



Books and Documents > The Army Medical Department 1818-1865
CHAPTER 8
The Civil War, 1861: Many Problems, Few Solutions
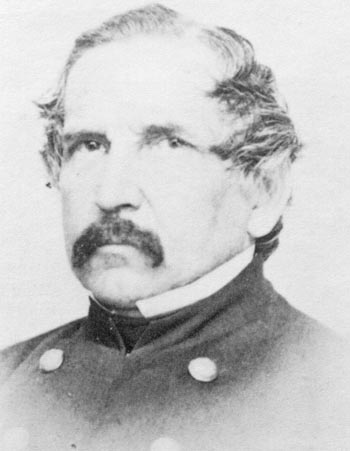
When Confederate guns began pounding Fort Sumter, South Carolina, on 12 April 1861, undoubtedly one of the least apprehensive men behind its walls was Assistant Surgeon Samuel W. Crawford. Taken from the same mold that produced Surgeon General Thomas Lawson, Crawford was more soldier than physician and eager for combat in which he could take an active part. He had led the rear guard of the unit abandoning Charleston`s Fort Moultrie in December 1860. Upon arriving at Fort Sumter, across the harbor from Fort Moultrie, he had volunteered to take his turn as officer of the day. Quickly familiarizing himself with the problems involved in defending Fort Sumter, he undertook the command of a battery during the bombardment. (Map 5) In spite of the fact that he was by then responsible for the care of the first four Union soldiers to be wounded by Confederate guns, Crawford also met Confederate representatives arriving at the fort on 14 April to discuss its surrender and conducted them to the fort`s commanding officer.1
The time was approaching when the professional demands on medical officers in wartime would be too great to permit them to play part-time active military roles as well. The care of thousands of patients, both sick and wounded, and the management of the various stages of their evacuation from battlefield to the hospital that completed their care would soon no longer allow a surgeon general to ride at his general`s side, as Lawson had done in the war with Mexico, or permit a medical officer the challenge of commanding a unit in battle. At Fort Sumter, however, where the casualties from the bombardment were few and their wounds slight, Crawford was still able to function successfully as both medical and line officer. The first fatal injury at the fort came only after the surrender, when at final ceremonies an accidental
1Primary sources, including Crawford`s own report and documents in the War Department`s War of Rebellion volumes, indicate that, contrary to statements in many secondary volumes, the Confederate bombardment of Ft. Sumter did produce Union casualties. Rpt, Crawford (12-14Apr 1861), RG 94, entry 634, hereafter cited as Crawford Report; War Department, The War of the Rebellion: A Compilation of the Official Records of the Union and Confederate Armies (Washington: Government Printing Office, 1880-1901),ser. 1, 1:12, 20-24, 62, 66-67 (hereafter cited as WOR); Paul E. Steiner, Physician-Generals in the Civil War: A Study in Nineteenth Mid-Century Medicine (Springfield, Ill.: Charles C Thomas, 1966), pp. 41-42, 44; A. Doubleday, Reminiscences of Forts Sumter and Moultrie in 1860-61 (New York: Harper, 1876), pp. 146, 166; Samuel Wylie Crawford, The Genesis of the Civil War: The Story of Sumter 1860-61 (New York: C. L. Webster & Co.,1887), pp. 430-70. Unless otherwise indicated, all material in this chapter is based on Brown, Medical Department, and Callan, Military Laws.
152
153
explosion of ammunition killed one man and hurt several others. These men were quickly evacuated, one to a Charleston hospital and the others to the North with the rest of the garrison. The summer after the surrender, Crawford announced his intention to resign from the Medical Department to become an infantry officer. In this capacity he rose to the rank of brigadier general during the war. Even after hostilities ended, he never returned to the practice of medicine.2
Administrative Problems of the Medical Department
Crawford was but one of many physicians to leave the Medical Department in the early months of 1861. Of 114 doctors serving at the time Fort Moultrie was abandoned, 24 resigned to join Confederate forces and 3 more were dismissed for disloyalty. Their departure left the Medical Department with a relatively small nucleus of experienced military surgeons around which it had to build a huge wartime organization.
SAMUEL W. CRAWFORD. (Courtesy of National Library of Medicine.)
{kind=link}
Even veterans of the Mexican War, however, had no concept of the difficulties that would be involved in dealing with casualties on the scale of those of the Civil War. Accustomed to handling the health problems of small and relatively isolated posts, old-time Army surgeons had never been called upon to develop plans for evacuating, hospitalizing, and caring for vast numbers of wounded and sick or for preventing disease in camps with populations of thousands. Because of the seniority system, the department`s initial responses to the Civil War were directed by "fogies," according
to George T. Strong, a contemporary familiar with their work- old codgers "paralyzed by routine habits acquired in long dealing with an army of ten or fifteen thousand and utterly unequal to their present work." Unable to accept the fact that their years of experience had taught them little that would be of value in the crisis, some of these "superannuated officers" on occasion also stood in the way of others more willing to innovate.3
The Medical Department`s most superannuated officer at the time of Fort Sumter`s surrender, Surgeon General Thomas Lawson, would soon no longer be contrib-
2Steiner, Physician-Generals, p. 44; Crawford Report; Ltr, Lewis A. Edwards to Crawford (19 Jul 1861), RG 112, entry2, 28:253.
3Quotes from George Templeton Strong, Diary of the Civil War,1860-1865, ed. Allan Nevins (New York: Macmillan Co., 1962), p. 181; U.S. Sanitary Commission (USSC), Sanitary Memoirs of` the War of the Rebellion(New York: Hurd & Houghton, 1867), p. 43.
154
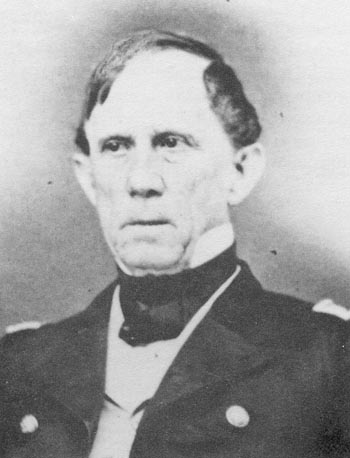
uting to the department`s problems. Apparently already ill when Confederate guns first fired on the South Carolina fort, Lawson died of apoplexy on15 May after fifty years in the Army and almost twenty-five as surgeon general. Unfortunately his aging successor, Clement A. Finley, was, as a contemporary put it, "utterly ossified and useless." Alread yin his sixties, Finley apparently had little to recommend him for so high a post except his forty years in the Army.4
CLEMENT ALEXANDER FINLEY. (Courtesy of National Library of Medicine)
{kind=link}
In the spring and early summer of 1861, a large group of younger surgeons with no military experience was rapidly gathering to join veteran Regular Army surgeons. Most of the new physicians were volunteers. Although Congress doubled the number of medical officers assigned to each of the forty volunteer regiments called up by President Lincoln in May, Surgeon General Finley considered one surgeon and one assistant surgeon per regiment still to be inadequate. Since state authorities often ignored the examination required for acceptance into the new volunteer force and a medical degree was nota prerequisite to service, the quality of the new physicians was as open to question as the quantity, and even homeopaths might be considered for positions as regimental surgeons.5
In July, in the process of approving the President`s call for troops, Congress added a requirement that brigades of three or four regiments each be organized and that the secretary of war assign each brigade a surgeon, who must have passed an exam "of practical character" administered by the Medical Department. The specific responsibilities of the brigade surgeon were not outlined at this time, leaving the medical director of each army or area to use his brigade surgeons as he wished. In practice the duties assigned these individuals were considerable, especially in view of the fact that many were young volunteers and at best familiar with Army routine only to the extent made possible by a few months of service as regimental surgeons. Those brigade surgeons who became medical directors when Regular Army medical officers were not available might be called upon for
4Quote from Strong, Diary, p. 181; Ltrs, Edward to W. T. Willard (15 May 1861), RG 112, entry 2,28:65; Wood to A Gand to Finley (both 18 May 1861), both in RG 112, entry 2, 28:75.
5WOR, ser. 3, 1:6 3 6; Ltrs, W. I. H. White to Joseph T. Howard(20 May 1861), Wood to P. W. Ellsworth (20 May 1861) and to Henry H. Smith(24 May 1861), Finley to Griswold (18 Oct 1861), and Wood to Gov Kirkwood(20 Nov 1861), all in RG 112, entry 2, 28:82, 83, and 102, and 29:9 and 120, respectively; "The Week," American Medical Times 3 (1861):224;Ltrs, J. D. S. Haslet and William Johnston to SG (both 13 Jun 1861), both in RG 112, Registers of Letters Received, 1862, entry 10:13.
155
advice on matters affecting the command`s health even though they were not likely to be authorities on either hygiene or sanitation.6
Regular Army surgeons, however, remained the backbone of the Medical Department. Whenever possible the positions of medical director and medical purveyor were assigned to them. Regulars with years of experience who were serving in the West were called east in the summer of 1861, their places to be taken by civilians. New regulars, both those replacing resigning physicians and the additional thirty for whom Congress called in August, were, however, as inexperienced as their volunteer counterparts, although their professional skills continued to be guaranteed by the examinations the department invariably administered to regulars.7
Contract surgeons, or acting assistant surgeons, and medical cadets were, for the most part, as lacking in military experience as volunteer and new regular surgeons. Contract physicians might have neither skill nor military background and were in some instances considered to be "charlatans and imposters" by their contemporaries. The creation of the position of medical cadet in the summer of 1861 represented a major innovation, since it made it possible for medical students eighteen to twenty-three years old to serve as dressers or ambulance attendants. Up to fifty of these young men could be signed on at one time and given the rank and pay of West Point cadets.8
To help in the care of the Army`s wartime patients, the Medical Department needed a larger group of hospital attendants and nurses that was usually available. Like the Department`s new physicians, many attendants were unfamiliar with the routine of military hospitals. Those detailed from the ranks might also be among the least fit of their units. Convalescents, who were familiar to some degree with hospitals, were sometimes found to be both physically weak and "inhuman in their treatment of patients."9
Many women were eager to serve as nurses, but it was an unusual candidate who had been given even the briefest of training, since nursing schools were few. Surgeon General Finley reportedly opposed the use of civilians and particularly the use of women. To bring order out of potential chaos as far as female nurses were concerned, the Army asked the formidable Dorothea Dix, already well-known for her work with institutions for the insane, to serve as superintendent of female nurses for the Army and to screen applicants for nursing positions. In August, however, Congress effectively undermined her position by ruling that surgeons in charge of hospitals could hire nurses without going through Superintendent Dix. Those women whom Dix found acceptable were plain of face and dress and over thirty years
6Quote from Ltr, M. I. Asch to J. Burd Peale(21 Oct 1861), RG 112, entry 2, 29:18; Ltrs, Wood to George G. Shumard(21 Jun 1861) and Finley to U. Goldsmith (3 Jul 1861), 28:183 and 213, respectively; John H. Brinton, Personal Memoirs of John H. Brinton, Major and Surgeon U.S.V. 1861-1865 (New York: Neale Publishing Co.,1914), pp. 18, 54, 62-63.
7Ltrs, Wood to Finley (27 Apr 1861) and to McCormick (6 May1861), both in RG 112, entry 2, 28:14 and 38, respectively.
8Quote from Brinton, Memoirs, pp. 65-66; Ltrs, Wood to Finley (27 Apr 1861) and to McCormick (6 May 1861), both in RG 112, entry 2, 28:14 and 38, respectively; William Quentin Maxwell, Lincoln`s Fifth Wheel: The Political History of the United States Sanitary Commission(New York: Longmans, Green, & Co., 1956), p. 62.
9Quote from Mary Ashton Rice Livermore, My Story of the War: A Woman`s Narrative of Four Years of Personal Experience (Hartford, Conn.: A. D. Worthington & Co., 1889), p. 127.
156
of age. The Army forbade female attendants to accompany units on the march or to work in regimental hospitals and paid them 40 cents a day plus a ration each, a sum roughly half of that paid male civilian nurses hired to care for military patients.10
Not all Army surgeons looked forward to the assistance of female nurses. A medical journal of the day stated that female nurses were often "a useless annoyance," lacking the physical strength needed to help wounded men. The article also suggested that its readers try to "imagine a delicate refined woman assisting a rough soldier to the close-stool, or supplying him with a bedpan. . ." Some admitted, however, that when aided by orderlies or convalescents, female nurses could serve a useful purpose, since they were more attuned to the emotional needs of the sick and more skilled at "sanitary domestic economy."11
In the Regular Army, the hospital steward, who before the war often added the role of nurse to his other duties, had by 1861 gained a position commanding considerable respect. Only men who could establish their competency as apothecaries were accepted for the required five-year enlistment. These men also served as wound dressers and were paid almost twice as much as female nurses, whose role, like that of all nurses, was seen as menial. Medical students sought positions as stewards through which they could gain experience in their chosen fields. In volunteer units, regimental surgeons followed the old custom of choosing their stewards from their own units, one being allowed for each battalion.12
Expansion and organizational changes affected the Department`s facilities as well as its personnel. The widespread network of post and regimental hospitals that supported the peacetime Army could never have been adequate to handle the vast numbers of sick and wounded that would result from the Civil War. To handle the overflow of patients from regimental hospitals, the Medical Department reinstituted the general hospital on a much larger scale than ever before. The first need for this institution developed in Washington, D.C., when more than 600 artillerymen and engineers were ordered to that city in January and early February 1861. By the end of January, Lawson had ordered the establishment of the first general hospital to care for the sick of units then in the capital and for any that might be sent through in the following weeks. With the advent of hostilities, the Medical Department started setting up more such facilities in Washington. Medical directors in other areas also began to establish general hospitals to shelter those who had to be left behind when their units were on the move. Realizing that they should act ahead of actual need, directors attempted to prepare these facilities before patients were actually waiting to enter them.13
10WOR, ser. 3, 1:262, 308, 398, 421;Ltr, Wood to Cuyler (11 Dec 1861), RG 112, entry 2, 29:15; Sylvia G. L. Dannett and Katherine M. Jones, Our Women of the Sixties (Washington: U.S. Civil War Centennial Commission, 1963), p. 9; Isobel Stevenson, "Nursing in the Civil War," Ciba Symposia 3 (1941-42):921-22; Helen E. Marshall, Dorthea Dix, Forgotten Samaritan (Chapel Hill: University of North Carolina Press, 1937), pp. 217-18.
11First and second quotes, "Duties of the Army Surgeon-Female Not Suitable for Nurses," American Medical Times 3 (1861):30; third quote, "Female Nurses in Military Hospitals," American Medical Times 3 (1861):25.
12Ltrs, W. I. H. White to E. Kissler (14 May 1861) and to J.C. Bucher (21 May 186 1), Wood to Ellsworth (20 May 1861), and Edwards to John S. Powell (21 Aug 1861), all in RG 112, entry 2, 28:61, 83, 85-86, and 354, respectively.
13Ltr, Edward to Satterlee (29 Jan 1861), RG 112, entry 2, 27:605;RG 94, Register of Hospitals, entry 554; Constance McLaughlin Green, Washington, Village and Capital, 1800-1878 (Princeton, N.J.: Princeton University Press, 1962), p. 233; WOR, ser. 3, 1:23.
157
Regimental hospitals with their tents and equipment continued to accompany units on the march. Having sent back to a general hospital men unable to march at the time the unit broke camp, the regimental surgeon cared for the wounded during and after battle wherever he could, sometimes in a ravine or under a tree. He often established his hospital in a house near the battlefield and pitched his tents nearby to take in those the building could not accommodate. During a battle that produced more casualties than regimental facilities could handle functioning as isolated units, the medical director might call for the creation of a temporary field hospital, manned by regimental surgeons. In certain instances this officer also permitted the creation of a brigade hospital, operated under the immediate supervision of the brigade surgeon. Regarded as a consolidation of regimental hospitals, they were in actuality something of a hybrid between the regimental and general hospital, more permanent than the former but less so than the latter.
Men assigned to hospital duties in regimental facilities were also expected to manage the evacuation of the wounded, a task they shared for a time with members of the regimental band. Only twenty-five men were available in both categories in each regiment since the regulations permitted the assignment of no more than ten men per regiment to work as hospital attendants. The secretary of war rejected all offers from outside the federal government to provide ambulance companies. Initially none of the men from the regiment were trained in the management of ambulances and stretchers, and as a result an occasional surgeon or medical director undertook to
14 Maxwell, Sanitary Commission, p.76; "Duties of Brigade Surgeons," American Medical Times3 (1861):282-83; War Department, SGO, Medical and Surgical History ofthe War of the Rebellion, 2 vols. (Washington: Government Printing Office, 1870-88), 1, app.: 10- 11 (hereafter cited as MSH).
15 Ltrs, Wright to Lawson (8 Mar 1861), RG 112, entry 12; Edwardsto Robert Landreth, to A. Orvis, and to John M. Maisch (all 27 Apr 1861),all in RG 112, entry 2, 28:15; Finley to L. Thomas (2 Aug 1861), RG 112,entry 2, 28:298; Frank H. Hamilton, A Treatise on Military Surgery and Hygiene (New York: Balliere Bros., 1865), p. 44.
158
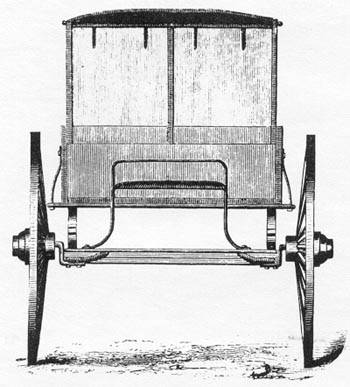
FINLEY AMBULANCE, FRONT VIEW, from illustration in Medical and Surgical History.
{kind=link}
join volunteer regiments. Many were soon sent home, and others "left he service irregularly," especially after the first battle of Bull Run in the summer of 1861. Only in August 1861 was examination by a surgeon actually required and even then the order was often flagrantly ignored.16
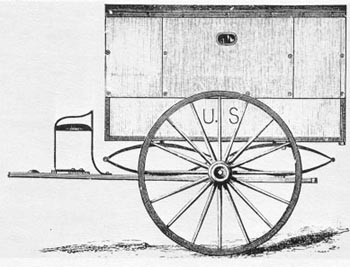
FINLEY AMBULANCE, SIDE VIEW, from illustration in Medical and Surgical History.
{kind=link}
Many recruits came from isolated areas, where they had never been exposed to measles and the other ordinary communicable diseases of childhood. In the camp where they were first received, as well as in the much larger ones to which they progressed, all were exposed to contagious diseases of many kinds. Furthermore, accustomed to having their clothes washed, food cooked, and quarters kept clean by wives or mothers, recruits were quite helpless when it came to maintaining high standards of hygiene and sanitation in the Army. Department doctors, who complained that their own ambiguous rank and the resultant lack of prestige crippled their efforts to have line officers enforce strict rules, blamed this lack of hygiene and sanitation for much disease. Veteran soldiers, who maintained higher standards, also suffered from such diseases associated with faulty sanitation as typhoid, diarrhea, and dysentery. The sick rate of the entire army in the last six months of 1861 exceeded 30 percent, with digestive complaints the greatest source of illness and typhoid the principal cause of death.17
In their effort to prevent the spread of disease, medical officers emphasized the dangers of overcrowding. Twenty or more
16 First quote, Sanitary Commission, Memoirs, p. 44; second quote, Ltr, Finley to F. Coakley Vanderpool (2 Nov 1861),RG 112, entry 2, 29:65; Maxwell, Sanitary Commission, pp. 31-32;MSH 1, app.:47.
17MSH 1, pt. 1:296-300; Brinton, Memoirs, p. 61;Maxwell, Sanitary Commission, pp. 71, 73; Joseph Janvier Woodward Outlines of the Chief Camp Diseases of the United States Armies (1863. Reprint. New York: Hafner Publishing Co., 1964), p. 9; William Howard Russell, My Diary, North and South, ed. Fletcher Pratt (Gloucester, Mass.: Peter Smith, 1969), p. 196; Sanitary Commission: Report of the Resident Secretary, "American Medical Times 3 (1861):60-61; Strong, Diary, p. 203n.
159
men often shared only 1,100 cubic feet of air in the Sibley tents used as shelters in the first months of the war, but even in barracks, which were usually hastily erected, overcrowding was a problem. Wet camp sites, overwork and exposure, and even poor blankets were also blamed for much illness. A civilian familiar with Army life maintained, however, that sending a soldier`s pay directly to his wife or to a savings account would significantly improve the Army`s health by making it impossible for him to buy "bad pies and rotgut whiskey."18
A potential cause of disease that received little attention early in the war was the Army`s defective diet. In the summer, when fresh fruits and vegetables were easy to find, the soldier usually had an adequate diet if he was stationed near a good source of supply or permitted to live off the land. Those in authority considered the basic Army ration to be "all sufficient for the men," but the potato was its only source of vitamin C. In the summer of 1861, Congress passed a bill adding fresh vegetables or their equivalent to the diet, but the equivalent was apparently dried vegetables, which required long cooking to be palatable. Furthermore, transportation for an adequate supply of any form of vegetable was hard to find and commanding officers sometimes failed to take the need for vegetables seriously. Soups were favored as a way of serving meats, but the recommended recipes called for hours of cooking, which undoubtedly destroyed the last traces of this perishable vitamin in potatoes and any other vegetable that might find its way into the pot. Scurvy was already appearing by the end of 1861,even though it takes some weeks or months to make its appearance in men whose supply of vitamin C has previously been adequate.19
To care for the large numbers of both sick and wounded that characterized the Civil War, a far more complex system than that existing in peacetime was necessary to provide medicines and hospital supplies, especially since the troops were often on the move. New York City remained the principal supply center, but medical purveyors opened additional depots at appropriate sites over the nation, including Baltimore and Cairo, Illinois. Minor depots were set up near large camps, preferably near railroads or water transportation and, if possible, near a market. Field purveyors accompanied armies on the march, obtaining supplies at the nearest depot and issuing them asneeded.20
The amount of supplies actually on hand when the war began was small, and the size of the Army was growing rapidly. The manufacture of the various items that were needed was time consuming. Buyers turned to contractors who might be interested only in a profit without regard to the dictates of patriotism. As reports came in about hospitals without either clothing or bedding for their patients, buyers became desperate, profiteers began to thrive, and fraud became common. Large amounts of cloth
18Quote from Strong, Diary, p. 85; Maxwell, Sanitary Commission, p. 34; Woodward, Outlines, pp. 46-47;MSH 1, app.:1
19Charles S. Tripler and George C. Blackburn, Handbook for the Military Surgeon (Cincinnati: Robert Clark & Co., 1861), pp.13-14, quote from p. 12; Maxwell, Sanitary Commission, p. 58; "Duties of the Army Surgeon . . . " "Sanitary Commission: Report of the Resident Secretary," and "The Week," all in American Medical Times 3 (1861):30, 91, and 107-08, respectively.
20Ltrs, Wood to Tripler (30 May 1861) and to J. H. Bailey (10 Jun 1861) and Edwards to J. S. Bobbs (18 Oct 1861), all in RG 112, entry 2,28:116 and 142 and 29:42, respectively; King to Finley (23 Aug 1861), RG112, entry 12; MSH 1, pt. 3:964; Huston, Sinews, p. 174.
160
had to be purchased from abroad. Surgeons sometimes lacked even a complete supply of instruments, and a physician who wanted those of the most modern design might have to furnish them himself.21
Medicines were not always a problem in the early months of the war. Many new regiments were initially supplied by the state from which they came, but others had to draw upon the Medical Department`s purveyor. When he could not contact a purchasing officer of his own department, the medical officer had to obtain medicines through the Subsistence or the Quartermaster`s Department. Many volunteer doctors further complicated the problem of supplying medicines by their failure to appreciate the advantages of limiting the variety bought. Some had favorite potions that were not to be found on the department`s supply table, a document to which few additions were made when it was revised in the summer of 1861. Surgeon General Finley insisted that no unlisted items could be distributed without his personal approval.22
Slow transportation, complex ordering procedures, and the efforts of well-intentioned civilians also complicated medical supply. Delays forced medical officers to buy locally, and citizens added to the confusion by donating items that were not necessarily needed. Ambulances and many items involved in the building and equipping of military hospitals had to be obtained through the quartermaster, which added further complexities to the Medical Department`s operations.23
Surgeons made ingenious attempts to stretch the Department`s resources. They sold the bones and fat from the meat fed to patients, for example, as well as stale bread, old newspapers, and similar items, and used the proceeds to buy whatever they believed to be of general benefit, such as books for the hospital`s library, daily papers, magazines, and even musical instruments. The Medical Department received credit on Subsistence Department books for unused rations. At those hospitals where the produce of gardens or fish caught by convalescents could be added to the facility`s larder, the amount in this so-called hospital fund could be significant. The sum was used to add special items to the diet, and at one hospital it also paid the salary of a professional cook whose skills resulted in considerable savings to the hospital by eliminating waste.24
While the varied demands of the early months of the war almost overwhelmed the Medical Department, many patriotic groups attempted to help in the care and feeding of Union soldiers. Their aid at first tended to be haphazard and inefficient, but not long after the war began and with Medical Department encouragement, a group of private citizens, one of whose leaders was a former Department surgeon, created an organization designed to coordinate efforts to aid the sick and wounded and to prevent disease. The U.S. Sanitary Commission was a less powerful but more pervasive version of a commission that had aided British soldiers during the Crimean War, and its work was officially approved
21Ltr, Satterlee to Wood (22 May 1861), RG112, entry 12; Huston, Sinews, pp. 179-80, 184; John Shaw Billings, "Medical Reminiscences of the Civil War," Transactions of the College of Physicians of Philadelphia, 3d ser., 27 (1905):114-15.
22Ltr, Finley to Med Dirs (11 Nov 1861), RG 112, entry 2, 29:95;SOs, Thomas (no. 232, 28 Apr 1861), RG 112, entry 57.
23Ltrs, Wood to L. Thomas (20 May 1861), RG 112, entry 2, 28:78;Laub to McLaren (11 Jun 1861), RG 112, entry 12; Courtney R. Hall, "The Lessons of the War Between the States," in History of American Medicine, ed. Felix Martin-Ibanez (New York: MD Publications, 1959),p. 73.
24MSH 1, pt. 3:959.
161
by President Lincoln and his first secretary of war, Simon Cameron.25
Within the War Department, opinions of the Sanitary Commission varied. Although he wished its power to be less than that of the British Sanitary Commission in the Crimea, Acting Surgeon General Robert C. Wood had encouraged its formation in the spring of 1861. Surgeon General Finley accepted its help, although apparently with reluctance, but Lincoln`s second secretary of war, Edwin Stanton, opposed it. Some Medical Department members believed that the need for supplies as perceived by the commission was only apparent and that it resulted almost entirely from the ignorance of volunteer surgeons, who asked for more than they really needed. As late as December 1861, departmental opposition to the commission was so strong that a commission official was moved to comment that it was a "pity that [the] Bureau will neither do its official duty nor permit volunteers to help it without throwing filth at them.26
Whether welcomed or not, the Sanitary Commission attempted to help the Medical Department with both advice and material aid. Its advice in the early months of the war was wide ranging. It urged more exacting physical exams for recruits, the creation of a nurse corps, an increase in the rank of members of the Medical Department, and greater attention to sanitation and disease prevention. It outlined a system to be used to determine the order in which patients were treated during and after battle and recommended the specific instruments and supplies a surgeon should take into the field.27
The more tangible assistance that the Sanitary Commission offered the sick and wounded, including prisoners of war, was as varied as the topics on which it offered advice. It provided papers, pens, and volunteer scriveners to write letters for those unable to do so, and supplied dressing gowns, slippers, and reading material. It appealed to the public for donations of wine, spirits, mosquito netting, flannel, sheets, and ice. Its surgeons followed the army into the field and brought with them ambulances, wagons loaded with stores, anesthetics, and surgical instruments. Its inspector kept watch over camp and hospital conditions. In time the Sanitary Commission even established a hospital directory by means of which relatives could determine the location of any individual patient. It supplied quinine when Finley delayed his decision to order it for prophylactic use in northern Virginia. Officials of the U.S. Sanitary Commission might provide lint for wound dressings, food, and even a hospital on short notice.28
The U.S. Sanitary Commission was not the only civilian organization of its kind that attempted to assist the Union Army with its wounded. Both the Western Sanitary Commission and the Christian Commission also operated along similar lines. The former was established in the summer of 1861,in large measure at the instigation of Maj. Gen. John C. Fremont, and functioned west of the Mississippi much as its counterpart, the U.S. Sanitary Commission, did in the east. Since the U.S. Sani-
25WOR, ser. 3, 1:225, 258-59, 308; Strong, Diary, pp. xxxvii, x1viii, 150; Neil Cantlie, A History of the Army Medical Department, 2 vols. (Edinburgh: Churchill Livingstone,1974), 2: 144-45.
26Strong, Diary, p. 15, quote from p. 198; "The Sanitary Commission," North American Review 98 (1864):163,168.
27Maxwell, Sanitary Commission, pp. 31-32, 74-75, 114; Stevenson, "Nursing," p. 921; USSC, Sanitary Memoirs 1:16,24-25.
28Maxwell, Sanitary Commission, pp. 5 5, 71, 79, 81, 295-96, 305, 307; Mary Livermore, My Story, pp. 131-32.
162
JOHN CUYLER.(Courtesy of National Library of Medicine.)
{kind=link}
tary Commission did not entirely restrict its activity to the East, there was conflict between the two organizations. They encountered many of the same difficulties in working with Army surgeons, some of whom gladly accepted their help and some of whom were determined to do without it. Although the main concern of, the Christian Commission was the spiritual welfare of the soldier, members of this organization also wrote letters, set up diet kitchens to provide special foods for hospital patients, and performed similar functions. As a result, the U.S. Sanitary Commission tended at times to regard the Christian Commission as yet another rival.29
Both the U.S. Sanitary Commission and the Medical Department broke new ground on a large scale in the first months of the Civil War. East and west of the Appalachians, medical directors were often forced to experiment and improvise. In each area of the country where there was military activity in 1861, the medical director was forced to solve the problems he encountered with little, if any, assistance from the surgeon general. Despite the lack of central direction, the senior surgeon of the Medical Department for each army or area found it necessary to establish general facilities to shelter those whose wounds or diseases were likely to keep them hospitalized more than a few days, to attempt to systematize evacuation when his supply of ambulances was inadequate and his attendants untrained, and to supervise subordinates who were often inexperienced in military medicine.
Care of the Sick and Wounded in the East
Medical directors of units serving east of the Appalachians found, long before year`s end, that their relative proximity to the surgeon general gave them few, if any, advantages. Surgeon General Finley was jealous o fhis own powers and prerogatives, but his support of members of his department was ineffective.
Perhaps the first medical director to discover how little he could rely on Finley was John M. Cuyler, a 27-year veteran of the
29Brinton, Memoirs, p. 48; Report to the Western Sanitary Commission on the General Military Hospitals of St. Louis, Mo. (St. Louis, 1862), p. 4; Jacob Gilbert Forman, The Western Sanitary Commission. A Sketch of Its Origin, History, Labors ...(St. Louis: R. P. Studley & Co., 1864), pp. 7-8, 16-17; Jack D. Key, William Alexander Hammond, M.D. (1828-1900) (Rochester, Minn.: Davies Printing Co., 1979), p. 19: Maxwell, Sanitary Commission, pp. 104,19 1; Western Sanitary Commission, Report of the Western Sanitary Commission for the Year Ending June 1, 1863 (St. Louis: Western Sanitary Commission,1863), p. 1.
163
Medical Department assigned to manage the medical care of soldiers in the Fort Monroe-Newport News area of Virginia. Cuyler was in a very difficult situation in the summer of 1861, caught between an inadequate surgeon general and an overbearing commanding general, the arbitrary Maj. Gen. Benjamin Butler. When Butler sent some of his units on an ill-conceived and ill-executed operation intended to eliminate a Confederate battery at Big Bethel, Virginia, physicians with his command were already struggling with a measles epidemic, and a general hospital had been opened to ease the strain on existing facilities. Furthermore, Cuyler had no ambulances. After the Big Bethel effort ended in fiasco, Butler apparently assumed that Cuyler`s organization could not provide care for his fifty-three wounded. He took over a hotel in the area, including its supply of bedding, and called in his family physician, Gilman Kimball, at that time a contract physician at the Army hospital in Annapolis, Maryland, to head the command`s general hospital. In so doing, Butler caused the surgeon general considerable dismay. The Annapolis hospital was left without a physician when Kimball joined Butler, which he did against Finley`s expressed orders. Kimball`s arrival, accompanied by several assistants, was not explained to Cuyler, who acquiesced in Kimball`s takeover of the hospital because he had no alternative.30
Kimball`s care of his patients may have been adequate- no complaint on this score has been found- but his departure in August 1861 revealed further evidence of his lack of appreciation for the way in which the Medical Department operated. While in office he had attempted to charge the Department for items it did not normally supply. After he left, Cuyler discovered that Kimball had also neither kept a record of expenditures and receipts nor collected a hospital fund. Despite his exasperation over the entire affair, Finley apparently later permitted Kimball to attain the position of brigade surgeon and to be reassigned from a position in the Western Department in order once again to join the politically powerful Butler.31
Unlike Cuyler, William S. King, Brig. Gen. Irvin McDowell`s medical director in northern Virginia, experienced no conflicts with his commanding officer, but the support he received from the surgeon general was as weak as that given his colleague at Fort Monroe. King, a 24-year veteran of the Medical Department, was handicapped by the fact that he had arrived in Washington from New Mexico and been assigned to McDowell`s force only a few days before it started south toward Manassas and the first battle of Bull Run. A high disease rate was already predictable, for camps were generally filthy. Latrines were inadequate, and the men were too unfamiliar with military life to see the need to use them. Seemingly undaunted, King set to work at once to do what he could to prepare for the coming operation. On 16 July, the day that McDowell`s army started south, King set up a general hospital in a former boarding school in Alexandria and
30RG 94, entry 544, Register of Hospitals; Ltrs, Edwards to Cuyler (19 Jun 1861) and Finley to G. Kimbal (19 Jun 1861),to E. D. Townsend (24 Jun 1861) , to Thomas (6 Jul 1861), and to Townsend(12 Jul 1861), all in RG 112, entry 2, 28:175, 175-76, 192, 232, and 309,respectively; Cuyler to Finley (17 Jun , 9 and 25 Jul, and 13 Dec 1861)and to Butler (copy, 4 Jul 1861), all in RG 112, entry 12; SOs, Thomas(no. 149, 3 Jun 1861), RG 112, entry 57; "Camp Butler" and "The Week," both in American Medical Times 3 (1861):64 and 79, and 222-23, respectively; WOR, ser. 1, 2:82, 85.
31Ltrs, Finley to Butler (17 Jul 1861) and to Thomas (4 and 23 Oct 1861), all in RG 112, entry 2, 28:245 and 485 and 29:29, respectively; Cuyler to Finley (18 and 21 Aug 1861), both in RG 112, entry 12.
164
requisitioned twenty more ambulances. Finley approved the order, but his initials upon it did not guarantee the delivery of the vehicles. One of the assistant surgeons working in his office apparently concluded that, since the order did not bear McDowell`s signature and since some ambulances had recently been delivered to the general`s headquarters, the new vehicles were not needed.32
When McDowell`s 34,000-man army began its march, King had had no time to train ambulance attendants or to devise plans for evacuation and hospitalization. Apparently unaware of the serious nature of these omissions, King decided to stay at McDowell`s side as much as possible in the belief that he could thus coordinate ambulances and "give a comprehensive supervision of officers connected with the medical department of the army, and see that the wounded were being attended to by the regimental officers." This approach had not worked particularly well for Surgeon General Lawson in the war with Mexico, and it was not likely to prove a good one when applied to an army more than three times the size of General Scott`s and to a group of physicians, most of whom lacked military experience of any kind. McDowell preferred to be at the head of his troops, and thus King was in a poor position, given the state of communications of the period, to advise his surgeons or coordinate their efforts. Moreover, there was no one below him in the medical hierarchy whose responsibility it was to supervise the work of the volunteer surgeons, who were unsure how to go about even such simple matters as ordering more supplies.33
This lack of preparation initially showed itself during and after a skirmish at Blackburn`s ford on 18 July, when an estimated 10 Union soldiers were killed and another 33 wounded, according to King, and others were felled by the heat-the total killed, wounded, and missing was later set at 83. Regimental surgeons gathered their patients for treatment wherever they could; at least one spot chosen proved too hot, and patients had to be moved. Troops fleeing in panic and blocking the roads hindered evacuation from the field. King made no attempt to establish a hospital himself until he saw ambulances coming in from the field with the wounded and the victims of heat exhaustion and realized that regimental surgeons could not handle the situation unaided. Troops coming through earlier, however, had drawn the wells dry in the Centreville area and the water supply at the hospital King`s aide had hastily set up there, two miles from the battlefield, proved in adequate. Physicians who were sometimes confused about their responsibilities also caused problems; one doctor refused until ordered to care for patients from units other than his own. McDowell failed to establish a guard for the hospital and mobs of soldiers wandered through the buildings, searching for friends and food. King finally succeeded in restoring order, once he left McDowell`s side, but only after "a great amount of exertion." After two days he was able to procure ambulances to evacuate those who could be moved east to Alexandria but the seriously injured were left behind to be captured by the enemy.34
32RG 94, entry 544, Alexandria, Va.; SOs, Asst AG (no. 178, 5 Jul 1861), RG 112, entry 57; Ltrs, King to Finley (13 and16 Jul 1861), both in RG 112, entry 12; Wood to McCormick (6 May 1861),RG 112, entry 2, 28:38; USSC, Documents of the U.S. Sanitary Commission(New York, 1866), vol. 1, no. 17:3-6.
33Quote from WOR, ser. 1, 2:309; MSH 1, app.:3,9; Ltr, King to Finley (16 Jul 186 1), RG 112, entry 12.
34MSH 1, app.: 1-5, 8, 17, quote from 2; MSH 2,pt. l:xxxv; WOR, ser. 1, 2:305, 309, 721; Russell, Diary, p. 213; S. Emma E. Edmonds, Nurse and Spy in the Union Army (Hartford: . S. Williams & Co., 1865), pp. 34-35.
165
By 20 July, the shortage of supplies was beginning to worry King. Twenty wagons with Medical Department supplies had been left behind in order not to impede the march, but King had requested that more supplies be sent by rail from Alexandria to the Fairfax station. Finley granted the request, but never made the shipment. Possibly because of King`s harrassed state of mind, he did not anticipate a full scale battle on the 20th, and, as a result, the scenes enacted after the skirmish at Blackburn`s ford were repeated on a larger scale, with supplies low and ambulances still toofew.35
Although McDowell himself heeded King`s advice that the men no longer be rushed because of the heat, his officers continued to push their soldiers, and doctors once again found themselves caring for the victims of heat exhaustion. Just before the two armies actually clashed, King realized that a facility to supplement regimental hospitals would once more be necessary. He placed the new hospital in the church at Sudley, where water supplies were adequate. Some by ambulance and many apparently on foot, patients soon came pouring into the various facilities, including those set up at King`s orders at Sudley and Centreville, as well as the regimental hospitals. Apparently neither King nor anyone else made any attempt to relate the number of physicians at any one hospital to the number of patients, who came in at random. Two hundred or more wounded eventually received treatment at Centreville and 300 of the remaining 900 were cared for in the Sudley church and other buildings nearby. Many of the less seriously wounded managed to reach Washington on their own, while many others lay on the field or in the shade of trees and bushes. Surgeons generally worked where they pleased-those who wished to work on the battlefield took their saddlebags with them to care for those who had not been moved to shelter.36
After the battle, fleeing soldiers and their equipment once again blocked the path of ambulances that were attempting to evacuate the wounded north to safety. When the Union flight was halted at the Potomac River, King returned south with ambulances, hoping that the victorious Confederates would allow him to retrieve his wounded still lying on the battlefield, but they would not. All the casualties that McDowell`s army left behind, either on the field or in hospitals, were taken captive. With them were captured a number of Union surgeons, five of whom had volunteered to remain with their patients at Sudley. The enemy permitted two Union physicians to take over a farmhouse and its outbuildings to use as a hospital although they had few supplies and the rebels could not provide them. At least one captured surgeon helped load Union wounded on trains for the long and agonizing trip to Richmond. Trains with wounded had low priority on the tracks and thus might not reach the Confederate capital for days, during which time those in the boxcars suffered for lack of food and care.37
35Ltrs, King to Finley (16 and 20 Jul 1861),both in RG 112, entry 12; MSH 1, app.:2.
36Ltr, King to Thomas W. Fry (26 Jul 1861), RG 112, entry 12;MSH 1, app.:5-8; WOR, ser. 1, 2:418; Maxwell, Sanitary Commission, pp. 19-20; W. W. Keen, "Surgical Reminiscences of the Civil War," Transactions of the College of Physicians of Philadelphia, ser. 3, 27 (1905):96; William 1. Sherman, Memoirs of General William T Sherman, by Himseff 2 vols. (New York: D. Appleton & Co., 1875),1:185; Louis C. Duncan, "The Battle of Bull Run," in The Medical Department of the United States Army in the Civil War (n.p., [ 1912-14]),pt. 2, pp. 10- 13, 17, 20.
37 Ltr, W. H. King to Finley (23 Jul 1861), RG 112, entry 12; MSH 1, app.:4, 7-8; WOR, ser. 1, 2:345, 416, 421.
166
The custom of not classifying medical officers as prisoners of war, which according to military historian Louis Duncan had existed to some extent in Europe for three hundred years, had apparently been forgotten since Napoleon`s time. Nevertheless, all the surgeons who were taken prisoner in the aftermath of the first battle of Bull Run were eventually released. Confederate Brig. Gen. Pierre G. T. Beauregard was strongly in favor of releasing them as soon as possible. Some were allowed to go before mid-April1862, but at least one was held captive in South Carolina for a year.38
The battle of Bull Run was a great shock to military and medical experts alike. The U.S. Sanitary Commission denounced the lack of advance planning for the care of the wounded, some of whom had been left for long periods unattended on the field. The lack of a coordinated system of evacuation had also forced many who could walk to drag themselves back to Washington unaided. The Surgeon General`s Office maintained that the number of physicians in attendance in the District of Columbia was more than adequate, but beds must have been in short supply, since the wounded and their ambulances were forced to wander the streets of the city, trying to find one of the four general hospitals there that would take them in. The new hospital at Alexandria was not yet entirely ready to receive patients; on 21 July it held but 26 of the 175 it was hoped it would eventually be able to accommodate. In the closing months of 1861, however, the Medical Department was at least aware of what it was facing and was preparing to meet future challenges .Large numbers of sick as well as wounded were a distinct possibility since typhoid deaths were increasing in Washington general hospitals. Fortunately, the Medical Department, realizing also that the poor sanitation of many barracks in the city was threatening not only their occupants but also the entire community with disease, began urging increased sanitation.39
When Maj. Gen. George B. McClellan was brought in to replace McDowell, Surgeon Charles Tripler, apparently a favorite of old General Scott, came in to serve as McClellan`s medical director in August 1861. Reported to be an "energetic, spasmodic, crochety, genial" soul, Tripler had been serving in the Medical Department since 1830. Since he had been giving a course of lectures on military medicine at the Cincinnati Medical College, the problems involved in caring for sick and wounded soldiers up to 1861 were fresh in his mind.40
Tripler was apparently not afraid of the task that lay ahead of him. At a time when sweeping changes were necessary, however, he was not s much an innovator as an administrator. He saw many inadequacies in the operations of the department in the area defended by the Army of the Potomac, among them deficiencies in sanitation, hy-
38MSH 1, app.:7-9; Duncan, Medical Department, pt. 2, pp. 16, 18-19. Duncan to the contrary, evidence exists that the English took French medical officers prisoner in the Napoleonic wars: Richard L. Blanco, Wellington`s Surgeon General. Sir James McGrigor(Durham, N.C.: Duke University Press, 1974), p. 134.
39MSH 1, pt. 1:60-62, app.: 1-9; Maxwell, Sanitary Commission, pp. 20, 88; Ltrs, Thomas R. Shelton to Finley (21 Jul 1861)and King to Finley (7 Aug 186 1), both in RG 112, entry 12; Wood to Joseph K. F. Mansfield (16 and 19 May 1861) and to A. N. McLaren (20 May 1861),all in RG 112, entry 2, 28:70, 76, and 77-78, respectively; Irwin, "Notes," p. 120
40Quote from Strong, Diary, p. 181; see also Ltr, Finley to Thomas (3 Aug 1861), RG 112, entry 2, 28:302; SOs, Williams (no. 25,13 Aug 1861), RG 112, entry 56; Tripler and Blackburn, Handbook; Eunice Tripler, Some Notes of Her Personal Recollections (New York: Grafton Press, 1910), pp. 127, 13 1. Unless otherwise indicated, all material on Tripler is based on MSH 1, app.:44-52, and WOR, ser. 5:76-113.
167
giene, and disease prevention; evacuation and hospitalization; and the competence of volunteer surgeons, but attempted to deal with them along entirely orthodox lines. Many of the problems were departmental and more appropriately the province of the surgeon general, but Finley apparently made no effective attempt to deal with them.41
Tripler recognized that some of the difficulties experienced by the Medical Department resulted from the incompetence of a few volunteer surgeons and the inexperience of many more. He called a board to examine physicians of questionable skills and ordered that from then on such a board examine any medical officer whose competence had been questioned. Tripler also decided to place his brigade surgeons in authority over regimental surgeon of their brigades. Then, by instructing the brigade surgeons about the measures he believed necessary to preserve the Army`s health and requiring them to be responsible for the medical officers under them, he was able to spread his doctrines downward despite the large number of surgeons involved.
Tripler hoped to inculcate in his subordinates the principle of avoiding general hospitals whenever possible. Tripler was aware that the general hospital was necessary to receive patients from an army on the move, but, like so many of the old-time surgeons, including King, he retained his dislike for an institution that took a patient far from his unit and appeared to delay his return to it. He also maintained, however, that "there was no authority for any hospital establishment in the vicinity of divisions or brigades, that might relieve the hospital tents if crowded" and still keep the men near their units. Tripler moderated his negative stance on such facilities only enough to allow brigade hospitals to exist as "aggregations of regimental hospitals.42
CHARLES TRIPLER.(Courtesy of National Library of Medicine.)
{kind=link}
Tripler recognized that general hospitals were a necessary evil. He believed that the capital`s supply of 2,000 hospital beds would have to be expanded. In a report apparently written a year later he maintained that he had specifically urged 20,000 beds as a minimum goal and that the U.S. Sanitary Commission had been willing to settle for a smaller number, but a commission spokesman, in recalling the same debate,
41Ltrs, Edwards to Byrne (15 and 18 Jul 1861)and Finley to AG (18 Jul 1861), all in RG 112, entry 2, 28:240-41, 249, and 250-51, respectively; SOs, Thomas (no. 193, 19 Jul 1861), RG 112, entry57; "Army Hospitals," American Medical Times 3 (1861):125.
42Quote from MSH 1, app.:48, 49; Ltr, King to Finley(7 Aug 1861), RG 112, entry 12.
168
reversed the figures and maintained that it was Tripler who was willing to settle for less than 20,000. Although Tripler was apparently successful in systematizing admission to these institutions, in his attempt to increase the number of beds available he encountered frustration, much of which came, directly or indirectly, from Surgeon General Finley.
Tripler was concerned with the quality as well as the quantity of the new hospitals being opened to serve the Army of the Potomac. He favored creating new hospitals from the ground up rather than taking over old buildings, but designs suggested to him by the Sanitary Commission were so expensive that eventually he had to settle for only two such structures. The buildings that were available for his use as hospitals were often outstanding examples of inappropriate design: halls were narrow, provisions for toilet and bathing facilities woefully inadequate, cellars damp and undrained. In some instances, dirt-retaining carpets still lay on the floor. Ventilation was invariably inadequate and bad odors often filled the rooms. Windows were both too small and too few, wards were too small to provide the desired amount of air per patient, and even beds were often of poor quality. Not surprisingly, erysipelas appeared in some of the Washington and nearby Georgetown hospitals at this time.43
Finally forced to accept the fact that even with strong Sanitary Commission support he would not be able to establish a network of completely new military hospitals in the capital area, Tripler continued his search for buildings suitable for hospital use in locations both in and around the capital. Not long after the end of the year, his efforts finally brought the total number of beds available for military patients in the Washington area to 6,000. He planned to move patients from Washington to such cities as Annapolis, Baltimore, and Philadelphia as promptly as possible so as to keep beds in Washington free for new patients.44
Tripler`s efforts to open hospitals in nearby cities to relieve the pressure on those in the capital area brought him into open conflict with the surgeon general, not because of any substantive issue but rather because Finley apparently resented his subordinate`s success and influence. The secretary of war had initially informed Finley that the surgeon general was directly in charge of general hospitals in the area of the Army of the Potomac, but Tripler, with McClellan`s backing and little consideration for Finley`s sensibilities, went blithely about his own schemes. The secretary of war eventually granted McClellan the right to proceed as he saw fit with the establishment of new hospitals, and such was Tripler`s position as McClellan`s medical director that McClellan`s victory was Tripler`s victory. Tripler and Finley remained at odds.45
Finley apparently kept a jealous eye on Tripler`s work in the fall of 1861, and when Tripler attempted to report to him about his search for suitable buildings in Philadelphia to serve as general hospitals for patients moved from Washington, the surgeon general flew into a rage. Cutting his subordinate off short, Finley charged that Tripler had not paid his superior the courtesy of notifying him of what he was doing in Philadelphia, that he was putting McClellan up to giving orders that humil-
43"Army Hospitals" and "The Week," both in American Medical Times 3 (1861):127-28 and 153,respectively.
44Strong, Diary, p. 186; RG 94, entry 544; Ltr, Wood to Kennedy (12 Sep 1861), RG 112, entry 2, 28:429.
45"Army Hospitals," American Medical Times(1861) 3:128; Strong, Diary, pp. 183-84.
169
iated the surgeon general, and that he was trying to upstage the surgeon general by locating more space for hospitals outside the District of Columbia than was needed, in view of Finley`s own efforts in this regard. Allowing Tripler no chance to explain himself, Finley berated him in the presence of a third party and then ordered him from the room. Tripler lost little time in placing charges against Finley, and on 6 December, a court-martial was called to consider the case. On 10 December, the surgeon general was charged officially with "Conduct unbecoming an officer and a gentleman" and "Conduct to the prejudice of good order and Military Discipline." The case was never tried, however, because Finley successfully raised the question of whether the general in chief, McClellan, was empowered to dismiss a bureau chief. Finley retracted such of his language as had offended Tripler, and the matter rested. Since the Sanitary Commission was by this point in full cry after Finley and since the question of the surgeon general`s competence was being debated in the public press, the charges placed against Finley and dismissed on a technicality probably contributed to the erosion of his position .46
Finley was not the only frustration in human form that Tripler had to endure. Volunteer help flocked to the hospitals, and not all of it was welcome. From Tripler`s point of view, his hospitals were full of civilians who considered themselves better able than he to manage them. "Sensational preachers, village doctors, and strongminded women" all "obtruded their crude suggestions." Competent nurses were too few rather than too many. Triple wished to have one nurse for every ten patients, but at the Kalorama facility, where contagious cases were isolated, for example, at one time only two nurses were responsible for 106 patients. Such attendants were generally either well-trained lay nurses, male and female, or members of one or another religious order.47
Not the least of the problems that Tripler faced when he became medical director of the Army of the Potomac was that of evacuation. Since he was not responsible for the choice of the fragile two-wheeled ambulance and was scarcely likely to be able to wean Finley away from his own design, one that he apparently attempted to patent, Tripler`s complaints were largely useless. He pointed out that 110 of the 228 two-wheelers issued by the Quartermaster of the Army of the Potomac in the three-month period that began July 1861 had "disappeared," statistics that to him indicated "reckless use." Tripler obtained an order ending the practice of using ambulances as taxis. This order may have been obeyed, since as of 31 December 1861, 314 of the Finley design ambulances and 71 four-wheelers were functioning in Washington and one two-wheeler was functioning with each regiment in the field.48
Convinced of the need for another method of evacuation to manage the removal of men lying in areas inaccessible to ambulances and apparently assuming that Finley would do nothing about the problem, Tripler began experimenting with a litter that could be attached to the back of a horse or mule. The initial model he tried was, at 140 pounds, too heavy, but Tripler
46Quotes from Court Martial Charges (10 Dec 1861), Records of the Judge Advocate General, Proceedings of Courts Martial and Courts of Inquiry, RG 153, box 2893, 11547; SOs, Thomas (nos. 322 and 327, 6 and 13 Dec 1861), both in RG 112, entry 57; Strong, Diary, pp. 183-84, 186, 190.
47Quote from Irwin, "Notes," p. 12 1; Maxwell, Sanitary Commission, p. 52; "Army Hospitals," American Medical Times 3 (1861):127-28; WOR, ser. 3, 1:636.
48Quote from MSH 1, app.:49; Maxwell, Sanitary Commission, p. 75; Hamilton, Treatise, p. 166.
170
continued to try different models in his search for one that could be used to replace the two-wheeled ambulance. Although the problem of the proper vehicle in which to transport the wounded remained, attempts to train attendants led to some improvement. Surgeons serving in the Poolesville, Maryland, area drilled their attendants in evacuation techniques and organized them by brigades to achieve greater efficiency. In October, McClellan ordered that all ambulance attendants take part in hour-long drills six times a week under the direction of regimental surgeons.49
Disease prevention was also one of Tripler`s major concerns. Some of the diseases that were beginning to plague the Army of the Potomac were preventable by medical means, others by improved sanitation and hygiene. Tripler learned that many soldiers serving under McClellan had not been vaccinated against smallpox. He ordered the situation remedied and attempted to require that thereafter all recruits be vaccinated before they left their assembly points. Finding the results of this campaign not entirely satisfactory, he ordered brigade surgeons to inspect all men and to immunize those in need of it. His efforts must have been successful, for in the first seven months he was in office there were but 168 cases, most of which had already been contracted before the victims entered the Army.
Since malaria was a major threat to the Army`s health, Tripler was intrigued by a report of one of his surgeons that it could be prevented by the ingestion of quinine in whiskey. The regulations did not recognize this remedy, and so Tripler turned to the Sanitary Commission to obtain the necessary ingredients. When the potion seemed successful, he managed to persuade Surgeon Genera Finley to issue it to those regiments most threatened by malaria. Tripler continued to receive favorable reports of the concoction and eventually ordered that supplies be kept on hand at all times.
In yet another effort to prevent disease, Tripler moved to improve living conditions, both for hospitalized soldiers and for those in the field. He assigned three medical officers to serve as field hospital inspectors and urged an end to the practice of using tents over submerged foundations to shelter soldiers in the field. He was also concerned with the design and heating of tents. Above all he urged upon surgeons and commanding officers alike "the paramount importance of hygienic morality."50
A certain amount of disease was, of course, inevitable. Measles, the scourge of new units, did not pass the Army of the Potomac by, and both malaria and typhoid appeared despite precautions. In October and November, among approximately 130,000 men, almost 8,000 cases of fevers of all kinds developed, with 1,000 described as typhoid. Although Tripler regarded typhoid as endemic in the United States, he also believed that many diagnoses of typhoid were in error. In December, alarmed at the high disease rate, General McClellan appointed three medical officers to serve on a committee to investigate the nature of the prevailing diseases. Their conclusion was that malaria was taking the highest toll but that typhoid was definitely present. Nevertheless, al-
49Maxwell, Sanitary Commission, p. 76;Duncan, "Pope`s Virginia Campaign," in Medical Department, pt. 3, p. 6; "Duties of Brigade Surgeons," American Medical Times 3 (1861):282-83; MSH 1, app.: 10-11.
50Quote from MSH 1, app.:47. These were not the first field hospital inspectors to serve in the East, since at least one was apparently serving in the Hagerstown, Md., area earlier in the summer. It is not known, however, whether he was appointed by Finley: Order, Asst AG Porter (27 Jun 1861), RG 112, entry 56.
171
though the number of cases of disease in the Army of the Potomac rose from 8,000 in July of 1861 to greater than 35,000 in December, the disease rate was falling, from 45 percent in July to 30 percent in September and then to slightly more than 23 percent in December.51
Tripler and the surgeons under him were struggling to find ways in which the Medical Department could meet the sudden and overwhelming demands that the new conflict placed on the medical service of the Army of the Potomac without altering the department`s basic structure. Though their efforts showed some success, they were handicapped in their attempts by factors beyond their immediate control. Both volunteer soldier and volunteer physician knew little as yet of the requirements of military life, stockpiles of supplies grew slowly, and, above all else, the great numbers of men joining the armed forces created overwhelming medical problems. Much time would be required to resolve these shortcomings, not only for the Army of the Potomac, but for all Union armies.
Care of the Sick and Wounded in the West
Military engagements to the west of the Appalachians took place on a smaller scale than the battle of Bull Run and thus, although disease took a growing and appalling toll, the number of wounded to be cared for after any single battle was relatively small. Even the battle of Wilson`s Creek, Missouri, caused only two-thirds as many wounded as Bull Run. Distances were great, however, and the campaigns lacked the sharp focus of those in the East. Action tended to take place far from any large and secure city where sufficient numbers of appropriate houses might be available to serve as general hospitals. Transportation became critically important and medical directors tended to set up general hospitals in cities convenient to major railroads or rivers. The patient load of general hospitals in the West was great even though some surgeons refrained from sending patients from regimental hospitals to these facilities until they were dying, a custom that tended to revive the old fear of general hospitals.52
JOSEPH J. B. WRIGHT. (Courtesy of National Library of Medicine.)
{kind=link}
In western Virginia and along the Ohio River, Union forces under McClellan and his successor, Brig. Gen. William S. Rosecrans, fought to uphold the independence of those who refused to join the eastern
51MSH 1, pt. 1:30-35 and pt. 3:364-72;Ltr, Finley to AG (4 Dec 1861), RG 112, entry 2, 29:167.
52Irwin, "Notes," p. 121; Maxwell, Sanitary Commission, p. 56.
172
portion of the state in secession. In the spring of 1861, the medical director for McClellan was Joseph J. B. Wright, to whom fell the responsibility for organizing the medical care of the troops in the Department of the Ohio. The regiments in the area were so newly called up that one of Wright`s first duties was to provide hospital supplies for them, a task he was able to complete quickly with the aid of the New York City purveyor. Because so many of these men were in poor condition when they joined the Army, Wright anticipated a need for general hospitals to serve the sick among them and hoped to locate these facilities at several different sites, from West Virginia westward.53
Wright questioned whether the hospitals that sheltered disabled merchant seamen in Cincinnati and Pittsburgh would be worth using for casualties. The hospital in Cincinnati was already available to volunteer patients, but despite its 100 to 150 bed capacity, it held only 15 to 30 men. He finally decided that the rising disease rates of late summer and fall made reliance on regimental hospitals and the homes of patients who lived in the Cincinnati area unrealistic. The arrival of wounded from various engagements that fall made Wright`s need all the more imperative. By October patients were pouring into Cincinnati by the hundreds, some from engagements in western Virginia whence they traveled much of the way by boat. Volunteer surgeons sent on many patients from Ohio who wished to be near their homes. Wright`s staff in Cincinnati was too small to handle the heavy case load, and malingerers were turning up in significant numbers. His problems, like Tripler`s, were only made worse by "scores, if not hundreds of officious & meddle-some women, & equally officious men, all of whom claim to have the direction of the Hospital." Some of these busybodies were undoubtedly drawn to the hospital by vivid newspaper stories about the sufferings of the wounded in poorly administered hospitals. Nevertheless, Wright also wrote the surgeon general of his indebtedness to the citizens of Cincinnati, whose charitable donations helped meet hospital expenses, and to that city`s physicians, who donated their time to help the Medical Department staff.54
Before his reassignment to St. Louis in the fall of 1861, Wright was also called upon to establish general hospitals near the battlefield in West Virginia. At Rich Mountain in July, for example, he set up a temporary field hospital in a three-story house and in tents pitched nearby. He also set up a general hospital in the town of Beverly, seven miles from Rich Mountain, both for the wounded from Rich Mountain and for those that came in a few days later from the engagement at Carrick`s ford. In this facility, five assistant surgeons cared for both Union and Confederate soldiers, on an equal but usually separate basis.55
Wright believed that, on the whole, his patients in the Department of the Ohio had been well cared for, despite what he apparently deemed the hopeless military ineptitude of his volunteer surgeons and
53Ltr, Wright to Finley (6 Jul 1861), RG 112, entry 12; SOs, Thomas (no. 139, 23 May 1861), RG 112, entry 57; MSH1, app.: 13. The way in which the area west of the Appalachians was departmentalized changed as the war progressed. The Department of Western Virginia, for example, was removed from the Department of the Ohio in September 1861 and added to another department in 1862, while the Department of the Cumberland lasted only from August to November 1861: MSH 1, pt. 1:74.
54Quote from Ltr, Wright to Finley (15 Oct 1861), RG 112, entry12); see also Wright to Finley (2, 9, and 21 Aug, 22 Sep, and 14 Oct 1861),all in RG 112, entry 12; MSH 1, app.:14; SO, Thomas (no. 139, 23 May 1861), RG 112, entry 57.
55MSH 1, app.:13, 14.
173
Finley`s failure to send him the ambulances he needed. Although the men for whom he was responsible were fighting in a primitive country far from supply centers, and supplies were limited, no serious shortage developed, even of such difficult-to-transport items as anesthetics. Surgeons were apparently able to use freely either chloroform or chloroform mixed with ether and did so with complete success, without anesthesia-related deaths. Wright recalled later that he had had "improvised ... ambulances insufficient number" from "light two horse spring wagons" bought at McClellan`s order. The evacuation of patients from Rich Mountain to the Beverly general hospital three days after the battle went well, although Wright admitted that part of the credit had to go to smooth roads and good weather.56
In the fall of 1861, the Surgeon General`s Office ordered the opening of yet another general hospital in the Department of the Ohio at Louisville, Kentucky, a unit that was to be staffed by contract physicians. By this time the Medical Department had assigned Robert Murray (who would serve as surgeon general from 1883 to 1886) to replace Wright. Murray set up his headquarters in Louisville and asked the surgeon general to appoint one of the assistant surgeons working in Cincinnati as medical director of that area so that he could focus his own efforts upon Louisville. By the end of November, a measles epidemic had struck in that part of Kentucky and the two general hospitals Murray had established in Louisville were both crowded. Two more hospitals were being prepared for opening, and plans were underway to set up still more, but meanwhile 100 men were in temporary rooms in the town and 400 more sick in camp. With 50,000 men in the field and more coming in, the situation was not likely to improve. Moreover, Murray was having difficulty hiring contract surgeons at $100 a month, the maximum he was permitted to offer.57
To the west of the Department of the Ohio were 23,000 men who would on 25 July come under the command of Maj. Gen. John Charles Fremont. Until August there was little action in Missouri and most of the sick of Fremont`s new command were cared for in regimental and post hospitals near St. Louis. Medical Director Samuel De Camp hastily set up the first general hospital in that city, located on a major railroad, the first week in August. After first accepting and then rejecting the smaller and "miserable, filthy Marine [merchant marine] Hospital," De Camp finally chose for his general hospital a new building with a capacity of more than 500. Only a few days later, Brig. Gen. Nathaniel Lyon and his 5,000 men left their camp near Springfield, Missouri, to attack the enemy near Wilson`s Creek, and their disastrous defeat brought the first significant number of wounded to the hospitals of General Fremont`s command.58
Lyon`s medical system was loosely organized in the summer of 1861, with no medical director to coordinate the work of the sixteen physicians who served within the command. The men who served as ambulance drivers and attendants had received no training. Ambulances and tents were in short supply. The number of ty-
56MSH 1, app.: 13, quotes from 14; MSH2, pt. 1:xxxv; Ltrs, Horace R. Wirtz to Finley (19 Dec 1861) and Wright to Finley (1 Jun 1861), both in RG 112, entry 12.
57Murray to Finley (28 Nov, 1 Dec, and 26 Dec 1861), all in RG 112, entry 12.
58Quote from Ltr, De Camp to Wood (25 Jul 1861), RG 112, entry12; Ltrs, De Camp to Finley (2 and 15 Aug 1861), both in RG 112, entry12; Report to the Western Sanitary Commission, pp. 3-6; SO, Asst AG (no. 13, 31 Jul 1861), RG 112, entry 56.
174
phoid and dysentery cases began increasing in August at about the same time that approximately forty men were wounded in a "smart skirmish. "Lyon now ordered a volunteer doctor to establish a general hospital in Springfield where his headquarters was located, since regimental facilities could no longer accommodate all his sick. The doctor selected an unfinished building originally intended to serve as a courthouse and chose at least one other medical officer, a Regular Army assistant surgeon, to serve with him there.59
On 9 August, Lyon ordered his command to leave camp near Springfield and to prepare to attack the enemy along Wilson`s Creek. The battle the next day was fierce, lasting six to seven hours. In the disastrous defeat that ensued, Lyon himself was killed, and the loss in dead and wounded was second in 1861 only to the casualties at Bull Run. But two vehicles, both "large spring wagons drawn by six mules," were available to remove the more than 700 wounded. Those who could walk were cared for in a ravine, and many of those who could not remained on the battlefield overnight. Most of the casualties were eventually brought to Springfield, and about 200 joined the rest of Lyon`s battered force in their 110-mileretreat from Springfield to Rolla, Missouri, whence they went by train to hospitals at St. Louis. One medical officer present at the battle of Wilson`s Creek believed that had Lyon appointed a medical director, 90 percent of the wounded could have been cared for and evacuated before the retreat began.60
The wounded who could not join the retreat were sheltered in the general hospital at Springfield, where seven Union doctors remained with them, but most of the men serving as nurses joined the retreat to Rolla. When Confederates took possession of Springfield the following day, they quickly made off with the hospital supplies and medicines that Union forces had left behind for their own wounded. The enemy preempted all available transportation, and a week was needed to retrieve all Union wounded from the battlefield. Although $5,000 had been left with Union surgeons for the purchase of supplies and food for their patients, no medical supplies were available. Surgeons did somehow manage to perform many operations, which was fortunate since conditions had not been favorable for surgery at the battlefield.61
The defeat at Wilson`s Creek placed an added burden on a hospital system already strained by increasing numbers of patients with typhoid, measles, pneumonia, and diarrhea, diseases that spread all the more rapidly because of the poor sanitation that characterized many of the camps in Fremont`s command. Those of Lyon`s casualties who had joined the retreat from Springfield to Rolla eventually arrived in St. Louis, where they were joined in time by the wounded who had been taken captive. A month after the defeat, the contending armies began a gradual exchange of wounded prisoners that was not completed until November. Taking advantage of the nearby railroad, surgeons sent most of these patients in boxcars 110 miles on new, unsettled, and bumpy track back to St. Louis, where hospitals were generally not highly regarded. Wounded from an engagement at Lexington, Missouri, in September also turned up at St. Louis. All available wards, including some in St.
59Quote from MSH 1, app.: 15.
60MSH 1, app.: 16, 17, quote from 16; From Sumter to Shiloh: Battles and Leaders of the Civil War, new ed. (New York: Castle Books & A. S. Barnes & Co., 1956), p. 306.
61Ltr, Edward C. Franklin to De Camp (16 Aug 1861), RG 112,entry 12; MSH 1, app.:16-17.
175
Louis charity hospitals, took in military patients, and even the charity hospitals were soon full to overflowing. To make matters worse, patients were coming in from crowded hospitals in other parts of Missouri and even from Cairo, Illinois, where the sick were too numerous for local hospitals to handle. De Camp opened a hospital for smallpox victims on an island in the Mississippi River and another for measles victims. He had smaller hospitals opened at intervals along the rail line in Missouri from Sedalia and Rolla to St. Louis and took over a steamboat to use as a hospital ship. He freed beds in the city by sending convalescents to camps outside the city. The Western Sanitary Commission began outfitting railroad cars for the sick and provided equipment for many of the hospitals, supplemented Medical Department supplies, and even opened its own hospital in a rented five-story building, where patients were cared for by an Army staff.62
By December of 1861 the condition of the 2,000 patients in St. Louis hospitals was outraging civilian observers, who reported the deaths of fifty-six patients in one week. A gentleman familiar with the St. Louis situation wrote the secretary of war that the Army`s hospitals there were" in a miserable, dirty, filthy and disgraceful condition" and that entry into them meant "certain death." The mortality varied, of course- from 26 October to 2 November, for example, only thirty-four died. Horrible as the rate may have seemed, it was perhaps to have been expected, since only the sickest patients were likely to be sent to general hospitals. The mortality was not significantly worse than that in the general hospitals of the East, where 151 of the little more than 2,000 patients died in December. This rate was actually lower than that in general hospitals of the entire central region, where 8 percent of the patients died during the last month of 1861.63
The story at many other hospitals in the West was much the same as that in Cincinnati and St. Louis. Crowding was frequent and inadequate housing common, as could be seen at the facility set up in Jefferson City, Missouri, to care for 500 men who broke down as Fremont drove his men hard to makeup for a string of defeats. This hospital was housed in an old seminary, two taverns, and a private home. Many windows were broken in these buildings, and some patients had to lie on the floor. A Sanitary Commission inspector noted that spittoons and chamber pots were not promptly emptied and that lazy and undisciplined soldiers had turned the hospital grounds into one large latrine. Hospitals in and near Cairo, Illinois, were apparently in better shape than many others, partially because overcrowding had been relieved by sending patients downriver to St. Louis. The rate of malaria among the patients in these units was high, although, like most physicians before the twentieth century, the medical officers there did not remark upon any possible relationship between the
62George Edgar Turner, Victory Rode the Rails: The Strategic Place of the Railroads (Indianapolis: Bobbs-Merrill Co., 1953), p. 297; Ltrs, De Camp to Finley (8 and 29 Jul, 2 and 16 Aug, 2 Sep, 14 and 21 Oct, and 1 Nov 1861), all in RG 112, entry 12; Report to the Western Sanitary Commission, pp. 3-6; Maxwell, Sanitary Commission, p. 105; Brinton, Memoirs, p. 35; Forman, Western Sanitary Commission, pp.8-10, 15; U.S. Sanitary Commission, Documents 1, no. 26:5, 9, 10,15, no. 36:6, 46, no. 38:3; Western Sanitary Commission, Report, p. 8.
63Quote from H. Phillips to Cameron (2 7 Dec 186 1), RG 112,entry 12; Ltrs, De Camp to Finley (19 Aug and 14 Oct 1861), both in RG112, entry 12; Forman, Western Sanitary Commission, pp. 13, 15; Report to the Western Sanitary Commission, p. 10; "Sick and Wounded Soldiers in St. Louis," American Medical Times 3 (1861):396; MSH 1, pt. 1:60-65, 114-19.
176
JOHN H. BRINTON.(Courtesy of National Library of Medicine.)
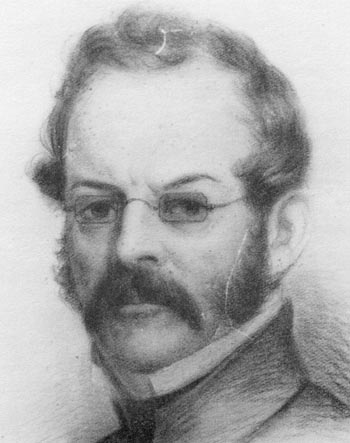{kind=link}
mosquitoes, "powerful and bloodthirsty ... pests, gray-backed, huge and insatiate," and the disease rate. As usual, inexperience joined ignorance and undiscipline as a major source of trouble. The young brigade surgeon, John Brinton, who set up a new hospital in Illinois at nearby Mound City to relieve overcrowding at the Cairo facility, commented sadly that, if he had had some experience before being called upon to establish that facility, he "could have accomplished in a few hours the work that cost me so many weary days of labor and nights of thought.64
Conclusion
In the West as in the East, the Medical Department`s inability to provide prompt and unfailing care for the sick and wounded of the Union army stemmed principally from two factors, both beyond the Department`s control. The frequency with which Union forces were defeated in 1861 greatly complicated the management of medical care and evacuation, and the newness of warfare on the scale of the Civil War made it impossible for anyone to have adequately anticipated the scope and magnitude of the problems that would arise. Nevertheless, the Department did not adjust as rapidly as it might have to the new demands placed upon it. Surgeon General Finley was apparently totally unable to grasp the significance of the situation that faced him and seemed more concerned with maintaining his image as head of the Department than with designing new approaches to new problems. Medical Director King, too, found the Lawsonian tradition hard to forget. Although King`s successor, Tripler, was capable of a certain amount of innovation, he was not daring by nature, and abandoned the old ways only with reluctance. To the West, such men as young Brinton and the veteran Wright struggled to adapt to the new situation, but youthful vigor could not make up for inexperience, nor mature judgment compensate for inadequate numbers of hospital beds. The first eight months of the war were long enough for serious problems to develop, but not long enough for adequate solutions to be devised and carried out.
![]()