



A Decade of Progress - Contents
Meeting the Challenge in War and Peace
We must be ready to dare all for our country.For history does not long entrust the care of freedom to the weak or the timid.-DWIGHTD. EISENHOWER.
COMBAT READINESS
The Army Medical Department prepares in peace for service inwar. Preparedness involves many tasks and functions, none of which isindependent of the others-mobilization and contingency planning to ensure thatthe right unit is at the right place at the right time; stockpiling of essentialmedical supplies at carefully selected sites to fill the gap until routinesupply procedures become possible; development of lightweight, durable fieldequipment for mobility on the battlefield; intelligence operations to gatherinformation on medical conditions in any area of the world where U.S. combatforces might be committed; and modification of the organization and structure ofmedical field units in response to changing strategic concepts and tacticalrequirements. Demanding, challenging, and necessary work, but at best, anestimate of needs and requirements. Combat, and combat alone, is the test ofcombat readiness.
EMERGENCY MISSIONS
Apart from combat support operations in South Vietnam, theability of the Army Medical Department to
186
react quickly in an emergency was significantly tested onthree occasions in the past decade. The first of these tests, the LebanonOperation, was completed before General Heaton became The Surgeon General.Because the evaluation of medical support activities was completed after heassumed office, and because he directed that the lessons learned in Lebanon beused as a basis for improving and strengthening such support operations, adiscussion of the operation has been included in this account.
Lebanon Operation, July 1958
The dispatch of U.S. Armed Forces to Lebanon early inJuly 1958 provided the first real test since the Korean War of how well the ArmyMedical Department was accomplishing one of its basic missions-combatreadiness. The number of participating troops ashore was approximately 13,000,including marines, and the operation lasted slightly more than 3 months(July-October 1958). No combat was involved; instead a "semigarrison"situation was encountered, with most of the medical problems being in the fieldof preventive medicine. Nevertheless, the incident did provide a test of thecapability of the Army Medical Department to deal with a sudden, unexpectedsituation in an overseas area.
The Army medical units that participated in this operationwere dispatched by air or water from Europe to Lebanon. The 58th EvacuationHospital was the largest medical treatment unit committed. Units deployed toLebanon in addition to the 58th Evacuation Hospital included the 4th SurgicalHospital (Mobile Army); the 1stClearing Platoon, 24th Airborne Brigade; Medical Platoon, 187th Airborne BattleGroup; medical detachments of the 3d Tank Battalion and the 299th EngineerBattalion; 100th Veterinary Food Inspection Detachment; and the 485th PreventiveMedicine Company. U.S. Army, Europe, also supplied the medical personnel for theHeadquarters, American Land Forces (Provisional).
187
To provide a focal point for compiling data,for developing emergency requirements, and for analyzing and disseminatinginformation, an Emergency Operations Center was established in the Office of TheSurgeon General. The center was abolished in October 1958 when the emergencyended.
A study conducted in the Office of The Surgeon General at therequest of the Assistant Secretary of Defense (Health and Medical) found thatseveral published accounts which were critical of the medical support in theinitial phase of the operation were nevertheless reasonably accurate andconstructive in nature. Subsequent detailed analysis established that ArmyMedical Department personnel performed their basic mission in a creditablemanner. Early deficiencies were resolved, and the effectiveness of the MedicalDepartment increased as the operation progressed.
On the basis of The Surgeon General's study, and similarstudies conducted in the offices of the Surgeons General of the Navy and the AirForce, the Secretary of Defense, on 14 March 1960, requested the Joint Chiefs ofStaff to include a permanent medical staff in the headquarters of eachestablished unified and specified command. He also asked that a medical staffsection be included in the headquarters of any specified commands set up for anoperation in which the use of a significant number of troops was anticipated. On17 June 1960, the Joint Chiefs of Staff directed the commanders of unified andspecified commands to establish the medical elements required by this newpolicy.
Insofar as the Medical Department was concerned, a number ofimportant lessons were learned in the course of the Lebanon Operation which werelater incorporated in operational plans. One was that medical support,particularly preventive medicine support, must accompany the first contingent oftroops, since medical problems are greatest at the onset of a campaign. A secondwas that sanitary orders must be prepared for issue before troops are committed.These orders should be sufficiently
188
comprehensive and detailed to assure maximum protection fromdisease. Third, preventive medicine units included in the task force must havebalanced and complementing organic elements reflecting all their capabilitieswhen they are committed. Survey and control sections should be committedsimultaneously to be effective. A fourth was that, in planning phased shipmentof organizational equipment, adequate insect and rodent control materiel must beincluded in the first or second phase. A fifth was that The Surgeon General mustbe provided with timely and comprehensive statistical and sanitary reports fromany joint commands in which Army troops are involved. Sixth, in planning foroperations of this type, an appropriate medical staff must be assigned to assurepreparation of adequate medical plans and to coordinate, control, and supervisethe execution of these plans. A seventh was that planning for any task forceoperation must provide for sufficient surgical capability concurrent with thearrival of troops in the area. An eighth was that plans should be developedwhereby individuals are not only designated for deployable units but are alsoindoctrinated and trained with the unit for their assigned mission. A ninth wasthat careful study must be made to ascertain that the troop lists and theequipment lists will satisfy anticipated requirements. Finally, automatic supplyshipments must be augmented with adequate quantities of any unusual items thatmight be required because of the nature of the country in which the task forceis to operate.
The Cuban Crisis, October 1962
The heaviest emergency demands upon the Army during 1962 weremade because of the forces deployed to South Vietnam. Closer to home than thechallenge in Vietnam was the Communist threat in Cuba that developed duringOctober of that year. When the crisis over the U.S.S.R. buildup of missiles inCuba arose in October 1962, the Army moved swiftly to prepare for
189
an outbreak of hostilities. On 16 October, it designated theCommanding General, U.S. Continental Army Command, as Commanding General, U.S.Army Forces, Atlantic, to assist the Commander in Chief, Atlantic, incontingency planning for an assault on Cuba.
War rooms and operational headquarters went on a wartimefooting in mid-October, and the Army sent alerts to its forces around the world.After President John F. Kennedy's speech on the Cuban crisis on 22 October, theArmy began to move combat and support units to assembly areas. The 1st ArmoredDivision moved on 23 October from Fort Hood, Tex., to Fort Stewart, Ga., whereit would be more accessible to port facilities. Signal units came from FortGordon, Ga., Fort Carson, Colo., and Fort Bragg, N.C.; artillery batteries andreplacement companies from Fort Lewis, Wash.; ordnance units from Fort Meade,Md.; transportation companies from Fort Eustis, Va.; hospital trains from Ogden,Utah; field hospitals from Fort Leonard Wood, Mo., Fort Sam Houston, Tex., andFort Bragg; and quartermaster units from Fort Lee, Virginia.
Nearly 200,000 troops and more than 100,000 tons of equipmentwere moved during the crisis. Troop units were located near outloading ports sothat they might reach the objective area quickly, should the need arise.
The Army established forward headquarters of U.S. ArmyForces, Atlantic, at Homestead Air Force Base, Fla., to coordinate Armyactivities in the base areas, and set up the Peninsular Base Command atOpa-Locka Air Force Base, Fla., to provide logistic and administrative supportof all Army troops in the Florida area.
In the meantime, the Third U.S. Army executed plans for thedefense of the southeastern United States and the Florida Keys. NIKE-HERCULESmissile units were deployed to provide area defense against medium- andhigh-altitude targets, and HAWK missile units guarded against low-level attacks.
The Army force remained ready until the crisis passed.Redeployment began on 29 November when the first
190
Army unit, a signal battalion, departed forFort Bragg. By 20 December, all major Army combat units had returned to homestations, with the exception of the air defense units still defending againstthe existent Cuban air threat.
The support mission assigned to the Army Medical Departmentfully tested the capability of medical personnel to implement plans for suchcontingencies. Within a week, a medical force of a medical group, four fieldhospitals, a clearing platoon, several motor ambulance platoons, a mobilelaboratory and blood bank, and a medical depot were in a state of operationalreadiness in Florida. Commenting on The Surgeon General's role in the Cubancrisis, Major General Conn L. Milburn, Jr., then Chief Surgeon, U.S. ArmyPeninsular Base Command, said:
General Heaton's capacity ofleadership was never more evident than the prompt and effective manner in whichhe met the Army Medical Department's challenge in the Cuban Affair in the fallof 1962. * * * As Surgeon of the Logistical Commandassigned in Florida to support the operation, I had the opportunity of seeing atfirst hand the manner in which General Heaton met a condition of crisis. Heimmediately grasped all of the facts concerned with the operation, analyzed themperfectly, and formulated a successful plan of execution. * ** As the Chief Surgeon on the spot in Florida, I was amazed at thesplit-second efficiency of General Heaton and his staff in meeting this crisisof such national importance.
The Dominican Republic Crisis, April1965
The ability of the Army Medical Department toreact quickly in an international emergency was significantly tested a secondtime in late April 1965. At that time, an abortive military coup in theDominican Republic set off a chain of events which led to the partial collapseof governmental authority, leaving sections of the capital city of Santo Domingoin the hands of Communist-infiltrated armed mobs. This necessitated the directemployment of U.S. combat forces to evac-
191
uate U.S. citizens and other foreign nationals, to prevent Communist elementsfrom seizing control of the government, and to allow time for the Organizationof American States to effect a cease-fire and prepare the way for freeelections.
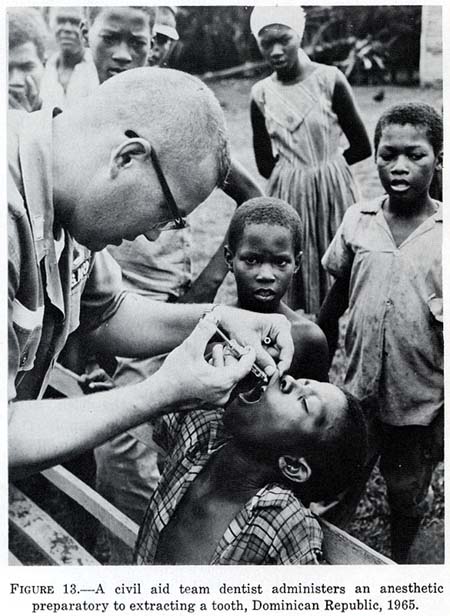
The dispatch of U.S. Armed Forces to the Dominican Republic provided arealistic test of Army Medical Department combat readiness. During the firstweek of this operation, 39,000 pounds of medical supplies for civil relief and2,800 pounds of medical supplies for U.S. military use were airlifted to SantoDomingo. In addition to their normal mission of providing medical support toU.S. Army troops, Army Medical Department units assisted the civil populationand treated casualties of both sides, loyalist and rebel (fig. 13).
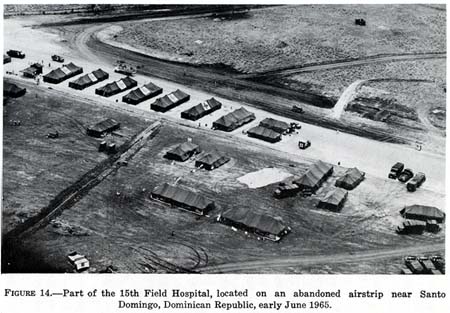
The 15th Field Hospital, the largest medical treatment unit committed (fig.14), received an average of 86 admissions a week. Units deployed to theDominican Republic in addition to the 15th Field Hospital included the 584thAmbulance Company, the 53d Surgical Team, the 714th Preventive Medicine Team,the 54th Helicopter Ambulance Detachment, the 545th Supply Detachment, the 139thOrthopedic Team, and the 307th Medical Battalion.
MERCY MISSIONS
Chile Disaster Relief Operations
After the devastating earthquakes and quake-generated tidal waves in Chilelate in May 1960, the Chilean Government appealed to the U.S. State Departmentfor assistance. Acting quickly in response to this appeal, the Joint Chiefs ofStaff, on 25 May, authorized the U.S. Army to airlift two fully staffed andcompletely equipped field hospitals to the disaster area to assist in theevacuation and care of the injured and to help prevent outbreaks of epidemicdiseases.
192
FIGURE 13.-A civil aid team dentist administers an anesthetic preparatory to extracting a tooth, Dominican Republic, 1965.
{kind=link}
The hospitals selected for this mission were the 15th Field Hospital from Fort Bragg, N.C., and the 7th Field Hospital from Fort Belvoir, Va. The former was staged out of Pope Air Force Base, Fort Bragg, and the latter out of Andrews Air Force Base, Washington, D.C. Each hospital was augmented by an Engineer Corps water
193
FIGURE 14.-Partof the 15th Field Hospital, located on an abandoned airstrip near Santo Domingo,Dominican Republic, early June 1965.
{kind=link}
194
purification unit, a Quartermaster Corps laundry detachment, and a SignalCorps communications team. The airlift, which involved about 1,230,000 pounds ofArmy supplies and equipment and 550 Army personnel, required the use of 59 gianttransport aircraft of the Military Transport Service (C-124 Globemasters and C-118's).It was the Army's largest emergency airlift since the Lebanon Operation in1958.
The first aircraft to leave on the 6,000-mile flight to Chile departed fromPope Air Force Base at 0509 hours and the second from Andrews Air Force Base at0549 hours on 26 May. These flights were the beginning of an airstreamwhich continued at the rate of approximately one plane per hour until the lastof the huge planes was airborne. The principal limiting factor in the airliftwas the lack of capability of the intermediate and destination airfields toservice the large transport aircraft.
To support the operations of the Army units, rations for 15,000 patients, 225 aid station supplement packs, and two medical maintenance units (medical resupply packs) were also included in the initial military airlift. Later, in response to an appeal from the Chilean National Health Director, the Louisville Medical Depot shipped 1,400 bottles of tetanus vaccine and gas gangrene antitoxin by commercial aircraft.
During the afternoon of 26 May 1960, the Joint Chiefs of Staff requested that the Army send 10 helicopters to Chile to assist in the disaster relief operations. Two medical helicopter ambulance detachments, the 56th from Fort Bragg, N.C., and the 57th from Fort Meade, Md., equipped with the new Iroquois (Bell HU-1A) helicopter, were loaded into the maws of C-124 aircraft and placed into the airstream to Chile. A small (12-man) Transportation Corps detachment accompanied the helicopter units to provide maintenance support.
These Medical Department helicopters, piloted by Medical Service Corps officers, played an important role in
195
the relief activities by surveying the disaster areas and by evacuating theinjured and rescuing the homeless from outlying and isolated regions, some ofwhich were virtually inaccessible except by helicopter. The helicopters alsoflew food, blankets, clothing, medical supplies, and medical personnel toregions where the people were in distress. Many of the missions flown were insupport of the extensive program that was carried on to suppress epidemics byflying Chilean physicians to administer mass inoculations.
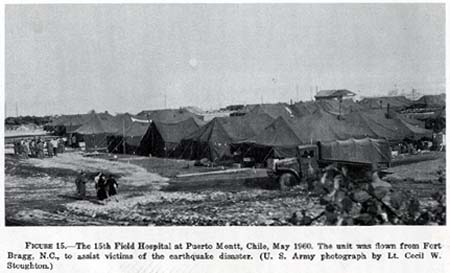
Upon arrival in Chile, the planes carrying the 15th Field Hospital wererefueled at Santiago before continuing about 500 miles south to Puerto Montt,where the hospital was unloaded and its tents set up in a stadium. The 7th FieldHospital had to be unloaded at Santiago and then moved by rail and truck to itssite in Valdivia, which did not have adequate facilities for handling the C-124aircraft. The hospitals began operations on 29 May and 1 June, respectively.
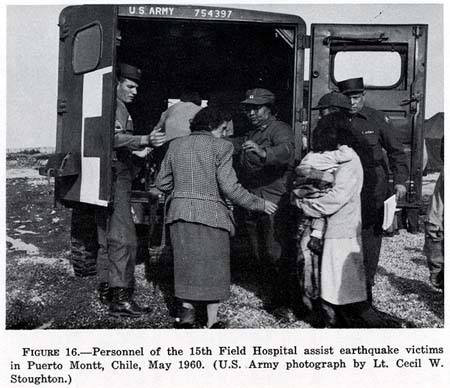
It soon became evident that the medical assistance required by Chileanphysicians in caring for disaster victims was not so great as had beenanticipated (figs. 15 and 16). In some instances, the tent wards of the fieldhospitals were pressed into service as temporary housing for refugees.
The 7th and the 15th Field Hospitals were the two largest medical treatmentfacilities sent to Chile. Units deployed to Chile in addition to these fieldhospitals were the 56th and 57th Medical Helicopter Ambulance Detachments, twolaundry detachments from the 496th Quartermaster Company, two water purificationunits from the 19th Engineer Battalion, two Signal Corps teams from the 50thSignal Battalion, and a detachment from the 25th Transportation Company(Maintenance).
All personnel of the Army units sent to Chile, except for small reardetachments, had accomplished their missions and had returned to their homestations by 30 June. Meanwhile, the U.S. Government announced its
196
FIGURE 15.-The15th Field Hospital at Puerto Montt, Chile, May 1960. The unit was flown fromFort Bragg, N.C., to assist victims of the earthquake disaster. (U. S. Armyphotograph by Lt. Cecil W. Stoughton.)
{kind=link}
197
FIGURE16.-Personnel of the 15th Field Hospital assist earthquake victims in PuertoMontt, Chile, May 1960. (U.S. Army photograph by Lt. Cecil W. Stoughton.)
{kind=link}
198
decision to donate all the equipment of the two field hospitals to theChilean Government. This transfer was completed by mid-July.
Apart from the humanitarian aspects of the mission to Chile, the airliftdemonstrated that a fully staffed and completely equipped field hospital couldbe assembled, transported, and set up for operation within a relatively fewhours, regardless of the distances involved. The 56th and 57th MedicalHelicopter Ambulance Detachments were selected by the American HelicopterSociety as recipients of the William J. Krossler Award for 1960 because of theiroutstanding performance during the Chilean disaster.
Earthquake Disaster Skopje, Yugoslavia
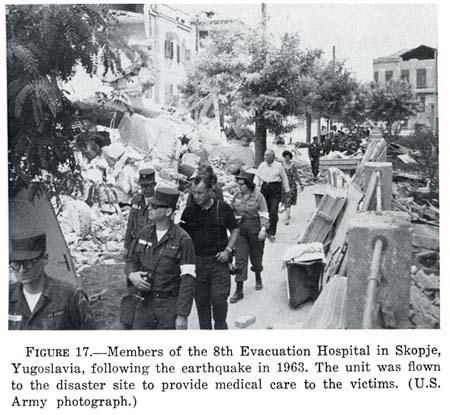
The readiness of the Army Medical Department to react to an emergencysituation was demonstrated when the United States assisted the disaster victimsin the Skopje, Yugoslavia, earthquake. On 27 July 1963, a 120-bed unit,reinforced, of the 8th Evacuation Hospital (fig. 17) at Landstuhl, Germany, wasairlifted from Ramstein Air Force Base at 2245 hours. The next morning, the unitarrived at Belgrade at 0730 hours, and departed an hour later for a 270-mileoverland move to Kumanovo, some 20 miles from Skopje. It became operational at0200 hours on the 29th, some 27 hours after takeoff, which included a 12-hourroad movement.
Earthquake and Flood Disasters, Alaska
On 27 March 1964, a severe earthquake caused widespread damage in Alaska.Anchorage was hard hit. Seward, 130 miles southeast of Anchorage, was damaged bythe earthquake, seismic sea waves, and fire. Valdez, Whittier, and Kodiak werealso heavily damaged by earth tremors and seismic sea waves.
The Army Medical Department responded promptly. In a matter of a few hours, amedical team of five doctors, 12 nurses, and 20 enlisted technicians from Mad-
199
FIGURE17.-Members of the 8th Evacuation Hospitalin Skopje, Yugoslavia, following the earthquake in 1963. The unit was flown tothe disaster site to provide medical care to the victims. (U.S. Armyphotograph.)
{kind=link}
igan General Hospital and Fort Lewis, Wash., was dispatchedto the scene to assist the 64th Field Hospital in Alaska. Alerted and ready torespond also were the 27th Surgical Hospital and the 47th Field Hospital.
Alaska experienced a second major disaster in the summer of1967. On 14 August, the Chena and Tanana Rivers near Fairbanks overflowed theirbanks, causing widespread damage to Fairbanks and Fort Wainwright. The risingfloodwaters made further operation of St. Joseph's Hospital, the only civilianhospital in Fairbanks, impossible. At the request of the Mayor of Fairbanks, the68 patients at St. Joseph's Hospital were evacuated to Bassett Army Hospital.Thereafter, Basset Army Hospital provided emergency hospitalization for thecivilian population until St. Joseph's was reopened on 6 September 1967.
Apart from these major missions, the Army Medical
200
Department has assisted in a number of minor operations suchas the relief of flood victims in Italy, earthquake disaster victims in Morocco,and the drought and famine stricken populace of the Somali Republic. In carryingout these mercy missions, it has served, in General Heaton's words, "asan instrument of peace in a war-torn world."
MEDICAL SUPPORT IN SOUTH VIETNAM
Field Medicine
President Lyndon B. Johnson's decision in July 1965 tocommit substantial U.S. forces to Southeast Asia placed the Army on thethreshold of one of its most challenging periods since World War II. The urgentneed for rapid deployment of sizeable Army forces and resources to SouthVietnam, while maintaining a state of readiness to meet contingencies elsewherein the world, created demands that were felt by every member and activity of theArmy. The Army Medical Department was thus faced once again with the challengeof maintaining and restoring the health of American soldiers fighting for theprinciples of freedom on foreign soil. As so many times before in the 194-yearhistory of the Medical Department, the story is one of highly trained anddedicated men and women working heroically to provide the American fighting menthe finest possible medical care.
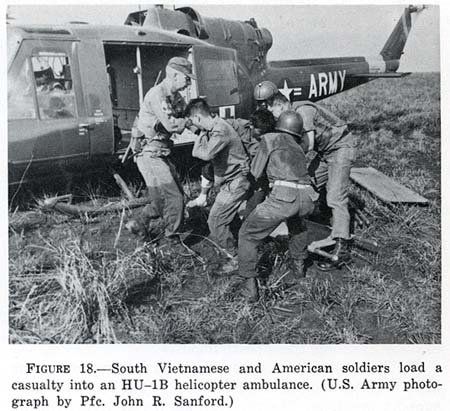
There are many individuals who could be singled out forpraise-the aidmen who, with no thought for their own safety, render emergencymedical care before and during evacuation; the helicopter crews who brave enemyfire to rescue the wounded and fly them quickly from the scene of battle tohospitals (fig. 18); the talented and dedicated doctors, nurses, and techniciansworking long hours, both to save the lives of wounded brought in from battle andto provide everyday medical care so vital to maintaining the health of militaryand civilian person-
201
FIGURE18.-South Vietnamese and American soldiersload a casualty into an HU-1B helicopter ambulance. (U.S. Army photograph byPfc. John R. Sanford.)
{kind=link}
nel engaged in the struggle in Southeast Asia. Working behindthe scenes are countless others, such as the administrators who keep the medicalfacilities operating smoothly and the researchers who work constantly to masterthe problems which arise to develop new equipment to provide better treatment.
In January 1965, the Army Medical Department had 110 hospitalbeds operational in South Vietnam. By June 1969, there were more than 4,750 beds in 21 installationswhich provided hospital service to the largest forces the United States hasfielded since World War II. Concomitant with this buildup of facilities andunits was the development of an effective organizational structure to coordinateand direct the activities of the Army Medical Department in Vietnam.
The 44th Medical Brigade was responsible for allnon-divisional medical service in support of Army forces in
202
South Vietnam. Initially a subordinate unit of the 1stLogistical Command, command control of this unit was transferred to the U.S.Army, Vietnam, on 10 August 1967. The Commanding General, 44th Medical Brigade,thus also functioned as Surgeon, U.S. Army, Vietnam.
While the 44th Medical Brigade was the principal medicaloperating agency of the U.S. Army, Vietnam, not to be overlooked were thedivisional medical elements, the aviation dispensaries of the 1st AviationBrigade, the floating medical stations of the 9th Infantry Division, and the"dustoffs" of the airmobile 1st Cavalry and 101st Airborne Divisions,as well as others. These "medics" constituted about one-third of themedical troops with the U.S. Army, Vietnam. They were the people who manned thevital facilities which kept a wounded man alive until the hospitals could takeover the task. Five of these heroic corpsmen (fig. 19) were awarded the Nation'shighest decoration, the Medal of Honor, for bravery in action, threeposthumously.
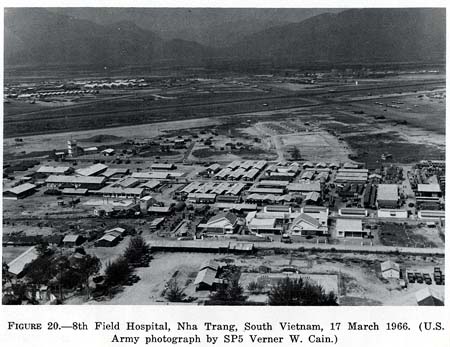
All Army hospitals in South Vietnam, including the MUSTunits, were fixed installations (fig. 20) with area support missions. Thepeculiar nature of counterinsurgency operations in South Vietnam and thetropical environment there required modification of the usual concepts ofhospital usage in a combat area. Since there was no secure road network in thecombat areas of Vietnam, surface evacuation of the wounded was bothimpracticable and almost impossible. Therefore, air evacuation of the injuredbecame routine. The importance of getting the casualty and the doctor togetheras soon as possible was an axiom of Medical Department philosophy. Thehelicopter was achieving this goal as never before. Of equal importance was thefact that the Medical Department was getting them together in a hospitalenvironment equipped to meet almost any situation. The degree of sophisticationof medical equipment and facilities everywhere in South Vietnam permitted Armyphysicians to make full use of their training and capability. As a result, thecare that was available in Army hospi-
203
FIGURE 19.-Specialist LawrenceJoel, first medical aidman to be awarded the Medal of Honor for service inVietnam. (U.S. Army photograph by Oscar E. Porter.)
{kind=link}
tals in South Vietnam was far better than has ever beengenerally available for combat support previously. All hospitals had facilitiesfor determining blood pH. Many, including all the evacuation hospitals, hadfacilities for doing blood gas determinations. Whole blood was consistentlyavailable in sufficient quantities. Many patients survived because means wereavailable to render massive transfusion. Procedures such as repair of arterialinjuries by anastomosis or vein grafting, which were
204
FIGURE20.-8th Field Hospital, Nha Trang,South Vietnam, 17 March 1966. (U.S. Army photograph by SP5 Verner W. Cain.)
{kind=link}
205
done by only a few selected surgeons in the Korean War, were performed routinely. For example, about 2,000 vascular repairs were performed in South Vietnam. Partial hepatectomy for certain liver injuries kept alive some patients who would undoubtedly have succumbed to older methods of treatment.
The backbone of this life-saving system was the helicopter ambulancecompany(fig. 21), which greatly shortened the critical time from wound to operatingtable. Several scores of flying "medics" whirled their unarmedhelicopters into hostile areas, risking their own lives to save those of others."Dustoff," so known from their radio call signal, medical evacuationflights averaged only about 35 minutes each, a feat which often meant thedifference between life and death for hundreds of patients. Of the wounded whoreached medical facilities, about 97.5 percent survived.
The helicopter air ambulances assigned to Vietnam evacuated approximately8,000 casualties each month during the Vietcong offensive in early 1968. Ofthese, approximately 27 percent were Vietnamese and another 5 percent werecasualties from other free-world nations. Army air ambulances completed morethan 94,000 aeromedical evacuation missions while flying approximately 47,000combat hours.
Helicopters were aided by new equipment designed especially for use in jungleterrain. The forest penetrator was a spring-loaded device which may be attachedto the end of a hoist cable and used to retrieve patients from areas too densefor a helicopter to land. The device was used extensively and to great advantagein Vietnam. Highly mobile and widely deployed forces must have a highly mobileand flexible medical evacuation system immediately responsive to their needs.The Army Medical Department developed such a system. Aeromedical support wasprovided by almost 140 air ambulances. These helicopters could transport six tonine patients at a time, depending upon the number of litter cases, and wereparticularly effective. The more seriously wounded usu-
206
FIGURE21.-General Heaton during a visit to South Vietnam inNovember 1967. (Walter Reed Army Institute of Research photograph.)
{kind=link}
207
ally reached a hospital within 1 to 2 hours of the time oftheir wounding.
The helicopter brought modern medical capabilities closer tothe frontline than ever before. Furthermore, combined with a medical radionetwork, the helicopter provided greater flexibility in regulating patients.Preliminary evaluation of the injury and the condition of the patient was madewhile in flight, and the use of the radio network permitted redirecting thepatient to the nearest hospital suited to his needs (fig. 22). Also, somehospitals may develop surgical backloads, and the combination of helicopter andradio facilitated regulating patients according to the immediate availability ofoperating facilities, rather than available beds. This combination was the coreof the Army medical support system in Vietnam.
The patient evacuation policy for South Vietnam wasestablished as a 15-day minimum or a 30-day optimum. Under this policy, it waspossible to return to duty in South Vietnam nearly 40 percent of those injuredthrough hostile action and 70 percent of other surgical patients.
Initially, out-of-country medical regulating was controlledat the Far East Medical Regulating Office in Japan through a representativefunctioning at the Office of the Surgeon, U.S. Army, Vietnam. Out-of-countryevacuation was by aircraft to Clark Air Force Base in the Philippines, followingwhich evacuees were subsequently routed either to the continental United States;to Tripler General Hospital in Hawaii; to the U.S. Army Hospital, RyukyuIslands; or to Japan. Since the summer of 1966, however, direct evacuation ofpatients from South Vietnam to the continental United States via one stop inJapan by means of jet aircraft has been in operation.
Patients received in the continental United States werelargely accommodated in general hospitals nearest their homes, but some wereregulated to class I hospitals even nearer their homes when these hospitals had
208
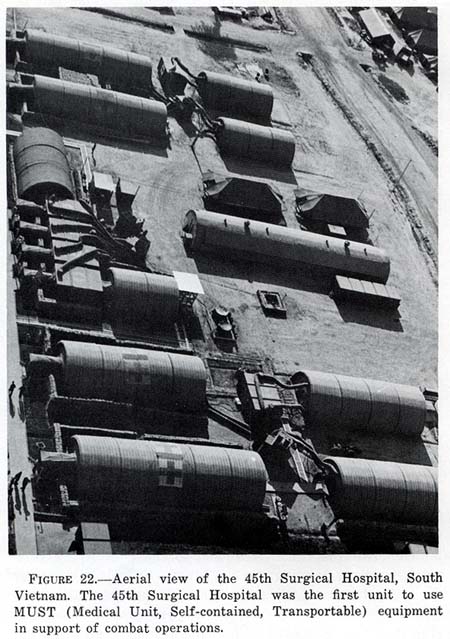
FIGURE 22.-Aerial view of the 45th Surgical Hospital, South Vietnam. The 45th Surgical Hospital was the first unit to use MUST (Medical Unit, Self-contained, Transportable) equipment in support of combat operations.
{kind=link}
beds available and the professional capability of managing their injuries.
As the entire Republic of Vietnam had been designated a combat zone, fixedhospitals that give long-term care to patients and that are normally found inthe
209
Communications Zone were not present. If all the injured or sick who couldnot be returned to duty in South Vietnam within the established 15- to 30-dayevacuation policy had been evacuated to the continental United States, it wouldhave created a great drain of experienced manpower from the combat zone. To givethis fixed-bed capability, the equivalent of about three and one-half generalhospitals were established in Japan to receive and care for patients who couldbe expected to return to duty within a period of 60 days.
Since substantial U. S. forces were committed to Southeast Asia in 1965, the relative continuity of combat wasas much a factor in building up patient leads as was the severity of fighting.Further, under such conditions, patient evacuation was accelerated to improvetheater capability for contingencies All these factors combined toincrease the flow of patients to the continental United States, directly andthrough Japan, and resulted in a rapid buildup of workloads in Army hospitals.During the first 9 months of 1968, for example, more than 21,000 evacueesoriginating from Army troops in South Vietnam were received in the continentalUnited States. Because of General Heaton's foresight in expanding thecontinental United States hospital system, physical facilities were available,and the patient flow presented no major problem.
Since 1965, General Heaton traveled more than a quarter of a million miles byair and made at least one extensive tour of the Far East each year to inspectmedical facilities and to inspire Medical Department personnel supporting thecombat soldier in South Vietnam. "Patient care in Vietnam can be describedonly in the most glowing terms," General Heaton said. Troops engaged incombat against aggression in Vietnam were supported by teams of highly trained,exceptionally skilled, and well-motivated medical personnel (fig. 23). "Ihave had the opportunity to observe these teams in action in Vietnam," headded, "and based upon my personal observation and the comments of fieldcommanders at all eche-
210
FIGURE23.-General Heaton observed patient care at an Army hospital in South Vietnamduring a visit in November 1967. (Walter Reed Army Institute of Researchphotograph.)
{kind=link}
211
lons, I can say without reservation that our fighting men are receivingmedical care which is far superior to that available to any army in any previousconflict. Never before in the history of warfare have the wounded received suchcomplete medical service so quickly."
Since 1965, disease has continued to be the biggest cause of hospitaladmissions in South Vietnam. Malaria was one of the chief afflictions. Time lostdue to illness caused by vivax malaria was about 12.5 days; the time lost fromfalciparum malaria has been reduced from 24 to 19 days, an outstanding exampleof medical advances that have been made in Vietnam.
Fevers of undetermined origin were a second major cause of hospitalization inVietnam, but the duration of such hospitalization was usually less than 7 days.Studies were underway in Vietnam to define the cause of these conditions.
Diarrheas of various types also contributed to temporary disability,including hospitalization. These conditions were usually short lived. Amebicdysentery, which normally causes a longer lasting illness, was not common amongAmerican troops.
Hepatitis occurred at a low rate, and most patients with this conditionreturned to duty within 30 to 40 days.
Although plague and cholera were endemic in South Vietnam and there had beensporadic outbreaks among the native population, there had been no cases amongU.S. servicemen. Other conditions which had occurred, but which created noserious problem, were dengue fever, scrub typhus, Japanese B encephalitis, andleptospirosis.
The U.S. Army Medical Department in Vietnam was staffed with specialists inall the surgical skills, and the care furnished casualties was superior. Withthe arrival of the specialty consultants in late 1965, an effective system ofsupervision and control of surgical care was initiated. Injuries from hostileaction constituted about 25 percent of hospital admissions. Because of the useof air evacuation of patients, Army hospitals in South Viet-
212
nam received more critically and mortally wounded patients than they had inany previous conflict. Since many of these patients could not be saved, ittended to result in higher case fatality rates. However, the survival rate forthe wounded reaching medical treatment facilities was no lower in Vietnam thanin the Korean War. Data from Vietnam indicated that of all patients with battleinjuries who were treated in medical treatment facilities, 975 per 1,000survived.
It is noteworthy that the resuscitation of the injured in Vietnam wasaccomplished largely through the use of blood, plus other fluids, withrelatively little usage of plasma substitutes such as albumin, dextran, andPlasmanate, although these were available in the theater and were used inemergencies. There was never any lack of an adequate supply of blood in SouthVietnam. Until the summer of 1966, this blood supply was collected exclusivelyin the Far East theater by the 406th Medical Laboratory in Japan from troops andother blood donors in other facilities in that theater. In the summer of 1966,this supply was supplemented by the regular shipment to the Far East of smallamounts of blood collected from military installations in the United States.
The rate of psychiatric illness in Vietnam was favorably low. Comparative statistics revealed that from a high of 101 admissions per 1,000 from one American army in the European Theater of Operations during World War II, and an average rate of 37 per 1,000 per year, in the period from July 1950 to December 1952, during the Korean War, the average admission rate for psychiatric disorders in Vietnam fell to about 12 per 1,000 per year.
Among the factors that contributed to the low incidence of emotional breakdown in American troops in Vietnam were better training, freedom from intense and prolonged artillery barrages or extended periods of combat, relatively frequent opportunities for rest and recuperation, the definite period of time of 1 year in the
213
combat zone, and refinements in the principles of combatpsychiatry such asthe availability of mental health workers at the combat level, where crisis andstress take place.
The American fighting men received medical care which was far superior tothat available to any army in any previous conflict, but the Medical Departmentcontinued its search for ways and means to improve further patient carecapability in Vietnam. Although the malaria rate decreased significantly in1968, it remained the most serious disease in South Vietnam, and a significantproblem in maintaining combat forces at peak strength. An experimentalantimalarial drug, which was expected to be more effective than the one in use,was field tested in Vietnam. Another recent advance in the fight against malariawas the development of a highly specific and extremely sensitive new test todetect malarial antibodies. Plans were underway to automate this test so that itcan be used in routine blood bank operations to confirm the acceptability of thedonor.
Since 1966, a surgical research team from the Walter Reed Army Institute ofResearch has been in South Vietnam conducting intensive studies of wound bacteriology, bloodcoagulation, blood volumes, blood gases, and pH andenzyme determinations. Use of the supraclavicular central venous catheter, aspopularized by the team, was widely utilized clinically to monitor circulatorychanges during resuscitation. The frequent use of blood gas determinationemphasized the syndrome of occult arterial hypokalemia in the severely wounded.Advanced research techniques were employed within minutes of wounding, and theinformation obtained contributed significantly to the clinical care of thesepatients. A similar team began studies at the 24th General Hospital in Japan.
Pulmonary insufficiency was found to be one of the major problems in thetreatment of both thermal and mechanical trauma. A unique and promisingcapillary oxygenator was undergoing testing. This oxygenator,
214
coupled with the Army pulsatile blood pump, which has already been usedsuccessfully in man, offered a new approach to circulatory support andoxygenation during the acute period of respiratory insufficiency.
Civic Action
The Vietnamese conflict has been described as two wars-the military effortagainst the enemy and the day-to-day struggle to win the minds and hearts of thepeople. In addition to medical support for the military effort, the Army MedicalDepartment was deeply engaged in this second effort. Medical personnel servedably and with dedication in the Military Advisory Assistance, the Medical CivicAction, and the Military Provincial Hospital Assistance Programs. They sharedtheir medical knowledge and instructed their South Vietnamese military andcivilian counterparts in the most recent medical advances. In their spare time,Army Medical Department personnel also worked voluntarily with the SouthVietnamese orphanages and sought out opportunities for expanding their help tosuch agencies. As General Heaton so aptly said:
The practice of medicine knows no language barrier and hence is one of themost effective forms of civic action. By treating the sick and injuredVietnamese, we demonstrate our concern for the welfare of the individual and ourtrue interest in the well-being of mankind. By training and advising SouthVietnamese personnel, we increase both the confidence of the native populationin their government and their ability and desire to establish democraticinstitutions.