



Books and Documents > The Army Medical Department 1818-1865
CHAPTER 9
The Civil War in 1862: Learning on the Job
The horrors experienced by the sick and wounded during the first months of the Civil War made the need for change in leadership, organization, and operations of the Medical Department in 1862 undeniable. No truly applicable model existed to guide these changes, however. The Medical Department would have to learn through trial and error what was required. The learning process had begun in 1861, but fast and imaginative learners as well as energetic leaders were still wanted.
The first developments to influence the Medical Department significantly, however, took place at a higher level. In January 1862 the relentless Edwin M. Stanton replaced Cameron as secretary of war. In April, Congress voted to allow promotion on the basis of competence rather than seniority. The new bill had barely passed when Stanton, using Surgeon General Finley`s alleged mishandling of a complaint as a pretext, removed the aging physician from office and exiled him to Boston, thereby triggering his resignation. At the urging of the U.S. Sanitary Commission, but against his own inclinations, Stanton then appointed a 33-year-old assistant surgeon with barely more than eleven years of Army experience to be the new surgeon general.1
Two days after appointing William Alexander Hammond surgeon general, the secretary of war called the new head of the Medical Department into his office. Stanton asked a casual question about the activities of the U.S. Sanitary Commission in a "tone and manner" Hammond recalled as being "offensive in the extreme," and then assured his subordinate that "if you have the enterprise, the knowledge, the intelligence, and the brains to run the Medical Department, I will assist you. "Determined not to "quietly submit to the insolence which [Stanton]constantly exhibited toward his subordinates," Hammond, as he later remembered it, replied:
Mr. Secretary, . . . I am not accustomed to be spoken to in that manner by any person, and I beg you will address me in more respectful terms ...during my service in the army, I have been thrown with gentlemen, who, no matter what our relative rank was, treated me with respect. Now that I have become Surgeon-General, I do not intent to exact anything less than I did when I was Assistant Surgeon, and I will not permit you to speak to me in such language as you have just used.
To which Stanton answered, "Then, sir, you can leave my office immediately." His
1Strong, Diary, p. xxxix; Maxwell, Sanitary Commission, pp. 126-27. Unless otherwise indicated, this chapter is based on Brown, Medical Department, and Callan, Military Laws.
178
WILLIAM A.HAMMOND. (Courtesy of National Library of Medicine.)
{kind=link}
head thoroughly turned by the respect his colleagues had shown for his ability and by his rapid rise to high office, Hammond thus planted the seeds of his own destruction as surgeon general and undermined the success to which his ability and energy entitled him.2
Hammond`s earlier experiences in the Army foreshadowed his future as surgeon general. His medical research and his work as a naturalist while serving as an assistant surgeon in the West brought him to the favorable attention of prominent scientists, but he was unable to tolerate a life characterized by, in his words, "restraint and uncertainty." He resigned from the Army in 1860, using as a pretext what now appears to have been a psychosomatic illness. When war broke out, however, he was determined to take part, even though to reenter the Medical Department he had to take the entrance examination again and enter at the very bottom of the list, losing credit for the years he had served earlier. He managed to counter Surgeon General Finley`s skepticism by signing a pledge stating that he had not suffered from his heart problem for three years and that if it returned, he would resign.3
Hammond`s work in the earliest months of the war demonstrated his administrative talents. With great energy he set up new hospitals and improved those already established in Pennsylvania, Maryland, and West Virginia, experimenting with a new system of ventilation. While doing so, he served under two men, Charles Tripler and Jonathan Lettermen, who were sufficiently impressed with his abilities to serve later as his subordinates without apparent objection, and under Maj. Gen. George B. McClellan, who become convinced that Hammond would make a good successor to Finley. Hammond`s success also brought him the enthusiastic support of the U.S. Sanitary Commission, but during this same period he managed to earn the enmity of Secretaries of War Cameron and Stanton and of Finley and Robert C. Wood, who several times served as acting surgeon general.4
2Quotes from William A. Hammond, A Statement of the Causes Which Led to the Dismissal of Surgeon General William A. Hammond From the Army (New York, 1864), p. 16.
3Quote from Ltr, Hammond to Baird (19 Apr 1860), RU 305, Smithsonian; Ltr, Hammond to Baird (18 Oct 1860), RU 305, Smithsonian; Strong, Diary, pp. 185, 185n; Bonnie Ellen Blustein, "A New York Medical Man: William Alexander Hammond, M.D. (1828-1900), Neurologist" (Ph.D. dissertation, University of Pennsylvania, 1979), pp. 77-78; Hammond (Pledge, 18 Mar 1861),RG 112, entry 2, 28:84; USSC, Documents 1, no. 41:2 9- 3 0, 31 n.
4Blustein, "Hammond," pp. 75-82; Ltr, Finley to AG(4 Mar 1862), RG 112, entry 2, 29:669; Strong, Diary, p. 187; MSH1, pt. 3:908; "The Sanitary Commission," p. 175.
179
From the outset, the key factors in Hammond`s military career were his considerable ability as a scientist, his energy and drive, and his unfortunate temperament. Even more than his administrative and scientific talents, his hot temper, his impulsiveness, and his "great self-confidence" that, in the words of friend and colleague S. Weir Mitchell, "led him to inconsiderate action," determined his fate in the Army. Many who knew Hammond as surgeon General were less charitable in their opinions than Mitchell; one remembered that, as head of the Medical Department, Hammond was "rarely anything but captious, irritable, and pompous."5
Just at the time Hammond came to office, Congress was acting to make major modifications in the structure of the Medical Department. In April 1862, it created the positions of medical inspector general and eight medical inspectors. It also revived the position of assistant surgeon general, a post to which Stanton, with Hammond`s approval, quickly named Robert Wood. Hammond later noted that Stanton had promised the position to Wood, subject to the surgeon general`s approval, anticipating, Hammond believed, that he would react vindictively. The inspectors were to be chosen from among both volunteer surgeons and regulars. They were to be responsible for the overall management of military hospitals and for the inspection of sanitary conditions in camps where crowding was leading to epidemics of such diseases as typhoid fever and dysentery. Congress added to the prestige of the Medical Department by giving the new medical inspector general the rank of colonel and the medical inspectors that of lieutenant colonel, and by raising the rank of the surgeon general to brigadier general.6
Congress was also aware at this time of the need to increase the size of the Medical Department. Under pressure from the Sanitary Commission it added ten surgeons, ten assistant surgeons, and twenty medical cadets to the roster in April and granted Hammond at the same time permission to appoint as many hospital stewards as he needed. Regimental surgeons and assistant surgeons were continuing to join the Army as part of each new regiment of volunteers and were serving the same terms as those signing up with them. But in July the legislators voted to increase the number of volunteer physicians serving outside the regimental framework as well. After changing the title of the Corps of Brigade Surgeons to Corps of Staff Surgeons, Congress added 40 surgeons and 120 assistant surgeons to the group, designating them surgeons and assistant surgeons of the volunteers. These men were to be "liable for detail for any professional duty the good of the services requires." Congress also gave each volunteer infantry regiment a second assistant surgeon and each cavalry regiment one surgeon and one assistant surgeon. It ruled that militia regiments, when called up, should be organized just as the volunteer units were.7
Amid these signs of progress, a new conflict began to take shape within the De-
5First and second quotes, S. Weir Mitchell, "Some Personal Recollections of the Civil War," Transactions of the College of Physicians, 3d ser., 27 (1905):89; third quote, Henry Crecy Yarrow, "Personal Recollections of Old Medical Officers, "Military Surgeon 60 (1927):174.
6Hammond, Statement, p. 4; Maxwell, Sanitary Commission, pp. 64, 139; Blustein, "Hammond," p. 78. Medical directors occasionally appointed their own inspectors on an informal basis, but such an appointment did not bring with it a change in rank.
7Quote from Ltr, SGO to David L. Magruder (8 Apr 1862), RG 112,entry 2, 30:158; see also Ltr, SGO to Hammond (1 Jul 1862), RG 112, entry2,31:311; Maxwell, Sanitary Commission, pp. 127-29, 135-37.
180
partment. The ill will between Stanton on the one hand and Hammond and his allies on the Sanitary Commission on the other initially lay beneath the surface, but it emerged to interfere with the Medical Department`s operations shortly after Hammond`s appointment as surgeon general. For two months after Congress created the position of inspector, the secretary of war delayed giving his official approval to the surgeon general`s nominees. Even then, Stanton accepted only four of the eight, substituting for the others men who were apparently not highly regarded by the medical profession. When Congress, recalling what appeared to be the unnecessary agonies of the sick and wounded in McClellan`s campaign of May and June, rejected Charles Tripler, McClellan`s medical director, for the position of inspector general, Stanton named in his place former Brigade Surgeon Thomas Perley, a man who was "quite unknown to the public service and to the profession, "as the editor of the American Medical Times put it. Despite the low caliber of the men named to the new positions, the lawmakers saw the position as important and in December created another eight openings for inspectors in the department. Congress also required that the inspectors assume, in addition to their other duties, the responsibility for examining patients in general hospitals and convalescent camps to determine who among them should be discharged from the Army.8
Congress also created another new position within the Medical Department, that of medical storekeeper. Although hospital stewards were capable of compounding medicines under a surgeon`s direction, Congress now authorized the secretary of war to hire as many as six medical storekeepers, who were to be well-qualified apothecaries or druggists and to work at a more responsible level than hospital stewards. They were required to be between twenty-five and forty years of age and to pass an examination administered by a board of at least three medical officers. The position of the medical storekeeper was temporary, to be eliminated at the end of the war, and apparently carried no rank. Like the medical purveyor, the storekeeper was expected to post bond. He apparently served as a captain and often acted as a substitute for medical purveyor.9
Despite these newly created positions, physicians remained the backbone of the Medical Department. Alone among them, volunteer regimental surgeons continued to be examined only by state authorities. They were joining the Army in great numbers, as many as 1,200 in the eight months preceding May1862. In July, in authorizing the increase in the number of volunteer staff surgeons, Congress ordered that medical officers serving at this level continue to be examined by a board of medical officers. The very strict examinations that Hammond designed for them, however, caused many to fail, and Stanton threatened to eliminate the examining board if more did not pass. Since the correlation between test scores and performance in the field was apparently open to question, this
8Quote from "The Week," American Medical Times 5 (1862): l1; see also "Sanitary Inspector in the Army," American Medical Times 5 (1862):94-95; Saul Jarcho,"Edwin Stanton and American Medicine," Bulletin of the History of Medicine 45 (1971):155; "The Sanitary Commission," pp.176-77.
9Henry N. Rittenhouse, "U.S. Army Medical Storekeepers, "American Journal of Pharmacy 37 (1865):88, 90; Ltr, SGO to W. S. King (5 Jul 1862), RG 112, entry 2, 31:367. The question of rank is not addressed in the legislation, but letters to the surgeon general make it apparent that medical storekeepers were addressed as "captain":Ltr, Rittenhouse to SG (6 Dec 1862), RG 112, Registers of Letters Received, 1862, entry 10, p. 447.
181
threat was not as outrageous as it might sound. Hammond was determined, however, to improve by this means the quality of the care that the Union soldier received. By the end of the year he had concluded that physicians taken into the regular medical service should have studied hygiene and military surgery. He wrote the heads of medical schools to urge the introduction of such courses into their curricula. Although he relaxed his standards somewhat for the examinations given volunteer surgeons, he began to work with eminent physicians in several large cities to improve the caliber of doctors made available to serve under contract.10
The quality of the Army`s contract physicians was important, since during the course of the war more than 5,500 civilian doctors assisted the Medical Department. Many routinely staffed general hospitals while others provided help only in emergencies when it was necessary to locate more physicians quickly. In the last group were some of the nation`s most prominent doctors. When a battle resulted in overwhelming numbers of casualties, those who flocked to the scene might include quacks, cultists, and practitioners of questionable ethics, men who were not under military discipline and who could, therefore, come and go as they liked, taking assignments that pleased them and rejecting all others. They often performed unnecessary operations or wrought havoc as they dug about for bullets. As a result of the problems experienced with doctors so casually assembled, the Medical Department decided to call only upon members of a reserve surgeons corps formed by the governors of various states. These gentlemen were paid the salary of contract surgeons and came in if called. They served under Medical Department orders and were required to remain at their assigned posts at least fifteen days, unless officially released sooner.11
Although, like his attempts to require strict examinations, Hammond`s efforts to gain for his medical directors a rank more suited to their responsibilities failed, medical officers did, in theory, attain one privilege in 1862. When the war was more than a year old, both sides agreed that they would not in the future hold noncombatants, including physicians, as prisoners of war. Unfortunately, many months would pass before this understanding, never formalized, was routinely heeded.12
The need for civilian hospital workers was more constant than that for civilian physicians and some system was required to guide their activities. In June 1862, the secretary of war issued more detailed regulations concerning civilian hospital workers than had been previously in force. Attendants were to serve under military discipline with a squad of eleven nurses assigned to serve every 100 patients. The chief of the squad was to report to the hospital steward. Regulations called for two male nurses for every one female in general hospitals, but many facilities had yet to hire their first woman.13
10Ltrs, Hammond to G. W. Mittenberger and to others (all 22 Dec 1862), all in RG 112, entry 2, 33:546; Hammond to S.D. Gross (5 and 9 May 1862) and to Cooper (14 May 1862), all in RG 112,entry 2, 30:350, 394, and 423, respectively; T. M. Markoe to SG (19 May1862), RG 112, entry 12.
11GO (no. 65, 12 Jun 1863), in William Grace, The Army Surgeons Manual, 2d ed. (New York: Balliere Bros., 1865), p. 47; "Volunteer Surgical Aid" and "The Week," both in American Medical Times 5 (1862):135 and 150, respectively; Hall, "Lessons," pp. 76-77; William A. Hammond, "Letter to `Gentlemen,`" Boston Medical and Surgical Journal 67 (1862-63):305-06.
12"The Week," American Medical Times 5 (1862):l1; GO (no. 60, 6 Jun 1862), in Grace, Manual, p. 44.
13Grace, Manual, pp. 109, 111-12; J. C. Stimson and L.C. Thompson, "Women Nurses With the Union," Military Surgeon62 (1928):228-29.
182
In the early months of 1862, the general hospitals in which these nurses served were still housed almost entirely in buildings originally erected for some other purpose. Hammond shared the U.S. Sanitary Commission`s enthusiasm for the pavilion concept, having experimented with hospital design as a medical officer in West Virginia before he was appointed surgeon general. He had become convinced that more than 3,000 patients could be cared for in one hospital if the ventilation was good. As the building program progressed, the Medical Department was able to abandon some of the old facilities, but the location of the new institutions became a political issue, both because communities usually wanted their wounded cared for nearby and because businessmen were aware of the profit such an institution could engender. Hospitals had also been established by states for their own wounded to supplement the Army`s facilities, and the Medical Department was having so much difficulty in finding enough beds that it had no choice but to cooperate with the states. In June 1862, at the urging of state authorities who found them very costly to support, the Medical Department assumed responsibility for many of the state institutions. Because for all practical purposes these facilities remained largely under state control, many patients who should have rejoined their units were instead discharged to civilian life.14
The enormous numbers of sick and wounded flooding hospitals with the start of the new campaign season made it necessary to find ways to limit the size of the hospital population. Surgeons attempted to weed out malingerers, but in the confusion that followed a battle, this was a difficult task. Medical officers also urged that more efficient procedures for discharging the chronically ill from the service be devised. The concept of the convalescent camp began to gain popularity because such a camp made it possible for soldiers almost ready to resume their duties to remain relatively near the units to which they would be returning.15
Hammond often visited proposed hospital sites to make sure that those chosen were healthy, but by the end of 1862 the Union Army`s 150 general hospitals, scattered about the North and West and in some areas of the South and staffed largely by contract surgeons, were not achieving the record for healthfulness that had been hoped for. Although 400 stewards, 300 wardmasters, 6,051 male and female nurses, 3,025 laundresses, and 2,017cooks served in general hospitals, many of these institutions were still filthy. Dirt, soiled dressings, and old clothing might be under the beds in wards that seemed clean. Bathrooms and tubs sometimes served as temporary repositories for "every uncleansed or unemptied chamber vessel, of soiled and offensive linen, and of every slop that a lazy nurse does not care to move." Laundries, kitchens, and mess rooms might be in a similar state, and hospital grounds could be littered with refuse and privies. Ventilation was likely to be deficient despite Hammond`s efforts, principally because architects valued warmth above fresh air.16
14Blustein, "Hammond," p. 83; Joseph R. Smith, "Hammond, The Surgeon-General," Post Graduate15 (1900):628; Emory Upton, The Military Policy of the United States(Washington: Government Printing Office, 1917), pp. 402-05.
15Ltr, William J. Sloan to Hammond, and Telg, Josiah Simpson to Hammond (both 7 Jul 1862), both in RG 112, entry 12; Ltrs, Sloan to Hammond (20 Aug 1862) and to SG (1 Sep 1862), both in RG 112, entry 10,p. 637; Finley to Thomas (17 Mar 1862), RG 112, entry 2, 30:47-48; MSH1, pt. 3:908.
16Quote from "Management of Military Hospitals," American Medical Times 5 (1862):292; War Department, SGO, Annual Report,1862, p. 6; "Locations and Appointments of Our Military Hospitals, "American Medical Times 5 (1862):24; Blustein, "Hammond," p. 83.
183
Conditions in the Army`s hospitals were all the more important because of the climbing sick rate, more than 16 percent higher than it had been for the period of 1845 to 1859. The death rate from disease had increased even more markedly, from 2.4 percent a year in the earlier period to 5.0percent from July 1861 through June 1862. Among the more common diseases was diarrhea, with over 200,000 cases recorded for the year starting July 1861. Physicians found it difficult to estimate the number of deaths from this source, however, since diarrhea often coexisted with other illnesses. Measles afflicted almost 22,000 in that period, causing 511 deaths. Figures for such problems as typhus, typhoid fever, malaria, and other fevers as well as for scurvy were unreliable, not only because one victim might have multiple diseases but also because physicians could not always distinguish one fever from another. Almost 24,000 cases of venereal disease appeared, although the author of one journal article noted that very few patients came from commands where lieutenants were "vigilant and sober. "The U.S. Sanitary Commission blamed the Army diet for scurvy. One authority suggested that scurvy had become a major Army problem when he maintained that the Commission could best promote the Army`s health "by resorting to measures that shall insure a sufficient supply of antiscorbutic vegetables and antiscorbutic care."17
Because of the sick rate and the growing numbers of wounded, the strain on the Medical Department`s supply system in-creased too rapidly for Hammond to hope to function without the aid of the U.S. Sanitary Commission and similar agencies. Congress eased his work by removing some of the red tape that restricted the ability of the purveyors to keep up with demand. Hammond revised the supply table so that it continued to reflect current usage and established large depots at Baltimore, Maryland; Fort Monroe, Virginia; Washington, D.C.; Cincinnati, Ohio; St. Louis, Missouri; and Nashville, Tennessee. Distribution in the field was handled from field depots, but buying was still handled principally from New York City and Philadelphia. Although urgent need still led to the occasional purchase of items that proved to be poor, the difficulties he was experiencing in keeping up with demand did not keep Hammond from obtaining Stanton`s approval of a plan to supply medicines to any families of volunteers that were totally indigent. In July Congress voted $15,000 for the purchase of artificial arms and legs for both soldiers and seamen, and made the Army Medical Department responsible for determining the models to be used. Hammond was interested in quality as well as quantity, and his efforts to improve the equipment used by physicians in the field also led to the development of two new designs for medical knapsacks.18
Among Hammond`s other successes were two of long-range rather than immediate significance, the establishment of the
17First Quote, "The Hospital at Portsmouth, R.I.," Boston Medical and Surgical Journal 67 (1862-63):116;second quote, Elisha Harris, The United States Sanitary Commission(Boston: Crosby & Nichols, 1864), p. 29; MSH 1, pt. 3:622-24;D. Hunter, "General Orders, No. 5," Medical and Surgical Reporter8 (1862):103; see also Harris, The United States Sanitary Commission, p. 30.
18Ltr, Hammond to Baird (29 Nov 1857), RU 305; Blustein, "Hammond," pp. 56-57, 95; Smith, "Hammond," p. 627; MSH 1, pt. 3:965-66;War Department, SGO, Annual Report, 1862, pp. 8-9; Reasoner, "Medica Supply," p. 17; Ltr, SGO to John Neill (28 Apr 1862), RG 112, entry 2, 30:301; John E. Summers to SG (23 Sep 1862), in RG 112, entry 10, p.664; Hennell Stevens, "The Medical Purveying Department of the United States Army," American Journal of Pharmacy, 37 (1865):92-93.
184
Army Medical Museum and the first steps toward the creation of what would become The Medical and Surgical History of the War of the Rebellion. The surgeon general was particularly sensitive to the possibilities for extending the boundaries of medical knowledge during such a vast conflict. Early in his tenure as head of the department he urged that his subordinates send in specimens both of human tissue and of the foreign bodies, such as shell fragments or bullets, found in wounds. He appointed two men to assist in collecting information and specimens for the history and for the medical museum. Although Stanton succeeded in thwarting Hammond`s desire to create a formal medical library in association with the museum, the Surgeon General`s Office continued to add to this collection of books on an informal basis until 1867 when the first librarian was appointed.19
As the new chief of the Medical Department, Hammond was full of energy and confidence in 1862. Before he had been in office a month, he was going out of his way to express to the medical directors of major armies his confidence in them. He wished them to feel assured of his support in taking the initiative in solving the problems they encountered. He was obviously more willing to delegate authority than his two immediate predecessors had been and desired that his medical directors exercise considerable independence in determining their own needs without directions from him. Rather than control the Washington complex of hospitals personally, as Finley twice attempted to do, Hammond made Surgeon Jonathan Letterman medical director for the capital area. Realizing that the control of both field and general hospitals in an area or for an army might be too much for one man, he began to divide these responsibilities, having one director, for example, for each of the major cities in the East where large numbers of Army patients were cared for and yet another for each army in the East.20
Care of the Sick and Wounded in the East
In early 1862, a visitor inspecting General McClellan`s Army of the Potomac, the principal army in the East, was pleased with what he saw. Physicians appeared to be both competent and hard working, camps were neat and orderly, drainage was good, and tents were warm, although their poor ventilation caused him some distress. The general hospitals serving the Army of the Potomac, of which there were ten in mid-March, needed little in the way of improvement, in his view, and he found the competence of the nurses, both male and female, to be particularly worthy of notice. In view of such reports, Medical Director Charles Tripler believed with some justification that his attempt to bring order into the medical support of the Army of the Potomac was at least partially successful.21
In March Tripler was apparently confident of his own ability to deal with the demands of the upcoming campaign. He sent all the sick except for convalescents to general hospitals, a necessary move that placed a considerable burden upon the facilities
19Smith, "Hammond," pp. 625-26; Grace, Manual, p. 110; Brinton, Memoirs, pp. 169, 179; Schullian and Rogers, "National Library," pp. 9-10; Wyndham Davies Miles, A History of the National Library of Medicine (Washington: Government Printing Office, 1982), pp. 18, 29.
20Ltrs, Hammond to Tripler (2 May 1862) and SGO to McDougall(12 May 1862), both in RG 112, entry 12, 30:335 and 408, respectively.
21L., "Sanitary Condition of the Army of the Potomac," and "Correspondence," both in American Medical Times 4(1862):45-46 and 214, respectively.
185
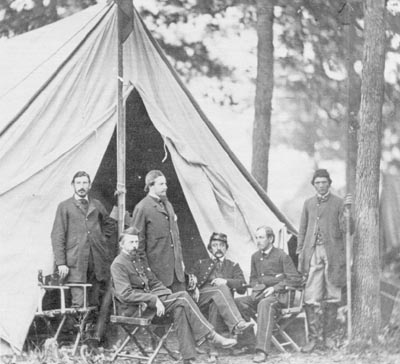
JONATHAN LETTERMAN(second from left, seated), Medical Director, Army of the Potomac, AND ASSISTANTS. (Courtesy of National Library of Medicine.)
{kind=link}
in Washington and nearby communities. To relieve the strain, he took over the barracks left vacant as McClellan`s army moved south. Unfortunately, much modification was necessary to make these buildings suitable for this use: they were poorly arranged, their ventilation was haphazard, their ceilings low. Their floors often showed wide cracks; they lacked appropriate space for laundry and kitchen; and their sites were frequently filthy. The two newly built hospitals in Washington were completed in time to assume some of the burden, but the number of patients was soon so large that tents had to be erected on the grounds of the new institutions to care for theoverflow.22
The continued establishment of facilities
22MSH 1, app.:52 and pt. 3:908-09, 920.
186
more removed from the battlefield, including those at Philadelphia and New York, relieved the situation in hospitals in the Washington area to some degree, as did the creation of temporary general hospitals near the battlefield. The more permanent facilities were often quite large; New York institutions, according to the surgeon general`s annual report of November 1862, held almost 5,000 patients and those of Philadelphia, 5,500.23
Tripler began laying plans for the care of sick and wounded in the field before McClellan opened his campaign against Richmond. He prepared instructions for his surgeons about the establishment of what he called "field depots," the organization of the medical officers to serve in them, the proper method of dealing with the wounded, and the way in which ambulances were to be divided up and used. A shortage of ambulances, however, interfered with the operation of Tripler`s modest ambulance corps. Although he repeatedly attempted to acquire more vehicles, the Quartermaster`s Department sent him only a few, and many of these were two-wheelers, which Tripler regarded as "good for nothing." He also attempted to obtain all the supplies that he anticipated needing. Unfortunately, just when McClellan`s forces were beginning their move by water toward the peninsula between the York and James rivers, Surgeon General Finley announced that, as ordered by the secretary of war on 7 April, he was resuming personal control overall general hospitals. Tripler was to leave behind his purveyor and some of his supplies, thus starting the new campaign season with only part of what he needed and the hope that the rest would be forwarded to him from New York City by the time he needed it.24
The tendency of many regimental surgeons early in the campaign to abandon supplies rather than to move them exacerbated Tripler`s supply problem, since the officers then turned to the purveyor for replacements. The tents belonging to some units, furthermore, were inexplicably left behind in Alexandria, making more difficult the establishment of field hospitals, especially since on the peninsula buildings suitable for hospital use were few. (Map 6) Pilfering and carelessness during shipment reduced the amount of supplies actually received, and late shipments resulting from the low priority given Medical Department supplies by the quartermaster only made matters worse. Tripler`s request in April 1862 that "an experienced quartermaster and assistant commissary of subsistence be attached to the command of the Chief Medical Officer of an army in the field" came to naught, and Tripler began protesting "beforehand against the Medical Department being held responsible for evils they have no possible means of obviating."25
During the Peninsular campaign, an extremely high rate of disease, sometimes called Chickahominy fever, probably either a combination of typhoid and malaria or typhoid alone, made the supply shortages even more critical. Tripler determined, therefore, to reduce the number of patients for whom he was responsible at any one time by evacuating them as quickly as possible. He made every effort to send both
23"Army Medical Intelligence" and "Medical Affairs," both in American Medical Times 4 (1862):360 and 5 (1862):28, respectively; "The Hospital at Portsmouth R.I.," p. 115; War Department, SGO, Annual Report, 1862, pp. 2-4; MSH1, pt. 3:908, 932-33, 935, 989.
24 Quote from MSH 1, app.:63. Unless otherwise indicated, all material on Tripler`s work is based on MSH 1, app.:50-63.
25Quote from MSH 2, pt. 3:933; see also Maxwell, Sanitary Commission, p. 160.
187
188
the sick and the wounded away from the battle area. Because the facilities at Fort Monroe were limited, many wounded were sent north to Washington, Baltimore, and Annapolis, Maryland, or even further. It was expensive, however, to ship those with slight wounds or self-limiting diseases north only to have to return them south again when they were ready to rejoin their units, and despite the efforts of both the Quartermaster`s Department and the U.S. Sanitary Commission, few adequately equipped river or oceans teamers were available for the final leg of the journey. On occasion, furthermore, the water was so shallow that the transports could not come close to shore, and Tripler was forced to act on his own to line up whatever shallow draft vessels he could find to take his patients out to the steamers.26
The lack of discipline that characterized so many Union soldiers contributed to Tripler`s problems. On one occasion at White House, on the Pamunkey River in Virginia, the 150 men assigned to pitch hospital tents worked so slowly that two days were required to erect thirty-four. On a number of occasions, furthermore, able-bodied soldiers eager to escape the horrors of the campaign swarmed aboard trains and steamers taking the sick and wounded north, displacing those entitled to evacuation. Once when Tripler insisted upon checking candidates for evacuation carefully, a gang of stragglers rushed aboard a vessel that was only half-loaded and refused to get off. Regimental officers who, Tripler believed, could have prevented this disorder did not do so. He finally decided to reduce the effects of this particular problem by retaining as many of the sick as possible in the peninsula. He ordered more hospital space at Yorktown and Williamsburg to house the ill from White House and asked for more medical officers. By mid-June, only half the tents he had requested a month earlier had arrived; and many of these could not be sent to Yorktown because they were needed for field hospitals nearer the battlefield. Tripler was thus forced to use some vessels as floating hospitals and to continue the evacuation of the sick as well as the wounded, and with them, inevitably, stragglers, north by steamer.27
Even moving the sick and wounded as far as the riverbank was no easy task. Ambulances were scarce. Hospital attendants were increasingly busy working in hospitals. Band members were often too frightened to venture near the battlefield. Tripler had no control over trains that brought some of the wounded to the waterfront, and the enemy often cut the lines. Asa result of these difficulties, severely injured men sometimes lay for twenty-four or even forty-eight hours on muddy, hot battlefields before they were collected, and then were left waiting in the rain for hours at a railroad depot without shelter, food, or water. Since the army was often in retreat, the wounded who could not walk also faced the possibility of capture.
As the situation on the peninsula deteriorated, Hammond became increasingly uneasy about Tripler`s ability to deal with the demands placed upon the Medical Department there. In encouraging Tripler to act decisively on his own, the new surgeon general had reassured him early in May that all the department`s resources were behind him and that he had only to let the department know his needs. By mid-May, however, Tripler was approaching frenzy.
26Ltrs, SGO to Cuyler (11 Apr 1862), Wood to M. C. Meigs (24 Apr 1862), and SGO to Tripler (17 Apr 1862), all in RG 112, entry 2, 30:189, 286, and 325, respectively; Tripler to Wood (14 Apr 1862), RG 112, entry 12; MSH 1, pt. 3:75; MSH 2, pt. 3:982, 984.
27Ltr, Tripler to SG (30 Apr 1862), RG 112, entry 12.
189
He was trying frantically to acquire the necessary transportation for his patients on both land and water and to arrange for the necessary hospita l facilities and for subsistence. He pointed out to Hammond that the problems that took all his time and energy lay properly within the purview of the Quartermaster`s and Subsistence Departments. He repeatedly begged Hammond for aid and predicted dire consequences if he did not receive it at once. Delays in the delivery of supplies were "producing frightful results, "he telegraphed Hammond on 18 May, while he added in another telegram the same day that the medical staff was "all nearly exhausted."28
Hammond obviously sympathized with Tripler`s predicament and pushed to obtain ambulances and steamers from the Quartermaster`s Department and to fill other requests as rapidly as possible. His answer to Tripler`s complaints, however, implied that Tripler was not doing all he could to help himself. He had already been granted, for example, the authority todo on his own many of the things he was now requesting permission to do. In addition, he had not worked as closely with General McClellan as Hammond believed he should. The surgeon general also pointed out that Tripler must accept the fact that the Medical Department could not always meet all his needs. Hammond obtained control over steamers from the quartermaster in June and at last, presumably concluding that Tripler could no longer cope with the situation alone, sent two surgeons to the peninsula with orders to organize the evacuation of the sick and the management of transports. He then gave Tripler specific instructions concerning the abandonment of several unhealthy hospitals and the establishment of others to replacethem.29
Nevertheless, as the end of June approached, confusion ruled at White House. The wounded continued to arrive in great numbers, communications were poor and then finally nonexistent, few tents were available, and no more could be obtained. Patients filled the shelters and spilled out onto the lawn. On 28 June when the evacuation south to Harrison`s Landing on the James River began, Tripler had to order more than 600 wounded abandoned to the enemy because he had so few ambulances, although he left behind surgeons who volunteered to stay with them, supplies, subsistence, and nurses. At Harrison`s Landing in the first days of July patients lay in the open, without tents or shelter of any kind. Dysentery, diarrhea, malaria ,scurvy, and typhoid fever raged unabated. On 1 July the rain was once again deluging the sick and wounded when Jonathan Letterman arrived from Washington to relieve the defeated Tripler.30
Although Tripler may well have done all he could in the situation, George Templeton Strong of the U.S. Sanitary Commission believed that he had beenproved totally incompetent. Strong held that Tripler and his staff were entirely responsible for the sufferings of Union soldiers in Virginia, and Congress apparently agreed with Strong. After some senators visited White
28Quotes from Telg, Tripler to Hammond (18 May 1862), RG 112, entry 12; Ltrs, Hammond to Tripler (2 and 8 May 1862),both in RG 112, entry 2, 30:335 and 382, respectively; Telg, Tripler to Hammond (9 May 1862), RG 112, entry 12.
29Ltrs, Hammond to Tripler (19 and 22 May and 8 Jun 1862), and to Edward Vollurn (17 Jun 1862), all in RG 112, entry 2, 30:467 and 493-94,and 31:47 and 150, respectively; Tripler to Hammond (19 and 20 May and 1 and 6 Jun 1862, all in RG 112, entry 12.
30USSC, Surgical Memoirs of the War of the Rebellion, Collected and Published by the United States Sanitary Commission, 2 vols. (New York: U.S. Sanitary Commission, 1870-71), 1:276-77.
190
House and saw the situation for themselves, they refused to confirm Tripler`s nomination as inspector general. Hammond, however, did not openly blame Tripler. Indeed, he showed considerable compassion when he learned of the Senate`s action and received Tripler`s request to be relieved. He asked his former superior to name the position he wanted north of the Potomac or along the Ohio River, and when Tripler asked for the post at Detroit, it was his.31
A most difficult situation had crushed a man of modest talent. When circumstances permitted him to exercise his administrative talents to their fullest, Tripler functioned well. His toleration for frustration, however, was low, and he had little ability to make the best of bad conditions. In the Peninsular campaign he knew that if the requirements for ambulances, tents, transports, and supplies were not met, the consequences might be horrible. Having been frustrated by Finley when he attempted to prepare adequately for the upcoming campaign, Tripler was unable to accept the fact that Hammond could not at once make everything right. Preoccupied by his inability to prevent the disaster he knew was coming, Tripler failed to seize the available opportunities to prevent a further deterioration. Although Letterman bore no responsibility for the management of the sick and wounded in the peninsula, after he became familiar with the situation at Harrison`s Landing, he too concluded that the Medical Department should not be blamed. Tripler was not responsible for the disaster; the worst that could be said, perhaps, is that he was unable to handle the disaster when it occurred.32
Initially when Letterman reported for duty, the crisis at Harrison`s Landing demanded all his attention. Time, however, was on his side. The new medical director had to face all the frustrations resulting from his limited control over the steamers that evacuated his patients; although he could direct their activities when they were evacuating patients, he could not prevent their diversion, even at critical moments, to other uses. Thus he could only watch while vessels he needed were taken over to move Confederate prisoners. But with the arrival of more transports, outfitted at Hammond`s order to carry the sick and wounded, and of some of the 100 tents and 200 ambulances that the beleaguered Tripter had vainly urged Hammond to send, the situation on the James River eased. Patients could now be shipped to hospitals in the North and in the Fort Monroe area, and those who remained could be put under shelter. Letterman was then able to look beyond the immediate situation and to implement his plans for thefuture.33
Lettermen had apparently already formulated plans to improve the efficiency of the Medical Department, and in this he had the support of both Hammond and McClellan. McClellan had discussed the possibility of devising such a scheme personally with Stanton and had received the permission of the secretary of war to formalize it. On 2 August, the general issued an order putting Letterman`s formula into
31Strong, Diary, pp. 222, 230, 230n; Telg, Hammond to Tripler (20 Jun 1862) and Ltrs, Hammond to Tripler and to L. Thomas (both 19 Jun 1862), all in RG 112, entry 2, 31:170, 176, and 191, respectively; Tripler to SG (16 Jul 1862), RG 112, entry 10, p. 797.
32Telg, Letterman to Hammond (29 Jul 1862), RG 112, entry 12. Unless otherwise indicated, all material on Letterman is based on MSH 1,app.:93-104, and Jonathan Letterman, Medical Recollections of the Army of the Potomac (New York: D. Appleton & Co., 1866).
33Ltr, Letterman to Hammond (17 Jul 1862), RG 112, entry 12.
191
effect within the Army of the Potomac, although according to Letterman the printer did not return the order until a few days before the Army of the Potomac was to leave Harrison`s Landing, thus delaying steps to fully implement it. On 21 August, McClellan forwarded Letterman`s plan to Stanton for approval to put it into effect throughout the Union Army, but eight days later Stanton rejected it, noting it would only "increase the expenses and immobility of our army ... without any corresponding advantages," an opinion Maj. Gen. Henry W. Halleck echoed less than three weeks later. As a result, just at the time that Letterman was beginning to move ahead with his plan within the Army of the Potomac, he learned that both the secretary of war and the general in chief of the Union Army thoroughly disapproved of it.34
Letterman`s plan specified that two men and a driver, plus two stretchers, be on board each ambulance. Each regiment would be supplied with two light two-horse ambulances, and each corps another two, to provide evacuation from field to depot. Four-horse vehicles carried patients back to field hospitals and beyond. Letterman called for the organization of ambulances and their attendants by Army corps, with a captain in charge at the corps level, a first lieutenant at the division level, and so on down the line, with a sergeant directing the ambulances at the regimental level. The ambulance corps captain, though a line officer, reported to the medical director, an innovation that caused less comment than might have been expected, in view of the long history of controversy concerning the command relationship f medical and line officers. Those named to man the ambulances were neither teamsters nor band members, nor even hospital attendants who might be called away just when they were most needed. They were soldiers permanently detailed from the ranks for ambulance work. Commanders were required to order only "active and efficient" men to serve with the ambulance corps, and all the men of the new organization were to be regularly and carefully drilled in their new duties. Although medical officers from each division accompanied every ambulance train, ambulance corps officers handled all administrative matters. By creating a permanent, disciplined, and professional ambulance corps, Letterman guaranteed more efficient evacuation and because surgeons and attendants were no longer responsible for transporting patients, better hospital care for the sick and wounded.35
While Letterman worked out his plans for the ambulance corps, the medical staff of the Army of Virginia under Maj. Gen. John Pope faced difficulties similar to those that Letterman and Tripler had encountered in McClellan`s Army of the Potomac. Although disease was not as great a problem in Pope`s command as it had been on the peninsula and the weather remained good, problems involving evacuation overwhelmed the Medical Department during and after the Second Battle of Bull Run in late August. Ambulances were scarce and attendants and drivers, except for those sent from McClellan`s army to reinforce Pope in August, untrained and undisciplined. Rail lines that were to have been used to evacuate the wounded from the battlefield were cut, and the patient load became too great for the field hospitals of the area. Those unable to walk lay by the thousands on the ground for twenty-four and more hours unattended. While surgeons worked out the truce that would permit their removal,
34Quote from MSH 2, pt. 3:934.
35MSH 2, pt. 3:933-34, quote from p. 936.
192
stragglers and the slightly wounded managed to be evacuated before their less fortunate comrades.36
Once again, the entire system was not prepared for the more than 8,000 casualties that flooded in upon it. Pope`s medical staff was too small, and the general hospitals at Alexandria were thrown into confusion in early September as casualties began to come in. Realizing, perhaps, from Tripler`s experiences that it was extremely difficult for one man to manage medical care and all stages of evacuation as well, Hammond appointed John Brinton to the new position of medical director of transportation, to supervise the movement of the wounded to Alexandria and between hospitals in that city.
During and after Second Manassas, Pope`s medical director, Thomas McParlin, tried two new approaches to the old, familiar problems. In his desire to achieve greater efficiency in the management of field hospitals, McParlin attempted to take centralization to its ultimate conclusion by locating all field operations in one area. But because a single facility could not be convenient for medical officers scattered about a large area, surgeons tended to render more care on the battlefield, and the amount of time they spent away from the central hospital left it undermanned. McParlin`s attempt to improve the efficiency of medical supply by leaving the items he needed on the railroad cars that brought them and by keeping those cars on conveniently located sidings was thwarted. The cars were so overcrowded that it was impossible to allow any to be left standing for storage and the enemy could cut rail lines so that trains could not get through.
Triggered by Lee`s invasion of Maryland in September, the renewal of the conflict brought together the men who had fought in the previously separate forces of the Armies of the Potomac and of Virginia. Letterman was the medical director of the newly enlarged Army of the Potomac. Although by this point his ambulance corps was a month old, ambulances and medical supplies had to be left behind because of the speed with which McClellan wished to move. The presence of units from Pope`s force that had not been introduced to the new system also kept the battles in Maryland from providing Letterman`s concept with a true test. The medical director ordered that ambulances and supplies be sent on to Frederick, Maryland, as soon as they became available, but delivery proved to be exceedingly difficult because the Confederates had destroyed the railroad bridge over the Monocacy River near Frederick. All supplies sent by rail had to be unloaded at that point, with much confusion and delay resulting. Fortunately, ambulances began to arrive just before the Army of the Potomac reached Frederick, and the U.S. Sanitary Commission, which had its own means of transportation, provided invaluable help with supply.37
Discipline remained poor throughout the army, however, and despite Letterman`s efforts, critics charged that the ambulance service at Antietam was characterized by "gross mismanagement and inefficiency, . . . lack of system and control" during the battle. Ambulance
36Unless otherwise indicated, all information about the medical care given the Army of Virginia is based on Brinton, Memoirs, pp. 196-201; Duncan, Medical Department, pt. 3;and MSH 1, app.: 108-29.
37Ltrs, Letterman to Hammond (13 Aug and 6 Sep 1862), both in RG 112, entry 12; Thomas T. Ellis, Leaves From the Diary of an Army Surgeon ... (New York: John Bradburn, 1863), p. 300; "The Wounded and the Ambulances of Our Army," American Medical Times 5 (1862):247;Ltr, Cornelius R. Agnew (22 Sep 1862), in U.S. Sanitary Commission, Reports, Correspondence, and Printed Matter, Ms C19, NLM (hereafter cited as Steiner Report).
193
drivers were accused of greed and thievery, and some of the more than 8,000 wounded remained on the battlefield as much as twenty-four hours. How many of the difficulties related to the presence of the still untrained attendants and drivers from the units that formed Pope`s army cannot be ascertained. The wounded were, in any event, finally evacuated to Frederick, and in many cases, beyond to Washington, Baltimore, and the north.38
His experiences with the problems of supply, and perhaps those of the unfortunate Tripler as well, led Letterman to conclude that a change in the pattern of distribution would reduce losses when troops were on the move. As a result, he decided in October that, from that time on, supplies would be issued by brigade and doled out to the individual regiments as needed. It would thus be almost impossible for large amounts of medicines, bandages, and hospital stores to be casually abandoned every time a regiment moved. His experience in Maryland also led Letterman to issue general instructions to govern the management of a field hospital system, which he preferred to have organized by division, guaranteeing that each physician would know precisely what his assignment was. Incorporated in the orders issued at the end of October was the concept of having surgery performed only by the three best surgeons in each division.39
THOMAS A. McPARLIN. (Courtesy of National Library of Medicine.)
{kind=link}
The value of Letterman`s system and the competence of his work under very unfavorable circumstances were most clearly demonstrated in the disastrous battle of Fredericksburg, Virginia, in mid-December 1862. Despite all difficulties, the management of the wounded during this engagement was one of the first Medical Department successes in the Civil War. The attempt by McClellan`s successor, Maj. Gen. Ambrose E. Burnside, to defeat
38Quote from "The Wounded. . . "American Medical Times 5 (1862):246.
39Cir (no. 3, 30 Oct 1862), in U.S. Army Medical Department Order and Letter book of the Hospitals of the 2d Division, 12th Army Corps,1863, Ms fB50, NLM. Unless otherwise indicated, all material on the Fredericksburg campaign is based on Gordon W. Jones, "The Medical History of the Fredericksburg Campaign: Course and Significance," Theory and Practice in American Medicine, ed. Gert Brieger (New York: Science History Publications, 1976), and on Duncan, Medical Department. The terminology used to classify hospitals during the Civil War was confused and confusing. What Tripler referred to as a field depot was directed by a surgeon. The function that had been performed by the regimental hospital was after 1861 usually handled at the brigade, the division, or occasionally the corps level. These field hospitals resembled the old general hospitals because they took in patients from more than one regiment, but, unlike general hospitals, they were moved with the units they served. Some of the less permanent general hospitals might now be called evacuation hospitals.
194
the Confederates was a bloody and spectacular failure, but Letterman had ready near the scene of the battle the tents, ambulances, and other equipment and supplies that would be needed. He had trained the men who were responsible for the care of the wounded and for their evacuation from the battlefield. Three ambulances, each with two stretchers, two attendants, and a driver as well as two hospital tents, were available for each regiment. Stretcher-bearers were instructed exactly where to bring the wounded to meet the ambulances that would take them to the field hospitals.
Despite the difficulties involved in moving casualties under fire, evacuation from the battlefield to field hospitals went well, but Letterman`s management of supply and of the final stage of evacuation left him vulnerable to criticism. He did not easily delegate authority, and without a commissary to manage the depot, supply problems engendered by the unexpectedly high casualty rate grew. The Sanitary Commission filled the gap once more with food, blankets, warm underwear, and other items, and evaluated the work of the Medical Department at Fredericksburg as "admirable." Both Walt Whitman, who worked as a nurse with the wounded from Fredericksburg, and the new inspector general, Thomas Perley, were highly critical of the last stage of the evacuation, but neither was in a position to understand the problems Letterman faced. In addition, Perley was a man of dubious reputation and indebted for his position to Stanton, so that his criticism of the Medical Department might have been motivated by self interest.40
Letterman could not have anticipated that Burnside would order all of his 9,000 wounded, regardless of their condition, moved from the Fredericksburg area; as medical director he had planned to keep the most seriously hurt where they were. Thus he cannot be held responsible for the horrors that were said to have resulted from journeys made on open railroad cars and long waits for steamers that were also devoid of accommodations for the wounded. Although he did anticipate problems with stragglers and malingerers, he was apparently unable to find guards competent enough to keep them from climbing aboard trains for a free ride to Aquia. It was these men, Letterman maintained, who, finding no shelter at Aquia, began to send up loud complaints about the inhumanity of the Medical Department.
Although surgeons did not have to manage the evacuation of large numbers of casualties, those in charge of hospitals serving small units in the East faced some of the same problems that confronted McParlin, Tripler, and Letterman. The men holding coastal areas of the south often suffered from the high disease rates characteristic of these areas, and the surgeons with them could not always locate buildings easily adapted for use as hospitals. In western Maryland and Virginia, some problems experienced by the troops serving under Maj. Gen. Nathaniel Banks resulted from the fact that they apparently received little attention from the Medical Department in the early months of the year. Although much illness occurred among the men serving near Cumberland, Maryland, for example, Tripler was apparently unaware of their existence for some time, and supplies there and in the Winchester area were inadequate.41
40Quote from Edmund Andress, Complete Record of the Surgery of the Battles Fought Near Vicksburg ... (Chicago: Fergus, 1863), p. 30; Maxwell, Sanitary Commission, p. 182; Brinton, Memoirs, pp 215, 220.
41MSH 1, app.: 228-29, 234-36, 243-44, 246; Ltr, SGO to William S. King (5 Apr 1862), RG 112, entry 2, 30:145; Steiner Report, Ms C19, NLM; "Army Medical Intelligence," American Medical Times 4 (1862):129; Walker DeBlois Briggs, Civil War Surgeon in a Colored Regiment (Berkeley: University of California Press, 1860),p. 61.
195
Care of the Sick and Wounded in the West
West of the Appalachians the Medical Department experienced many of the same problems that it encountered in the East. For the Medical Department, the principal difference between the East and the West lay in the character of the chain of evacuation from field hospitals to general hospitals. In the East, where the navigable portions of the rivers ran east and west, patients were most often moved to the north or northeast from the battlefield, as water transportation was not always feasible. In the West, however, the existence of a widespread network of rivers running both east and west and north and south made it possible to rely on large-scale evacuation by water, and fluctuating loyalties and battle lines made rail lines especially vulnerable. Many of the hospital steamers that plied the principal rivers of the midwest could carry 200 to 600 patients or more. They were equipped, manned, and even chartered by one of the sanitary commissions or by a state organization, but Surgeon General Hammond controlled their use. Because of the extensive system of rivers, major hospitals could be located at sites as widely separated as St. Louis, Missouri, and Cincinnati, Ohio, and could shelter patients from battlefields hundreds of miles away.42
Although in Louisville and Cincinnati combined, the patient load was almost 3,500 in late 1862, the largest number cared for in the river cities of the midwest could still be found in St. Louis. Hospitals in the city itself in the autumn of 1862 held over 2,700 patients, while another 1,000 were sheltered at the nearby Jefferson Barracks. This building, unlike those upon which Tripler had to rely on in Washington in the spring of the year, was considered excellent for the purpose. It had piazzas and shaded walks for the patients, and its rooms were large and well ventilated. In time new buildings were erected at the Jefferson Barracks, increasing its capacity by 2,500. Benton Barracks and the marine hospital within the city were also taken over in the spring of 1862, but demand continued to exceed capacity. The Western Sanitary Commission deplored what it regarded as the crowding of the city`s general hospitals, which it blamed for high death rates from typhoid fever and erysipelas.43
Most of the patients in the general hospitals of the midwest came from the armies of Brig. Gen. Ulysses S. Grant, Maj. Gen. William S. Rosecrans, and Brig. Gen. Don Carlos Buell. Unlike McClellan in Virginia, Buell, headquartered in Louisville, Kentucky, appeared indifferent to the welfare of his sick and wounded. His regimental surgeons were few, averaging about three for every two regiments, many physicians having either fallen ill or resigned. Twelve percent of Buell`s men remained in Kentucky because they were ill when his army moved. His medical director, Robert Murray, was forced to establish hospitals along the army`s line of march to care for the large numbers who fell ill along the way. Ambulances were so few that the sick could not be carried far, and the two-wheeled type disintegrated on the rough roads of the West. Bedding and medicines were scarce
42Te1g, Hammond to McDougall (22 May 1862), RG 112, entry 2, 30:496; Forman, Western Sanitary Commission, pp. 42-46;Maxwell, Sanitary Commission, p. 121.
43Forman, Western Sanitary Commission, pp. 45, 49, 65-66; War Department, SGO, Annual Report, 1862, pp. 4-5; MSH 1,pt. 3:907.
196
and Buell begrudged the assignment of healthy soldiers to serve as nurses for their ailing comrades, so that little for the care and comfort of these unfortunates could be left behind.44
Despite Buell`s lack of concern for his sick, Murray was able to gain his consent for the establishment of a convalescent camp for 1,000 near Elizabethtown, Kentucky, a town located along the railroad that connected Nashville with Louisville, enabling these men easily to rejoin their units. Murray also set up a hospital at Elizabethtown, although whether the convalescents were used to nurse the sick there, an arrangement Buell favored, is notknown.45
The medical director for Grant`s Army of the Tennessee was fortunate in having a commander more sympathetic to the problems of the Medical Department than Buell, but he, too, faced high disease rates. Supplies were shore and, because of "irregularities in the quartermaster`s department. . . in the District of Cairo," ambulances and hospital tents for Grant`s army were even harder to obtain than they were for other armies. No buildings suitable for large hospitals were found along the line of march, and the army was soon far from its supply bases. The two-wheeled ambulances that composed half of the force`s allotment once again proved too fragile for the uses to which they were put, and although each regiment apparently had its full quota of medical officers, even this number was not enough to care for men in malaria-ridden country under the prolonged stress that characterized Grant`s campaign against Fort Henry and FortDonelson.46
In the West, as in the East, the responsibility for general hospitals and that for field hospitals were often assigned to different men. As a result, Grant`s senior surgeon, James Simons, as well as the medical officer who sometimes acted in Simons` stead, John Brinton, often remained in the north at Cairo, Illinois, while Henry Hewit, a volunteer surgeon, accompanied Grant and served as his medical director in the field. Hewit sent one surgeon with each regiment into battle, ready to render whatever immediate care might prove necessary. The regimental medical officer then sent the wounded back to a depot where ambulances could meet them. From these depots, the wounded were taken to large hospitals established out of the line of fire in whatever buildings were available and if necessary in tents, Hewit`s main problem being the lack of suitable shelter. Hewit also formed ambulance trains, each managed by a noncommissioned officer. Although his arrogance and rough manners alienated U.S. Sanitary Commission officers, his system, an unsophisticated version of that later devised by Letterman in the East,a pparently worked well, even when snow and sleet fell upon the battlefield. Within several days of the struggle for Fort Donelson in February, and apparently after a period of neglect, the wounded were shipped by steamer to the Cumberland River and thence to general hospitals at Mound City, Illinois, and Paducah, Kentucky, as well as at Cincinnati, St. Louis, and Louisville. The troops remaining in the field soon began to succumb to stress and disease, and those stricken with dysentery,
44MSH 1, app.:23; Ltr, Murray to Finley(22 Jan 1862), RG 112, entry 12; USSC, Sanitary Memoirs, p. 55;U.S. Army, Surgeon General`s Office, Medical History of the Army of the Ohio and the Cumberland, 1862, Ms C125, p. 5, NLM.
45USSC, Sanitary Memoirs, p. 55; Ms C125, pp. 1-2, NLM.
46Unless otherwise indicated, all material on Fts. Henry and Donelson and the battle of Shiloh is based on MSH 1, app.:23-44.
197
JAMES SIMONS.(Courtesy of National Library of Medicine.)
{kind=link}
diarrhea, pneumonia, and typhoid fever began to join the wounded under the care of Hewit`s medical officers.47
After the capture of Fort Donelson, Grant`s army traveled by steamer 120 miles from Fort Henry to Savannah, Tennessee. The men were packed closely together, and many apparently remained on board for some time after their arrival at their destination. As a result of the long confinement in close quarters, a typhoid fever epidemic struck, and many died. Supplies of medicines and hospital space ran short, and hospital tents could not be found. Only one steamer was available to move the sick; the quartermaster`s men occupied her lower deck and apparently scheduled her use, giving the Medical Department a low priority. Grant ordered Brinton to travel to St. Louis to see whether he could obtain more vessels. "After some delays," Brinton reported, he "succeeded in procuring other steamers, the first of the noble hospital fleet of the western waters."48
HENRY HEWIT.(Courtesy of National Library of Medicine.)
{kind=link}
By the time the Confederate forces attacked Grant`s army at Shiloh on6 April, a "prolific diarrhea that resisted obstinately the ordinary therapeutic means" had added to the afflictions of his men. In combination with malaria, this ailment, which was blamed on the water of the Tennessee River, greatly weakened many of Grant`s soldiers. The nature of the battle,
198
furthermore, made prompt and proper care of the sick and wounded extremely difficult, for in overrunning the Union camp, the enemy made off with the medical supplies, stretchers, and ambulances they found there. No shelter was available to protect the wounded from a heavy rain, bedding was nonexistent, and food supplies were low. Nevertheless, medical officers made the best use of what they could find, while sending a "pitiful telegram" to the newly installed Surgeon General Hammond asking for help. The reply they received the next morning promised 10,000 mattresses which, unlike the items requested by Tripler during the Peninsular campaign, "came with wonderful quickness." Grant ordered that all tents in his army be taken over for the use of the wounded, and at least one surgeon made wholesale use of captured tents for his patients. Hewit, as Letterman would do several months later, appointed his most skilled surgeons to conduct all operations. Steamers, including the fleet provided by the U.S. Sanitary Commission, aided in evacuation, and Hewit ordered a medical officer to board each vessel and to perform en route further surgery as needed.49
When Buell`s army arrived to aid Grant at Shiloh, his surgeons could offer little in the way of medical supplies to ease the effects of the shortage. They had few of the needed items with them because they had moved so quickly. A few days after the battle, however, the supply train arrived, along with "constant stream of civilian surgeons, and sanitary commission agents, men and women," and a constant stream of the sick as well. Steamers took them off by the thousands, while three doctors at a nearby convalescent hospital screened those who appeared chronically ill before discharging them from the service. The work load of the medical officers at Shiloh began to diminish only many days after battle.50
The spectacle of unnecessary suffering brought about by the lack of tents and medical supplies at Shiloh apparently did not impress General Buell with the need to give his medical director more support. Before the battle of Perryville, Kentucky, on 8 October, for example, after Murray had carefully acquired all the supplies needed for each regiment, Buell ordered that everything that could not be carried in one wagon per brigade be left behind. Since his men were not allowed to bring tents with them, none were available for use by surgeons. The strain of the long march that preceded the battle was great, and illness took a heavy toll above and beyond that of the battle itself. After the conflict, Buell abandoned the sick, without tents, often without shelter of any kind, without blankets, without bedding. Supplies that had been ordered were inexplicably held up by the quartermaster and did not arrive for two weeks. Thousands were ill with typhoid fever, erysipelas, measles, diarrhea, and dysentery, and only the prompt aid of the U.S. Sanitary Commission prevented an even greater disaster. When the sick and wounded could be moved, they were evacuated, usually in empty wagon trains used by the commissary to carry stores.51
Major General William Rosecrans, who led the Army of the Mississippi before succeeding Buell in command of the Army of
49First quote, MSH 1, app.:29; second and third quotes, Brinton, Memoirs, p. 171; see also Maxwell, Sanitary Commission, p. 132, and Duncan, Medical Department, pt. 3, p.4.
50Quote from Sherman, Memoirs 1:246; Ltrs, McDougall to Hammond (4 and 8 May 1862), both in RG 112, entry 12.
51USSC, Documents 1, no. 56:1, 15. Unless otherwise indicated, all material concerning operations in the West in the fall of 1862 is based on MSH 1, app.:242-65.
199
the Cumberland in October, was a man more in Grant`s mold than in Buell`s. In Mississippi, at both the battle of Iuka on 19 September and that of Corinth in early October, the surgeons with his army were well supplied with all they needed, from tents to ambulances. The establishment of hospitals was easily managed and, according to his medical director, surgeon Eben Swift, the wounded received prompt and excellent care. Oddly enough, however, Swift also noted, without explanation but almost proudly, that patients wounded at Iuka received no anesthetic and that "not a groan or sign of pain was heard." Even after the battle of Murfreesboro in Tennessee in late December, when the hospitals of the right wing, their wounded, and their supplies were captured, when the killed and wounded eventually numbered about 4,000, and when several surgeons deserted, the ambulance corps "worked admirably" under the system originally set up by Murray, and Swift was able to provide "comfortable shelter for all."52
EBEN SWIFT.(Courtesy of National Library of Medicine.)
{kind=link}
Although the engagements west of the Mississippi in 1862 did not become as famous as the battles of Shiloh, Antietam, and Fredericksburg, two battles each resulted in at least 800 wounded. In March the battle of Pea Ridge in northwestern Arkansas left almost 1,000 injured, while in December about 800 were hurt in the struggle at nearby Prairie Grove. The surgeons involved faced the same problems as their counterparts east of the Mississippi. Supply was particularly difficult. The end of the Pacific Railroad was in Rolla, Missouri, 240 miles from the battlefields in Arkansas, and Confederate raiders easily cut off supply wagons before they reached their destination. Buildings of a size adequate for hospital use were also hard to find, but the lack of a network of deep rivers made evacuation to distant general hospitals difficult. Because ambulances and wagons had to use rough roads, medical officers preferred not to move their patients far. The number of casualties forced surgeons to rely heavily on the Western Sanitary Commission for hospital supplies, bedding, and clothing after both battles, but by late December medicines, hospital stores, and ambulances were plentiful.53
Most of the casualties from the Arkansas battles remained west of the Mississippi, and at least one general hospital, near Las Vegas, New Mexico, was established to care for the wounded from military action in the Far West. This facility, established at a hot
52Quotes from MSH 1, app.:256.
53Forman, Western Sanitary Commission, pp. 27-30, 61-62;MSH 1, app.:340-43.
200
spring a few miles from the town, served more as a shelter for convalescents than as a hospital because the seriously ill or wounded could not tolerate the long overland trip necessary to reach it. When a few casualties from beyond the Mississippi ended up in general hospitals of the Midwest, however, complaints arose because nurses were not always sent with the sick and wounded, and officers commanding units near the hospitals were thus forced to detail their own men to care for patients from other commands.54
Conclusion
The problems of the Medical Department were much the same in both the East and the West, and the solutions devised to deal with them were generally similar. The immediate care and evacuation of the wounded from the battlefield was everywhere largely dependent upon the tide of battle. Patients could never be guaranteed speedy and efficient care, but medical directors learned much in 1862 that helped them devise a more effective chain of evacuation from battlefield to general hospital. As line officers began to understand both the importance of speedy evacuation and efficient medical care and the nature of the problems facing the Medical Department, the significant progress already made in dealing with the administrative problems involved in evacuation would continue. Nevertheless, as the year came to a close, medical problems in the form of disease and infection were becoming increasingly insistent. The sick rate was three to five times that found in young civilian men because as the Army expanded, ever larger numbers of men were being thrown together under conditions of stress, inadequate sanitation, and poor diet. Efficiency required centralization, and the sick and wounded would be crowded into hospitals that were increasing in size. As a result, the growing threat of typhoid, erysipelas, scurvy, and other forms of disease and infection cast ahead of it an ominous shadow as 1862 drew to a close.55
54Sherman, Memoirs 1:274; MSH1, app.:346-47.
55Jarvis, "Sanitary Condition," p. 473.
![]()