lawson (24 Aug 1837), RG 112, entry 12.
26Ltr, Lawson to Russell (20 Jun 1844), RG 112, entry 2, 15:204.
83
Despite his open dislike for "too much convenience," Lawson also appears to have been receptive to ideas for improving hospital equipment. When the secretary of war expressed an interest in having iron bedsteads used throughout the Army, for example, Lawson moved quickly to look into the matter. In the fall of 1837 he had one single and one double metal bedstead made up and sent to the War Department, confident that if these frames could be obtained at a reasonable price, the secretary would order them for hospitals as well as for barracks. The price of $15 each proved acceptable. Congress appropriated funds for the purpose, and Lawson began to buy bedsteads and to send them out to many post hospitals. By 1843 the money voted for this purpose had all been spent. Lawson noted that the new frames held up well, were free of insects, had a neater appearance than their wooden counterparts, and took up less space. He placed a second order for metal frames in 1845, using a slightly different, improved, and less expensive design, one for which "the parts will be made with such nicety and precision as to fit each other promiscuously."27
Lawson was also interested in having some sort of ambulance developed for use in Florida during the Second Seminole War. He envisioned a plain, light, two horse wagon "on Boston or Cradle springs." In this vehicle the wounded would lie upon canvas slings, ten to twelve inches above the floor, so that medicines could be stored beneath them. An ambulance and a set of panniers made of tin and slung across a saddle by means of a leather case should be provided for each battalion. A prototype of the desired wagon appears to have actually been built, but there is no recordof its having been put into regular service at this time.28
As far as posts in the West were concerned, transportation presented a greater problem than purchasing. Ships came to grief from time to time and floods could delay the delivery of much-needed goods. Some forts appear to have been particularly unfortunate. In March 1845, for example, a packet ship loaded with supplies for Forts Snelling and Crawford, as well as for Forts Leavenworth, Atkinson, Des Moines, and Scott, was wrecked, and only three months later, when another ship, bound for New Orleans, met misfortune on the coast of Florida, the mishap deprived Fort Crawford of sixteen iron bedsteads and Fort Snelling of another twelve.29
Lawson was concerned about the care and disposal of old Medical Department property as well as with the purchase and transportation of the new. He was, for example, interested in the use of old bedding and linens. Great care should be taken, he believed, to ensure that boards of survey were not called upon to condemn property that could still be made to fulfill its original purpose, but only a board of survey could condemn items that could no longer be used for their original purpose. The actual disposal then became the responsibility of the surgeon involved. Worn-out linens
27First quote, ibid.; second quote, Ltr, Mower to Lawson (23 Oct 1844), RG 112, entry 12; Ltrs, Lawson to Thomas Mower (1 Sep 1837), RG 112, entry 2 , 8:476; Lawson to Leonard, to Simpson, and to Russell (all 29 Jul 1840), all in RG 112, entry 2, 11:432-33; Heiskell to M. Mason (24 Nov 1841) and Lawson to Abadie (26 Oct 1843) and to Moses H. Grinnell (16 Feb 1844), all in RG 112, entry 2, 13:192,14:452, and 15:48-49, respectively; Mower to Lawson (17 Apr 1843, 23 Oct and 3 Dec 1844, and 16 Jan, 12 Mar, and 26 Apr 1845), all in RG 112, entry 12.
28Quote from Ltr, Lawson to Sec War (26 Jul 1837), RG 112, entry 2, 8:423-24; Ltr, Lawson to A. MacKay (17 Aug 1837), RG 112, entry 2, 8:458.
29Ltrs, Mower to Lawson (25 Mar and 13 Jun 1845) and Griffin to Lawson (1 Apr 1846), all in RG 112, entry 12.
84
were not, Lawson informed one surgeon, to be used as dishcloths or for "other household purposes," but superannuated pillowcases and sheets beyond repair were to be used for bandages and dressings.30
Among other problems that arose in connection with the Medical Department`s expenses was that of how properly to allocate a soldier`s commutation allowance for food, a matter that came to a head in 1841. The difficulty stemmed from the fact that the food of hospitalized soldiers was provided by both the Subsistence and the Medical Departments. Should the Subsistence Department be unable to supply the specialized type of diet that a patient might require, the expense for his food became the responsibility of the Medical Department. The issue, therefore, was whether the monetary value of the ration normally supplied by the Subsistence Department but not used for a hospitalized patient should be paid out to acting medical purveyors for the Medical Department`s use as needed without restriction. The alternatives involved either using the ration allowance solely and specifically for the benefit of the individual soldier or crediting the sum to his unit. The surgeon general decided that it was illogical for a soldier to receive both hospital rations and the benefit of the government allowance at the same time and ruled that such money should go into a common fund for use by the Medical Department.
Problems of Surgeons in the Field
Except for the high morbidity in Florida that resulted from the Second Seminole War, disease patterns, like the other problems facing the Medical Department, did not change materially in the first years after Lawson succeeded Lovell as surgeon general. Alcoholism continued to cause difficulties, despite Lovell`s campaign against hard liquor and reports that intemperance was undermining the health of untold numbers of men. The Army itself provided each soldier with a daily gill of rum, whiskey, or brandy until 1838, when it substituted six pounds of coffee and twelve pounds of sugar per 100men for the liquor ration.
In the early 1840s, the average soldier serving in the northern states was reported sick once every 41/2 months, whereas in the middle and southern states he was ill once every 4 months. Serious epidemics rarely challenged surgeons assigned to long established forts along the Canadian border and the northern Atlantic coast, and they found it difficult even as late as the mid-1840s to raise official enthusiasm for long overdue improvements to hospitals or living quarters. Those caring for soldiers on the western frontiers, on the other hand, were often engaged in the struggle against disease. The combination of diarrhea and dysentery, the traditional camp disease, and malaria continued to scourge the Army.
The number of forts in the rapidly expanding nation grew as both white and red men moved west of the Mississippi, but the consequences of the Indian removal policy, and particularly of the Second Seminole War, added to the burden of some post surgeons in all parts of the country. A few post hospitals far from either Florida or the frontier cared for ill recruits or sheltered invalids returned from the southern fighting. One post representative of collection points for recruits was Madison Barracks at Sackett`s Harbor, New York, where the
30Quote from Ltr, Lawson to Russell (20 Jun 1844) RG 112, entry 2, 15:203; Ltrs, Lawson to Foot (21 June 1844), to John M. Cuyler (9 Jul 1844), to King, Simpson, and James R. Conrad (1 May 1845), and to other recipients, all in RG 112, entry 2, 15:210, 226, 486, 487, and 488-505, passim.
85
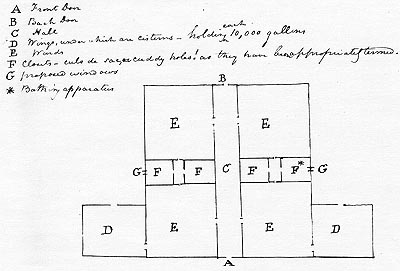
MADISON BARRACKS HOSPITAL, 22 April 1842. Thomas Henderson, Asst Surg. RG 112, ser. 12, box 301.
{kind=link}
surgeon was responsible for a large number of sick from among the unacclimated recruits. Housing there was dilapidated, and the post surgeon blamed the water for the high number of diarrhea cases. Among other problems afflicting both recruits and veterans were boils, skin infections, and scabies, as well as malaria, respiratory problems, and rheumatism.31
When no recruits were assigned to Madison Barracks for a brief time in 1840, the total number of men at the post fell well below 100, but by the fall of 1840, recruits were coming in again and the population was rising. By 1842, veterans of the Florida war were appearing there as well, bringing with them the fevers that plagued soldiers in the South. Within a few months of the end of the Second Seminole War, however, life at Madison Barracks was settling back into a pattern of few and generally mild illnesses, punctuated by occasional outbreaks of scarlet fever, which in some cases was severe.32
The facilities available for the patients of the Madison Barracks` surgeon were, like so many in the North, old and inadequate. They consisted of three rooms located at the far end of the enlisted men`s barracks. One room was used as a dispensary, the other two were used as wards. One ward was approximately 400 square feet and the second almost twice that, but chimneys took up much of the space in both. As a
31Surgeon`s Quarterly Rpts, Madison Barracks (30 Sep 1838-30 Sep 1845), all in RG 94, entry 634.
32Surgeon`s Quarterly Rpts, Madison Barracks (30 Jun 1840-30 Sep 1845), all in RG 94, entry 634.
86
result, the facility could hold only eighteen beds, two or three of which were regularly used by hospital attendants. On the basement level of this wing were two "matron`s rooms," a "bathing room," and a "kitchen and eating room."33
The post surgeon at Madison Barracks in 1838 emphasized that the rooms occupied by the sick there were never intended to be used as a hospital and so "of course [were] extremely defective in arrangements as well as in other important particulars." Among the defective arrangements were those for ventilation. Furthermore, in the surgeon`s opinion, hospitals should also be entirely separate from barracks. By 1839, however, the construction of a new and separate hospital, built of limestone and designed by the Surgeon General`s Office with modifications by the post surgeon, was underway. The main body of the building contained the ward for the sick, while a bathing room occupied one wing and a morgue a second. Only the site itself appears to have been criticized: it was judged too near a freshwater stream and too exposed to the wind during long winters. Furthermore, a steep ravine that lay between the hospital and the barracks made the hospital inaccessible during the heavy snows characteristic of that part of the country.34
The Quartermaster`s Department turned the new facility over to the surgeon in November, but some of the problems involved in housing the sick remained. Experience showed the new hospital at the Madison Barracks to be a mixed blessing. The planks used for the flooring were kiln-dried and poorly seasoned and, as a result, shrank rapidly. Because the building`s fireplace proved inadequate for heating, stoves had to be used; their installation appeared to aggravate the problem with the floors. The excessively dry floorboards rapidly absorbed any stains, so the post surgeon urged that they be painted, which he believed would solve all the difficulties he had been experiencing with them. The records, unfortunately, do not reveal whether this step was actually taken.35
At many of the northern posts along the Atlantic coast, damp casemates, the masonry rooms designed to contain cannon, continued to be the only shelter available for all those in the garrison, sick or well. As a result, the surgeon in the field might be preoccupied with the effects of such accommodations upon himself and his family as well as with their effects upon the soldiers. At Fort Hamilton in New York Harbor, for example, the post surgeon reported that he had spent $4,000 of his own money to have his personal quarters modified so as "to protect my own health and make myself and family comfortable and respectable." The hospital accommodations at this post were so poor that for several years patients were periodically taken to the new Fort Columbus facility nearby, but in the summer of 1845 the Army authorized the improvement of the hospital casemates. Nevertheless, and despite the surgeon general`s dislike for casemate facilities, the long-standing suggestion of the surgeon at Fort Hamilton that a separate hospital building be constructed appears to have been ignored.36
33Quotes from Ltr, Heiskell to Lawson (23 Feb 1839), RG 112, entry 12; Ltr, Heiskell to Lawson (I I Nov 1838), RG 112, entry 12.
34Quote from Ltr, Heiskell to Lawson (23 Feb 1839), RG 112, entry 12; Statistical Report, 1839-55, p. 39.
35Ltr, Heiskell to Lawson (22 Apr 1842), RG 112, entry 12.
36Quote from Ltr, Eaton to Lawson (13 Feb 1845), RG 112, entry 12; Ltrs, Eaton to Lawson (2 Jul 1842 and 10 Jan 1843) and Mower to Dr. Carpenter (21 Dec 1839), all in RG 112, entry 12; for details on similar conditions at Ft. Adams, R.I., see also Statistical Report, 1839-55, p. 10, and Ltrs, Lawson to Joseph G. Totten (16 Aug 1844), RG 112, entry 12.
87
At Fort Columbus, on Governors Island, the post surgeon, Joseph P. Russell, faced problems both with his quarters and with an influx of invalids from Florida. While Russell was serving in Florida early in the Second Seminole War, a major from the Corps of Engineers took over the quarters usually assigned to the fort`s post surgeon, rooms that had been modified for Russell`s use on the orders of the Medical Department. On returning north in November 1838, instead of being assigned to his usual quarters or even to those in which the post clerk was living, which were only slightly inferior to those of the surgeon, Russell was offered space he found entirely unacceptable. After Lawson appealed in his behalf to the secretary of war, urging that Russell be allowed to displace the clerk, the returning surgeon appears to have made no further complaints.37
A year later, Russell wrote to the surgeon general of his pleasure with the new post hospital nearing completion at Fort Columbus, adding that he hoped to furnish it with the new iron bedsteads. To this fine new hospital the Army shipped fifty-seven invalids from Tampa, Florida, in June 18 39 and either thirty-nine or forty-seven more- the sources are contradictory on this figure- from the Cedar Key hospital in 1840, by which time the hospital was presumably being used to train hospital stewards. The Cedar Key transferees arrived in such poor condition that Russell immediately wrote Lawson, complaining bitterly of the decision to send these men to his facility. Removing invalids from a warm climate to a cold one during the winter was "extremely injudicious, and ill advised." Furthermore, the vessel that carried them had been very uncomfortable, the weather during the voyage "boisterous," and the men at times drenched by bilge water. By the time they reached Fort Columbus, "they presented a most pitiable spectacle, were generally in a very filthy and lousy condition, two of them had involuntary and unconscious discharges, and were literally wallowing in their excrement."38
Russell protested further that his hospital could take only fifty patients without crowding and that the poor condition of the men arriving from Florida would be very bad for morale at a base where recruits were to be trained for duty in the Seminole wars, and would generally discourage enlistments. Any future victims of the Seminole wars, he asserted, should be sent to Fort Monroe in Virginia or to Fort Moultrie in South Carolina, where the climate was better and where there would be no new recruits to be horrified by the spectacle of what service in Florida could do to a man`s health. But the Florida invalids continued to pour in, seventy-three more from Cedar Key in late June 1841 and fifty-six from Pilatka in early July.39
A continuing health problem that grew to surprising proportions at Fort Columbus after the first invalids arrived from Florida was venereal disease. In December 1836 the post surgeon reported that 10 of the 120 men newly entered on his sick list in the past quarter were suffering from gonorrhea and 10 from syphilis (the records do not make it possible to guess how many of these patients might actually be suffering from
37Ltrs, Russell to MacKay (10 Dec 1838) and to Lawson (10 Dec 1838) and Lawson to Sec War (23 Dec 1838), all in RG 112, entry 12; Surgeon`s Quarterly Rpt, Ft. Columbus (31 Dec 1838), RG 94, entry 634.
38Quotes from Ltr, Russell to Lawson (29 Nov 1840), RG 112, entry 12; Ltr, Russell to Lawson (15 Dec 1839), RG 112, entry 12; Surgeon`s Quarterly Rpts, Ft. Columbus (30 Jun 1839 and 31 Dec 1840), both in RG 94, entry 634.
39Ltr, Russell to Lawson (29 Nov 1840), RG 112, entry 12; Rpts, Russell to Lawson (22 Jun and 7 Jul 1841), both in RG 94, entry 634.
88
both diseases). Two years later, the surgeon reported only 10 cases of venereal disease, but in the following June, nine days after the arrival of the 57 invalids from Tampa, the venereal disease case load figure stood at 14, this from a sick list totaling 433 for the quarter. Three months later, however, despite the fact that the total number of new cases of all kinds of diseases and wounds at that post had decreased by 67, 59 were newly recorded victims of gonorrhea and syphilis. Russell did not suggest how many of these might have been Florida veterans who had acquired a new problem in the course of celebrating their return to civilization. The venereal disease rate slowly dropped from this high point and reached its more customary level several months later.40
To the south of the New York forts, the health problems that had plagued such posts as Fort McHenry in Maryland and Baton Rouge during Lovell`s term as surgeon general appear to have been relieved before Lawson had long served in that position. Conditions at the Maryland post reached a nadir in the months immediately following Lovell`s death in the fall of 1836, and the post was subsequently abandoned briefly in 1837. When troops reoccupied it in 1838, the poor location and dilapidated condition of the old hospital inspired a quick start on a new one, a structure that greatly pleased the civilian surgeon assigned there. The retreat of malaria from the country`s more northern areas may have been responsible for an improvement in health at the Fort McHenry garrison. Although, during the winter months, soldiers on guard duty who went from the overheated guard room at Fort McHenry out into the cold air suffered considerably from head colds (or catarrh as it was then called), by 1844 the men at this post apparently considered it one of the most desirable assignments.41
At Baton Rouge, the new hospital was also finished in 1839, complete with brick walls, a much-admired system of ventilation, and a ten-foot-wide gallery around the entire structure. The fevers and digestive problems characteristic of southern posts continued to plague Baton Rouge, however, with the third quarter of the year being particularly unhealthy. In 1843, the weeks of the late summer and early fall were unusually difficult; yellow fever struck the post in September when the surgeon was already struggling to care for men transferred from Florida who were "worn out ... by Climate and Severe service- particularly Intemperance."42
Except for the influenza epidemic of 1843, the health of the garrisons at such northwestern posts as Forts Snelling and Mackinac, the latter in Michigan, remained good once the stresses and shortages related to their establishment were past. The surgeon at Fort Mackinac, however, like his colleague at Fort Hamilton, felt compelled to use his own money for improvements more appropriately made at the Army`s expense. Although the physician paid personally to have the hospital rooms painted,
40Surgeon`s Quarterly Rpts, Ft. Columbus (31 Dec 1836, 31 Dec 1838, and 30 Jun and 30 Sep 1839), all in RG 94, entry 634.
41Surgeon`s Quarterly Rpts, Ft. McHenry (1818-45, esp. Rpt, 31 Mar 1845), all in RG 94, entry 634; Ltrs, G. C. U. Roberts to unknown recipient (24 Dec 1836), Henderson to SG (1837), and Roberts to Benjamin King (10 May 1839) and to Lawson (30 Nov 1846), all in RG 112, entry 12; King to Sec War (30 Jan 1838) and to Thompson (21 Mar 1838), both in RG 112, entry 2, 9:141 and 183, respectively; French, Two Wars, p. 26.
42 Quote from Surgeon`s Quarterly Rpt, Baton Rouge (30 Sep 1843), RG 94, entry 634; Surgeon`s Quarterly Rpts, Baton Rouge (1822-45), RG 94, entry 634; Statistical Report, 1819-39, P. 254; Statistical Report, 1839-55, pp. 147, 254, 265.
89
in an attempt to start a fund to cover this sort of expense in the future, he asked each civilian treated in the facility to donate fifty cents tothe cause .43
Despite its grim beginnings, Fort Snelling had acquired an excellent reputation by 1836, and the early sufferings of its garrison were almost forgotten. Its garden was admired for its unfailing supply of vegetables, and scurvy was no longer a threat. In the opinion of an Army inspector in 1838, "No soldier ought to desire to live better than they have always done at this post." The post surgeon could not afford to relax his vigilance, however. Smallpox occasionally afflicted the Sioux Indians who lived near the fort, threatening any in the garrison who were not immune. After 1839, when alcohol became available for the first time in the vicinity of the post, the surgeon recorded that "The increase to our sick list is owing in my opinion to the introduction of Ardent Spirits amongst us." Many of the ills that came to the attention of the post surgeon at Fort Snelling, however, were of a type usually associated with long, cold winters. Colds and rheumatism were common, and some soldiers suffered from chronic bronchitis or chilblains, a painful engorgement of the fingers, toes, and earlobes caused by cold, damp weather. Army surgeons did not often encounter malaria in such a chill climate except when units already afflicted with this disease came to Fort Snelling.44
Unlike the reports of many post surgeons, those of George Turner at Fort Snelling separated the number of patients treated in their quarters from those treated in the post hospital. Turner usually hospitalized up to a third of his patients, or as many as eighty-six per quarter. Given the size of most post hospitals in relation to the length of their post sick lists, it is probable that most of those treated by post surgeons were outpatients.45
The forts located in or near the lands assigned to the tribes moving west from Florida, Alabama, and Georgia were not as healthy as Forts Snelling and Mackinac. The health record of Fort Gibson (located in Cherokee lands on the banks of the Grand River along the main emigrant route from St. Louis to Texas) was particularly miserable. In the sickly season every man on post might be ill more than once in a quarter. The Army did not abandon Fort Gibson, however, because the secretary of war believed that its existence was crucial to the Cherokees` security in their new lands. The infantrymen who shared the post with a detachment of dragoons were still sheltered in rotting, badly ventilated barracks when Lawson became surgeon general; perhaps because of the hope that the fort would soon be closed, authorities were loath to invest more money in its buildings. The occupants of the infantry barracks fell ill at a particularly high rate when the wind shifted to the southwest, from the direction of the bottomlands between the Grand and Verdigris rivers. Although the dragoon quarters were sheltered from the southwesterly winds by a ridge, they were exposed to the prevailing winds of summer, which also brought disease. During the last nine months of the year at Fort Gibson, malaria was the most
43Surgeon`s Quarterly Rpt, Ft. Mackinac (30 Sep 1843), RG 94, entry 634; Croghan, Army Life, p. 75.
44First quote, Croghan, Army Life, p. 66; second quote, Surgeon`s Quarterly Rpt, Ft. Snelling (30 Jun 1839), RG 94, entry 634; Ltrs, Lawson to Jones (18 Aug 1843), RG 112, entry 2, 14:275; John Emerson to Lawson (14 Dec 1838 and 26 Aug 1839), both in RG 112, entry 12; Jones, Citadel, p. 216; Surgeon`s Quarterly Rpts, Ft. Snelling (1836-45), all in RG 94, entry 634.
45Surgeon`s Quarterly Rpts, Ft. Snelling (31 Mar 1842 and 30 Jun 1843). both in RG 94. entry 634.
90
common illness, 700 or more cases developing in the course of a quarter. In addition, diarrhea increased the garrison`s miseries in the summer, while in the winter, respiratory diseases posed an additional problem.46
Because the post`s surgeons themselves also suffered from repeated attacks of disease, providing adequate medical care for the garrison, normally about 500 strong, was difficult. The Surgeon General`s Office tried briefly to insist that four surgeons could handle all the fort`s health problems, but in 1837 authorities realized that five would be better. Despite the recognized need for at least four to five surgeons, by June 1838 only three medical officers were present at Fort Gibson. In the winter of 1839, when there were approximately 540 men at Fort Gibson and 236 cases of disease reported for the quarter, only two surgeons were serving at the post, with the health of one "fast declining" and that of the other scarcelybetter.47
In the fall of 1839, when over 600 cases of disease were reported during the quarter, the medical staff once again consisted of only three men. When a contract for a civilian physician was presented to Lawson for his approval, however, he refused to allow the expense on the grounds that the Regular Army surgeons already at the fort should be able to handle the load. Struggling to provide an adequate medical staff for the troops fighting the Seminoles, Lawson refused to understand why a garrison of 483 officers and men should need so many doctors, noting that the 258 men at Fort Wayne, just sixty miles away, made do with the services of only one physician. To the secretary of war Lawson protested that in only eight months the commanders of the troops in Arkansas had spent over $3,000 for private physicians, in spite of the services of the five Regular Army surgeons sent west to care for the 1, 196 men at their four posts.48
By 1840 Lawson was willing to admit that, because of its poor location, Fort Gibson had proved for ten years to be "the most sickly military Post in the United States" and that the diseases there were often serious enough to cause death or the permanent destruction of health. His sympathy for the surgeons serving there, however, was limited. Typically, he looked for fault in their conduct. He admitted that assistant surgeon Joseph H. Bailey was of good character, but he deplored Bailey`s custom of spending much of his time and energy on his private practice, principally in caring for Indians, thereby neglecting both his duties at the fort and his own health.49
The surgeons at Fort Gibson were manning two hospitals, one for the infantry and the other for the dragoons, both of which
46Statistical Report, 1819-39, pp. 221-22; Statistical Reports, 1839-55, p. 267; Prucha, Sword, pp. 359-60-Surgeon`s Quarterly Rpts, Ft. Gibson (1836-46), ali in RG 94, entry 634; Ltrs, Lawson to Gales and to Seaton (both 8 Mar 1843), both in RG 112, entry 2, 1: 186 and 187, respectively; Wharton to King (6 Jul 1838), and to Lawson (13 Feb 1839), both in RG 112, entry 12; Francois des Montaignes, The Plains .... eds. Nancy Alpert Mower and Don Russell (Norman: University of Oklahoma Press, 1972), pp. 167-68.
47Quote from Ltr, Wharton to Lawson (13 Feb 1839), RG 112, entry 12; Surgeon`s Quarterly Rpts, Ft. Gibson (1837-39), all in RG 94, entry 634; Ltrs, King to Sec War (13 Dec 1836 and 25 Mar 1837) and Tripler to AG (7 Oct 1837), all in RG 112, entry 2, 8:134 and 278 and 9:10, respectively; Wharton to King (24 Jan 1838), Mills to King (27 Jun 1838), and Wharton to Lawson (15 Dec 1840), all in RG 112, entry 12.
48Ltrs, Lawson to Sec War (11 Nov 1839), RG 112, entry 2, 11:58-59; Wharton to Lawson (9 Jul 1839), RG 112, entry 12; Surgeon`s Quarterly Rpt., Ft. Gibson (30 Sep 1839), RG 94, entry 634.
49Quote from Ltr, Lawson to Sec War (30 Apr 1840), RG 112, entry 2, 11:312; Ltrs, Lawson to Lewis (27 Aug 1840) and to Bailey (4 Sep 1840), both in RG 112, entry 2, 11:500 and 12:15, respectively.
91
were inadequate. Because Lawson anticipated the abandonment of the post, he initially withheld his support from the campaign of these physicians to override the post commander`s unexplained opposition to the addition of two wards to the existing facilities. By May 1838, however, Lawson had agreed to the expansion. The commanding officer`s consent was then obtained, and before another year passed, one of the two new wards was completed and the old buildings were improved.50
One of the dragoon officers complained, however, that the custom of having the post`s physicians rotate between the two hospitals was not an ideal arrangement for the sick because the physicians never had the opportunity to know their patients as individuals. Presumably in answer to his complaint, sometime before the beginning of 1839, one surgeon at Fort Gibson was assigned to work exclusively at the dragoon hospital. When only two medical officers were at the post, however, the sickness of either rendered this arrangement less than ideal, because the patients of the sick physician were then cared for by a doctor who was completely unfamiliar with their problems. Although by 1840 Lawson had apparently capitulated on the matter of hiring a civilian surgeon, he believed that the most efficient approach to providing care for the post`s sick would be to combine the two hospitals in one building. His suggestion to this effect was ignored until later in 1840, when many of the dragoons appear to have left the post. The commanding officer then declared that the infantry hospital would function as a general hospital and shelter patients from all units represented at the post.51
At least two of the surgeons at Fort Gibson in the 1840s found it an appropriate post for further study of the use of quinine for malarial fevers. Charles McCormick, who had developed his approach to the treatment of malaria while he was in Florida, introduced to Fort Gibson the practice of treating malaria with large doses of quinine administered during the fever`s paroxysm as well as during its remission. The intermittent fevers affecting the men at Fort Gibson tended to return regularly at seven-day intervals, making it possible to administer quinine in anticipation of the attacks. Physicians discovered that by giving 10 grains of quinine twelve hours before the expected paroxysm and another 10 grains six hours later, they could prevent the fever`s return. They also learned that, for a febrile patient, 15 to 20 grains of quinine given as a single dose was effective, and its effectiveness was enhanced when it was repeated at four to six hour intervals thereafter, for a total of two to three days. Although physicians might also prescribe bleeding or even emetics and cathartics, fortunately for the patients, they found that usually no preparation was necessary for the administration of quinine.52
Although the demand for quinine at Fort Gibson was great, a hospital steward stationed there in the 1840s stated that "to protect the men from malaria, the government served a gill of whiskey daily to each man. "His comment may have referred to
50Ltrs, Mills M. Mason (copy, 11 Apr 1838), Mills to Lawson (14 Apr 1838), and Wharton to King (21 Mar and 6 Jul 1838) and to Lawson (13 Feb 1839), all in RG 112, entry 12; King to Wharton (25 Apr 1838) and to Mills (21 May 1838), both in RG 112, entry 2, 9:23 5 and 272, respectively; De Camp to Lovell (May 1836), RG 94, entry 634.
51Ltrs, Wharton to Lawson (12 May 1837 and 13 Feb 1839), Order, Arbuckle (no. 13, 21 Jan 1840), and Ltr, Wharton to Lawson (29 Jan 1840), all in RG 112, entry 12; Ltr, Lawson to Wharton (25 Jan 1840), RG 112, entry 2, 1:175.
52Coolidge, "Gibson," pp. 447, 449-50; Statistical Report, 1839-55, p. 267.
92
the time when a boat bearing a new supply of quinine sank on the Arkansas River, forcing the surgeons to rely on other medications. In any event, the number of men requiring medical attention doubled after the sinking, and deaths were prevented only by the reservation of the small remaining supply of quinine for those most seriously ill. Shortly after a new shipment of quinine arrived at the post, the patient population was back to normal.53
In the 1830s fevers were also a common affliction at Fort Leavenworth, Kansas, a base that grew in importance as increasing numbers of settlers moved west and greater numbers of Indians from east of the Mississippi arrived in the Oklahoma Territory and in Arkansas to the south of this post and in what later became Iowa to the north. The size of the garrison fluctuated as expeditions to establish peaceful relations with and among the Indians or to escort settlers or traders farther west came and went. The problem of providing these detachments with medical attention was a difficult one, especially during the years when so many surgeons were needed in Florida.54
Although the greatest consistent cause of disease at Fort Leavenworth was malaria, such disorders of the digestive system as dysentery and diarrhea were also common. A severe epidemic struck in the late summer of 1837, afflicting 260 men, or more than five times the number then suffering from malaria, out of a garrison whose average size numbered only 334. The 1843 influenza epidemic also reached Fort Leavenworth, bringing 153 men to the attention of the surgeons in the third quarter of the year. Many men also suffered from wounds and so-called contusions. One Fort Leavenworth surgeon, however, believed that most of the patients under his care could thank alcohol for their health problems, no matter what their symptoms might be. He added to his quarterly report of 31 December 1843 the assertion that "Nearly all the cases arise primarily from liquor." The surgeons` reports from Fort Leavenworth also hint at other vices in addition to alcoholism. In recording the discharge of a dragoon because of his "general debility," for example, another surgeon later noted, "This man destroyed himself with vicious secret practices."55
In the late 1830s, and especially in the third and fourth quarters of those years, the recorded number of cases of disease treated at Fort Leavenworth could exceed by as much as 80 percent the number of men in the garrison. Fortunately, not long after Lawson became surgeon general, a new hospital began to rise there; when complete, it was a "very capacious brick hospital, two stories high with every necessary appurtenance."56
Because it was not always possible to assign two or more surgeons to Fort Leavenworth, on at least one occasion a hospital steward provided the medical care for an expedition leaving that post. The detach-
53Quote from James D. Elderkin, Biographical Sketches and Anecdotes of a Soldier of Three Wars... (Detroit, 1899), p. 10; Statistical Report, 1839-55, p. 269; Coolidge, "Gibson," p. 450; Ltr, McCormick to Lawson (6 Oct 1844), RG 112, entry 12.
54Walton, George H. Sentinel of the Plains: Fort Leavenworth and the American West. (Englewood Cliffs, N.J.: Prentice-Hall, 11973]), pp. 48-49; Croghan, Army Life, pp. 10, 73; Ltrs, Macomb to Lawson (1 Apr 1838 and 3 Apr 1840), both in RG 112, entry 12.
55Quotes from Surgeon`s Quarterly Rpts, Ft. Leavenworth (31 Dec 1843 and 31 Dec 1845, respectively), both in RG 94, entry 634.
56 Quote from Croghan, Army Life, p. 73; Statistical Report, 1819-39, pp. 164-65; Aurora Hunt, Major General James Henry Carleton, 1814-1873: Western Frontier Dragoon (Glendale, Calif.: Arthur H. Clark Co., 1959), p. 97; Surgeon`s Quarterly Rpts, Ft. Leavenworth (1827-44), all in RG 94, entry 634.
93
ment of 11 officers and 200 men started out for the territory of the Osage Indians in the spring of 1838 without a physician because the surgeon did not believe that he should leave the post without a medical attendant. Two years later, shortly after a second physician finally arrived at Fort Leavenworth, the newly assigned surgeon left with a detachment ordered to establish a new post. Since his replacement had already been diverted to Florida, Fort Leavenworth was once again down to a single Army surgeon.57
By 1843 a second surgeon was once again on duty at Fort Leavenworth, but in June he, too, left the post, accompanying three companies of dragoons escorting traders to Santa Fe. The physician remaining at the post was temporarily handicapped in his work by a broken bone in his right hand. The bone apparently healed in time, but since the surgeon also suffered each winter from a "thoracic disease," in 1844 he was sent to Fort Jesup, Louisiana, after he had requested reassignment to protect hishealth.58
Another Fort Leavenworth expedition departed not long after the ailing surgeon left for Louisiana. Its goals were to effect a reconciliation between the warring Pawnee and Sioux and to create a favorable impression of the white man among them and the other Indian tribes living near the confluence of the Missouri and Platte rivers. The five companies involved, accompanied by a surgeon, set out in mid-August of 1843 but were scarcely on their way before men began to fall ill, twelve, it would seem, in the first twenty-four hours alone. The second day out of Fort Leavenworth, a private "fell from his horse in convulsions, and, although the surgeon was promptly in attendance, died in a few minutes." Less than two weeks later, yet another private died, "of Chronic Diarrhea with which he had been ill almost from the day of our departure from the Fort." By the end of August, many among the officers, men, and hired teamsters were sick; to the victims of disease were also added those of accidents and carelessness, bringing the total on the surgeon`s list to twenty four. Among the injured was a private who shot himself in the hand early in September, "such accidents from the Carbines ... not [being] of unfrequent [sic] occurrence in the Dragoons." When the sick and injured were unable to continue the journey by horseback, the surgeon had them placed in a hospital wagon, to complete the trip in this uncomfortable vehicle.59
Conclusion
In his attempts to provide adequate medical care for the soldiers at forts like Leavenworth and Gibson, as well as for those at posts scattered about the country, without neglecting the men fighting in Florida, Lawson was severely handicapped by the unwillingness of Congress to face the need for a significant increase in the basic size of the Medical Department. To compensate for the inadequate number of physi-
57 Ltrs, Macomb to Lawson (1 Apr 1838 and 3 Apr 1840), both in RG 112, entry 12.
58Quote from Ltr, Wharton to Lawson (4 Apr 1844), RG 112, entry 12; Ltrs, ibid. (3 Jun and 17 Oct 1843), both in RG 112, entry 12. It is interesting to note that Wharton anticipated the establishment of the Army Medical Museum by several decades. In a February 1841 letter to Lawson, he suggested that medical officers be required "to forward to your office, such specimens of Morbid Anatomy as may be revealed in the performance of their Duty.... Would not a few years produce a cabinet of specimens ... alike honorable to the chief & to the members thereor" Ltr, Wharton to Lawson (12 Feb 1841), RG 112, entry 12.
59C. Wharton, "The Expedition of Major Clifton Wharton in 1844," Kansas State Historical Society Transactions 16 (1923-25):273, 275, 281-82, 290, 293, 302, quotes from 275, 281, and 290, respectively.
94
cians at his disposal, Lawson drove his surgeons hard, raging at any subordinate who showed signs of submitting to weakness or discouragement and denying leave to all who were not seriously ill. He encouraged his surgeons fighting to have the importance of their contributions to the Army recognized. He worked to lighten their loads where he could by attempting to improve the facilities where they worked and by initiating a training program to enable stewards to assist the medical officers more effectively. When all else failed, Lawson hired contract surgeons. His supply system, inherited from his predecessor, functioned well; few surgeons complained of significant shortages. Although, unlike Lovell, Lawson leapt at the chance to go into the field, the men whom he appointed to act for him in his office were competent, and the medical service did not suffer from his occasional absences from the surgeon general`s desk.
Up until 1846, however, the Army Medical Department as organized in 1818 had been tested only in hostilities against Indians, fought between small units. The challenge presented in 1846 by the Mexican War would draw Lawson once again away from his office and into the field, where he would for the first time be in a position to direct personally the medical care of US Army units during a conventional war.
![]()