



The Histories of the Commissions - Contents
Commission on Acute Respiratory Diseases
Incorporating Three Other Commissions: Commission on Air-Borne Infections Commission on Meningococcal Meningitis Commission on Pneumonia
This history is dedicated with grateful appreciation to Drs. John H. Dingle and Colin M. MacLeod. Dingle`s pioneering work was highly instrumental in ensuring success of the Commission on Acute Respiratory Diseases. MacLeod, his friend and associate, directed the first Commission on Pneumonia and made lasting contributions not only to a number of commissions, but to the Armed Forces Epidemiological Board. It is not possible to measure the impact of each of these two remarkable medical scientists in the whole field of preventive medicine.
Foreword
The annals of military preventive medicine provides a remarkable record of achievement extending from Beaumont to Billings to Sternberg, Reed, Strong, Siler, Simmons, and so many more. Their work was a culmination of intelligent thought and scientific innovation all aimed at solving problems that arose from those social forces and political upheavals that involve society as a whole. So often, there has been productive interaction between military and civilian scientists. Their combined opinions and collective funds of knowledge have helped determine just what should be done and how it might be accomplished, all with the aim to better maintain the highest standards of health in military personnel.
William S. Jordan, Jr., has carefully evaluated and addressed these principles in preparation of his history of four commissions of the Armed Forces Epidemiological Board (AFEB). Each commission, in its own unique way, was involved in vital issues that required identity of cause, clarification of pathogenesis, and how best to prevent specific illness in the individual and throughout the military population.
Throughout the AFEB`s illustrious history, no one has been more devoted and contributed more to the cause of prevention and control of infectious diseases in the U.S. military services than Dr. Jordan. He was in an admirable position to prepare this account of the activities of the Commission on Acute Respiratory Diseases (CARD) and three related, short-lived Commissions, having knowledge of them almost from their beginnings. John Dingle, first director of the CARD, was one of Jordan`s attendings in 1940 and 1941, when he was a medical student serving as a substitute intern on the Harvard Medical Service at Boston City Hospital (BCH). After graduation in 1942, he interned at BCH with such mentors as Drs. Chester Keefer and Maxwell Finland before active duty as a Naval Medical Officer. When home on leave in his hometown of Fayetteville, North Carolina, in the summer of 1944, he visited Dr. Dingle and the CARD laboratory at Fort Bragg. After World War II and more training at BCH, he joined Dr. Dingle`s new Department of Preventive Medicine at Western Reserve University, working there during the years that Dr. Dingle continued as director of the CARD and later as president of the AFEB. Dr. Jordan then moved to the University of Virginia School of Medicine in Charlottesville to create his own Department of Preventive Medicine and to serve for 6 years as the CARD director. Subsequently, as dean of the College of Medicine at the University of Kentucky in Lexington, and as director of the Microbiology and Infectious Diseases Program at the National Institute of Allergy and Infectious Diseases, he continued to participate in the activities of the AFEB.
Never have I known Bill to shirk a difficult assignment because of being "too busy." Furthermore, the ultimate product always came as close to the best solution as possible. Although technically retired, he continues as an involved public servant performing with his characteristic alert, vigorous, and wise approach to problem solving.
-Theodore E. Woodward, M.D.
History of the Commission on Acute Respiratory Diseases, Commission on Air-Borne Infections, Commission on Meningococcal Meningitis, and Commission on Pneumonia
William S. Jordan, Jr., M.D.
INTRODUCTION
Five of the first seven commissions formed at the first meeting (6 February 1941) of the Board for Investigation and Control of Influenza and Other Epidemic Diseases in the Army dealt with respiratory pathogens: Commissions on Influenza, Measles, Meningitis, Pneumonia, and Streptococcal Infections. At its third meeting 5 months later, the Board formed the Commission on Cross Infections in Hospitals, which was renamed the Commission on Air-Borne Infections shortly thereafter because the sterilization of air was a common problem for all groups seeking to prevent disease by limiting the dissemination of airborne organisms. Within 1 year, the Commissions on Acute Respiratory Diseases (CARD) and Neurotropic Viruses began. Thus, 7 of the first 10 commissions were concerned with airborne bacteria and viruses that cause respiratory infections.
As the Board gained experience with the commissions and as new problems were identified, new commissions were formed and existing ones merged or terminated. The Commission on Measles soon added Mumps to its title and eventually joined the Commission on Neurotropic Viruses to become the Commission on Viral and Rickettsial Diseases. The Commission on Hemolytic Streptococcal Infections was folded into the CARD in 1946 but was revived in 1949. The other three respiratory pathogen-related commissions were incorporated into the CARD after World War II,: Pneumonia in December, 1945, and Air-Borne Infections and Meningococcal Meningitis in April, 1946. These and subsequent administrative actions are listed in chronological order in Appendix 1. The research projects undertaken and observations made by the last four above-named commissions are listed in approximate order in Appendix 2.
As far as possible, study results are dated when they were reported to the Board or to the Commissions, rather than when they were published, to illustrate better the evolution of the problems explored, information gained, and control measures tested. Except for the items in Appendices I and II, the material related to streptococcal infections has been incorporated in the account of the Commission on Streptococcal and Staphylococcal Diseases (CSSD).
The following sections discuss the origins and organization of these four commissions, with emphasis on the longer-lived CARD. The scientific contributions made during their periods of service are then summarized, along with information as to the current knowledge of the etiology, epidemiology, prevention, and control of the diseases of concern to them. Lists of the publications of the Commissions are appended and will not be referenced here. Those interested in learning of the details of a particular study can do so by matching Appendix 2 with the list of publications and by consulting the supplemental references that cite the relevant and subsequent reports of others.
6
ADMINISTRATION
Acute Respiratory Diseases
The specter of a repeat of the influenza pandemic of 1918 and 1919 and its attendant high mortality from pneumonia accounted for the inclusion of influenzas the only specific disease mentioned in the title of the Board for the Investigation and Control of Influenza and Other Epidemic Diseases in the Army. The structure of the Board and its commissions was similarly shaped by the experience in these years. In World War I, the Pneumonia Commission of 1917 had supplemented undermanned military staffs with civilian physicians, and the Pneumonia Board of 1918 had organized specialist groups on short notice to investigate pneumonia whenever the need arose.
Among the commissions formed by the Board at its first meeting 10 months before the attack on Pearl Harbor were those for Influenza and Pneumonia. The minutes of this meeting note that the Influenza Commission is to include "related acute respiratory diseases," although a mission statement prepared after the third meeting of the Board just a few months later makes no mention of this fact.
One year later, at the fifth meeting of the Board in May, 1942, John H. Dingle, M.D. presented the report of a group appointed to investigate primary atypical pneumonia at Camp Claiborne, Louisiana. In addition to discussion of that disease, the minutes emphasize the difficulty in characterizing respiratory disease, noting that "advance requires a major effort in etiology and serology." There was prolonged and detailed discussion of the proposal, first outlined by Dr. Dingle in response to an informal suggestion by Colonel James Stevens (Steve) Simmons, that a permanent commission or group be established to study respiratory diseases. The Board recommended to The Surgeon General that provision be made for a permanent year-round study of respiratory disease by a specially selected group of investigators, provided details could be worked out satisfactorily. Such was the genesis of the CARD, a commission that differed from all others in that it was "organized on a full-time or permanent basis for the purpose of making a continuing study of various types of acute diseases of the respiratory tract, particularly those of undetermined etiology."
The report that Dr. Dingle presented to the Board summarized studies of the Commission for the Investigation of Atypical Pneumonia and Other Respiratory Diseases at Camp Claiborne, the forerunner of the CARD. Dr. Dingle had been studying this recently described syndrome with Dr. Maxwell Finland at the Boston City Hospital and had earlier led a team of Harvard scientists to investigate simultaneous outbreaks of diphtheria, meningococcal meningitis, and scarlet fever at Halifax, Nova Scotia, an important wartime port for the British Commonwealth. He was already a member of the Influenza Commission. Drs. Dingle and W. Barry Wood, Jr. (Associate, Department of Medicine, The Johns Hopkins Medical School, Baltimore, Maryland), a member of the Commission on Pneumonia, were dispatched by the Board to Camp Claiborne to investigate an outbreak of an unusual "acute pneumonitis." When the scope of the problem became obvious, the group of investigators was expanded by the addition of Drs. G. John Buddingh (Associate Professor of Bacteriology, Vanderbilt University School of Medicine, Nashville, Tennessee) and Alto E. Feller (Associate, Department of Internal Medicine, State University of Iowa, Ames, Iowa) of the Commission on Influenza, Drs. Theodore J. Abernethy (Associate Professor of Medicine, George Washington University, School of Medicine, Washington, D.C.) and James M. Ruegsegger (Chief, Pneumonia Service, Cincinnati General Hospital) of the Commission on Pneumonia, and consultants in biostatistics, Dr. George F. Badger(Associate in Biostatistics, School of Hygiene and Public Health, The Johns Hopkins University) and epidemiology, and Dr. Alexander Langmuir (Deputy Commissioner, Westchester County Health Department, New York). An Army staff member assigned to assist was Captain Norman L. Cressy of the Fourth Corps Area Laboratory.
The initial field team of Drs. Dingle (laboratorian) and Wood (clinician) was elected by Dr. Colin MacLeod (Professor of Bacteriology, New York University, New York, New York), Director of the Com-
7
Front row, left to right: Captain Norman L. Cressy, Dr. G. John Buddingh, Dr. James M. Ruegsegger, Dr. Theodore Abernethy, Dr. John H. Dingle, Dr. W. Barry Wood, Jr., and Captain Rappoport (Base pathologist).
Back row, left to right: Dr. Edward Weiss, Dr. Alexander D. Langmuir, and Dr. George F. Badger.
8
mission on Pneumonia, at the request of Dr. Francis Blake (Professor of Medicine, Yale University, School of Medicine, New Haven, Connecticut), President of the Board; the team was supposed to include Dr. Langmuir, as recommended by Dr. Dingle. The members of the team were to be released on leave with pay by their respective institutions and paid as "Consultants to the Secretary of War" at the rate of $10.00 per day; however, Langmuir`s superior refused to recommend him for leave with pay. Dr. Blake then persuaded the National Academy of Sciences to fund Dr. Langmuir`s salary and travel, and he reported 2 months after Drs. Dingle and Wood to Camp Claiborne, where he and the others stayed for 3 months.
When CARD was activated on 1 August 1942, with Dr. Dingle as Director, all members of the Claiborne Commission, with the exception of Drs. Buddingh and Wood, including Captain Cressy, became members of this permanent group. They were joined within the year by Drs. Elias Strauss(Research Associate in Epidemiology, College of Physicians and Surgeons, Columbia University, New York), Charles H. Rammelkamp (Instructor of Medicine, Boston University School of Medicine), and Hugh Tatlock, a National Research Council Fellow.
The CARD, like the Board, was a creature of the Boston-to-Baltimore axis, with a few extensions to the middle west, reflecting the dominance of the eastern medical schools in the early 1940s. Drs. Dingle and Badger were graduate students at The Johns Hopkins School of Hygiene and Public Health at the same time. Dr. Dingle then went to Harvard Medical School, Boston, Massachusetts, and met Dr. Wood when the latter was a fellow in bacteriology. Ten years earlier, Dr. Ruegsegger had done work on the pneumococcus with Dr. Finland at the Thorndike Memorial Laboratory of the Boston City Hospital before joining the Department of Medicine at the University of Cincinnati. Dr. Dingle knew Drs. Rammelkamp and Strauss at the Boston City Hospital, Dr. Langmuir at both that hospital and at Johns Hopkins, and Dr. Feller at Harvard before Feller joined Dr. MacLeod`s department at New York University. Dr. Abernethy had entered practice in Washington, D.C., after a residency with Dr. William S. Tillett at Johns Hopkins (before Tillett moved to New York University) and after 3 years at the Rockefeller Institute, New York, New York, where he met Dr. A. R. Dochez, a member of the Board. The youngest member to join the group in November 1943 was Dr. Irving Gordon, who had done work on the influenza virus with Dr. Frank Horsfall at the Rockefeller Institute before spending 1942 at Trudeau Sanatorium with tuberculosis. After leaving Trudeau, Dr. Gordon worked in the laboratories of the New York State Health Department in Albany, where he met Dr. Langmuir, who was then Deputy Health Commissioner of Westchester County. All of these relationships were of great value, for these friends and acquaintances became an extremely effective, productive, and congenial group of investigators.
In the interval between Camp Claiborne and Fort Bragg, North Carolina, the initial CARD members worked on the report of the Camp Claiborne studies at Johns Hopkins, accommodated through the kindness of Dr. Lowell Reed, while awaiting construction of facilities at the station hospital at Fort Bragg. A W-1 ward building at Fort Bragg was remodeled to serve as a laboratory, and an animal house was constructed as an addition to the hospital morgue. The staff reported on 19 October and lived for about 6 weeks in a nurses` barracks, while seeking housing in nearby Fayetteville. The rooms in the barracks were retained in subsequent years as on-call sleeping quarters. As the work expanded, a ward adjacent to the CARD`s laboratory was made available, and a new nine-room air-conditioned animal house constructed.
Additional facilities were obtained to house volunteers during attempts to transmit primary atypical pneumonia and other respiratory illnesses to them. A preliminary study was conducted at a Civilian Public Service Camp in the Great Smoky National Park near Gatlinburg, Tennessee in buildings formerly used by the Civilian Conservation Corps. Subsequent experiments were conducted in the Holly Inn in nearby Pinehurst, North Carolina, a hotel with facilities adequate for the isolation of volunteers in individual rooms equipped with a private bath. Volunteers were recruited from a group of conscientious objectors identified with the assistance of Selective Service, the National Service Board for Religious Objectors, and the American Friends Service Committee.
When the establishment of a commission to be located on a military base was discussed at the fifth meeting of the Board, the Chief of Personnel Service, Colonel George F. Lull "was of the opinion that it
9
Kneeling, left to right: T / 4 R. L. Robinson, Private G. O. Whitaker, T / 4 L. P Godifer, Private First Class R. W. Mott.
Standing, second row, left to right: Captain H. L. Cressy, M.C., Dr. G. F. Badger, Dr. E. Strauss, Dr. J. M. Ruegsegger, B. A. Mulliken, M. Buckingham, E. E. Searles, Dr. J. H. Dingle, Dr. A. E. Feller.
Third row, left to right: Dr. A. D. Langmuir, A. Keogh, A. M. Galligan, M. E. Corcoran, L. W. Powell, Dr. C. H. Rammelkamp, Jr., Dr. T. J. Abernethy, 2nd Lieutenant A. Ignatow, M.A.C.
Fourth row, left to right: T. J. Oliver, W. A. Mickle, D. D. Graham, Sergeant H. E. Duke.
Back row, left to right: Private L. M. Ragland, Private First Class E. J. Noal, Private J. E. Stanfield, Private First Class C. E. Owens.
10
would be possible to hold together a group of commissioned medical officers for this purpose." It was noted that a "waiver of disability could be applied to any member of such a group for limited service." As it happened, the professional members and associates of the CARD remained primarily a civilian group for the first 18 months. About this time, Ruegsegger left to accept a commission in the Navy because, "I didn`t think I was contributing much to the war effort" looking for unknown agents. During his 3 years as a Naval Preventive Medicine Officer, he helped make the diagnosis of pneumococcal endocarditis in President Franklin Roosevelt and to obtain penicillin for the President`s treatment. By the spring of 1944,the majority of the physicians were commissioned in the Army of the United States. Despite a limp attributed to poliomyelitis in childhood, Dr. Dingle was commissioned Major, as were Drs. Abernethy, Badger, and Langmuir. Dr. Tatlock was made a Captain; Dr. Cressy advanced from Captain to Major, and Dr. Strauss, from 1st Lieutenant to Captain. Despite the prior waiver statement, Drs. Feller, Gordon, and Rammelkamp were not commissioned because of their medical histories. The group did manage to stay together, although Dr. Langmuir received orders for detached duty (never executed) shortly before all were decommissioned and returned to civilian status. Dr. Dingle received a terminal commission as Lieutenant Colonel.
Funds for the CARD budget were provided through a War Department contract with Yale University. The budget approved by the Board for the year beginning 1July 1943 was $4,000 short of the $100,000 requested by Dr. Dingle, as follows:
|
CARD Budget for Year Beginning 1 July 1943 |
|
|
Professional salaries |
$40,000 |
|
Secretarial and technical salaries |
15,000 |
|
Equipment, supplies, and travel |
41,000 |
|
|
$96,000 |
The major source of financial support was obtained from private foundations, presumably through the combined efforts of Commission Director Dingle and Board President Blake. Contributions to the Board on behalf of CARD were as follows:
|
Private Financial Support for CARD |
|
|
Rockefeller Foundation |
$25,000 |
|
W. K. Kellogg Foundation |
20,000 |
|
Commonwealth Fund |
15,000 |
|
John & Mary R. Markle Foundation |
10,000 |
|
|
$70,000 |
By November 1945, the budget for the Central Board and 10 commissions totaled$570,544, with the largest budget, $86,200, being that for the CARD. The available records do not make clear how the foundation funds were melded into the total or why the CARD budget appeared to decrease by $10,000 in 2 years. One possible explanation is that the fiscal year 1946 Board budget included an additional $14,330 for civil service employees at the CARD laboratory and $6,000for supplies. The field laboratory closed 8 months later, at which time the CARD budget consisted of all research contracts and CARD with its investigators and their institutions.
Such a contract was awarded to Western Reserve University in Cleveland, Ohio, on behalf of Dr. Dingle, to continue studies on acute respiratory diseases. Although the war was over, the military decided that it still needed the advice of the Army Epidemiological Board and the expertise of certain of its commissions. Dr. Dingle, who continued as CARD Director until 1955, and his colleagues at Fort Bragg, conceived the idea of applying the epidemiological and laboratory methods used to study recruits to the study of a civilian population. Dr. Dingle and three other members of the CARD, Drs. Badger, Feller, and Rammelkamp, were persuaded by Dr. Joseph T. Wearn, then Dean of the School of Medicine at Western Reserve, to come to Cleveland to undertake such studies using as a base a new Department of Preven-
11
Staff of The Commission Acute Respiratory Diseases (CARD) Laboratory, November, 1944.
Kneeling, left to right: Dr. C. H. Rammelkamp, Jr., Dr. A. E. Feller, Dr. 1. Gordan, Private W. Park, Private E. Oliver, T/5 D. Foltz, Staff Sergeant E. Gold, Sergeant C. Hoover.
Standing, second row, left to right: J. P Neeley, D. C. Mickle, M. J. Croker, R. Chase, I. A. Salamandra, Private A. Adler, Private F. Sullivan, Corporal M. H. Kaplan, Sergeant H. E. Duke, Corporal W. W. Skatrud, Private First Class V Culver.
Third row, left to right: B. Smith, S. Harlam, S. Taylor, R. M. Kierman,1. Weissinger, Technical Sergeant L. P Codifer, Corporal G. J. Leuty.
Fourth row, left to right: Major J. H. Dingle, MC, C. Kaldus, 2nd Lieutenant W. A. Mickle, SnC, B. A. Mulliken,1st Lieutenant H. M. Lemon, MC, M. Pate, Frank David, H. H. Bobbitt.
Fifth row, left to right: 1st Lieutenant T. J. Oliver, SnC, Major T. J. Abernethy, MC, Captain Straus, MC, 1st Lieutenant H. Tatlock, MC, 1st Lieutenant R. L. Robinson, SnC, Captain C. G. Loosli, MC, 1st Lieutnant A. Ignatow, MAC.
Back row, left to right: Captain A. D. Langmuir, MC, Captain G. F. Badger, MC, Major N. Plummer, MC, Major N. L. Cressy, MC.
Sergeant E. Gold (front row, second from right), a technician, later followed CARD members to the School of Medicine at Western Reserve University as a medical student and became Professor and Chairman of the Department of Pediatrics at the University of California, Davis.
12
Front row, left to right: Major T. J. Abernethy, MC, Major J. H. Dingle, MC, Captain A. D. Langmuir, MC.
Second row, left to right: 1st Lieutenant H. Tatlock, MC, Dr. A. E. Feller, Captain C. G. Loosli, MC (Commission on Air-Borne Infections), Dr. I. Gordon.
Third row, left to right: Major N. Plummer, MC (Commission on Influenza), Captain E. Strauss, MC, Captain G. F. Badger, MC.
Back row, left to right: 1st Lieutenant H. M. Lemon, MC (Commission on Air-Borne Infections), Major N. L. Cressy, MC, Dr. C. H. Rammelkamp, Jr.
13
tive Medicine, of which Dr. Dingle was to be Chairman. They were joined at the outset by Dr. Richard G. Hodges, a pediatrician, who had conducted the studies of pneumococcal vaccine at the Army Air Base Technical School in Sioux Falls, South Dakota, with Dr. MacLeod of the Commission on Pneumonia. This nuclear group was joined later by William S. Jordan, Jr., who had known Dr. Dingle at the Boston City Hospital, Harold S. Ginsberg, also trained at Boston City and formerly Chief of the Medical Service at the Station Hospital at Fort Bragg; Floyd W. Denny, Jr., once assigned as a young medical officer to the Department for training before a tour of duty at the Streptococcal Diseases Laboratory at Warren Air Force Base, Cheyenne, Wyoming; Harold B. Houser, who served as Field Director of the Laboratory on Housing and Illness, Robert Oseasohn, and others. When Dr. Dingle became President of the Board, Drs. Feller, Jordan, and Denny, in turn, became Director of CARD.
Dr. Dingle served as Chairman of the Department of Preventive Medicine at Western Reserve until 1969. Despite a progressive disability, he maintained an interest in education and research until his death in 1973. Dr. Badger became Chairman of the Department of Biostatistics before retiring in 1972 to a community southeast of Cleveland, where he died on 30 November 1991 of a heart attack. Dr. Feller became Chairman of the Department of Microbiology at the University of Virginia School of Medicine, Charlottesville, Virginia, but unfortunately died at an early age of coronary heart disease in 1946 while vacationing at Nag`s Head, North Carolina. Dr. Hodges died in Cleveland of myocardial infarction at an even earlier age. Dr. Rammelkamp, as Professor of Medicine, became Director of the Department of Medicine at the Cleveland City Hospital and played a major role in transforming it into the Metropolitan General Hospital of Cuyahoga County. He died in 1981 of a ruptured abdominal aortic aneurysm. Dr. Denny served as Chairman of the Department of Pediatrics at the University of North Carolina for 17 years and continued as a professor there in 1992. Dr. Ginsberg served sequentially as Chairman of the Departments of Microbiology at the University of Pennsylvania and the College of Physicians and Surgeons of Columbia University, retiring in1993 to Bethesda, Maryland, where he continued studies of adenoviruses in the Laboratory of Infectious Diseases of the National Institutes of Health (NIH).Dr. Houser became Chairman of the Department of Epidemiology and Biostatistic sat Case Western Reserve, the eventual successor of Dr. Dingle`s Department of Preventive Medicine, retiring in 1992 to Sun Lakes, Arizona. Dr. Jordan became, in succession, Chairman of the Department of Preventive Medicine and Professor of Medicine at the University of Virginia, Dean of the College of Medicine at the University of Kentucky, Lexington, Kentucky, and Director of the Microbiology and Infectious Diseases Program at the National Institute of Allergy and Infectious Diseases (NIAID), NIH. Dr. Jordan retired in 1987, continuing as a member of the AFEB until 1992 and as a consultant to the National Vaccine Program Office in 1994. Dr. Oseasohn served sequentially as Chairman of the Department of Epidemiology and Community Medicine and Professor of Medicine at the University of New Mexico, Albuquerque, New Mexico; Professor of Epidemiology and Associate Dean, University of Texas School of Public Health, Houston; Chairman, Department of Epidemiology and Health, McGill University, Montreal, Quebec; Professor of Epidemiology; and Associate Dean, University of Texas School of Public Health, Master of Public Health Program at San Antonio. In 1992, his wife having died the previous year, he retired to a nursing home suffering from Alzheimer`s disease. He died on June 7,1994.
Worthy of note is Dr. Eli Gold. He was a Sergeant in the laboratory at Fort Bragg and followed the senior staff from there to Western Reserve to enroll as a medical student. After graduation, he was an intern and resident of the Children`s Medical Center in Boston, before returning to Cleveland as Dr. Frederick Robbins` Chief Resident in Pediatrics at the City Hospital. He advanced through the academic ranks to become Chairman of the Department of Pediatrics at the University of California, Davis, Medical Center at Sacramento. He retired in 1987 to Mercer Island, Washington, from where he recalled the occasion of Dr. Dingle`s marriage to Doris Brown in June of 1946, when the 6 x 6 truck used to transport the enlisted men got mired in the mud on the grounds of her parents` house. The new Mrs. Dingle, a native of Fayetteville, which was also Dr. Jordan`s hometown, had worked as a secretary for CARD at Fort Bragg, and followed her husband`s activities with the CARD and the AFEB for many years.
The other original CARD members` careers continued as follows. Dr. Abernethy returned to private practice in Washington, D.C., retiring after over 40 years to Baltimore, where he died on 4 January
14
DIRECTORS OF THE CARD
ALTO E. FELLER, M.D.
1955 to 1959
WILLIAM S. JORDAN, JR., M.D.
1959 to 1967
JOHN H. DINGLE, M.S., M.D.
1942 to 1955
President AFEB
1955 to 1958
FLOYD W. DENNY, JR., M.D.
1967 to 1972
GEORGE G. JACKSON, M.D.
Acting Director
September 1971 to September 1972
15
1992 after a stroke. Dr. Ruegsegger joined Lederle Laboratories. Dr. Strauss maintained an active practice in Texas until his death in 1988. Dr. Tatlock ended his Army career as Chief of Infectious Diseases at Walter Reed General Hospital and then spent 35 years in the practice of internal medicine in North hampton, Massachusetts, becoming Chief of Medicine at Cooley Dickinson Hospital before retiring in 1981 to devote himself full time to photography. Dr. Gordon returned to the New York State Department of Health in Albany to head its virology laboratory before moving to California as Chairman of the Department of Microbiology at the University of Southern California, where he continued to teach in 1993, even after retiring. Dr. Langmuir returned to Johns Hopkins as Associate Professor of Epidemiology before moving in 1949 to the Centers for Disease Control (CDC) in Atlanta, where he founded the Epidemic Intelligence Service and from which he retired in 1970 to teach at The Johns Hopkins School of Hygiene and Public Health until his death from kidney cancer on 22 November 1993 at age 83.
During the postwar life of CARD, the major investigators and their associates supported by the AFEB, in addition to Dr. Dingle at Western Reserve, included Drs. Harry F. Dowling and George G. Jackson at the University of Illinois, Chicago; J. Thomas Grayston, Hjordis M. Foy, and E. Russell Alexander, University of Washington, Seattle; Floyd W. Denny, Wallace A. Clyde, and Gerald W. Fernald, University of North Carolina at Chapel Hill; Carl G. Harford, Washington University, St. Louis; Harry A. Feldman, State University of New York(SUNY)-Syracuse; Lewis Thomas, New York University; Charles E. Smith, initially at the School of Medicine of Stanford University in San Francisco, then later at the University of California at Berkeley with Demosthenes Pappagianis; Alto E. Feller, William S. Jordan, Jack M. Gwaltney, and Owen Hendley, University of Virginia, Charlottesville; Harold S. Ginsberg, University of Pennsylvania, Philadelphia. An important group of investigators supported by another source of federal funds was housed at the NIH Laboratory of Infectious Diseases under the leadership of Dr. Robert M. Chanock, an associate member of the CARD.
Among the members of this group not previously mentioned, Dr. Dowling retired to Northern Virginia to author a book, City Hospitals, to add to his earlier ones, The Acute Bacterial Diseases and Medicines for Man. Dr. Jackson served with distinction as Editor of the Journal of Infectious Diseases , moved to England to become Director of Virology at the London Hospital Medical Center, and then retired to his home state of Utah. Dr. Grayston became, in succession, Chairman of the Department of Preventive Medicine, School of Medicine; Dean of the School of Public Health; Vice President for Health Science, all at the University of Washington Medical Center before returning to research in 1984 as Professor of Epidemiology. Dr. Harford remained active at Washington University after his official retirement, but 1992 found him in a nursing home suffering from Alzheimer`s disease. Dr. Foy continued at the University of Washington; Dr. Alexander moved to the University of Arizona and then to the CDC, before returning to Washington; both were still active in 1993. Dr. Feldman served for many years as Chairman of the Department of Preventive Medicine at SUNY Syracuse and as President of both the American Epidemiological Society and the Infectious Diseases Society of America, each of which established awards in his name after his death in 1985. Dr. Thomas authored delightful and insightful notes as an observer of biology and medicine (The Lives of a Cell, The Medusa and the Snail, The Youngest Science), while en route from medical school deanships at NYU and Yale to the Chancellorship of Memorial Sloan-Kettering Cancer Center, retiring to continue as Scholar-in-Residence at Cornell University Medical College. Thomas died of Waldenstrom`s disease on 3 November 1993, at age 80. Smith continued to work oncoccidioidomycosis while serving as Dean of the School of Public Health at Berkeley. After Dr. Smith`s death in 1967, Dr. Pappagian is moved these studies to the University of California at Davis when he became Chairman of the Department of Microbiology at its medical school.
Among noncontractor members who made significant contributions were Drs. Robert Austrian, Professor of Medicine, University of New York, Downstate Medical Center, who became Professor of Research Medicine at University of Pennsylvania, where he continued to study the pneumococcus in 1994; Theodore E. Eickhoff, who was at the CDC when recruited to serve on the Committee on Meningococcal Infections, and was to become Professor of Medicine at the University of Colorado School of Medicine and Chief of Medicine at Presbyterian/St. Luke`s Medical Center in Denver, continuing there in 1994; and Jay P. Sanford, initially at the University of Texas Southwestern Medical School, who
16
served as Dean and Vice President of the Uniformed Services University of the Health Sciences before returning to Texas. Worthy of special mention is another non contractor and loyal associate member, Dr. Finland, who consistently refused to become a member because he didn`t want to participate in contract reviews. Dr. Finland trained many CARD investigators on the wards of the Harvard Medical Service or in the laboratories of the Thorndike Memorial Laboratory at the Boston City Hospital during his 50 years at that institution. He died in 1987 at the age of 85.
An outstanding feature of the structure and function of the AFEB and its commissions was the interchange that occurred when these investigators met periodically, along with those from military laboratories, to review work in progress and to learn of current problems in the armed forces. Between meetings, commission members and associates could respond to calls for assistance more effectively than might otherwise have been the case because of their knowledge of each other and of three military services. The major annual CARD meeting was held in the spring, usually in tandem with the Commission on Streptococcal and Staphylococcal Diseases (CSSD), so that the two groups could share an overlapping agenda for a day. In the fall, CARD and the Commission on Influenza took advantage of the meeting of the Central Society for Clinical Research in Chicago to meet for 1 day before the Society meeting. Drs. Dowling and Jackson often arranged a dinner for the attendees at a convenient university facility. At the 1959 fall meeting, Dr. Thomas Francis labeled the challenge resulting from the explosive identification of new viruses as "viral smog," and the suggestion was made that CARD sponsor the preparation of a laboratory guide for the isolation and characterization of the new respiratory viruses. Dr. Jackson enlisted the help of Drs. Chanock, Karl Johnson, and Robert Muldoon to produce a loose-leaf Manual of New Viruses Causing Respiratory Illnesses in Man. The first 100 copies of this manual, prepared at a cost of $377.66, exclusive of the authors` time and effort, were distributed in June 1961. The publication was widely acclaimed, with requests for copies coming from the World Health Organization, and laboratories in many countries.
Concurrently, the use of cell cultures had resulted in the discovery of a host of enteric viruses "in search of disease" or "orphan viruses." Investigators who sought to relate these enteroviruses to clinical syndromes and to distinguish them from polio viruses needed appropriate antisera and antigens. Because this was also true of those working with respiratory viruses, the AFEB sought the support of the NIAID, which, like the National Foundation for Infantile Paralysis, also had recognized the need for standardized reference reagents. NIAID had created an adenovirus committee for this purpose. The committee was initially chaired by Dr. Jerome Syverton, Chairman of the Department of Microbiology, University of Minnesota, with Drs. Ginsberg and Jordan of CARD and Dr. Edwin Lennette of the Commission on Influenza among the members. Dr. Syverton died of a heart attack in a New York taxi on his way to another meeting, after an early meeting of the adenovirus committee. He was succeeded as chairman by Dr. Jordan.
At a meeting at NIAID on 16 February 1960, representatives of the Public Health Service (PHS) and AFEB agreed to seek mechanisms to expand the scope of the adenovirus committee. Those in attendance were Drs. Dorland Davis, Scientific Director (subsequently Director), Paul Peterson, Associate Director, and Robert Huebner, Chief, Laboratory of Infectious Diseases, all of NIAID; Dr. Francis, President, AFEB; Dr. Fred Davenport, Commission on Influenza; Dr. William Hammon, Commission on Virus Diseases; Dr. Ralph Hogan, Chief, Laboratory of Virology, CDC; Dr. Harvey Scudder, Division of Research Grants, NIH; and Dr. E. H. Arnold, affiliation not recorded. Out of this meeting grew the Reference Reagents Program of NIAID that was to provide high quality antigens and antisera to investigators for many years before its repository and distribution functions were transferred to the American Type Culture Collection in the 1980s. The contributions made by CARD investigators and others to the dispersal of the etiologic smog are summarized in the research section.
Air-Borne Infections
The Commission on Air-borne Infections (CABI) began life in June 1941 as the Commission on Cross Infections in Hospitals. The investigations required by The Surgeon General, at that time, were to "carry on work pertaining to the prevention of cross-infections in Army Hospitals. Cross-infections
17
As a Professor of Medicine at Harvard Medical School and Chief of Infectious Diseases at the Thorndike Memorial Laboratory at Boston City Hospital, Dr. Maxwell Finland, long a student of pneumonia, conducted pioneering studies of the sulfonamides and penicillin. He trained many members of CARD and served it faithfully as a Associate Member for over 12 years.
18
have been an important problem for many years and it is now believed that their control can be brought about through the installation of air filters on sterilizing lamps. These studies will involve the purchase of extensive equipment and very close observation by highly-trained specialists and technicians over extended periods of time."
Dr. Oswald H. Robertson, Professor of Medicine at the University of Chicago and already a member of the Commission on Influenza, was named Director. He had just published the results of studies of the effectiveness of propylene glycol vapor as an aerosol against a number of organisms, including influenza A virus. Three other members also represented liaison with other Commissions: Drs. C. Philip Miller, also a Professor of Medicine at the University of Chicago (Meningococcal Meningitis); Wilson G. Smillie, another former research fellow at the Rockefeller Institute, Chairman of the Department of Public Health, Cornell Medical College (Influenza); and Joseph Stokes, Jr., Professor of Pediatrics, University of Pennsylvania (Measles and Mumps). Two other physician members were Drs. Clayton G. Loosli, who had done research with Dr. Robertson and had advanced to Assistant Professor of Medicine at the University of Chicago, and Dr. Francis F. Schwentker, Staff Member, International Health Division, Rockefeller Foundation (Director, Commission on Hemolytic Streptococcal Infections). Undoubtedly at the suggestion of Dr. Stokes, Mr. William F. Wells, Associate Professor in Air-Borne Infection, an expert from the University of Pennsylvania, completed the roster. This group, with the exception of Dr. Schwentker who was added later, met in Chicago the following October to plan how to exploit air sterilization methods to reduce the number of pathogenic bacteria and viruses in operating rooms, hospital wards, and barracks. A field study was initiated at the Station Hospital at Chanute Field, Illinois, and research with animals begun in laboratories at the University of Chicago and the University of Pennsylvania. During the following year, the CABI program was designed to include the following:
(1) Study of the effects of ultraviolet light, under varied conditions of radiation, for its bactericidalaction on air-borne microorganisms and for the prevention of spread of bacteria from patient to patient.
(2) Investigation of the pharmacological effects of propylene glycol vapor on animals and the ability of this vapor to destroy pathogenic microorganisms and viruses.
(3) When satisfactory evidence is obtained showing that propylene glycol vapor is not toxic, study of the activity of the vapor in the same manner in which ultraviolet light is being investigated.
(4) Study of the comparative effectiveness of both ultraviolet radiation and propylene glycol vapor on dust-borne bacteria.
(5) Investigation of the bactericidal and viricidal properties of other glycols.
(6) When deemed appropriate, the application of these measures for the control of air-borne infection to relatively isolated and fairly large non-hospitalized groups.
The first budget found in the records is for $53,705.00 in fiscal year 1946, by which time two other members had been added to the commission: Morton Hamburger, Jr., M.D., and Theodore T. Puck, Ph.D., both members of the Department of Medicine, University of Chicago. Hamburger, who had worked in Robertson`s laboratory in 1938, was named Field Director. In addition, Captain Henry M. Lemon participated in CABI studies as they were transferred to Camp Carson, Colorado, and later to Fort Lewis, Washington. After development of an apparatus for dispensing glycol vapor, its use was tested at the Harriet Lane Home, The Johns Hopkins Hospital, and laundry methods were sought for the application of an oil emulsion to bedding.
Increasing attention was being paid to the physical aspects of housing prompted by the decision of the Commanding General, Services of Supply, in October 1942, to reduce the space allowance for troop housing to 40square feet per man. At the request of The Surgeon General, 10 members of the AFEB and its commissions visited 19 Army posts and camps during December to consider the current and expected incidence of acute respiratory disease in troops. The survey called particular attention to inadequate provisions for proper ventilation and recommended that steps be taken to ensure that ventilation of 1,800 cubic feet per man hour be provided in barracks at night. Members of the AFEB were critical, of the overcrowding that existed but did not consider double bunking undesirable because it created more floor space and airspace and less actual contact of men while sleeping.
19
Dr. Oswald H. Robertson served as Professor of Medicine, University of Chicago, and Director of the Commission on Air-Borne Infections from 1942 to 1946. He was one of the first to study the effectiveness of propylene glycol vapor as an aerosol against influenza virus.
20
Dr. Kenneth F. Maxcy, in his report on Fort George G. Meade, Maryland, noted that
Attention is particularly directed to defects in design and operation of the heating systems installed in standard two-story barracks (Plans 700-1165 and 800-443). From the point of view of comfort and spread of infection improvement could and should be made. This is a very practical and important problem which might receive more extended attention from Dr. O. H. Robertson and his Commission on Cross Infections in Hospitals.
At a special meeting on 29 January 1943, the AFEB transmitted the following resolution to the Surgeon General:
In view of the increasing incidence of acute respiratory diseases and meningococcal meningitis during December 1942 and January 1943 and based upon an inspection of camps by members of the Board and its Commissions, the Board desires to go on record as emphasizing the influence of crowding in barracks, mess halls, and recreation halls on the spread of meningitis, acute respiratory and other epidemic diseases. Crowding is only one factor in this situation but a highly important one. In general terms it can be positively stated that the greater the crowding the greater is the risk of an epidemic of serious proportions. The order reducing the minimum floor space per man in barracks from sixty (60) square feet to forty (40) square feet, while a military necessity, is in an undesirable direction from the standpoint of maintenance of health. The effect of this provision not only results in overcrowding in barracks but also an equally undesirable overcrowding in mess halls, wash rooms, latrines, post exchanges, etc., and overloads all existing facilities. The Board especially emphasizes the greater susceptibility of recruits to acute respiratory and other epidemic diseases and the greater risks of epidemics during the winter months (December through March), particularly under conditions of crowding.
In May 1943, the name of the Commission was changed from Cross Infections in Hospitals to Air-Borne Infections in keeping with the emphasis on housing and the search for methods to limit the spread of respiratory pathogens in barracks. The CABI and CARD addressed these problems for the next 3 years, in collaboration with the Commission on Hemolytic Streptococcal Infections. A report in 1945 noted that significantly lower rates were observed during an epidemic of acute respiratory disease among men living in barracks with double bunks than in control barracks. At the same meeting of the AFEB on 15 April 1946, at which the CABI was terminated, the AFEB reaffirmed its position of being opposed to the use of double bunking unless over crowding is avoided.
It is recommended that double bunking is justified in barracks, but should not be used to accommodate more than one man per sixty square feet of floorspace (i.e., per one hundred and twenty square feet of floor space for each double bunk).
The notes of this meeting called for the Commission on Environmental Hygiene to continue the studies of the CABI. In truth, that Commission focused on occupational health and toxicology, studying the adaptation of a human to his environment, the medical aspects of clothing, cold, heat, ventilation, and the disposal of waste. Yet, a need existed for additional studies of the effect of housing on the occurrence of disease, both infectious and neuropsychiatric. An ad hoc committee of CARD on space allocation in troop housing recommended that a Laboratory on Housing and Illness be established at Sampson Air Force Base, New York.
At the time of organization of this Laboratory in January 1954, Sampson Air Force Base had been a recruit training center for about 3 years. The Air Force had established the Epidemiological Detachment, 1141st Medical Service Squadron of the 1070th Medical Activity Group at Sampson in 1951 to study streptococcal infections and methods of prophylaxis. In addition, the Epidemiological Detachment was cooperating with the Commission on Influenza in influenza vaccine trials. The stated ap-
21
proach of the new laboratory was fundamental study of the problem of military housing on a long-term basis, rather than simple determination of the ideal number of square or cubic feet per man. The work of the Epidemiological Detachment was to be coordinated with and under the direction of the director of the housing studies. Initial support of the Laboratory was by contract with the School of Aviation Medicine. Drs. Feldman (SUNY-Syracuse) and Houser (on assignment from Western Reserve University) were the responsible investigators, with Dr. Houser designated as Field Director. Planning and conduct of the studies were under the aegis of CARD. From 1 August1955, the laboratory was supported through Department of Army contracts, with Hr. Houser as the responsible investigator.
Field, laboratory, and clinical studies were well underway by February 1954. The deficiencies of the original laboratory space for virological work and the increased volume of bacteriologic and other laboratory procedures necessitated remodeling of the laboratory; this remodeling was completed in September 1955. In December 1955, input of recruits to Sampson was markedly reduced and the decision to close the base was announced. In June 1956, the base officially closed. Dr. Houser transferred records and selected biological specimens to the Upstate Medical Center at Syracuse. There, a new laboratory was completed and in operation by late fall of 1956. Work continued at Syracuse on the collected material and specimens until June 1958 when the contract and certain materials were transferred to Western Reserve University, where work on the contract continued until 31 July 1960.
The subsequent careers of Drs. Feldman and Houser have been recorded earlier. Of the original CABI members, Dr. Robertson retired to California in 1949 to devote himself to the study of the endocrinology of salmon and trout; he died in 1966. Dr. Miller became Professor Emeritus in 1960; he died in 1985. Dr. Smillie continued as head of the Department of Pubic Health at Cornell until 1955, during which time he coauthored a textbook on preventive medicine with Dr. Edwin D. Kilbourne, then a member of his department and a long-time member of the Commission on Influenza. Dr. Smillie died in 1971. Dr. Stokes died in 1972 after a distinguished career in academic pediatrics. Dr. Loosli moved from Chicago to Los Angeles to become Dean of the School of Medicine of the University of Southern California; he died in 1976. Dr. Schwentker, the first Director of the CSSD, had been the first to report, along with coauthors Drs. Sidney Gelman and Perrin H. Long in 1937, that sulfanilamide was effective in the treatment of meningococcal meningitis. Suicide shortly after the commissions were formed ended Dr. Schwentker`s promising career.
Dr. Hamburger became Professor of Medicine at the University of Cincinnati and was a continuing contributor to the CSSD, until he drowned in1970 while fishing in the Snake River in Wyoming. Dr. Puck, who had received his doctorate only 1 year before joining CABI, remained at the University of Chicago until 1947, spent 1 year at the California Institute of Technology, Pasadena and then became Professor of Biophysics and Chairman of the Department at the School of Medicine of the University of Colorado, Boulder. A recipient of many awards for his work in genetics and immunology, he retired as department chairman in 1967, but continued as Director of the Eleanor Roosevelt Institute of Cancer Research. In 1972, he authored The Mammalian Cell as a Microorganism: Genetic and Biochemical Studies In Vitro. Although his contribution to the control of airborne infections is not evident, of interest is the fact that he listed his brief CABI membership in Who`s Who.
Meningococcal Meningitis
The Commission on Meningococcal Meningitis was the seventh of the eight commissions created by the Board in March 1941. The Surgeon General "determined" that:
The Meningitis Commission will study the incidence, treatment and prevention of cerebrospinal meningitis. In the control of meningitis, it is necessary to determine the type of germ causing the disease. For this purpose, typing laboratories Will be set up and a more efficient means of typing will be studied. Through work with small groups of individuals, an attempt will be made to develop effective administrative methods for the control of meningitis carriers. Such carriers are apparently normal individuals who harbor the germ in the nose or throat and who disseminate the infection through their secretions during contact, or in sneezing or coughing.
22
{kind=link}
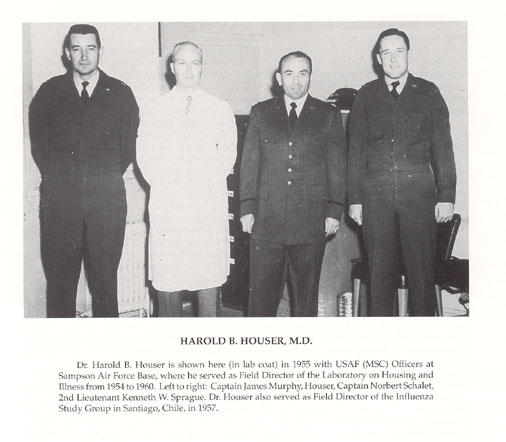
Dr. Harold B. Houser is shown here (in lab coat) in 1955 with USAF (MSC)Officers at Sampson Air Force Base, where he served as Field Director of the Laboratory on Housing and Illness from 1954 to 1960. Left to right: Captain James Murphy, Houser, Captain Norbert Schalet, 2nd Lieutenant Kenneth W. Sprague. Dr. Houser also served as Field Director of the Influenza Study Group in Santiago, Chile, in 1957.
23
Dr. Long, who, like many others, had trained for 2 years at the Rockefeller Institute before becoming Professor of Preventive Medicine of the School of Medicine, The Johns Hopkins University, was named Director. An organizational meeting held in Washington on 19 March brought together Dr. Mary C. Kirkbride, Associate Director, Division of Laboratories and Research, New York State Department of Health; Dr. Miller, Professor of Medicine, School of Medicine, University of Chicago; Lieutenant Colonel Arthur P Hitchens, U.S. Army, retired, Professor of Public Health and Preventive Medicine, School of Medicine, University of Pennsylvania; and Dr. John J. Phair, Associate in Epidemiology, School of Hygiene and Public Health, The Johns Hopkins University. Drs. Long and Miller were charged with reviewing the therapy of the disease, Lieutenant Colonel Hitchens and Dr. Phair were to act as epidemiological consultants, and Drs. Miller and Kirkbride were to set standards for bacteriologic and immunologic studies.
A tentative program for study and control of meningococcal meningitis was formulated and submitted to the AFEB on 26 April. A recommendation was made that a central laboratory be established at The Johns Hopkins School of Hygiene and Public Health to act as a focal center for interim laboratory studies, preparation and distribution of meningococcal typing sera, and analysis of case data for correlation with strain characteristics. An investigative team was planned to carry on the necessary field studies and to evaluate therapeutic and prophylactic measures. In addition, the importance of a specialized consultation service for the Office of The Surgeon General, Commanding Officers of Army posts, and medical laboratories was recognized and provided.
The organization and these plans were approved at the third meeting of the AFEB held on 19 June. After this action, the laboratory and personnel of the Department of Epidemiology of the School of Hygiene and Public Health, The Johns Hopkins University, under the direction of Dr. Phair, were made available through the courtesy of Dr. Maxcy, Professor of Epidemiology. Additional personnel and funds were provided by Dr. Long`s Department of Preventive Medicine. The work of the central laboratory was begun late in May 1941 under the supervision of Dr. Phair.
A contract between the Army and The Johns Hopkins University, effective 22November 1941, and totaling $25,000 in 1942,provided support for the Central Laboratory. In addition to the work of the central laboratory, two other studies were financed from November 1941 through June 1943 by contracts, one at the University of Chicago, under the direction of Dr. Miller, the other at Columbia University, under the supervision of Dr. Elvin A. Kabat.
Anticipating an increasing demand for consultation, the personnel of the CARD were augmented in August 1942 by the addition of Drs. Robert W. Graves, Assistant Professor of Neurology, Duke University School of Medicine; Lowell Rantz, Assistant Professor of Medicine, Stanford University School of Medicine; Smith, Professor of Public Health and Preventive Medicine, Stanford University School of Medicine, also a member of the Commission on Epidemiological Survey (CES); and Wood, Professor of Medicine, Washington University School of Medicine, also a member of the Commission on Pneumonia. On 31 August 1942, Dr. Long resigned to accept a commission in the Medical Corps of the Army, and Dr. Phair was chosen to replace him as Director.
In February 1943, Dr. Emanuel B. Schoenbach, who had been a member of the CES, received a commission in the Medical Corps and was assigned to The Johns Hopkins University. He was appointed to the Commission on Meningococcal Meningitis and took charge of the field investigations. He served as Acting Director during the two brief absences of Dr. Phair between 1 August and 1 November 1943 and between 15 August and 15 November 1945.
After not quite 3 years of existence, the Commission on Meningococcal Meningitis was terminated at the meeting of the Board in April 1946. Although the minutes of this meeting refer to the assignment of responsibility for streptococcal infections and pneumonia to CARD, no such assignment was recorded for meningococcal infections. Such infections were to be a continuing problem in the postwar years because an increasing proportion of meningococcal strains became resistant to sulfadiazine, rifampin was yet to be introduced for chemoprophylaxis, and an effective vaccine was still under development.
The personnel of the wartime CARD continued to make major contributions to infectious diseases and to other commissions. Dr. Long became Professor of Preventive Medicine and Chairman of the
24
{kind=link}
Dr. Perrin H. Long served as Professor of Preventive Medicine, School of Medicine, The Johns Hopkins University. He was the first Director of the Commission on Meningococcal Meningitis, serving from March 1941 to August 1942 before joining the Army Medical Corps as a Colonel for service as a medical consultant to the Chief Surgeon of the Mediterranean Theater. He made major contributions to the early study of sulfonamides, the first effective antibacterial agents.
25
{kind=link}
Dr. John J. Phair served as Associate in Epidemiology, School of Hygiene and Public Health, The Johns Hopkins University. He was a charter member of the Commission on Meningitis, succeeded Dr. Perrin Long as its Director in August 1942, and served in this capacity until April 1946. He contributed to developing new knowledge of meningococcal, streptococcal, and respiratory tract diseases.
26
Department at SUNY Downstate, before retiring in 1961. He died in 1965. Dr. Phair left Johns Hopkins in 1946 to join the faculty of the School Medicine of the University of Louisville before becoming chairman of the advisory committee to the Commissioner of Health of the City of Cincinnati and then Commissioner. He died in 1970. Dr. Schoenbach became Professor of Medicine at College of Medicine, SUNY-New York City and Director of Medical Services at Maimonides Hospital. He died of coronary thrombosis in 1952. Dr. Smith became a member of CARD while also serving as a member of the AFEB. The date of his death and that of Dr. Miller are recorded in earlier sections. After a distinguished career as chairman of the Department of Medicine at Washington University in St. Louis, Dr. Wood returned to Johns Hopkins as Vice President for Medical Affairs, a position he held for 3 years before returning to research as Professor of Microbiology; he died of myocardial infarction in 1971. Dr. Rantz continued his studies of hemolytic streptococci, but he too died of a heart attack at age 53 in 1965.
When CARD assumed responsibility for meningococcal meningitis, Dr. Feldman, Professor of Preventive Medicine, SUNY, Upstate Medical Center-Syracuse, was asked to head its Committee on Meningococcal Infections. He was well-qualified to do so. He (with Drs. Dowling and Sweet) was among the first to confirm, in1942, the effectiveness of sulfadiazine in the treatment of meningococcal meningitis, reported the previous year by Drs. Dingle and Thomas (with Morton).When he entered military service in October 1942, Dr. Feldman was assigned to the Fourth Service Command Laboratory located at Fort McPherson, Georgia, a reference center that served more than 100 Army hospital laboratories. Meningococcal infections were prevalent from Florida to North Carolina, from the Atlantic to the Mississippi. Feldman developed methods for the identification of strains, for testing their sensitivity to sulfadiazine and participated in carrier surveys and field trials to evaluate sulfadiazine as a prophylactic agent. After the war, his laboratory at SUNY-Syracuse became a national and international reference center for meningococci, tracking the increasing resistance of strains to sulfadiazine and the eventual ineffectiveness of that drug for treatment or prophylaxis. Other members of the committee included, at various times, Drs. Denny, Dingle, Eickhoff, Finland, and Jordan of CARD, Malcolm S. Artenstein, WRAIR, Captain James Kingston, USN, John Y. Bennett, CDC, and Richard Roberts, Commission on Streptococcal Infections.
Although penicillin became available for treatment, the inability to eliminate the carrier state heightened the consternation and frustration that accompanied any outbreak of meningitis. At such times, largely for reassurance and public relations, members of the Committee on Meningococcal Infections were asked to visit bases experiencing epidemics. One such visit was made to Fort Ord, California, in September 1964 by Drs. Feldman, Austrian, Eickhoff, Finland, and Jordan with Dr. Gold representing Dingle, along with Drs. Ross L. Gauld, WRAIR, and Arthur W. Frisch, University of Oregon.
The incidence of meningococcal meningitis in California had shown a gradual increase since 1959, the case rate rising from 1.4 per 100,000 in 1959 to 3.0 in 1964. The build-up of cases at Fort Ord was as follows: 2 in 1960, 6 in 1961, 38 in 1962, 64 in 1963, and 108 in 1964. The first fatalities occurred in 1963, and it was in this year that Dr. Feldman was called to visit San Diego Naval Training Station to consult about the occurrence of meningitis. The call came while he was attending a meeting of the American Epidemiological Society in Washington. With the encouragement of Dr. Jordan, CARD Director, and the assistance of the AFEB Office, Dr. Feldman promptly headed west with little more than his toothbrush. He had a little more time to prepare for the visit to Fort Ord the next year.
As expected, most cases of meningitis at Fort Ord occurred in basic trainees in the first 8 weeks of training. No meningitis was noted in cadre men who were instructors and had daily contact with trainees or in physicians and nurses. A survey of Monterey County in which Fort Ord is located revealed only one case of meningococcal meningitis in the civilian population in January through September, 1964. This was the only case in that county in 1964,whereas 89 cases occurred in military personnel and 10 among civilian dependents. The carrier rate in new inductees was the same (20%) as in University of California students and was believed to reflect the current carrier rate in the male civilian population of California in ages 17 to 24. All of the strains of Neisseria meningitides were either serotype group B or C, with 90% being group B.
27
The occurrence of cases on the base had attracted growing media attention, with frequent bulletins on television and scare headlines in the press. After the Committee had assessed the situation and confirmed that meningococci were widely disseminated throughout the civilian population, Dr. Feldman appeared on television to point out that the safest place for a civilian in California to reside was in the vicinity of Fort Ord and that it was doubtful that military personnel posed any greater hazard to the civilian population than the hazard encountered by civilians in their daily exposure to civilian carriers. The public, press, and politicians were not convinced, and an episode the following month forced the closure of the base.
A basic trainee spent a day on leave with his fiancee. After his return to the base, she developed fulminant meningococcal meningitis caused by a group B organism and died. He remained well; a culture of his throat yielded a group B meningococcus. Not until after the assumed connection between the soldier and his girl had increased public anxiety further was it shown that the meningococci were probably different strains. The military was forced to suspend the intake of new basic combat trainees and Army Reserve personnel in support of a governor pressured and harassed by a frightened electorate.
In December 1964, the Board adopted the following recommendation:
That, in view of the epidemiological behavior of meningococcal infections with cyclic recurrences of epidemics at approximately 10-year intervals, thought and planning be given now for studies to be carried out, especially at military posts, approximately 8 to 10 years from now.
Fortunately, group C meningococcal vaccine became available before this time(1972), just before CARD and its Committee on Meningococcal Infections were terminated.
Pneumonia
The Commission on Pneumonia was listed third among the first seven commissions formed by the Board at its first meeting on 6 February 1941. Its first meeting took place in May 1941, a month before the memorandum that stated the investigations required by The Surgeon General of the then eight commissions listed it fifth, with the shortest of charges:
The Commission on Pneumonia will study the causes, prevalence, treatment and control of pneumonia. It will study epidemics in certain localities and will carry on work concerning the types of pneumonia caused by all the various kinds of germs and also the nonbacterial pneumonias.
The fact that the Commission on Cross Infections now had been added as the eighth commission was a result of the program of interim and field investigations drafted by the Commission on Pneumonia in May and submitted to the Board in June. The program, as outlined then, was divided into the following sections: prophylaxis by nonspecific measures, therapy of pneumonia and its complications, and recommendations for field investigations. It was realized at the outset that the personnel and facilities available to the Commission could not possibly include all these activities. A recommendation was made that the question of air sterilization by ultraviolet irradiation and germicidal aerosols should become the province of a special commission to be composed of one member from each of the commissions already set up, because the sterilization of air was a problem common to all. As previously noted, the AFEB agreed.
The members in attendance at the organizational meeting were the Director, Dr. MacLeod (Professor of Bacteriology, New York University College of Medicine; Dr. Abernethy, Associate Professor of Medicine, George Washington University School of Medicine; Michael Heidelberger, Ph.D., Associate Professor of Biochemistry, College of Physician and Surgeons, Columbia University; Dr. Edward S.
28
{kind=link}
Dr. Harry A. Feldman served as Professor of Preventive Medicine, State University of New York at Syracuse. He served the CARD in many ways, especially as Chairman of the Committee on Meningococcal Infections, and by providing a university base for the Laboratory on Housing and Illness when Sampson Air Force Base was closed. Highly respected for his extensive knowledge of infectious diseases, he was much admired for his willingness to assist in the investigations of outbreaks at military bases. One of the first to demonstrate that some meningococcal strains had become resistant to sulfadiazine, he used his laboratory to test isolates sent to him from throughout the world.
29
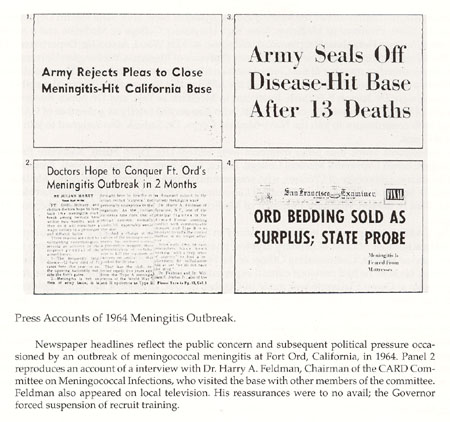
Press Accounts of 1964 Meningitis Outbreak.
{kind=link}
Newspaper headlines reflect the public concern and subsequent political pressure occasioned by an outbreak of meningococcal meningitis at Fort Ord, California, in 1964. Panel 2 reproduces an account of a interview with Dr. Harry A. Feldman, Chairman of the CARD Committee on Meningococcal Infections ,who visited the base with other members of the committee. Feldman also appeared on local television. His reassurances were to no avail; the Governor forced suspension of recruit training.
30
Rogers, Assistant Commissioner for Medical Administration, New York State Health Department; Dr. William S. Tillett, Professor of Medicine, New York University College of Medicine and a member of the Commission on Hemolytic Streptococcal Infections; and Dr. Wood, Associate, Department of Medicine, The Johns Hopkins Medical School and, later, Professor of Medicine, Washington University School of Medicine, already a member of the Commission on Meningococcal Meningitis. The records note that Drs. Dochez and Oswald T. Avery represented the AFEB at this first meeting. Original members not in attendance were Dr. Joseph F. Sadusk, Instructor in Medicine at Yale, and Dr. James Ruegsegger, Department of Medicine, University of Cincinnati, who also served briefly as a member of CARD before leaving both commissions to join the Navy Medical Corps. Dr. Sadusk also resigned to join the Army Medical Corps.
In subsequent years, four other members were added: Drs. Jacob Furth, Associate Professor of Pathology, Cornell University Medical College, Ithaca, New York; Clayton G. Loosli, Assistant Professor of Medicine, University of Chicago, who was commissioned a Captain in the Army Medical Corps; Wheelan D. Sutliff, Acting Director, Bureau of Laboratories, New York City Department of Health; and, in 1941, Paul B. Beeson, Assistant Professor of Medicine, Emory University Medical School, Atlanta, Georgia.
The CARD participated in its first field study in October 1941. Beginning in the summer of that year, a large number of cases of primary atypical pneumonia had been occurring at Camp Claiborne. Colonel Lucius Wright, Commanding Officer of the Station Hospital, was aware early of the nature of the disease, because he had previous clinical experience in Hawaii with a similar disease. A survey of the epidemic at Camp Claiborne was made in October by Drs. Dochez of the Army Epidemiological Board, Yale Kneeland, Jr. of the Influenza Commission, and MacLeod of the CARD. After this survey, a recommendation was made that a special commission be sent to Camp Claiborne to investigate the clinical and laboratory aspects of this disease. As detailed in the section on CARD, the commission for the study of atypical pneumonia at Camp Claiborne was under the directorship of Dr. Dingle of the Influenza Commission, assisted by Drs. Abernethy, Ruegsegger, and Wood of the Pneumonia Commission and others. Studies of a comprehensive nature were carried out through the winter and spring of 1942, when the group of investigators became the nucleus of CARD. Drs. Abernethy and Ruegsegger remained with the field staff of that CARD.
Dr. MacLeod`s final report for the Commission on Pneumonia noted
that prior to the original survey at Camp Claiborne, only a very small number of cases of atypical pneumonia were reported from Army installations in the United States. Based on the cases previously observed in civilian hospitals and the original survey at Camp Claiborne in October 1941, an official statement was prepared on the subject of primary atypical pneumonia by the Pneumonia Commission and issued by the Surgeon General`s Office early in 1942. Following this description and despite the cumbersome name of primary atypical pneumonia, etiology unknown, the number of reported cases of the disease took a remarkable upswing, and throughout the whole period of the war, the incidence of atypical pneumonia far exceeded pneumonia caused by all other agents combined. It was apparent that the vast majority of cases had gone unrecognized until this clinical description was circulated and opportunity afforded to use the term as a specific diagnosis.
The proposed budget of the Pneumonia Commission for 1943-1944 was $27,380.The actual budget recorded for 1945 was $27,100. This funded a $19,800 contract with New York University for Dr. MacLeod, and two subcontracts, one with Cornell University Medical College ($3,900) and one with Columbia University College of Physicians and Surgeons ($3,400). The latter was for the "Work of Dr. Michael Heidelberger on the polysaccharides of pneumococci, particularly in connection with preparation and use of these polysaccharides in immunization against pneumonia." This modest investment yielded a great dividend.
The major contribution of the Commission on Pneumonia during its 4.5 year life was the development of an effective vaccine for the prevention of pneumococcal pneumonia in young adults. At the outset, as Dr. MacLeod reported, "the Commission felt that it could fill an important need by athor-
31
{kind=link}
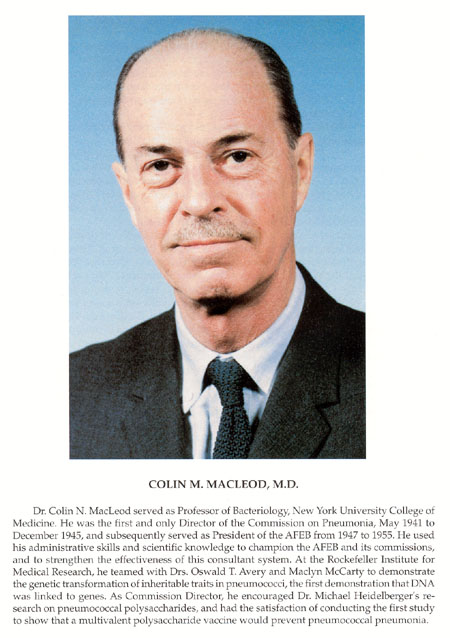
Dr. Colin N. MacLeod served as Professor of Bacteriology, New York University College of Medicine. He was the first and only Director of the Commission on Pneumonia, May 1941 to December 1945, and subsequently served as President of the AFEB from 1947 to 1955. He used his administrative skills and scientific knowledge to champion the AFEB and its commissions, and to strengthen the effectiveness of this consultant system. At the Rockefeller Institute for Medical Research, he teamed with Drs. Oswald T. Avery and Maclyn McCarty to demonstrate the genetic transformation of inheritable traits in pneumococci, the first demonstration that DNA was linked to genes. As Commission Director, he encouraged Dr. Michael Heidelberger`s research on pneumococcal polysaccharides, and had the satisfaction of conducting the first study to show that a multivalent polysaccharide vaccine would prevent pneumococcal pneumonia.
32
ough analysis of immunization with specific capsular polysaccharides of pneumococcus." A survey of previously recorded epidemics of pneumonia, both in the United States and abroad, showed that in all instances, types 1, 2, or 5 had been responsible. For this reason, it was proposed that attention be devoted specifically to these types and that the immunologic response of immunized subjects be assayed by quantitative methods. It was considered important to have on hand large amounts of the purified polysaccharides of these three types. Accordingly, in the event that immunization on a wide scale might be deemed necessary in case of an epidemic,100 g of each were obtained commercially, the preparation being controlled by Dr. Heidelberger.
The opportunity to test a multivalent pneumococcal vaccine containing polysaccharides for these three serotypes, and in addition, type 7, was found at the Army Air Base in Sioux Falls, South Dakota. Lieutenant Richard G. Hodges, MC, had been assigned to Sioux Falls as epidemiologist in the summer of 1943,and he remained there for the next 2 years. The detailed epidemiological analyses of respiratory infections that he made in collaboration with the Pneumonia Commission contributed greatly to knowledge of pneumococcal pneumonia and its relation to other respiratory diseases. These analyses and the results of the pioneering vaccine trial are summarized in the section on scientific contributions. The Commission on Pneumonia was terminated in December 1945.
After the war, Dr. MacLeod served the AFEB as a member and President from his academic base at New York University and later from other positions as follows: Professor of Research Medicine, University of Pennsylvania; Professor of Medicine, New York University; Deputy Director of the Office of Science and Technology of the White House; Vice President for Medical Affairs of the Commonwealth Fund; and President of the Oklahoma Medical Research Foundation. A strong supporter of international health research, he died suddenly in London in1972 while on his way to visit the Southeast Asian Treaty Organization Cholera Research Laboratory in Dhaka, Bangladesh. The subsequent histories of Drs. Abernethy, Hodges, Loosli, and Wood have been recorded in earlier sections.
Dr. Beeson became Professor of Medicine and Chairman of the department at Emory University Medical School, moving to the comparable position at Yale in1952. From 1965 to 1974, he served as Nuffield Professor of Clinical Medicine at Oxford University before returning to the United States as Professor of Medicine at the University of Washington. Dr. Tillett continued as Professor of Medicine at New York University and Director of the Third Medical Division at Bellevue Hospital until becoming Professor Emeritus in 1958. He died in 1974.
Dr. Furth rose to Professor of Pathology at Cornell in 1945, leaving in 1949to become Chief of the Pathology and Physiology Section of the Biology Division of the Atomic Energy Commission, Oak Ridge National Laboratory, Tennessee. He then held sequential appointments as Associate Director of Research, Children`s Cancer Research Foundation, Harvard Medical School; Director of Experimental Pathology, Roswell Park Memorial Institute, Buffalo, New York; and Professor of Pathology, Columbia University, becoming Professor Emeritus there in 1967.
Dr. Heidelberger advanced to Professor of Biochemistry at Columbia University`s College of Physicians and Surgeons in 1945 and to Professor of Immunochemistry there in 1948. Although he became Emeritus in 1956, he remained active in the field of polysaccharide immunochemistry, becoming the recipient of numerous awards and medals for his contributions before celebrating his 100thbirthday in 1988. Often referred to as the "father of modern immunology," he died of a stroke on 25 June 1991. Dr. Rogers became Professor of Public Health and Medical Administration, School of Public Health, University of California at Berkeley in 1946, also serving as Dean of the school until 1951. He became Professor Emeritus in 1971 and died shortly thereafter.
Dr. Sadusk served as Assistant, then Associate Clinical Professor of Medicine at Stanford University School of Medicine for 13 years; Professor of Preventive Medicine and Community Health, George Washington University School of Medicine 1962 to 1966, during which time he was Medical Director of the Food and Drug Administration; and Professor and Associate Dean for Community Medicine at The Johns Hopkins University, 1966 to 1967. He then served as Group Vice President for Medical and Scientific Affairs for Parke-Davis& Co. from 1967 to 1972 and Senior Vice President and Director of Medical and Scientific Affairs for Warner-Lambert Co. He died in 1978.
33
Dr. Sutliff left the New York City Health Department to become chief of the Infectious Diseases Section of the Veterans Administration Hospital in Memphis and Professor of Medicine at the College of Medicine of the University of Tennessee. He, became Professor Emeritus in 1971. He died in 1983.
SCIENTIFIC ACCOMPLISHMENTS
Respiratory Diseases
In 1942, the bacteriology laboratory was able to assist the clinician in the diagnosis of infections caused by meningococci, pneumococci, and streptococci. The virology laboratory could assist in the diagnosis of influenza, but that was all. Except for influenza, attempts to infect the chick embryo and other animals, including the mongoose, with secretions from persons with common colds or more severe nonbacterial respiratory diseases were unsuccessful. However, these nonbacterial, presumed viral, diseases were causing most of the hospital admissions and sick cell visits. Of necessity, clinical descriptions and epidemiological patterns were developed to separate cases into clinical syndromes that might indicate specific etiologies.
This was not easy. The first CARD annual report for 1942 and 1943 reflected the frustration experienced at Fort Bragg:
Data which have been collected indicate that, in the differential description of respiratory disease of supposedly different etiology, a summation of symptoms and signs present at any time during the illness is inadequate. By the time of recovery, most patients with a respiratory disease have presented such a variety of signs and symptoms that their mere enumeration does little to aid in classification.
Nevertheless, an attempt was made to separate cases into clinical syndromes that might indicate specific etiologies. Although no sharp clinical distinctions on the basis of symptoms, physical findings, laboratory results, or the clinical course of the diseases had been observed, it was possible to separate patients into three groups, namely, primary atypical pneumonia, exudative pharyngitis, and acute respiratory disease. However, the epidemiological studies in the first year failed to show any relationship between cases or to elucidate any factors of importance in the spread of these diseases.
For subsequent special studies, the investigators developed the following classifications.
1. Acute undifferentiated diseases (ARD): This category [also termed acute respiratory disease (ARD) of recruits] included acute illnesses, usually febrile, with respiratory symptoms or generalized constitutional symptoms, or both, ordinarily lasting fewer than 2 weeks. Patients having exudative tonsillitis or pharyngitis, specific contagious diseases, antibody responses to influenza viruses A or B or to streptolysin O, or pulmonary infiltration demonstrable radiographically were excluded from this classification.
2. Non streptococcal exudative tonsillitis or pharyngitis: This diagnostic category included patients with respiratory illnesses characterized by exudative lesions on the tonsils, palate, or oropharynx without either b-hemolytic streptococci or an increase in titer of antistreptolys in antibodies during convalescence.
3. Primary atypical pneumonia: This diagnosis indicated a respiratory illness accompanied by roentgenographic evidence of pulmonary infiltration but not by clinical and laboratory evidence of bacterial pneumonia, bronchiectasis, or other causes of pulmonary consolidation.
4. Hemolytic streptococcal infection: This diagnosis was made only when the illness was clinically compatible with such infections and, in addition, when b-hemolytic streptococci were isolated from the throat and a significant rise in antistreptolys in titer was demonstrable during convalescence.
34
5. Other illnesses: A small number of patients admitted with tentative diagnoses of respiratory disease proved to be suffering from other types of illness, such as immunization reactions, contagious exanthemas, meningococcal infection, or acute or chronic allergic disease. Such cases were excluded from further consideration.
The above is from a retrospective review of the CARD studies at Fort Bragg prepared 25 years later by Drs. Dingle and Langmuir. This was published first in the American Review of Respiratory Disease and then as a monograph with a foreword by Dr. MacLeod in which he stated "because of the meticulous epidemiologic studies, enough was learned about the behavior and natural history of these diseases so that when putative etiologic agents were isolated during the next dozen years one could move quickly and confidently to test their causative role."
There is no better background for consideration of these etiologic agents and what has since been learned about the diseases they cause than the "synoptic view" of the Commissions work prepared by Drs. Dingle and Langmuir:
Leads as to possible etiologic entities were sought from the clinical, epidemiologic, and laboratory observations, separately and collectively. Thus, the segregation of ARD as a possible entity was made primarily on the basis of the epidemiologic data supported, of course, by clinical and laboratory observations, whereas delineation of primary atypical pneumonia and non-streptococcal exudative tonsillitis and pharyngitis came principally from the clinical and laboratory data. Much effort was devoted to attempts to isolate agents from materials obtained from representative cases in these diagnostic categories, to induce illness or identifiable lesions in a variety of laboratory animals, and to obtain serologic indications of possible infectious agents. These attempts were unsuccessful because either nothing unusual was found or the results could be duplicated with what were thought to be appropriate control materials.
The decision was therefore made to attempt to transmit some of these types of respiratory disease to humans, and volunteers were enlisted for this purpose. The results may be summarized as follows: (1) Primary atypical pneumonia, together with minor illness without radiographic evidence of pulmonary infiltration could be transmitted to volunteers using filtered bacteria-free secretions of the respiratory tract of patients having the naturally occurring disease and could be transmitted in second passage. (2) ARD could be similarly transmitted, and the volunteers were immune to a second challenge with the same inoculum. (3) Illnesses characteristic of the common cold could likewise be transmitted. (4) Volunteers who had experimentally induced ARD or common colds, or both, were not immune to primary atypical pneumonia. The clinical characteristics and incubation periods of the induced illnesses were in general consistent with what was known about the corresponding naturally occurring illnesses. No presumptive or definitive causative agents were isolated in the laboratory from any of the specimens obtained from either the donors or recipients of the in ocula in these studies.
Drs. Dingle and Langmuir noted that it was then possible to make some inferences and interpretations and to draw certain conclusions, as follows:
1. An acute respiratory disease (ARD) was the predominant respiratory infection at military training posts, and affected recruits almost exclusively. Clinically, it was an acute, febrile or "grippe-like" infection resembling influenza, from which it was indistinguishable, at least in the individual patient. It was not a "coryzal" disease.
Epidemiologically, it had a distinct pattern of behavior. Like most other respiratory diseases, its prevalence was higher in the winter than in the summer. The level of incidence, however, depended on the time and rate of influx of recruits into the training center. Those units of men inducted in summer months usually did not experience outbreaks of the disease until fall, and the outbreaks were rather prolonged and less abrupt, although the total number of men affected was approximately the same as in acute outbreaks. Those units inducted in fall or winter usually experienced an outbreak within the first 4 to 5 weeks of training, following which both the individual men and the unit seemed to be immune. During such outbreaks, from one quarter to one third of the men required hospitalization. A high turnover rate of recruits resulted in high prevalence of the disease. Thus, ARD seemed to behave as an epidemiology entity.
35
No then known and identifiable bacteria, viruses, fungi, or rickettsiae could be associated etiologically with the disease, nor could any new agent be isolated and shown to play a causative role. The infection could, however, be transmitted to volunteers by inoculation of filtered, bacteria-free secretions of the respiratory tract from a typical patient with the naturally occurring disease. The incubation period ranged from three to nine days with a median of five to six days. The resultant illnesses were similar to the "spontaneously occurring` infection. After recovery the volunteers were immune to challenge with the same inoculum. No cross immunity could be demonstrated between ARD and the common cold or primary atypical pneumonia as transmitted by inocula from the donors selected as having illnesses characteristic of these infections.
The conclusion was thus reached that the cause of ARD was most probably a virus or one or more of a closely related group of viruses.
2. Epidemic influenza A had an epidemiologic pattern that was distinctly different from ARD in that it affected both seasoned men and recruits simultaneously and to an almost equal extent.
3. Although the incidence of primary atypical pneumonia, which by definition required radiographic evidence of pulmonary infiltration for diagnosis, roughly paralleled that of ARD in a ratio of approximately 1 to 10, the relationship was not seasonally constant. Cold hemagglutinins developed in only about one-third of the patients during convalescence. In volunteer studies, ARD did not appear to confer immunity to primary atypical pneumonia. These findings suggested that some, but by no means all, of the cases diagnosed as primary atypical pneumonia could have been caused by the agent or agents responsible for ARD.
4. The occurrence of exudative tonsillitis and pharyngitis, not attributable to infection with group A b-hemolytic streptococci, was infrequent and in general correlated more closely with the incidence of ARD than with any other recognizable factors.
5. The occurrence of minor respiratory illness and symptoms among men on duty, as determined by weekly platoon surveys, at times correlated with hospital admissions for acute respiratory disease, but at other times, particularly in the fall, showed a definite divergence and suggested different etiologies.
6. The epidemiologic behavior of other infections and entities, such as group A b-hemolytic streptococcal infections, bacterial pneumonia, and rubella, was typical of those diseases and did not appear to be dependent on the occurrence of the acute respiratory diseases such as ARD.
Similar diagnostic limitations persisted when CARD investigators transferred their studies from the military population at Fort Bragg to a civilian population in the "Heights" suburbs of Cleveland, within a few miles of their laboratories at Western Reserve University. The study began in July 1947, with the recruitment of five families, all with children, to test the feasibility of data and specimen collection procedures. In addition to assessing the commitment of the parents, particularly the record-keeping mothers, to a long-term study, this meant enlisting the cooperation of the children in welcoming visits to their every illness by physicians and weekly visits by a field nurse. To this end, Dr. Rammelkamp sometimes arrived with a guinea pig in his pocket or with a number of white mice, and, at least once, with a goat(in his pocket!). The staff eventually recruited 86 middle-class families, with443 individuals, to participate in the Cleveland Family Study.
As at Fort Bragg, this longitudinal study of the occurrence of illness in families with young children was largely descriptive. Apart from influenza, few respiratory viruses could be isolated or used for serologic studies until adenoviruses were isolated in the mid-1950s to be followed by respiratory syncytial and parainfluenza viruses. However, by this time, the10-year study was nearly over. As a consequence, the investigators used a term -"common respiratory diseases" - previously used at Fort Bragg to classify respiratory admission based on weekly reports prepared by the hospital registrar. In the Cleveland Family Study, this designation included all nonbacterial illness except influenza, nonstreptococcal exudative tonsillitis and pharyngitis, and primary atypical pneumonia, these three accounting for only approximately2.5% of total illnesses.
Common respiratory diseases included the common cold, rhinitis, bronchitis, and other acute respiratory illnesses of undifferentiated type. This group, now known to be caused by multiple viral agents, was responsible for 95% of all illnesses, of which the common cold accounted for approximately 60%, or
36
about 40% of all illnesses. An average of slightly over six common respiratory illnesses occurred per person-year. Incidence rates for children increased until the age of 3 years and then decreased progressively. In the absence of serologic studies, the decline appeared to be related more to the aging process than to the development of active immunity. Among children, males had higher incidence rates than females, but the reverse was true for adults. The highest attack rates for respiratory disease were found in young schoolchildren. Preschool children with siblings who attended school had consistently higher attack rates than did comparable children without school siblings, presumably because of increased exposure. In general, the larger the family, the greater the individual and family attack rates for common respiratory illnesses. No syndrome comparable to ARD in military recruits was observed, although cases of nonbacterial pharyngitis, some with exudate, that were seen during an epidemic in July and August 1954, were related to the then recently described type 3 adenovirus.
ARD?Adenoviruses
Acute respiratory disease of recruits (ARD), a major cause of morbidity in all military training camps, during and after World War II, and as defined clinically and epidemiologically at Fort Bragg, is a specific etiologic entity caused by several adenovirus types. The first adenovirus associated with ARD was isolated by WRAIR investigators Drs. Maurice R. Hilleman and J. H. Werner from cases that occurred during an influenza-like epidemic at Fort Leonard Wood, Missouri, during the winter of 1952 and 1953. One of the five strains, RI-67, isolated from the pharynx of a patient with the clinical diagnosis of primary atypical pneumonia, was used to demonstrate rises in neutralizing antibodies in the majority of patients studied, most of whom did not have pulmonary infiltration. This finding confirmed the prior observation at Fort Bragg that the percentage (10% to 25%) of patients with infiltrates, and therefore labeled atypical pneumonia, paralleled the incidence of ARD.
In the same year, investigators at the Laboratory of Infectious Diseases of the National Microbiological Institute, NIH, reported the isolation of three immunologically distinct agents from human adenoid tissue undergoing degeneration in tissue culture. They were termed adenoid-degenerating (AD)agents, becoming types 1, 2, and 3, with RI-67 becoming type 4. By the following December, six types had been observed, and the name was changed to adenoidal-pharyngeal-conjunctiva) (APC) agents to reflect the clinical manifestations of cases caused by type 3 that were seen in northern Virginia in association with swimming pools. The adenovirus name for the group was adopted in 1956.
Because sera collected from the donors of respiratory secretions and the volunteers who received them in the human transmission experiments in 1945 had been stored in Cleveland, it was possible to titer them for neutralizing antibody to the RI-67 virus (type 4). Two donors, one diagnosed ARD and one diagnosed bronchitis resembling atypical pneumonia, developed antibody rises. A donor classified as primary atypical pneumonia and two classified as common colds did not. Of recipients of ARD secretion, 20 of 24 developed antibody rises; 40 recipients who received either atypical pneumonia or common cold secretions did not. Tests with these and other sera that used the AD agents(types 1, 2, and 3) showed that they were not associated with ARD. Many subsequent studies have established type 4 adenovirus as a major cause of ARD. Curiously, type 4 infections are rare in civilian populations, and a search for such infections among young men in college or at the U.S. Military and Naval Academies found none.
Over 30 adenovirus serotypes are now known, most of the higher types being inhabitants of the gastrointestinal tract. The most prevalent types among military groups have been types 4, 7, 14, and 21 and, to a lesser extent, type 3. Types 4 and 7 are the predominant types in the United States; types 14 and 21 are prevalent in Europe. In civilian populations, most children become infected with types 1, 2, and 5 early in life. Type 3, as noted, may produce epidemics of pharyngitis or conjunctivitis or both. Perhaps 50% of childhood adenovirus infections result in disease, with 2% to 7% of lower respiratory tract disease in young children seeking medical care being attributed to adenoviruses, particularly type 7. The frequency of these illnesses is not great enough to justify immunization of children. Immunization of recruits, however, is a major success story.
37
CHARLES RAMMELKAMP, M.D., AND WILLIAM S. JORDAN, JR., M.D.
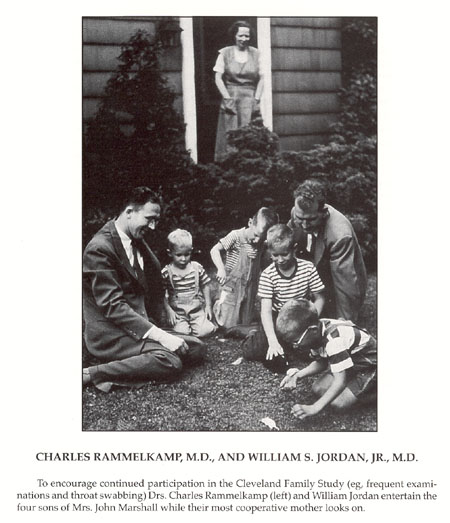{kind=link}
To encourage continued participation in the Cleveland Family Study (eg, frequent examinations and throat swabbing) Drs. Charles Rammelkamp (left) and William Jordan entertain the four sons of Mrs. John Marshall while their most cooperative mother looks on.
38
As a continuation of their studies of type 3 adenovirus, Dr. Huebner and his associates at NIH prepared a killed type 3 vaccine in 1955 that induced neutralizing antibody and prevented illness in volunteers challenged with homologous virus by the conjunctival route. That serum antibody may be protective was suggested in 1956 by studies at Sampson Air Force Base that showed that doses at 5 to 15 mL of gamma globulin prevented illness caused by adenovirus types 4 and 7. With the demonstration that these serotypes were mainly responsible for respiratory disease in military recruits, Dr. Hilleman and his associates at WRAIR developed a killed bivalent types 4 and 7 vaccine with the use of viruses adapted to growth in monkey kidney cell cultures. When evaluated at Fort Dix in 1956, a single dose effected a 98% reduction in hospitalized cases of ARD caused by these agents. Subsequent trials were less successful, apparently attributable to the variable potency of different production lots. Then the oncogenic simian virus 40 (SV40) was found to be present in the killed adenovirus vaccine as well as in viral seed stocks, including adenoviruses and Sabin live polio viruses. A second deterrent to vaccine development was the demonstration of the primary oncogenicity of certain adenovirus types for newborn hamsters, particularly types 12 and 18, and a series of scientific articles reporting the recovery of adenoviruses from a variety of human tumors. Furthermore, the discovery was made that a portion of the SV40 virus genome could become incorporated into the type 7 adenovirus virion, resulting in the formation of a hybrid virus that possessed the oncogenic potential of SV40 virus. In consequence, the Division of Biologics, NIH, acted in 1961 to prevent the distribution of vaccines containing viableSV40 virus and in 1964 to ban additional studies of live adenoviruses in humans until the problem of oncogenicity had been resolved.
The NIAID successor to the National Microbiological Institute contracted with Dr. Maurice Green of the Institute of Molecular Virology, St. Louis University School of Medicine, to search for evidence of oncogenic adenoviruses in a wide variety of human tumors. Green found none. NIAID scientists could not implicate adenoviruses in serologic surveys of human cancer patients for antibody to adenovirus T antigens. Next, adenovirus seeds were obtained free of SV40 and propagated in human cells. When Dr. Chanock and associates at NIAID capitalized on the observation that human adenoviruses exhibit a predilection for infection of the lower intestinal tract, the stage was set for the development of live oral vaccine.
The NIH investigators, using virus grown in human embryonic kidney cell culture, showed that type 4 or type 7 adenovirus could selectively infect the lower intestinal tract when virus was administered in enteric-coated capsules. Virus did not spread from the lower intestinal tract. Selective intestinal adenovirus infection stimulated moderately high levels of neutralizing antibody and was not associated with any signs or symptoms of illness. Because human embryonic cell culture is not suitable for large-scale vaccine production, type4 virus was propagated in human diploid fibroblast cultures to provide large pools of inocula. These were shown to be free of adventitious microbial agents and to be no noncogenic in thymectomized newborn hamsters. When administered to40 volunteers in enteric-coated capsules, the virus infected the lower intestinal tract, induced moderately high levels of neutralizing antibody, and did not spread from enterically infected volunteers to susceptible contacts.
In collaboration with U.S. Navy scientists, Dr. Chanock and his associates at NIAID had observed that adenovirus infections were infrequent among recruits during their basic training at the Marine Recruit Depot at Parris Island, South Carolina but caused epidemics among them when they were transferred to Camp Lejeune, North Carolina for additional training. This sequence made it possible to assess the safety and antigenicity of encapsulatedl ive type 4 virus at Parris Island and to evaluate the protective effect of the vaccine-induced enteric infection when the recruits were later challenged during a type 4 epidemic at Camp Lejeune. When such a placebo-controlled study was done in 1964, no differences in illness patterns were observed at Parris Island between vaccine and placebo groups. The vaccine induced neutralizing antibody within 10 days that reached a median level only twofold lower than that of recruits undergoing natural infection. Of 125 men in the vaccine group, none were hospitalized at Camp Lejeune, and only one experienced a febrile illness(without respiratory symptoms). Of 128 men in the placebo group, 32 were hospitalized and 38 experienced a febrile illness. This
39
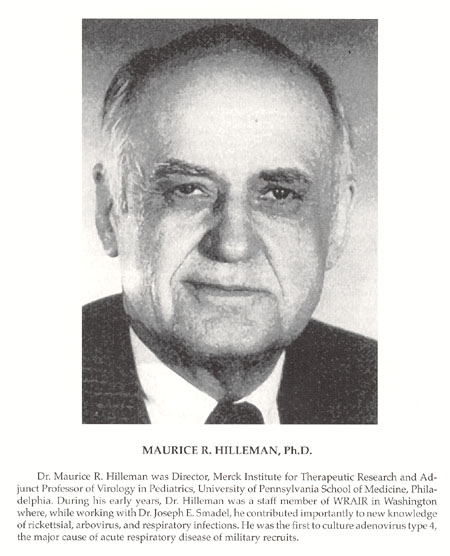{kind=link}
Dr. Maurice R. Hilleman was Director, Merck Institute for Therapeutic Research and Adjunct Professor of Virology in Pediatrics, University of Pennsylvania School of Medicine, Philadelphia. During his early years, Dr. Hilleman was a staff member of WRAIR in Washington where, while working with Dr. Joseph E. Smadel, he contributed importantly to new knowledge of rickettsial, arbovirus, and respiratory infections. He was the first to culture adenovirus type 4, the major cause of acute respiratory disease of military recruits.
40
demonstration of the effectiveness of selective intestinal infection was followed by similar studies at other recruit bases, including the Great Lakes Naval Training Center, Illinois and Fort Dix.
Dr. Jackson and associates at the University of Illinois studied the communicability of live enteric type 4 vaccine in families of military dependents living in government housing at Great Lakes. When the vaccine was given to the mothers of 22 families, 1 of 8 nonimmune fathers and only 1 of 64 children developed evidence of infection. When the vaccine was given to a child in 26 other families, serologic evidence of infection occurred in 3 of 23 nonimmune parents and in 5 of 49 siblings. More extensive spread was recorded when 1 partner in each of 39 married couples drawn from the student population of the University`s Medical Center was given vaccine and the other partner a placebo, but no illnesses occurred attributable to the vaccines. The investigators concluded that while the asymptomatic intestinal infection induced by the vaccine can be spread beyond the bowel to the oropharynx or to other persons by intimate physical contact, the vaccination was benign and highly immunogenic.
The studies at Fort Dix that were conducted by members of the Department of Virus Diseases at WRAIR were the first to show that suppression of type 4 virus by type 4 vaccine fostered the emergence of type 7 virus in the immunized population. A trial of type 4 vaccine in 1965 had reduced hospitalization for ARD by 67.1% and adenovirus type 4 infections by 95.5%; but in a second trial early in 1966, the vaccine apparently failed after 6 weeks of effective suppression. The explanation was the emergence of type 7 adenovirus. Once introduced, it replaced type 4 virus as the epidemic strain. Accordingly, onces tudies failed to implicate type 7 adenovirus as an oncogene for humans, WRAIR investigations assessed the safety, infectivity, and antigenicity of a live enteric type 7 vaccine in humans. Like type 4, type 7 vaccine virus reproducibly infected the gastrointestinal tract, stimulated neutralizing antibody in nearly all susceptible volunteers, and was not associated with illness. Simultaneous administration of type 4 and type 7 vaccines to volunteers confirmed that both types could be administered together without interference. When bivalent vaccine was administered to trainees at Fort Dix in 1969 during an outbreak of ARD caused by type 7 adenovirus, the rate of ARD associated with type 7 adenovirus was reduced by 96%, and no decrease in the immunogenicity of type 4 vaccine was evident.
By the following year, Wyeth Laboratories had replaced the capsules with enteric-coated tablets, and another controlled trial at Fort Dix confirmed the efficacy of tablets of type 4 virus containing between 103.6 and 104.7TCID50 and of tablets of type 7 virus containing between 104.6and 104.7 TCID50. The WRAIR investigators made the important observation that no other respiratory pathogens emerged to replace adenovirus types 4 and 7 as the major causes of ARD in military recruits. The routine use of types 4 and 7 vaccines for the immunization of recruits entering basic training was introduced at Forts Dix, Lewis, and Wood in fiscal year 1970, and at all Army posts in fiscal year 1971. WRAIR personnel estimated that these vaccines prevented nearly 27,000 hospitalizations during these two periods, saving $7.53 million at a cost of $4.83 million, including the cost of a comprehensive surveillance program. In May 1971, the AFEB recommended that type 4 vaccine be administered to recruits and advanced training personnel of all three services and that type 7 vaccine be studied further for clinical effectiveness. By September 1973, 9 months after the termination of the CARD, the AFEB could recommend that vaccine containing both types 4 and 7 adenovirus be administered routinely to these personnel in all services. Adenovirus types 4 and 7 vaccine continues to be administered to recruits in all military services. During the life of CARD and subsequently, Dr. Ginsberg and others characterized further the biochemical and structural properties of adenoviruses and defined the genetic control of their synthetic pathways. Adenovirus vectors containing gene coding for the key antigens of other pathogens are now being used to construct vaccines for other diseases.
Atypical/Mycoplasma Pneumonia
This is the disease that served as the stimulus for the creation of the CARD early in World War II. Historical records suggest that similar syndromes occurred during the Civil War and World War I. During World War I, a pneumonia of an atypical nature unrelated to influenza was recognized clinically. Although similar syndromes were described in Europe in the 1920s and in the United States in
41
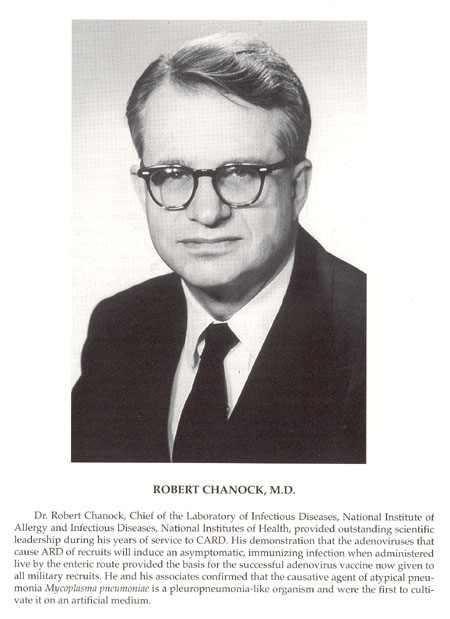{kind=link}
Dr. Robert Chanock, Chief of the Laboratory of Infectious Diseases, National Institute of Allergy and Infectious Diseases, National Institutes of Health, provided outstanding scientific leadership during his years of service to CARD. His demonstration that the adenoviruses that cause ARD of recruits will induce an asymptomatic, immunizing infection when administered live by the enteric route provided the basis for the successful adenovirus vaccine now given to all military recruits. He and his associates confirmed that the causative agent of atypical pneumonia Mycoplasma pneumoniae is a pleuropneumonia-like organism and were the first to cultivate it on an artificial medium.
42
the early 1930s, Dr. Hobart A. Reimann, a Philadelphia internist, described a series of cases in 1938 and popularized the term "atypical pneumonia." Ironically, Dr. Reimann preferred the term "viral" because he believed the causative agent to be a virus. With mobilization, sporadic outbreaks of presumed "virus pneumonia" occurred in civilian and military populations, with the one at Camp Claiborne in the fall of 1941 attracting particular attention. Because the Army Medical Department considered it desirable to adopt a suitable term to differentiate the syndrome from other types of pneumonias, it published an Official Statement in March 1942, that included a clinical description prepared by Dr. MacLeod, Director of the Commission on Pneumonia, and mandated use of the term "primary atypical pneumonia, etiology unknown" because "the description virus pneumonia should be discouraged since a virus has not been demonstrated as the causal agent." The disease became officially reportable by direction of Circular Letter No. 19, Office of The Surgeon General, U.S. Army, 2 March 1942.
As investigators at Fort Bragg tabulated cases with this diagnosis, there were times when atypical pneumonia incidence paralleled that of total respiratory disease, but at other times it did not. It was not related to epidemic influenza, but could it be a manifestation of the agents of ARD and/or minor respiratory illnesses? Definitive epidemiological studies required a diagnostic test more specific than the rise in cold hemagglutinins observed in more severe cases of atypical pneumonia, but repeated attempts failed to yield an etiologic agent with which to develop a test. Accordingly, as noted above, a series of studies were undertaken to transmit the disease to humans to identify secretions that contained the then unknown infectious agent. It had not been possible to transmit the disease to animals.
A preliminary experiment that used unfiltered inocula prepared from pooled throat washings and sputa collected from seven patients on days 3, 4, 12, and 13of typical illnesses and administered intranasally and by aerosol inhalation three times daily for 3 consecutive days induced respiratory illness in 10 of 12volunteers, of whom 3 had roentgenographic evidence of pneumonia and 3,including one in the radiograph-positive group, developed cold agglutinins.
The second experiment was essentially a repeat of the first except that the inoculum was in three forms. Untreated, filtered, or autoclaved inoculum was administered to each man three times during the course of a single day. Of 12 volunteers given filtered inoculum, atypical pneumonia developed in 4and minor respiratory illness in 5. Of 12 men given untreated inoculum, atypical pneumonia developed in 3 and minor respiratory illness in 9. However, of 12volunteers given autoclaved material, atypical pneumonia, although mild, also developed in 3 and minor illness in 9.
The third experiment used a similarly prepared inoculum that consisted of pooled throat washings and sputa collected from six subjects in the second experiment, all of whom developed a rise in titer of cold hemagglutinins. The inoculations, administered by an atomizer and nebulizer, were given out doors to minimize the opportunities for cross-infection. Professional personnel changed gowns and masks between the inoculation of each individual, perhaps because, although not mentioned in prior reports, a physician who administered the inocula for an earlier experiment developed atypical pneumonia. An outbreak of diarrhea among volunteers at the Holly Inn in Pinehurst also was not mentioned. This resulted in scrubbing, painting, and maximum efforts at infection control before it was discovered that someone had quietly put phenolphthalein in the alcohol to determine if the subjects were drinking the alcohol in their thermometer glasses.
The results of the third experiment were as follows: The filtered and untreated inocula each induced atypical pneumonia in 3 of 12 volunteers and minor illness in 5 of 12. The incubation period of the experimental disease was approximately 1 week in subjects who received untreated inoculum and approximately 2 weeks in those given filtrate. Autoclaved inoculum induced no pneumonia in 18 subjects and minor illness in only 1. Thus, infection with the agent of atypical pneumonia was carried through two successive groups of well persons. It was postulated that the minor respiratory illnesses induced might be caused by the same agent responsible for the pneumonia. Equally likely was the possible presence of multiple agents.
As recorded previously, the last volunteer experiment conducted at Fort Bragg demonstrated that two filterable agents, presumably viruses, could induce two types of minor respiratory illness: One was a coryza-like infection with an incubation of 24 to 48 hours (common cold); the other was charac-
43
terized by sore throat, minimal nasal discharge, and an incubation of 5 to 6 days (ARD). Surprisingly, those with ARD (shown later to have been caused by adenovius type 4) experienced no greater febrile responses than those with colds. None developed atypical pneumonia. Volunteers recovered from ARD were resistant to challenge with homologous filtrate. Volunteers who had experienced common colds showed little or no resistance when challenged with homologous filtrate. This filtrate had been prepared with the use of pooled nasal and pharyngeal washings from four donors and may have contained more than one agent, perhaps rhinoviruses. Three volunteers who had one or more previous inoculations with ARD or common cold filtrates developed atypical pneumonia when inoculated with filtrate from a single donor who had atypical pneumonia, suggesting that the filterable agent that causes atypical pneumonia is distinct from the two agents that cause ARD and the common cold. All were presumed to be viruses, a presumption that clouded attitudes regarding the nature of the atypical pneumonia agent for over 15 years.
In December 1942, 2 months after the CARD laboratory was activated at Fort Bragg, Dr. Monroe Eaton and his associates at the Research Laboratory of the California State Department of Public Health reported that an infectious agent from cases of atypical pneumonia could be transmitted to cotton rats and to chick embryos. Passage in cotton rats yielded confusing results, raising the possibility of contamination with an indigenous agent. However, the agent propagated in chick embryos was specifically neutralized by convalescents era from patients with atypical pneumonia. Theses studies continued with support of the Commission on Influenza (and the International Division of the Rockefeller Foundation) and were reported in greater detail in 1944. The agent, also thought by Eaton to be a virus, was now referred to as the Eaton agent. Several investigators attempted unsuccessfully to confirm or repeat Eaton`s studies, and many viewed his results with skepticism. Those at fort Bragg employed the following animals: ferrets, mice, mongooses, kittens, cats, dogs, cotton rats, guinea pigs, hamsters, hogs, monkeys, chimpanzees, chick embryos, chickens, doves, and Java rice birds. No record exists that the investigators obtained and successfully passaged the Eaton agent. After the Fort Bragg team moved to Western Reserve University in 1946, their attempts to isolate the "virus" of atypical pneumonia were minimal while time was devoted to creating a new department and initiating the study of illness in families.
A major advance was reported in 1955 by Dr. Chien Liu, who teamed up with Dr. Eaton, now in the Department of Bacteriology and Immunology of Harvard Medical School. He applied the fluorescein-labeled antibody technique developed by Dr. Albert H. Coons of that department to studies of Eaton agent in chick embryos. Antigen of the agent, still considered to be a virus, was consistently found in the cytoplasm of the epithelial cells lining the lower trachea, bronchi, and air sacs. Interestingly, no antigen was demonstrable in the bronchial epithelium of cotton rats. Between 1954 and 1956,seven strains of "virus" were isolated from patients with atypical pneumonia; one strain was isolated from the frozen lung of a patient who died at the Boston City Hospital in 1943. All isolates were antigenically closely related to or identical with Eaton`s original Mac strain. When the indirect method of fluorescent staining was applied to paired sera from patients with atypical pneumonia, 67% to 92% of patients in several outbreaks showed a rise in antibody titer, including 34 of 38 boys at a private school in Exeter, New Hampshire.
When stored sera from 70 volunteers who participated in the transmission experiments were tested for fluorescent-stainable antibodies at Western Reserve with the use of Liu`s method, 64% to 75% of volunteers showed fourfold or greater rises whether they had developed mild or severe illnesses or no illness at all. Although the greatest mean fold titer rise developed in 7 of 11 volunteers with atypical pneumonia, the data were puzzling and could not be interpreted as proof of the etiologic role of Eaton agent in the infections transmitted at Fort Bragg. Undoubtedly, it was.
When Dr. Chanock and associates at NIH joined with Navy investigators to apply the fluorescent antibody technique to a study of Eaton agent infections in Marine recruits at Parris Island, 161 of 738 patients with pneumonia were serologically positive. Approximately 44% of recruits were infected at some time during the 3-month training period, with only 1 in 30 such infections being manifest as clinical pneumonia.
44
The rate of advance accelerated greatly in the1960s. British investigators B.P. Marmion and G.M. Goodburn were the first to suggest that Eaton agent was not a virus but a pleuropneumonia-like organism (PPLO),having observed minute coccobacillary bodies in infected chick embryo lungs and having noted that the organism was sensitive to an organic gold compound. Dr. Wallace Clyde, a new arrival at Dr. Dingle`s department at Western Reserve, reached a similar conclusion about the same time. Next, Dr. Chanock and associates at NIH and then Dr. Clyde reported the growth of Eaton agent in monkey kidney cell cultures, the latter noting that the agent resembled other members of the genus Mycoplasma in being resistant to penicillin and sensitive to the tetracyclines. Finally, Dr. Chanock and colleagues succeeded ingrowing Eaton agent on fortified PPLO agar and in recovering fresh isolates from12 of 13 serologically positive patients with pneumonia directly on agar.
As the organism was characterized further and distinguished from other mycoplasma, it was designated Mycoplasma pneumoniae. Dr. Clyde described a method for the identification of Mycoplasma species based on inhibition of growth on solid medium around antiserum-impregnated filter paper disks. Seventy-three percent of strains were inhibited by antisera against a strain (Patt prototype) previously unrecognized as a component of the microbiological flora of the normal human throat. This method confirmed that tissue cultures are frequently contaminated by M. hominis type 1. The Patt strain was first called M. pharyngis and is now classified as M.orale type 1.
A number of investigators were quick to use the newly available culture and serologic (complement fixation) methods to study the epidemiological and clerical characteristics of M. pneumoniae infections in selected populations. Chief among these were Drs. Grayston, Foy, Alexander, George Kenny, and their coworkers at the University of Washington. In studies of M. pneumoniae infection in 114 families in which a case of atypical pneumonia was noted, M. pneumoniae was isolated from the throat of an index patient in 36 families. Transmission to other family members occurred in 23 of these 36families, with 84% of the children and 41% of the adults becoming infected. Of59 patients with family-contact infections, 42 had lower respiratory tract symptoms, 6 had pharyngitis alone, 9 (all children) were asymptomatic, and 2were judged to have unrelated symptoms. The results obtained indicated that M. pneumoniae spreads slowly but extensively, especially in families with small children, and the clinical response includes a spectrum from inapparent infection to pneumonia. Treatment with tetracycline did not abolish the carrier state.
After 5 years of surveillance of the population of a large medical cooperative, the Seattle investigators reported that M. pneumoniae was associated with 20% of all pneumonia. During an epidemic that lasted approximately 18 months, the highest attack rate occurred in children 5 to 9years old, while the proportion of pneumonia caused by M. pneumoniae was highest among the teenagers. Treatment with tetracycline or erythromycin reduced the length of illness but not the antibody response. Understandably, the incidence of atypical pneumonia stimulated attempts to develop a vaccine. The protective effect of an inactivated M. pneumoniae vaccine prepared by Pfizer Laboratories was evaluated by Chanock`s group at NIH by first injecting volunteers with vaccine and then challenging them with the organism. Growth-inhibiting antibody developed in 10 of 19 seronegative volunteers; only 1of these 10 became ill when challenged. Respiratory disease developed in 7 of 9men who failed to respond to the vaccine and in 10 of 13 seronegative volunteers in the unimmunized control group. The most severe illnesses developed in men who failed to respond to the vaccine. The investigators suggested that the vaccine had a protective effect in those who developed antibody, while those vaccinees who failed to develop antibody may have been sensitized.
Dr. William Mogabgab of Tulane University, a contractor of the Commission on Influenza, evaluated an inactivated vaccine prepared by the Merck Institute for Therapeutic Research in trainees at Keesler Air Force Base, Mississippi, including over 10,000 men in each vaccine and placebo group. Because 40% of vaccines showed no antibody response by complement fixation and27% by neutralization, a second dose of vaccine was administered. Little increase in antibody response resulted. Serologic studies of 167 cases of pneumonia in the 2 groups suggested that the vaccine did reduce the number of men with pneumonia caused by M. pneumoniae, but the rate of all clinically diagnosed pneumonia was lowered by only 45%.
45
In the waning days of the CARD, investigators in Dr. Denny`s department at the University of North Carolina administered an inactivated M. pneumoniae vaccine prepared by the Huntington Research Center under contract to NIAID/NIH to 12antibody-negative children and 6 antibody-positive children. Few or no rises in complement-fixing (CF) or growth-inhibiting antibody were detected in the 12subjects who were initially antibody negative, and minimal increases were observed in children with preexisting antibody. Peripheral lymphocytes obtained before immunization from antibody-negative children were not stimulated by M. pneumoniae antigen in vitro, but five of the six immune subjects had reactive lymphocytes. Antigen-reactive lymphocytes appeared in 58% of the antibody negatives after the first inoculation and in 91% after the booster dose. These data suggested that inactivated M. pneumoniae vaccine may be inadequate for primary immunization and that rises in antibody, when elicited, may be caused by anamnestic stimulation of naturally acquired immunity. This finding provided a possible explanation for the prior observation that some immunized volunteers who did not develop detectable antibodies experienced more severe disease after challenge.
In 1974, 2 years after CARD was terminated, former colleagues of Dr. Jordan at the University of Virginia evaluated an inactivated vaccine prepared under contract with NIH by investigators at Ohio State University. Dr. Richard Wenzel and associates followed 7,861 Marine Corps recruits at Parris Island in a double-blind study. Twenty-one vaccinees (5.5 per 1,000) and 43 placebo recipients (10.9 per 1,000) were hospitalized with pneumonia; the overall protective efficacy was 51%. Based on serologic data, the protective efficacy was 67%; based on culture for M. pneumonia it was 42%. No hypersensitization was observed.
Concurrently, attempts were made to develop an attenuated vaccine on the premise that infection of the respiratory tract with a living but a virulent organism would stimulate greater local immunity. These attempts were abandoned because the mutants developed were either over attenuated or there was fear of reversion to virulence. Work on vaccines ceased in the mid-1970s for a variety of reasons, including the unpredictable, sporadic occurrence of infection; the availability of effective antibiotic therapy; and the fear that immunization that does not result in a protective level of antibodies may lead to more severe disease in the face of natural challenge. The latter concern was based in large part on a series of observations made in Denny`s laboratories at the University of North Carolina.
When Denny moved from Cleveland to Chapel Hill, Dr. Clyde went with him, and they were soon joined by others, particularly Dr. Gerald Fernald, to study M. pneumoniae infections in hamsters. Electron micrograph studies showed that a differentiated portion of M. pneumoniae, consisting of an extension of the unit membrane containing an electron dense core surrounded by a lucent space, serves as the means of attachment to host cell membrane. No mycoplasma were seen within cells. The initial infection was judged to be a superficial one that disturbs ciliary function and injures tracheal epithelium. When the protective effect of prior infection was compared with protection after immunization with killed vaccine, previous infection precluded infection in all animals, but parenteral vaccine was not protective despite high serum antibody titers. This suggested that local immunity, either humoral or cellular, plays an important role in resistance. Accordingly, hamsters were immunized with an attenuated strain. Resistance developed only after intranasal infection. Again, serum antibody levels did not correlate with protection. A virulent vaccine prevented pneumonia in animals challenged with homologous virulent organisms but not in those receiving an unrelated strain. Virulent vaccine provided protection against both homologous and heterologous challenge. Clearly, local immune factors were of primary importance and it would be necessary to find a way to preserve the immunogenicity of live attenuated strains.
Histological and immunological studies of hamsters showed that a perivascular-peribronchial reaction occurred on the 3rd day on reinfection of previously infected animals. Very few cells were positive for immunoglobulin. These recall lesions suggested that delayed hypersensitivity is a major component of acquired immunity. On the contrary, could such an inflammatory response play a major role in the pathogenesis of the disease inhumans? Could it be that primary, usually asymptomatic, infections in children sensitize them for more severe infections as teenagers and adults? Second infections have been reported by investigators at the University of Washington and others, but the data are
46
insufficient to answer these questions. They and the problems cited above have been sufficient, however, to eliminate M. pneumoniae from a priority listing of vaccines that merit development.
Common Cold/Rhinoviruses
The third acute respiratory disease identified clinically and epidemiologically by the CARD investigators at Fort Bragg and transmitted to volunteers was a coryzal illness with a short incubation characteristic of the common cold. Unlike the situation with atypical pneumonia and ARD, a number of prior studies in volunteers had provided evidence that the common cold was an infectious illness caused by a filterable agent. The first of these volunteer studies was reported in 1914 by Dr. W. Kruse, who suggested that the agent be called A phanozoum coryzae. During and after World War I, in Germany, between 1917 and 1928, approximately eight groups of investigators administered filtered (Berkefeld candle) secretions to volunteers, but four groups failed to demonstrate transmission. The results of the others were confounded by the detection of anaerobic, filter-passing, gram-negative microorganisms in the inocula.
Over 2 years in the late 1920s, Dr. Dochez and associates at the College of Physician and Surgeons, Columbia University, satisfied themselves that the microorganisms were contaminants and that another agent was responsible for causing colds in 44% of both chimpanzees and male volunteers. Dr. Long and his associates at The Johns Hopkins School of Hygiene and Public Health knew of this work and set out to confirm it in June and July 1930. They did so using female volunteers. Coryzal infections with incubations of 20 to 70 hours were transmitted singly and in series through 2 and 4 passages in 9 of 15 persons. Both groups concluded that the filterable infectious agent was a virus, and subsequent investigators tended to refer to the search for the virus of the common cold.
Dr. Dochez was to become one of the first members of the Board; Dr. Long became the first Director of the Commission on Meningococcal Meningitis. Through visits to the CARD laboratory at Fort Bragg and participation in meetings of the AFEB, they undoubtedly played a role in encouraging CARD to conduct its series of volunteer experiments. As a result of many other volunteer studies in the following years, conducted principally by Drs. Jackson and Dowling at the University of Illinois and by Sir Christopher H. Andrewes and his successor Dr. David Tyrrell at the Medical Research Council Common Cold Research Unit in Salisbury, England, it became evident that infectious secretions from different individuals with colds contained different viruses, observations validated with the identification of rhinoviruses.
Dr. Andrewes, the Head of the Department of Bacteriology and Virus Research at the National Institute of Medical Research in London, took on the challenge of the common cold after World War II when the prefabricated facilities first occupied during the war by the Harvard Hospital were given to the Ministry of Health. Dr. Andrewes had begun his studies by taking volunteers to the northern islands to expose them in drafty halls and to cold foot baths to mimic the changes that seemed to bring on colds. With the support of the Medical Research Council, Dr. Andrewes and his colleagues moved to "a wind-swept hilltop just outside Salisbury," in southern England, to found the Common Cold Research Unit. By the time he came to Boston in 1949 to deliver the Dunham Lectures, he was already able to report on observations in 1,500 volunteers inoculated with filtered or unfiltered nasal washings. Dr. Andrewes` host for the lectureship was Dr. Finland of the Thorndike Memorial Laboratory of the Harvard Unit at the Boston City Hospital.
One of Dr. Finland`s Fellows, Dr. Jackson, was assigned to chauffeur Dr. Andrewes to his various appointments and social occasions. Dr. Jackson has recalled that Dr. Andrewes` "knowledge and enthusiasm about opportunities and puzzles in the emerging information about viruses as causes of disease bubbled over with a catching enchantment." When Dr. Jackson joined Dowling at the University of Illinois College of Medicine in Chicago, Jackson and his colleagues took full advantage of an elabo-
47
rate laboratory built by the university for the study of the biological effects of climatological environment to investigate the effect of chilling on the pathogenicity of infectious nasal washings. Using thermocouples for continuous recording of cutaneous, turbinate, and central temperatures of volunteers placed in chambers with precisely controlled temperature and humidity, they created their own Common Cold Research Unit under the sponsorship of CARD. A friendly rivalry continued between the two units and Drs. Jackson and Tyrrell, their leaders for many years, as they studied a variety of respiratory viruses. Dr. Jackson was to serve for several years as a Professor at the London Hospital Medical College and head of its Department of Virology before returning to his home state of Utah; Dr. Tyrrell retired in the late 1980s and the Common Cold Research Unit at Salisbury was deactivated.
That minor respiratory illnesses are caused by multiple agents could also have been inferred from data provided by the Cleveland Family Study. Families with young children living in the suburbs of Cleveland in the late 1940s and early 1950s experienced nearly 10 illnesses per person per year. Common respiratory diseases, a description that included the common cold, constituted 60% of all illnesses and 95% of all respiratory illnesses. An average of 6.2 common respiratory illnesses occurred per person per year. Babies acquired infections with considerable frequency after the first 30 days of life. Incidence rates for children continued to increase until the age of 3years and then decreased progressively. The highest attack rates were found in young school children. Preschool children with siblings who attended school had consistently higher attack rates than did comparable children without school siblings. Once introduced into the home, the highest secondary attack rates were in preschool children (49%) and schoolchildren less than 6 years of age(37.5%). Among the parents, mothers (27.4%) had higher secondary attack rates than fathers (17.0%).
However, the investigators tended to analyze common respiratory disease as a clinical entity and to interpret the data as indicating a gradual development of immunity caused by an aging process rather than as the result of repeated experience with "the agent." This concept was reinforced by the observations that secondary attack rates for preschool children were similar regardless of whether there were schoolchildren in the family and whether the school children had higher total attack rates and a greater risk of infection outside of the home but had no greater secondary attack rate than did preschool children of the same age. The hypothesis was advanced "that there is little prolonged modification in immune status as the result of repeated experiences with infection, but that there is a gradual process which reduces susceptibility as age increases." The data were sufficient to predict the frequency of infections currently experienced by young children in day-care centers but, perhaps because there was still a tendency to think of "the agent," were not interpreted as predicting the eventual discovery of over 100 common cold viruses.
For the next decade, investigators depended on volunteers for studies of the common cold, efforts that did identify multiple cold viruses and that continue to the present to explore the mechanisms of their transmission, the pathogenesis of the resulting infections, and approaches to their treatment and prevention. For no other infectious disease have so many human subjects willingly agreed to suffer an experimentally induced illness.
In a series of thoughtfully designed studies, requiring first the use of an objective symptom score for assessing the presence of an illness and its severity, Drs. Dowling and Jackson and colleagues observed nearly 4,000 volunteers who participated in controlled challenge studies. Because their subjects were not isolated, extra controls were necessary. Among the first 1,034 subjects who received an infectious secretion as an initial challenge, 449 (42%) developed colds compared with 70 (10%) of 696 subjects who served as a control population and simultaneously received a buffer solution.
Among 73 subjects who developed no cold on initial challenge, 7 (10%) developed colds on rechallenge with the same infectious secretion. Among 71subjects who developed a cold on initial challenge, 6 (8%) developed a cold on rechallenge. The interval between challenges varied from 3 to 45 weeks. No evidence was noted that the secretions had lost their infectivity between challenges.
In contrast, among 74 subjects who developed no cold on initial challenge with an infectious secretion, 31 (40%) developed a cold when challenged later with another secretion. Among 41 subjects who developed a cold on initial challenge with an infectious secretion, 19 (46%) developed a cold when challenged later with another secretion. The interval between challenges varied from 10 to 74 weeks.
48
Common Cold/Rhinoviruses
With the use of nasal secretions as inocula, the investigators induced colds in 35% to 40% of young adults. Secretions differed in infectivity; none infected all subjects. The "take rate" was slightly higher in allergic subjects but was not influenced by smoking or a history of tonsillectomy. The rate was higher in females in the middle third (77%) of the menstrual cycle than in the first and third of the cycle (28% to 30%). Neither sex nor season altered susceptibility. It was not possible to induce increased susceptibility of the subjects by chilling them with controlled alterations of temperature and humidity. In addition to specific immunity to reinfection to the same nasal secretion, pooled human gamma globulin was shown to neutralize the infectivity of nasal secretions. Sera collected 6 and 12 months after infection provided nearly complete protection against infectious secretion. These observations suggested that the common cold is caused by a number of different viruses that are antigenically different and that following infection, human subjects develop a specific immunity against each virus.
The first rhinoviruses were isolated by Dr. Winston Price at The Johns Hopkins School of Hygiene and Public Health (JH strain) and Dr. W. Pelon and associates at Naval Medical Research Unit (NAMRU) No. 4, Great Lakes (2060strain), using procedures that had been successful in isolating adenoviruses but substituting primary monkey kidney cells for HeLa cells. In view of the number of serotypes subsequently identified, it was a surprising coincidence that J Hand 2060 viruses were shown to be antigenically identical. Drs. Jackson and Dowling, along with one of Dr. Pelon`s coinvestigators, Dr. Mogabgab, soon demonstrated that JH and 2060 viruses produced colds in volunteers and that infection with one virus protected against not only the homologous virus but against the other, corroborating the close immunological relationship between them. They became prototypes for rhinovirus IA.
Dr. Mogabgab, who was to continue his studies at Tulane University School of Medicine, had observed that 2060 virus was also cytopathic for human embryonic kidney cells but not for HeLa cells. Then Dr. Tyrrell and associates reported the isolation of strains that would grow only in human cells, and Drs. Hamparian, Ketler, and Hilleman (now at the Merck Institute for Therapeutic Research) soon isolated at least six distinct serotypes by using human fetal kidney and human fetal lung cells. Drs. Hamparian, Ketler, and Hilleman proposed the name "coryza virus,"but this designation and Dr. Kruse`s A phanozoumcoryzae lost out to rhinovirus, the name suggested by Dr. Andrewes and the staff of the Common Cold Unit.
The use of readily available human diploid cells and of microneutralization tests, such as that developed by Dr. Jack N. Gwaltney in Dr. Jordan`s laboratory at the University of Virginia, facilitated numerous epidemiological studies and resulted in the identification of multiple rhinovirus serotypes. Use of the 73different antisera available in 1967 typed 75% of the rhinovirus isolates collected over a 3-year period. Forty-eight different types were identified; 61strains were untyped. The most frequent isolate, type 14, was associated with only 8.4% of rhinovrus illnesses. In 1987, 100 types were classified officially, and at least 25 untyped isolates awaited full comparison with these 100.
The Charlottesville investigators found that rhinoviruses accounted for 23% of respiratory illness experienced by an industrial population during a 3-yearperiod. Recurrent annual fall peaks occurred during which rates of rhinovirus isolation exceeded 45%. In a study of military recruits during 4 weeks of training, investigators at NAMRU No. 4, Great Lakes, found that 90% became infected with one or more of at least 12 different serotypes. Forty percent of recruits sustained two or more infections confirmed by virus isolations, with many infections occurring in the first week of training. During a 4-year period of observation of families in Seattle, Dr. John Fox and associates at the University of Washington recorded spring and fall peaks of rhino virus infections. Such infections accounted for 16% of all respiratory illnesses (20% of upper respiratory), with rhinovirus illness in children being more severe and twice as frequent as in adults. Infants experienced a 78% secondary attack rate. Homeotypic immunity was associated with relative protection (52% to 59 %effective).
As with other picornaviruses, rhinovirus immunity is serotype specific. Although studies that used volunteers have shown that experimental vaccines can reduce the rate of symptomatic illness and viral shedding (but not the overall rate of infection), the large number of specific antigenic types has caused
49
investigators to turn their attention to search for forms of prevention other than conventional viral vaccines (eg, receptor blockade, interferonprophylaxis).
Finally, during the Cleveland Family Study, antihistamines were shown to have no beneficial effect on the occurrence and subsequent course of common colds in families or in experimentally infected volunteers. This observation wasc onfirmed by many others and reconfirmed by an extensive review in 1987. Neither the report in 1950 or the recent review has had any impact on the incorporation of antihistamines in cold remedies.
Of course, many other viruses exist that cause acute coryza. Among these are influenza; coronaviruses such as 229 E, OC43, and BB14; certain adenoviruses andentero viruses; viruses important in childhood that reinfect both children and adults, particularly respiratory syncytial and parainfluenza viruses; and viruses yet to be discovered. Vaccines are being developed for some of these, but clearly there will be no universal all-purpose vaccine or antiviral for common respiratory disease.
Pneumococcal Pneumonia
The story of the prevention and treatment of pneumococcal pneumonia before, during, and after World War II has many stars, including a number of scientists associated with the AFEB and its commissions. This account focuses on vaccine development and particularly on the contributions of three outstanding investigators and their associates: Drs. Heidelberger and MacLeod of the Commission on Pneumonia and Dr. Austrian of the CARD. Effective treatment (eg, sulfonamides or penicillin) that became available late in World War II, is mentioned only to note that its arrival served to suspend and delay vaccine research for a number of years.
Dr. Heidelberger began his studies of the constituents of the pneumococcus in the 1920s with Dr. Avery of the Rockefeller Institute and soon became one of the leading students of bacterial polysaccharides, particularly those of pneumococcal serotypes. Dr. MacLeod, who also had studied the pneumococcus while a postdoctoral fellow with Dr. Avery before moving to New York University, later engaged in studies with Avery, in collaboration with Dr. Maclyn McCarty, which were to identify deoxyribonucleic acid (DNA) as the substance that could transform one type to another, ie, the carrier of genetic information. Dr. MacLeod was named Director of the Commission on Pneumonia before the report of this seminal observation was published and was to lead it through a successful trial of pneumococcal quadrivalent polysaccharide vaccine in military personnel in 1944 and 1945. Dr. Austrian, who collaborated with Dr. MacLeod on studies on the pneumococcus at New York University after the war, was to revive interest in the use of the vaccine 20 years later when he and Dr. Jerome Gold, at SUNY Downstate Medical Center, documented the continuing importance of bacteremic pneumococcal pneumonia as a cause of mortality in Kings County Hospital, Brooklyn, despite the use of antibodies.
In the spring of 1963, Dr. Austrian reported at the annual meeting of the Association of American Physicians that the mortality of bacteremic pneumococcal pneumonia treated with antibiotics was still nearly 20%. Of all deaths, 60%occurred in the first 5 days after onset of illness, apparently from irreversible physiological injury that was unaffected by antibiotic therapy. When the details of this study were published 1 year later, Drs. Austrian and Gold emphasized that "evidence extant suggests strongly that the morbidity and mortality from pneumococcal infection can be reduced significantly by prophylactic vaccination of persons at high risk with a preparation of six pneumococcal polysaccharides."
Dr. Austrian has credited Drs. O. Schiemann and W. Casper with being the first to report in 1927 that specific soluble substances of pneumococci were immunogenic in the mouse. Similar observations were described in humans 3 years later by Drs. Francis (first Director of the Commission on Influenza and later President of the AFEB) and Tillett (one of first members of the Commission on Pneumonia). Then, studies by Dr. Finland (later an associate member of CARD) with Drs. Sutliff (later a member of the Commission on Pneumonia) and Ruegsegger (later a member of CARD) led to the first large trials of vaccines of pneumococcal capsular polysaccharides in the Civilian Conservation Corps in the late 1930s. Dr. Felton and associates administered ambivalent vaccine containing 1 mg each of the polysaccharides of types 1 and 2 to over 40,000 adult males; the results, although promising, were inconclu-
50
sive. Meanwhile, Dr. Heidelberger had been continuing his studies and was soon able to provide purified type-specific polysaccharides when the need a rose at Sioux Falls Army Air Base.
As previously noted, one of the first official acts undertaken by Dr. MacLeod was preparation of a clinical description of atypical pneumonia that became part of an official statement published in March 1942. In November of that year, he was sent to Sioux Falls Army Air Base to investigate an epidemic of atypical pneumonia. This base had been opened in the summer of 1942 as a Technical School for the training of radio operators and continued as such until the late spring of 1945. The epidemic of atypical pneumonia began shortly after the base opened, but beginning in December 1942, the picture changed; pneumococcal pneumonia appeared as the most important pulmonary infection and remained at epidemic levels throughout the whole period of operation of the school.
In the summer of 1943, Lieutenant Hodges was assigned to Sioux Falls as epidemiologist and remained there for 2 years. Facilities for typing pneumococci had been set up after Dr. MacLeod`s visit and one technician had been trained in these techniques. Consequently, a picture of the type distribution of pneumococci became available.
In January 1944, the experience of the preceding years was reviewed, and from this analysis it became evident that six pneumococcal types were responsible for75% to 85% of all cases of pneumonia. Type 2 was the most important epidemic type, causing approximately 35% of all cases, followed by types 1, 5, 7, 12, and4, in that order. Because of the consistent behavior of these types of pneumonia throughout the preliminary study and because it could be anticipated that pneumonia would remain epidemic at this post, a controlled study of antipneumococcal immunization was suggested. This study was approved by the AFEB and, with the collaboration of Colonel William P Holbrook and Major A. C. van Ravenswaay of the Army Air Force Rheumatic Fever Control Program, was put in operation in August 1944. The Office of the Air Surgeon constructed a special pneumonia laboratory and assigned trained personnel. The presence of Dr. Hodges and the provision of excellent facilities and laboratory personnel made possible extensive epidemiological studies, particularly with reference to distribution of pneumococci in the throats of normal and sick men and in their environment.
Between September 1944 and April 1945, a carrier survey for pneumococci was conducted. The subjects consisted of one squadron in the Technical School, whose members were cultured at intervals, and control subjects consisted of all admissions to the hospital for upper respiratory infections and a group of 100surgical patients. The carrier rate was similar in each of these groups and pneumococci showed the same type distribution. Accordingly, it was concluded that the method of sampling provided a good cross-section of the population. From an analysis of cultures carried out on men at various periods after arrival at the post, it was shown that the infective or epidemic types were acquired after arrival. Moreover, the predominant types of pneumococci in the throats of the men could also be isolated regularly from the dust of the schoolrooms where the men spent their entire training time as well as from the dust of the barracks. The population thus became uniformly seeded with the infective types. Pneumococcus type 12 was of particular interest, because during 3 months between January and March 1945, more than 12% of the population of 10,000 men were carriers. At the same time, type 12 was the chief cause of pneumococcal pneumonia, far outstripping types 1, 2, 5, and 7, which in the preceding 2 years had been predominant, but as noted below were controlled during the winter of1944 and 1945 by means of immunizing with specific capsular polysaccharides of these four types.
In addition to the widespread distribution of infective types of pneumococci, it was shown that nonbacterial respiratory disease was a second important factor contributing to the maintenance of epidemic pneumonia. Throughout the whole period of the operation of the school, one patient with pneumococcal pneumonia was admitted for every 10 patients with nonbacterial respiratory disease, and the incidence curves paralleled each other. As at other bases, this relationship held true even during the periods when influenza A and B were epidemic in 1943 and 1945, respectively. During both of these influenza epidemics, which involved a considerable portion of the population, the incidence of pneumonia also increased considerably, but the 10 to 1 ratio was maintained. Dr. MacLeod, from whose final report of the director this information has been reproduced, suggested that these findings appeared to indicate influenza A and B do not cause a greater predisposition to pneumococcal pneumonia than undifferentiated nonbacterial respiratory disease. Rather, the increased morbidity from pneumonia
51
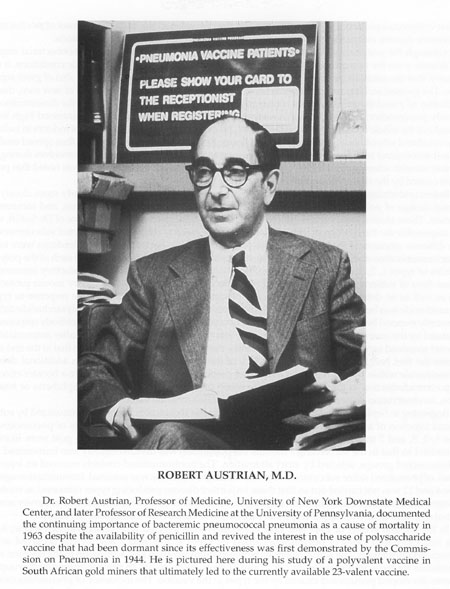{kind=link}
Dr. Robert Austrian, Professor of Medicine, University of New York Downstate Medical Center, and later Professor of Research Medicine at the University of Pennsylvania, documented the continuing importance of bacteremic pneumococcal pneumonia as a cause of mortality in 1963 despite the availability of penicillin and revived the interest in the use of polysaccharide vaccine that had been dormant since its effectiveness was first demonstrated by the Commission on Pneumonia in 1944. He is pictured here during his study of a polyvalent vaccine in South African gold miners that ultimately led to the currently available 23-valent vaccine.
52
during influenza epidemics is caused by the absolute increase in the number of cases of nonbacterial respiratory disease and not to a predisposing capacity of the influenza virus infections.
Although the pneumococcal carrier rate for infective types and the incidence of nonbacterial respiratory disease were the two most mportant components in the perpetuation of epidemic conditions, it was apparent that the constant inflow of young, susceptible individuals into the post was also of great significance. The greatest incidence of pneumonia occurred within the first 6 weeks of arrival of new men, during which they acquired the infective types of pneumococci. The nature of training favored the dissemination of not only pneumococci but also agents of nonbacterial respiratory disease, which maintained high levels throughout the whole of the operation of the school. All of the working hours were spent indoors in indifferently ventilated school rooms with dusty cement floors. Respiratory disease pathogens thus spread easily. It was not determined how the infective types of pneumococci were able to maintain themselves during the summer months when environmental conditions were clearly improved, although it was noted that pneumonia caused by the these types occurred even during the summer months.
Before undertaking the proposed vaccine trial, it was considered important to study more closely the optimal dosage of polysaccharides for immunization, quantitate the immune response, and measure its duration. These studies were carried out chiefly by Dr. Heidelberger with the assistance of Dr. Sutliff, who was responsible for the titration of sera in mice. Groups of medical students were injected subcutaneously with different amounts of the polysaccharides and with a whole bacterial vaccine. Bleedings were taken before immunization and at intervals for 2 years thereafter. It was found that 0.06 mg of each of the polysaccharides of types 1, 2, 5, and 7, injected subcutaneously in a single dose, gave a satisfactory immune response. Sera of subjects immunized showed type-specific antibody (types 1 and 2) by mouse protection tests as well as on determinations of specifically precipitable nitrogen. In general, the response to type 2 polysaccharide was better than to type 1, but individuals who responded well to one polysaccharide did not necessarily respond better than average to the other polysaccharide. The height of the antibody response, as measured by the quantitative precipitin technique, was found to occur about 3weeks after immunization; the level remained more or less constant for 6 months thereafter, declining gradually, so that at the end of 18 months the titer had fallen to about 33% or 50% of the highest level. Injection of an additional dose of polysaccharide within the first year and a half after original immunization did not give a booster effect, in sharp contradistinction to the experience with protein immunizing agents such as diphtheria or tetanus toxins, an observation since shown to be true of other polysaccharide vaccines.
Beginning in September 1944,50% of the students in the Technical School were immunized by subcutaneous injection of a single dose of 0.06 mg of each of the capsular polysaccharides of pneumococcus types 1, 2, 5, and 7 in a volume of 1mL. Thereafter, alternate men arriving on the post were likewise immunized so that in the succeeding 7 months the population was divided equally into immunized and nonimmunized groups, selected by strict alternation. The nonimmunized controls received an injection of 1 mL of phenolized saline subcutaneously. Reaction to the injections was minimal. Immunization against types 4 and 12 was not carried out so that these important disease-producing types remained as controls. To determine the effect of immunization on pneumococcal carrier rates, a continuous carrier survey among normal men and men with upper respiratory disease was carried out throughout the study.
In the fall and winter of 1944 and 1945, 8,586 men were injected with quadrivalent vaccine; 8,449 were not. Only four cases of pneumonia caused by types 1, 2, 5, and 7 adenovirus occurred in the immunized population. The actual intervals between immunization and admission to the hospital with pneumonia for these four cases were 2, 6, 7, and 11 days, respectively. In the nonimmunized group, 26 patients developed pneumonia caused by the types in the vaccine. The incidence of pneumonia caused by all other types was identical in the two groups. These studies demonstrated clearly that immunization of humans with specific capsular polysaccharides of selected pneumococcus types was effectivei n preventing the development of pneumonia caused by those types.
Of equal interest was the observation that immunizing 50% of the population greatly reduced the incidence of pneumonia caused by the vaccine types in the nonimmunized subjects. This conclusion was based on the observed behavior of pneumonia caused by types 4 and 12 during the seasons of 1942 and 1943, 1943 and1944, and 1944 and 1945. During these three seasons, the rates for pneumonia caused by types 4 and 12 were closely similar; during the 1942 and 1943 and 1943and 1944 seasons the
53
ratios of the incidence of types 4 and 12 pneumonia to the incidence of pneumonia caused by 1, 2, 5, and 7, respectively, were similar. From the actual incidence of types 4 and 12 pneumonia in the 1944 and 1945season, it was thus possible to calculate the expected incidence of types 1, 2,5, and 7 pneumonia for the winter of 1944 and 1945, when immunization was in practice. The incidence of pneumonia in the nonimmunized fraction of the population caused by the four types in the vaccine was but 17.6% of the expected.
Explanation for the reduction in pneumonia caused by vaccine in nonimmunized men was provided by the carrier studies. The carrier rates for these types in the immunized population were significantly lower compared with the nonimmunized population. Thus, immunization prevented the development of the carrier state for these specific types or else shortened its duration, and because thorough mixing of the immune and nonimmune groups occurred, the immune subjects acted as a barrier in the transmission of these types of pneumococci from one man to another.
The study at Sioux Falls has been described at some length because it was the first definitive demonstration of the efficacy of a tetravalent vaccine. In his final report as Director of the Commission on Pneumonia, Dr. MacLeod prophetically stated, "There is no reason to believe that the number of polysaccharides to be used in a single injection could not be considerablyi ncreased, to include most of the predominant disease-producing types of pneumococcus." Indeed, he soon reported that six capsular antigens could be combined in a single vaccine and that most subjects responded to all antigens.
E. R. Squibb and Sons then developed and marketed two six-valent pneumococcal capsular polysaccharide vaccines. One vaccine, formulated for use in adults, contained polysaccharide types 1, 2, 3, 5, 7, and 8; the other vaccine, intended for use in children, contained types 1, 4, 6,14,18, and 19.Neither of Squibb`s vaccines ever gained widespread acceptance. Physicians in the early 1950s chose to rely on new antimicrobial agents to treat bacterial pneumonia, rather than on prevention through immunization. In 1954, therefore,S quibb terminated its production of pneumococcal vaccine. The Laboratory of Biologics Control of the National Microbiologics Institute, NIH, withdrew without prejudice Squibb`s license to produce these vaccines, and the Squibb subsequently abandoned all of its pneumococcal vaccine research and development programs.
After this, with increasing reliance on antibiotic treatment therapy, perception of the need for the development of a pneumococcal polysaccharide vaccine generally diminished until Drs. Austrian and Gold produced data between1952 and 1962 showing that, despite antibiotic treatment, the mortality rate for bacteremic pneumococcal pneumonia was still high. In their study at Kings County Hospital, these researchers found that 10 types of pneumococci accounted for at least 70% of pneumococcal pneumonia cases. Of patients treated for bacteremic pneumococcal pneumonia with penicillin or other antibiotics, 17%died. Among patients over 50 years of age, the mortality rate was 28%,and among individuals with complicating illnesses such as heart disease, stroke, and pulmonary emphysema, the mortality rate was 30%. Patients died despite early treatment. In addition, other investigators found that the emergence of antibiotic-resistant strains of pneumococci was becoming a significant problem in the treatment of pneumococcal diseases. These findings sparked renewed interest in the development of a pneumococcal vaccine, with Dr. Austrian being its leading proponent.
In 1967, the newly created Vaccine Development Committee of NIAID recommended to Dr. Davis, the Institute`s Director, that funds be provided for research and development of pneumococcal vaccine. NIAID contracted with Eli Lilly and Company to develop an experimental polyvalent polysaccharide vaccine with Dr. Austrian and other investigators to test it. In 1976,13 years after his first report to the Association of American Physicians, Austrian informed that group of the convincing results obtained in a population of novice goldminers (strikingly like military recruits) in South Africa. In a trial of at ride cavelent vaccine, there were 17 cases were noted of radiologically confirmed putative pneumococcal pneumonia and/or bacteremia or both in 1,493vaccinees versus 160 such illness in 3,007 control subjects, a 78.5% reduction in illness. There were 10 bacteremic infections noted that occurred later than 14 days after immunization with the vaccines versus 113 such infections in control subjects, an 82.3% reduction. Much less convincing efficacy was later demonstrated in trials in two elderly U.S. populations.
54
Just as Lilly`s vaccine was being shown to be effective in South Africa, the company made a corporate decision in 1975 to stop producing it, terminating most of its other vaccine research, development, and production in the following year. Fortunately, Merck Sharp and Dohme intensified its efforts to develop a pneumococcal vaccine. Merck, with Dr. Hilleman leading its vaccine program, had committed itself earlier to the task of developing and producing a meningococcal polysaccharide vaccine for the Army. Merck conducted independent clinical trials among gold miners in South Africa and obtained levels of safety and efficacy comparable to those found by Austrian with the product produced by Lilly.
Merck applied to the Food and Drug Administration (FDA) in 1976 for a license to manufacture and market a 14-valent vaccine. The company was issued a product license on 21 November 1977, and began marketing PNEUMOVAX in February 1978. Lederle Laboratories, another vaccine producer, obtained a product license for its 14-valent vaccine in August 1979 and began marketing PNU-IMMUNE shortly thereafter. These vaccines were replaced by 23-valent vaccines in 1983 that contain polysaccharide antigens for the 23 capsular types, which cause 88%of bacteremia pneumococcal disease in the United States. The clinical effectiveness of these vaccines has varied greatly in different population groups in studies that are difficult to evaluate. No other testing opportunities have existed comparable to those presented by the illness in the recruits at Sioux Falls and the novice gold miners in South Africa. The consensus is that the 23-valent vaccine is 65% to 70% effective, and its use is recommended.
Streptococcal Infections
The respiratory tract is victimized by a multiplicity of microbes, so it is inevitable that those studying a particular respiratory pathogen will of necessity recover other agents and contribute information about them. Such is the case with hemolytic streptococcal infections and influenza, for which the AFEB formed separate commissions. Detailed accounts are to be provided of the work of these two commissions, so only observations made under the auspices of CARD at Fort Bragg and Cleveland are included here. In both locations, cultures were used to identify streptococcal infections and to describe their epidemiological behavior. At Fort Bragg, the absence of positive cultures inpatients with exudative pharyngitis served to identify a new syndrome?nonstreptococcal-exudative pharyngitis. At other bases, the CABI used streptococci as markers to track the dissemination of bacteria in barracks. This section follows the one on Streptococcus pneumoniae with an account of CARD and CABI studies on S. pyogenes. The next section summarizes CARD studies of influenza.
A year after the CARD laboratory was activated at Fort Bragg, the occurrence of an extensive epidemic of streptococcal pharyngitis and tonsillitis as a result of group A, type 5 adenovirus in November 1943 presented an opportunity for a detailed study of the clinical, epidemiological, bacteriological, and immunologic aspects of streptococcal infection and an opportunity to conduct a controlled study of sulfadiazine therapy. The epidemic was confined to members of two companies of an airborne infantry regiment. Epidemiological evidence incriminated creamed eggs served at breakfast as the probable vehicle of infection.
The outbreak was explosive, with a median incubation period of 38 hours and a primary attack rate of 42%. The secondary attack rate was 30%, of which one half were cases and one half carriers. Of patients with type 5 infection, 100 were hospitalized from a group consisting of 32 officers and 228 enlisted men. None of the patients had scarlet fever.
The illnesses were mild to moderately severe and did not differ appreciably from sporadic contact or airborne cases caused by other types of streptococci. As in previous studies of sporadic streptococcal infection, the history and appearance of the throat were typical in the majority of cases, but in some the diagnosis could not have been made by clinical criteria alone. Pharyngeal or tonsillar exudate was present in 90% of the cases; in only 25% was it confluent and in another 25% it was no more than a pinhead. Although symptoms, physical signs, and fever were rapid in onset, maximal in intensity within 48 hours, and declined rapidly, complete return to normal was frequently protracted. Untreated patients who
55
MARGARET PITTMAN, M.D., MICHAEL HEIDLEBERGER, M.D., AND WILLIAM JORDAN, JR, M.D.
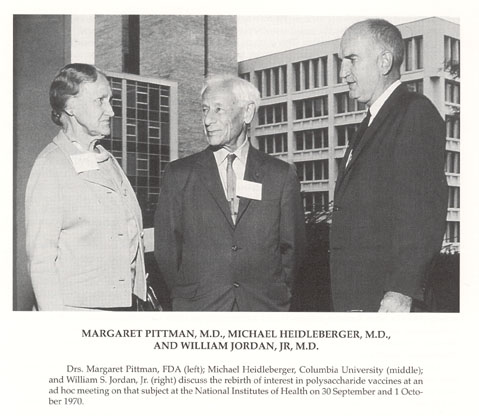{kind=link}
Drs. Margaret Pittman, FDA (left); Michael Heidleberger, Columbia University (middle); and William S. Jordan, Jr. (right) discuss the rebirth of interest in polysaccharide vaccines at an ad hoc meeting on that subject at the National Institutes of Health on 30 September and 1 October 1970.
56
previously had a tonsillectomy exhibited somewhat more fever than those with tonsils, but other significant or consistent differences in clinical severity between the two groups were not found.
Alternate patients were treated with sulfadiazine. A slight reduction was demonstrated in fever and in the daily frequency of certain symptoms, particularly sore throat, but no objective evidence of benefit was found with regard to the local inflammatory reaction. It was concluded that no benefit was derived from sulfadiazine chemotherapy.
Suppurative complications were few, but a number of nonsuppurative complications were detected. These included three cases of acute rheumatic fever and two others in which that diagnosis was suggested but not established. One probable exacerbation of chronic glomerulonephritis was encountered, but no examples of acute glomerulonephritis were found. Transient microscopic hematuria was detected frequently early in the course of illness.
A significant rise in titer of antistreptolys in or antifibrinolys in was found during convalescence in 85% of hospitalized cases. Another 12% of cases had arise in titer of antistreptolysin of less than two tubes. No correlation was found between the severity of illness and either the initial titer ofantistreptolys in antibody or the maximum titer during convalescence. However, the termination or persistence of the convalescent carrier state did appear to be related to the height of the antistreptolysin response. Similar antibody responses appeared in nearly half of the "healthy" carriers, indicating that a proportion of these carriers were subclinical cases. Transient carriers did not exhibit an antibody response, whereas those who carried the organisms for more than 10 days did.
Subsequently, an analysis of approximately 3,000 consecutive admissions to the hospital for respiratory disease was made to establish the importance of hemolytic streptococci as a cause of respiratory illness. The patients were new recruits studied from March 1943 through April 1945. On admission to the hospital, a throat culture was obtained, and in those patients showing exudative lesions of the pharynx or whose first culture showed hemolytic streptococci, a second and usually a third culture of the throat was taken. A blood specimen was taken at the time of admission to the hospital and approximately 3 weeks later. Antistreptolysin O and antifibrinolysin titers were determined on all acute and convalescent sera obtained from patients harboring streptococci. All subjects whose convalescent sera showed an increase in either the antistreptolysin or antifibrinolysin titer were considered to have a streptococcal infection.
Of the 3,000 hospital admissions, 466 or 15.6% were found to harbor streptococci. The carrier rate of new recruits in the field was approximately10%. Group A streptococci, or group A in combination with other groups, accounted for approximately 90% of the infections. Group C infections were found in 5.5% and group G in 3%. Acute- and convalescent-phase sera from 92% of the466 patients harboring streptococci were available for study. Of the convalescent sera of the patients, 38% exhibited a significant increase instreptococcal antibodies. When all soldiers hospitalized for respiratory disease were considered, cultural and serologic results indicated that only 6% had immunologic evidence of streptococcal infection, although more than twice this number harbored streptococci in their throats. Nonstreptococcal exudativepharyngitis was twice as common as true streptococcal exudative pharyngitis.
In sum, streptococcal infections accounted for very few respiratory illnesses among new recruits at Fort Bragg. In his Director`s report for 1945, Dr. Dingle stated, "The etiology of non-streptococcal pharyngitis is unknown but its clinical pattern suggests a close resemblance to ARD." As noted previously, he was correct; adenoviruses, along with other viruses, were the most important cause of disease.
At other bases, CABI investigators had used streptococci to test sampling procedures for assessing the bacterial content of air in barracks. In the process, they identified the nasal carrier as the "dangerous carrier" of hemolytic streptococci. Individuals with strongly positive nasal cultures were shown to disperse, on average, nearly 100-fold as many streptococci as throat carriers.
In the Cleveland Family Study, streptococcal pharyngitis and tonsillitis accounted for 2.8% of approximately 15,000 respiratory illnesses. No case of streptococcal respiratory disease was diagnosed during the first year of life. After that, attack rates increased to a peak during ages 5 to 7 years, then decreased with advancing age. By age 5.8 years, children had experienced, on average, one case per child, by 8.5 years, two cases, and by age 13, three cases per child. A detailed study from 1
57
January 1948 through 1 July 1952, undertaken to describe the frequency of the acquisition of group A streptococci and the factors influencing the spread within families, disclosed certain similarities between the epidemiology of streptococcal acquisition and the occurrence of common respiratory diseases.
Acquisition most commonly occurred during January through June, with rates of acquisition being highest in young schoolchildren. Once a group A streptococcus was acquired, there was a 40% rate of streptococcal illness, but types 4 and 12resulted in higher illness rates and were the most common types isolated in the study. Schoolchildren most commonly introduced a group A streptococcus into the family unit?six times as frequently as their parents. The secondary carrier rate was 25% when the index carrier had a group A streptococcal illness but only 9% when he or she did not have such an illness. Children 3 and 4 years old had the highest risk of becoming secondary carriers (50%).
The spread of streptococci in the family unit often occurred quite slowly, and the carrier state frequently persisted for a long time. No cases of rheumatic fever were recognized, but the occurrence of a case of acute glomerulonephritis after a type 12 infection in November 1950, accompanied by asymptomatic hematuria in other members of the family, provided the clue that led Dr. Rammelkamp to postulate that only certain types of group A streptococciare nephritiogenic. This hypothesis was reinforced by the occurrence of a second case of nephritis after a type 12 infection in March 1953.
Influenza
During the first 3 years of the CARD studies at Fort Bragg from December 1942 to April 1945, paired sera were collected from 2,433 patients with respiratory disease and tested for increases in titer of hemagglutination-inhibiting antibodies to influenza A and B viruses. During an epidemic of influenza A in December 1943 and early January 1944, 120 serologically confirmed cases were documented. In nonepidemic periods, eight fourfold or greater increases in titer of antibodies to influenza A and 10 to influenza B were detected in cases that were not recognized clinically. Such endemic occurrence of sporadic cases was proposed to constitute the reservoir of virus between epidemics, but of course, no viruses were isolated to support this suggestion.
During the epidemic, influenza, in contrast to ARD, attacked seasoned men and recruits without preference. Subclinical infections, as determined serologically, were apparently three times as common as overt clinical illness. Although no unusual incidence was noted of pneumonia during the epidemic, a shift occurred away from the predominant occurrence of atypical pneumonia toward an increased incidence of pneumococcal pneumonia.
A comparison of the clinical features of cases of epidemic influenza with the clinical features of cases of ARD observed during the epidemic of influenza and the succeeding epidemic of ARD showed that the clinical picture in these two types of respiratory illness were similar. This conclusion also was reached during the epidemic because difficulty was encountered in making a differential diagnosis between the two syndromes, a problem encountered at other bases. The first adenovirus isolated from a patient with ARD came from a specimen collected during overlapping influenza and ARD epidemics.
A correlation was noted between the pre epidemic titer of antibody and the incidence of febrile illness during the epidemic. A titer of 16 or less indicated a relative susceptibility to febrile illness, and a titer of 64 or more indicated a relatively high degree of immunity. Similar results were subsequently obtained by others, and roughly equivalent antibody levels (≤10and ≥40) are still cited by those interested in influenza immunization as indicative for relative susceptibility or immunity.
Studies on the distribution of influenza virus were carried out to determine the duration of infectivity of cases of influenza and to search for carriers of the virus. A total of 247 throat washings were collected from hospitalized and well soldiers. Tests on 110 washings obtained from 46 hospitalized patients whose convalescent sera showed a twofold or greater increase in titer of antibody to influenza A virus showed that patients with influenza commonly carried the virus for as long as 5 days and occasionally as late as the 11th day. Influenza virus was most readily isolated from washings obtained during the first 3 days of illness.
58
Serial throat washings were obtained from 38 well soldiers during the epidemic. A total of 108 washings was obtained. Influenza virus A was isolated from the washings of two individuals. Each of these two men admitted having had a mild illness, but neither had reported to sick call. Convalescent serum from each showed a definite increase in antibody titer to influenza virus A. Virus was not isolated from any individual whose serum failed to show an antibody response. Thus, cases of influenza were shown to have been infectious for the first 3 to 5 days after onset of illness and occasionally for as long as 11 days. No true carriers of influenza virus were found.
Epidemic influenza B was encountered in Puerto Rico when members of the CARD were on the island carrying out studies in the mongoose on the etiology of atypical pneumonia. An epidemic of respiratory disease in soldiers occurred during late July and August 1943 in Puerto Rico and St. Thomas, Virgin Islands. Tests on acute and convalescents era from 16 patients were negative for influenza A (PRB strain). Sera from six patients showed fourfold or greater increases in titer and sera from three patients showed at least a twofold increase in titer when tested with influenza virus B (Lee and Bon strains). The increases in titer were of greater magnitude with the Bon strain in seven instances and with the Lee strain in one instance. Thus, the epidemic strain was more closely related to the Bon strain than to the Lee strain. (The Bon strain was isolated by Sir McFarland Burnet in Australia; the Lee strain was isolated by Dr. Francis in the United States) This was one of the early demonstrations that influenza B viruses, like influenza A, exhibit antigenic variation.
An imaginative attempt to find a cyclical pattern to recurrent epidemics of influenza and to define their periodicity was made by the CARD staff, almost certainly at the initiative of Dr. Langmuir. A theory was devised by examining the 16 widespread epidemics that occurred between 1920 and 1944. The theory classified the 16 epidemics in an orderly fashion on the assumption of a 2- or 3-year cycle for influenza A and a 4- to 6-yearcycle for influenza B. This concept of the periodicity of influenza varied from earlier theories in two essential respects: "1) was based on the knowledge that two serologically distinct viruses may cause epidemics, an essential point unknown until recent years; and 2) no attempt was made to establish rigid or fixed cycles but rather a definite but limited degree of variation in the cycles is postulated." The investigators proposed that four implications regarding the epidemiology of influenza seem warranted if their theory was correct:
-
There is no need to postulate a third variety of influenza virus (exclusive of pandemics);
-
The probability rather than the actual prediction of an epidemic in any specific year becomes possible;
-
Influenza survives between epidemics as an endemic or sporadic disease; and
-
The epidemics of influenza depend, in addition to the factors, upon an upset of the balance between susceptible and immune in the population.
Dr. Langmuir was sufficiently confident in his ability to predict the year and viral type of the next epidemic that he wagered a bottle of Scotch that he could do so with any colleague. The theory had a short life, and Dr. Langmuir probably lost more bets than he won. Things changed, particularly the influenza A virus. In 1947, a new A variant, prototype FM/1/47 (FM for Fort Monmouth) replaced the H1N1 virus of the late 1930s and early 1940s, the PR8 strain. The viruses were sufficiently different as to cause PR8 to be classified initially as H0N1.In 1950, progressive antigenic drift brought another set of H1N1viruses, which persisted until a major antigenic shift brought the H2N2(Asian) pandemic. H2N2, in turn, exhibited progressive antigen drift until replaced by the H3N2 (Hong Kong)pandemic. Then an HIN1 virus antigenically similar to those of 1950 reappeared in China in 1977 and spread through Russia and the rest of the World. H2N2 virus has not yet reappeared.
Thus, the passage of time and new data have invalidated the first assumption on which the theory of periodicity was based. More than two serologically distinct viruses exist because there is more than one A virus. In recent years, two A strains (H1N1 and H3N2) and a B strain have caused illnesses every year, although some outbreaks have been predominantly A or B.
Both viruses undergo progressive antigenic "drift"; A viruses undergo more major antigenic changes referred to as "shifts," once suggested to occur roughly every 10 years. However, this periodicity has
59
not held up either, unless the reappearance of H1N1 be counted as such. Despite elegant studies that have described the three-dimensional structures of the two surface glycoproteins? the hemagglutinin(HA) and neuraminidase (NA)-and have located the amino acid substitutions that distinguish one A variant from another, it has not been clearly established how influenza survives between epidemics, other than in humans. Because animals and birds have their own influenza A viruses, and ducks, in particular, have viruses with many HA antigens, including H1, H2, and H3, it has been suggested that genetic recombination between a human virus and an animal or avian, particularly duck, virus produced the new pandemic human viruses in the past. As yet, no one has proposed a theory to predict when this gene transfer will occur in the future.
The Cleveland Family Study was carried out from 1947 to 1957 when influenza H1N1viruses were prevalent and was well-prepared to assess the impact of Asian (H2N2) influenza during its initial epidemic appearance in the United States. The laboratory was well-established by 1948. H1N1 viruses were isolated in 1949, 1950, 1951, and 1953, and influenza B viruses were isolated in 1950 and 1952.Thus, measurement of the occurrence and recurrence of influenza in the same individuals and families was possible over a period of years. Furthermore, it was possible to examine simultaneously the importance of two variables immunity and antigenic variation? in relation to recurrent infections with members of the H1N1 set of viruses. In addition to the study of epidemics in 1950, 1951, and 1953, an opportunity existed to examine sera collected at 6-monthintervals since 1948. These serologic studies spanned a 6-year period and provided information regarding the pattern of antibody response during and between epidemics.
Moreover, the population was suited for the collection of data regarding the impact of Asian influenza during its initial epidemic appearance in the United States in the fall of 1957. Therefore, the study, which had been terminated in May 1957, was reestablished for this purpose. Clinical and serologic attack rates were determined and measurements made of the influence of this new influenza virus on the bacterial flora of the upper respiratory tract. Furthermore, the clinical characteristics of the illnesses produced by the H2N2 strain and those produced by the previous H1N1 strains were compared.
In the three H1N1 epidemics, virus was isolated from 71 individuals: 30 adults and 41 children. Viruses were isolated from one person in two different years, 1950 and 1953. Virus was isolated only once from specimens collected from asymptomatic individuals. Thus, 70 individuals, representing 40 families, were infected as demonstrated by virus isolation studies, but recurrent infection in the same individual apparently was rare. A rather constant percentage (25% to 28%) of families yielded virus in each of the 3 years. Of the 14 families with virus in 1950, 11 remained in the study in 1951, and virus was isolated from 1.Ten of the 1950 virus-positive families were under observation in 1953, and viruses were isolated from three. Of the 15 families with virus in 1951, 14 were in the study in 1953, and viruses were isolated from 4. Of the 18 families with viruses in 1953, 17 had been observed in both 1950 and 1951, and viruses were obtained from 7 in one of these years. In each instance, the numbers observed are the numbers expected if the virus isolation rates for the given years are applied to the various families in the groups, except in the case of the 1950positive families when three isolations would have been expected in 1951. Thus, on the basis of presence of virus in the families, a slight suggestion was noted that those families infected in 1950 were spared in 1951 but not in 1953. On the basis of presence of virus in families, those families infected in 1951 showed no evidence of family immunity in 1953.
Of the individuals exposed to virus in the families in three different years, about the same percentage developed respiratory symptoms. Thus, the occurrence of H1N1 infections in the community in the two preceding years (1949 and 1950) did not reduce the clinical manifestations of the disease in 1951. Indeed, a greater percentage of individuals had influenza like illnesses in 1951 than in 1953 after an interval of 1 year, during which influenza infections were not recognized clinically or by isolation.
Although analysis of virus isolation data alone showed little or no evidence of immunity and the clinical expression of influenza like infection did not diminish in the total population in successive epidemics, the clinical data suggested that natural infection did confer some degree of immunity. When the occurrence of influenza like illnesses during the three epidemic periods was tabulated in relation to
60
ALEXANDER D. LANGMUIR, M.D., M.P.H.
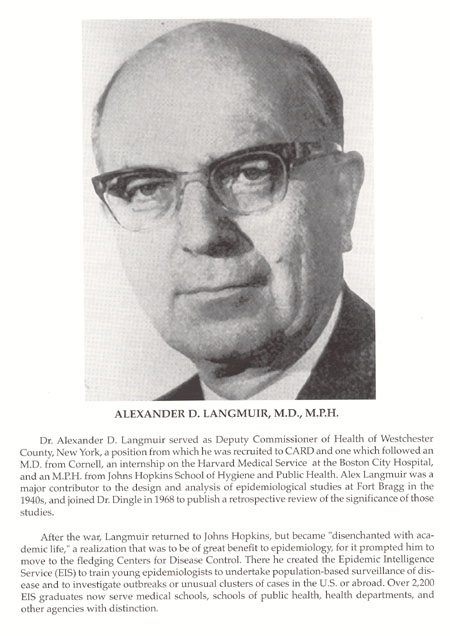{kind=link}
Dr. Alexander D. Langmuir served as Deputy Commissioner of Health of Westchester County, New York, a position from which he was recruited to CARD and one which followed an M.D. from Cornell, an internship on the Harvard Medical Service at the Boston City Hospital, and an M.P.H. from Johns Hopkins School of Hygiene and Public Health. Alex Langmuir was a major contributor to the design and analysis of epidemiological studies at Fort Bragg in the 1940s, and joined Dr. Dingle in 1968 to publish a retrospective review of the significance of those studies.
After the war, Langmuir returned to Johns Hopkins, but became "disenchanted with academic life," a realization that was to be of great benefit to epidemiology, for it prompted him to move to the fledging Centers for Disease Control. There he created the Epidemic Intelligence Service (EIS) to train young epidemiologists to undertake population-based surveillance of disease and to investigate outbreaks or unusual clusters of cases in the U.S. or abroad. Over 2,200 EIS graduates now serve medical schools, schools of public health, health departments, and other agencies with distinction.
61
the previous virus experiences of the family of the individual, the occurrence of such illnesses in the members of a given family during one epidemic apparently was influenced by whether or not virus had been isolated from that family during the preceding epidemic. Of those individuals in virus-positive families in 1950, 6% had influenza like illnesses in 1951. In contrast, of those not in demonstrated contact with the virus in 1950, 24% had such illnesses in 1951. Of those individuals living in families from which virus was isolated in 1951, 6%had influenza like illnesses in 1953; in contrast, 20% of persons not in contact with the virus in 1951 suffered influenza like illnesses in 1953. Thus, prior familial contact with the virus effected an approximate 70% reduction in rates of influenza like disease after an interval of either 1 or 2years.
Individuals who developed fourfold or greater increases in titer as a result of the 1951 epidemic experienced a 50%reduction in development of such increases during the 1953 epidemic. However, individuals who had influenza in 1950 did not have a reduced attack rate in1953. Thus, when influenza like illnesses in the families were used as the criterion for immunity, individuals in families infected in 1950 had significantly less influenza in 1951, and individuals in families infected in1951 had less influenza in 1953. Some degree of immunity, then, persisted for 1or 2 years but not for 3.
Hemagglutination-inhibition tests on sera collected at approximately 6-month intervals indicated that infections with influenza viruses were constantly occurring. During epidemic periods, 15% to 25% of individuals showed significant increases in titer to the prevalent viruses, both A and B in1950, A in 1951 and 1953, and B in 1952. During each endemic period, rises in titer were found. The majority of increases in the endemic periods were measured with antigens closely related to the current strain; when FM1 was examined for a single antigen, FM1 virus, 17% to 60% of significant increases were eightfold or greater. These facts support the conclusion previously drawn at Fort Bragg that the titer increases were indeed induced by endemic infections; again, infection was not documented by virus isolation.
Tabulation of the increases and decreases in antibody titers showed that before the influenza A epidemics of 1951 and 1953 and the influenza B epidemics of 1950 and 1952, the population exhibited more falls than rises and thus, in a sense, had developed a negative antibody balance. Similarly, the B epidemic of1952 and the A epidemic 1953 were preceded and followed by periods during which the average antibody titer of the population decreased.
In summary, studies during the 6 years from 1948 to 1953 provided information particularly regarding the occurrence of infection with H1N1viruses. During the H1N1 epidemics of 1951 and 1953,approximately 25% of the population demonstrated serologic evidence of infection. As measured by virus isolation, approximately 25% of the families were infected in each of the three H1N1 years, and 50% to75% of the individuals in these families suffered respiratory illness at that time.
In anticipation of the 1957 Asian (H2N2)epidemic, two teams were sent to South America (see below), and the Family Study was reactivated when the 60 remaining families agreed to participate again in the collection of detailed clinical and epidemiological data. H2N2virus was first isolated in Cleveland in June 1957, and two other sporadic infections were documented in July and August. The first known case in the study population occurred on 2 September just after the study resumed; Cleveland schools opened 9 September; the next two cases occurred on 19 and 20 September at the beginning of the epidemic.
As in previous years, respiratory disease rates had risen after the opening of schools and were already high by the week of 22 September. For the next 2 weeks, nearly all of the respiratory illnesses resembled the common cold and its variants. Then more severe, influenza like illnesses increased in frequency, reaching a peak during the week of 13 October. In 8weeks, the epidemic was over. Approximately 73% of all respiratory illnesses were sampled; H2N2 virus was recovered from 42.5%. Virus was isolated from 92% of those thought clinically to be influenza, and 27% of milder illnesses were classified clinically as common respiratory diseases. Viruses were isolated from 52 (86.7%) of the 60 families and from 126 (40.9%) of the 308 members of these families. The combined results of the complement-fixation and hemagglutination-inhibition tests showed that 93% of persons from whom virus was isolated developed fourfold or greater increases in antibody titer. All told, 60% of the population developed increases in antibody titer during the epidemic. Attack rates for children were much higher than for adults and were
62
maximum in the age 5 to 15+ year groups. The pattern of attack rates in the family resembled that of the common respiratory diseases, being lowest in the fathers and highest in the schoolchildren. The importance of the school was emphasized by additional examination of the data. Considering the first virus-positive case as the index case, influenza was introduced into the 52households as follows: 43 times by a schoolchild (83% of all introductions),once simultaneously by a schoolchild and mother, 3 times by a mother and preschool child, and only twice by a father.
With members of the H1N1 set of viruses, the occurrence of influenza was related to at least three factors: (1) chance, (2) persistence of immunity for 2 years, and (3) the emergence of minor antigenic variants. A major variant was responsible for the Asian pandemic. When H2N2virus appeared, few, if any, members of the population had specific antibody. In contrast to serological attack rates of 15% to 25% observed with the H1N1strains, the serological attack rate in unvaccinated persons was 55% for the H2N2virus. In comparison with the earlier H1N1 epidemics. Asian virus infected more than three times as many families and two to three times as many persons. Despite this high attack rate, the clinical disease produced resembled that caused by the H1N1 strains; no significant alterations in the bacterial pharyngeal flora in the population accompanied or followed the virus infections, and no complications occurred. There were no individuals over age 60 years in the particular population understudy, and this may be the reason no complications were observed, for in the greater Cleveland area, as throughout the United States and the world, the Asian influenza epidemic was associated with an excess number of deaths from influenza and pneumonia. Dr. Masaro Kaji, a visiting scientist, isolated virus from the extra pulmonary tissues of some of these fatal cases. Because schoolchildren, to an even greater extent than military recruits, are immunological virgins, the importance of the school was of interest. The attack rate was highest in the age5 to 15+ year group, and schoolchildren were responsible for more than 80% of the introductions of virus into the homes. Furthermore, the length of the intervals between the onset of the index and subsequent virus-positive cases in the families suggested that many of the secondary infections were acquired at school rather than in the home. The median interval of 7.4 days between the first and all subsequent cases was similar to the interval observed in outbreaks in other cities. These data suggested that during the initial wave of Asian influenza, community spread of the virus was greater than intrafamily spread. Although no ready explanation existed for this apparently paradoxical behavior of a highly infectious agent, one explanation that was offered was that it was the result of a combination of the greater susceptibility of children plus the opportunity for greater multiplicity of contact within the school. Virus had been present in the community for more than 3 months before the epidemic, and in Cleveland, as elsewhere, the opening of schools seems to have been one of the provocations that triggered the epidemic.
Because influenza often occurs in the southern hemisphere during its winter season before occurring later in the northern hemisphere in its winter season, the appearance of the H2N2 influenza A variant in Asia prompted the decision to explore the possibility of studying the anticipated epidemic of Asian influenza in South America before its arrival in the United States. In July 1957, a team composed of Dr. Keith Jensen, University of Michigan, for the Influenza Commission; Dr. Jordan, Western Reserve University, for CARD; Captain John R. Seal, for the U.S. Navy; and Dr. Arturo Saenz, Pan American Health Organization, visited health officials and laboratories in Brazil, Uruguay, Argentina, and Chile to select a site for such studies. Santiago, Chile, was recommended. Health authorities in Santiago planned to organize a Committee on Influenza under the chairmanship of Dr. Abraham Horwitz, Professor of Preventive Medicine and Sub-Director of the National Health Service. This team and the subsequent Influenza Study Group were greatly assisted by Dr. Manuel Borgono of the sub department of infectious diseases, National Health Service.
An Influenza Study Group composed of members of three commissions was formed to collaborate with the Chilean Committee. On 8 August 1957, four members of the group, Dr. Houser, SUNY at Syracuse, Field Director (CARD), Dr. Davenport and Mr. Peterson, University of Michigan (Influenza); and Dr. Willard C. Schmidt, Western Reserve University (Streptococcus), arrived in Santiago to learn that Asian influenza had occurred aboard a naval ship in Valparaiso the day the first team departed.
63
The rapid spread of the disease in Santiago and Concepcion precluded vaccine trials, but joint observations were made of the epidemiological, clinical, virological, bacteriologic, serologic and pathological features of the epidemic.
As the survey team later learned, influenza was first noted in the north of Chile in the second week of July 1957. A week later it was in Santiago and subsequently in the central and southern provinces of the country. The epidemic was accompanied by a high rate of pulmonary complications. The sharp increase of pneumonia in Santiago on 2 August came 10 days after the sharp increase of influenza cases. The twofold increase in deaths during the epidemic was coincidental with the increase in pneumonia, and most of the increase in deaths was attributable to influenza and pneumonia. The very young and the elderly contributed predominantly to the fatalities, but an increase was noted in deaths in all age groups. Post influenzal pneumonia was more severe than the typical pneumonia of past years but responded relatively well to antibiotics with only a slight increase in hospital fatality rates. Although a variety of organisms was associated with the fatal cases of pneumonia, S. pyogenes was most frequently isolated. Some fatal cases were attributed to primary influenzal pneumonia. The majority of the patients with pneumonia developed antibodies against the Asian virus.
These observations alerted those in the United States as to what to expect, although with not as much lead time as hoped. The successful collaboration between United States and Chilean scientists also led to continuing studies of streptococcal infections and rheumatic fever under the auspices of the Commission on Streptococcal Diseases.
An account of vaccine studies is found in the history of the Commission on Influenza. As for another form of prevention, Dr. Jackson of CARD and his associates were among the first to confirm reports of Soviet scientists that amantadine prophylaxis will prevent influenza A virus infections in volunteers. The drug has been shown to be about as effective as vaccine in field trials when given early in an influenza A epidemic. Unfortunately, resistant viral mutants have appeared that may diminish its usefulness in the future.
Meningococcal Meningitis
Epidemics of meningococcal infection and its most dramatic manifestation, meningitis, have occurred in all wars since the illness was first described in the early 1800s in Europe. Within a month of mobilization in World War I, the incidence began to increase in the U.S. Army; within 7 months, an explosive outbreak of meningitis had begun. The AFEB anticipated that a similar sequence would occur in World War II.
In 1941, when the Commission on Meningococcal Meningitis was first formed, the incidence of meningococcal meningitis was low and sporadic in nature. Beginning with the fall of 1942, cases of meningococcal meningitis began to increase among both the Army and civilian personnel. From 1942 through 1944, the United States experienced the most severe epidemic ever recorded by the Public Health Service. Army personnel shared in this experience, and the CARD, from July 1941 through June 1943, received over 5,000 case records from Army personnel stationed in the continental United States.
Among Army personnel the disease was one of new recruits. Of the cases, 67% occurred among men in the Army fewer than 3 months, 15% in those who were in the Army for 4 to 6 months, 7% for 7 to 9 months, and 4% for 10 to12 months. Although this was a period of rapid expansion in the Army, the concentration of cases in the first 3 months of service was consistent throughout the entire period.
When compared with previous experience, the mortality from meningococcal meningitis and meningococcemia was exceedingly low because of the availability and effectiveness of sulfadiazine therapy. In 1937,Drs. Schwentker, Gelman, and Long had reported from the Sydenham and Johns Hopkins Hospitals of Baltimore that the then new compound sulfanilamide cured 10of 11 patients with invasive meningococcal disease. In 1940 and 1941, during the previously mentioned outbreak in Halifax, Nova Scotia, Drs. Dingle, Thomas, and A. R. Morton showed that a successor sulfonamide, sulfadiazine, was effective in another small group of patients. Extensive use of sulfadiazine during the
64
major group A epidemic in late 1942 and early 1943 confirmed the value of the drug as a therapeutic agent and related studies showed that small doses eliminated the carrier state and could be used for prophylaxis.
In the last paragraph of his final report as Director of the Commission on Meningococcal Meningitis, Dr. Phair summarized its contributions as follows:
A disease like meningococcal meningitis whose symptomatology is so striking and whose mode of spread is so mysterious often occasions far more concern than the associated morbidity or mortality warrants. Through study of the disease and its mode of spread the Commission has been able to represent the probable mode of dissemination. The bulk of the epidemic wave was found to result in subclinical or inapparent infection. Clinical cases were erratic and unreliable indicators of the extent of infection. These subclinical infections apparently stimulated and increased capacity to resist future clinical infection. The organism could be eradicated quickly and easily with the sulfonamide drugs. In this way fear was allayed, and the shifting and deployment of troops, so urgent at this period, were not affected.
During the life of the Commission on Meningcococcal Meningitis, its members assisted in a number of field studies. In these instances, an investigative team and equipment from the central laboratory at The Johns Hopkins School of Hygiene and Public Health were dispatched to the post in question. These were Jefferson Barracks, Missouri, Fort Eustis, Virginia, and Fort George G. Meade, Maryland. All involved carrier surveys; at Fort Meade it was shown that 2 g of sulfadiazine a day for 3 days caused an abrupt drop in the carrier rate from 51% in the control group to 0% in the group 3 days after the last day of therapy.
At Jefferson Barracks, a sample of 200 men selected from permanent party personnel were cultured once a week for 10 weeks. The weekly carrier rate varied between 24% and 42%, and during the period, 75% of the men were found to be carriers of meningococci at one time or another. Group A meningococci were isolated from 25.6%, group B from 46.7%, group C from 23.6%, and group D from 10.5% of the men cultured during the interval. Negative cultures were found in 50 men or 25% of the sample. Later, Drs. Phair and Schoenbach were to report an average composite prevalence rate of 40% during carrier studies of an Army Medical Service Unit. Infections with at least one type were found in 92.9% of men during the 10-week study. Most significantly, a single dose of 2 g of sulfadiazine reduced the carrier rate to 0% without toxic reactions.
Because of the early success of Drs. Heidelberger and MacLeod in demonstrating the immunizing capabilities of pneumococcal polysaccharides, Dr. Kabat, an associate of Dr. Heidelberger`s at Columbia University, undertook the purification of group A (then group I) meningococcal polysaccharide. His product gave a specific precipitin reaction with group A sera of horse, rabbit, and chicken, and reacted with convalescent sera of cases. However, the polysaccharide was not antigenic in animals and when injected into 60 humans induced low-level antibody responses in only 20%. After April 1946, other investigators were to take on the twin challenges of vaccine development and emerging sulfadiazine resistance.
At the April 26, 1945, meeting of the AFEB, Dr. Phair reported that a strain of group A meningococci had been made resistant to sulfadiazine by serial passage through fertilized eggs containing increasing concentrations of drug. Thus, the potential for the development of resistance after widespread use of sulfadiazine was anticipated. Dr. Feldman was later to test a number of group B strains from the collection of Dr. Sarah Branham made available to him by Dr. Margaret Pittman of the Bureau of Biologics of the FDA. One strain isolated in Baltimore in 1937 showed low-level resistance, whereas another obtained in 1938 in Washington was markedly resistant. By 1954, 14 (28%) of 50 strains in one collection were resistant. In the spring of 1963, sulfadiazine prophylaxis proved to be ineffective at the San Diego Naval Training Center; and the prevalent group B strains were highly resistant. As previously noted, a group B epidemic at Fort Ord the following year attracted statewide attention. Among civilian strains examined by Dr. Feldman during 1965 and 1966, approximately 50% were found to be resistant. In
65
Interagency Team Arriving in Santiago, Chile.
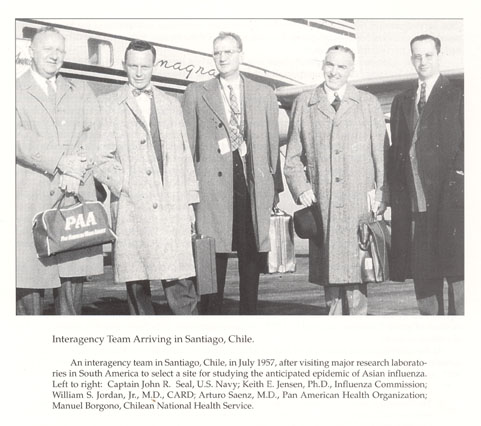{kind=link}
An interagency team in Santiago, Chile, in July 1957, after visiting major research laboratories in South America to select a site for studying the anticipated epidemic of Asian influenza. Left to right: Captain John R. Seal, U.S. Navy; Keith E. Jensen, Ph.D., Influenza Commission; William S. Jordan, Jr., M.D., CARD; Arturo Saenz, M.D., Pan American Health Organization; Manuel Borgono, Chilean National Health Service.
66
1968, investigators at NAMRU No. 7, Naples, reported the occurrence in Morocco of the first epidemic caused by sulfadiazine-resistant group A meningococci. Of the strains, 90% were resistant to 1 mg of sulfadiazine per 100 mL of serum.
A partial solution to chemoprophylaxis was found when investigators at NAMRU No. 4, Great Lakes Naval Training Station, demonstrated that 600 mg of rifampin administered orally for 4 days reduced the meningococcal carrier state by 89%,compared with a group given placebo. A similar dose was 94.7% effective in eradication of nasopharyngeal carriage in a trial among Air Force students at Lowry Air Force Base. However, as reported by Dr. Eickhoff, four rifampin-resistant strains were identified during the follow-up period. Four resistant strains also emerged after a 4-day course of therapy of recruits at Fort Lewis. Because the high rate of emergence of meningococcal strains resistant to rifampin promised to limit the usefulness of this drug for prophylaxis, as with sulfadiazine, it is fortunate that a team of scientists at WRAIR pursued the vaccine studies initiated by Kabat and Heidelberger.
In June 1969, three members of the Department of Bacteriology at WRAIR (Drs. Malcom Artenstein, Irving Goldschneider, and Emil Gotschlich) together with Dr. Teh Yung Liu of the Department of Biology at Brookhaven National Laboratories published five classic papers reporting studies previously presented to the AFEB and the Committee on Meningococcal Infection. These studies brought together evidence for the protective role of circulating bactericidal antibodies, described the preparation of purified groups A, B, and C meningococcal polysaccharides, confirmed that groups A and C polysaccharides were immunogenic in humans, and reported that intradermal injection of 50 mg of group C polysaccharide significantly reduced the acquisition of group C meningococci by recruits at Fort Dix.
Next, a 1969 trial of two lots of group C vaccine followed: one prepared by the Division of Biologics Research at WRAIR, the other by E. R. Squibb under contract. One dose of 50 mg of polysaccharide administered either by jet injector or subcutaneously by needle and syringe effected an 87% reduction in group C disease among nearly 14,000 recruits at five basic training centers. When the lot prepared by Squibb was tested in a smaller number of Marine recruits at San Diego by a team from NAMRU No. 4, no cases of group C disease occurred in 3,018 vaccinees compared with three cases in a similar number of control subjects.
At the meeting of the Board on 14 and 15 May 1970, the Committee on Meningococcal Infections submitted several recommendations that were endorsed, in modified form, by the Board on 28 May 1971, as follows:
1. The Committee desires to continue to facilitate the development and assessment of prophylactic measures and aid in the planning and execution of vaccine trials. The current use of group C polysaccharide vaccine is endorsed. Problems are anticipated in trying a group A vaccine which is now available, and a product manufactured in France is under test by the World Health Organization (WHO).
2. The Committee is concerned that there is no useful group B antigen, nor does its availability appear likely in the immediate future. The problem requires attention be given to suitable chemo- or antibiotic prophylaxis as alternatives to immuno prophylaxis for group B infections. Continued effort toward isolation of the basic antigen in the group B meningococcal is recommended.
3. It is of increasing concern that when the group C antigen is used as vaccine, meningococci belonging to groups B and Y may become important causes of disease in the military.
On 26 September 1972, the Secretary of the Army recommended that group C meningococcal vaccine be administered to all individuals entering basic combat training. The following May the AFEB recommended that group C vaccine be used on a routine, year-round basis in all Navy and Marine
Corps personnel entering training. Only minor problems were encountered in manufacturing the group A vaccine. That produced in France by Institut Merieux for the WHO proved to be effective in Africa. That produced by Merck Sharp and Dohme was shown to be safe and effective in Finnish military recruits. There is still no effective group B vaccine despite persistent efforts by investigators at WRAIR and elsewhere. As detailed below, the concern about other groups was addressed by adding antigens for groups Y and W-135 to A and C antigens to make a tetravalent vaccine.
67
With the demise of CARD and its Committee on Meningococcal Infections, responsibility for vaccines was assumed by the rechartered AFEB`s Subcommittee on Disease Control. Recommendations regarding the use of group A vaccine were developed after a meeting on 15 September 1977 at which data were reviewed relative to three topics of concern to The Surgeon General: meningococcal vaccines for military recruits, alternative therapy for penicillin-resistant gonorrhea, and the administration of live virus vaccines to female recruits. The AFEB made the following recommendations regarding protection of recruits against meningococcal disease:
That the licensed bivalent, group A and group C, meningococcal vaccine be administered to military personnel entering recruit training during those periods of the year for which epidemiological experience indicates that protection against meningococcal disease is necessary in that locality.
That the use of this vaccine should be accompanied by a program designed to identify meningococci causing disease so that a continuing evaluation of the program is possible.
By the time the first recruits received the bivalent A and C vaccine in January 1979, the question of the inclusion of antigens for groups Y and W-135 had already arisen. In 1978, 50% of military cases of meningococcal meningitis were caused by either Y or W135, stimulating scientists at WRAIR to accelerate efforts to purify specific polysaccharides for these types. Encouraging progress was reported at the AFEB meeting in June 1982. Because the Y and W-135 antigens induced levels of bactericidal antibody comparable to those produced by A and C antigens (and antibodies to the latter had been shown to be protective), the Y and W-135 antigens were accepted as efficacious without extensive field trials. Administration of tetravalent A, C, Y, and W135 vaccine was instituted in 1982. Unfortunately, group B continues to be an important cause of meningitis and no effective vaccine is available.
Control of Airborne Infections
Recruit training camps are the military counterpart of civilian day-care centers. New input of young adults from diverse geographic areas creates a population of immunologically naive subjects susceptible to each others` pathogens and to organisms (eg, adenovirus type 4) with a peculiar predilection for such settings. The more the characteristics of housing and the conditions of training facilitate the exchange of bacteria and viruses, the greater the incidence of respiratory disease. Accordingly, with the encouragement of the Committee on Sanitary Engineering of the National Research Council and the Sanitation and Hygiene Division of the Office of The Surgeon General, CABI and CARD undertook studies to determine whether it was possible to control illness by reducing the spread of airborne microbes with the use of anyone or a combination of measures: altering living and sleeping quarters; reducing dissemination of organisms into the air; and sterilizing the air with germicidal vapors.
Oiling of floors had been used in World War I, more to reduced us than to control disease. Germicidal mists had been used since the days of Lister. Dr. Robertson had studied the effectiveness of propylene glycol as an aerosol against a number of organisms. The publication of the results of this work in 1941 coincided with his appointment as the Director of CABI.
The initial CABI studies examined oiling. At Camp Carson, oiling of floors reduced the bacterial content of air in barracks by 70%,compared with similar barracks with unoiled floors. Oiling of both floors and blankets reduced the bacterial count, particularly of streptococci, by as much as 90%. At the ninth meeting of the AFEB in April 1944, it was reported that studies in 16,000 subjects showed that there were 28% fewer hospital admissions for common upper respiratory infections among soldiers housed in oiled barracks than in untreated barracks and 16% fewer admissions for streptococcal infections.
Turning to Dr. Robertson`s interest, CABI investigators showed that propylene glycol and ethylene glycol applied in small concentrations as an aerosol also resulted in reductions in the bacterial content of air in buildings. They developed a device for metering the aerosol into the air and determined that
68
ethylene glycol was preferable to propylene glycol because it was effective at lower concentrations. In five separate studies, triethylene glycol vapor introduced into the air in scarlet fever wards reduced the number of R hemolytic streptococci by 38% to 100%. Glycolization together with oiling of floors and bed clothes gave maximum reduction in bacterial content of the air, up to 95% in some circumstances.
The CABI studies were conducted under endemic conditions; the CARD studies at Fort Bragg encompassed both endemic and epidemic periods of respiratory disease. The study of the effect of oiled floors and bedding on the incidence of disease was conducted at Fort Bragg during the winter of 1944 and1945. Four battalions of approximately 1,000 men each were chosen for the study, and the men in alternate batteries (approximately 250) were housed in barracks having oiled floors and bedding. The remaining men were housed in untreated, control barracks. Oil was applied to the floors, and bedding by techniques evolved by CABI and the effectiveness of the procedure were checked by inspection and bacterial analyses of air, blanket, and floor dust. The incidence of respiratory disease was measured by hospital admissions, dispensary visits, and interviews with platoons of soldiers on active duty. Standardized criteria were established for allocation of patients to quarters or to the hospital and for clinical diagnosis of illnesses.
During the entire study, 20 batteries were observed, 10 oiled and 10controls. The air of the oiled barracks constantly yielded from 75% to 90% fewer organisms than were obtained from the air of untreated barracks. Cultures from blankets having an oil loading of 2% or more oil as dry weight grew out from 90% to 95% fewer organisms than did those from unoiled blankets. Of 307 cultures from oiled beds, 8.5% were positive for hemolytic streptococci. Of 441 samples from unoiled beds, 36.3% yielded similar streptococci. The period of observation was divided into two parts. During the first, beginning 22 October and ending 30December, the incidence of ARD was regarded as being within the usual or endemic limits. During the second period, from 31 December to 17 March, ARD were regarded as being epidemic. During the endemic period, in agreement with CABI results, there appeared to be a reduction of between 30% and 40% in the cases of ARD from the oiled group compared with the control group. During the epidemic period, however, the reduction was approximately 6% to 12%. The investigators concluded from a practical point of view that the results indicated that oiling of floors and bedding had a moderate effect in reducing ARD during a period of low endemic incidence but was ineffectual in controlling an epidemic of ARD in new recruits. Contaminated dust in barracks may be a contributing factor in the spread of the endemic illnesses, but this mode of spread appeared to be relatively unimportant during the epidemic. Hemolytic streptococcal infections and other respiratory diseases of known etiology did not occur with sufficient frequency for the effects of the oiling procedures to be evaluated. Some years later, Dr. Rammelkamp at the Streptococcal Diseases Laboratory at Warren Air Force Base showed that dust contaminated with streptococci did not induce illness when placed in the throat of a volunteer, an observation that emphasizes the importance of close personal contact.
Prior to the oiling studies at Fort Bragg, CARD investigators examined the effect of double bunking in barracks on the incidence of respiratory disease. The study was begun in October 1943, in a battalion of 1,000 men. Alternate barracks were equipped with double-decked bunks, without changing the total number of men in each barracks. The weekly incidence rates of duty and quarters cases and of hospitalized cases of influenza A and ARD from double-bunked and control groups were carefully monitored. The procedure had little, if any, effect on the incidence of duty and quarters cases or on hospitalized cases of influenza A or endemic ARD. During an epidemic of ARD in January 1944, however, the incidence of hospital cases from the double-bunked barracks was markedly lower than in the control barracks. These results indicated that double bunking may be a desirable procedure for housing troops in barracks provided that it is not used as a means of crowding larger numbers of men into the same space.
Apart from studies on the heating and ventilation of barracks conducted until1946 under non-AFEB auspices by the NRC Committee on Sanitary Engineering, no additional studies on housing were undertaken until the Laboratory on Housing and Illness opened at Sampson Air Force Base in 1954. When this base served as a Naval Training Center in 1943, it was used by the Navy and the
69
Committee on Sanitary Engineering to investigate the use of ultraviolet irradiation to sterilize air. A unit of22 barracks with 4,400 men was divided into four groups-one treated with high-intensity ultraviolet irradiation, one with low-intensity ultraviolet irradiation, and the other two serving as control groups. The training period of5 weeks allowed only short observation of any group of men; in all, some 30,000men passed through the unit between 15 December 1943 and 1 June 1944. The low-intensity ultraviolet irradiation showed little effect, but hospital admissions for respiratory infections in the high ultraviolet irradiation groups were 25% lower than in the control groups. Bacterial counts showed a reduction of about 50% in airborne organisms in the irradiated barracks compared with control barracks. It was concluded that an average reduction of cross-infection of about 18% occurred.
In summary judgment of all these studies, the minutes of the April 1944 AFEB meeting record the conclusion of the CABI that sterilization of air by ultraviolet light or glycol vapors does not appear to be practicable either in barracks or hospital wards, and the marginal benefit of oiling was judged to be insufficient to counter its objectionable features. Accordingly, the reactivated studies at Sampson Air Force Base focused on features of barracks construction that impact on contact between occupants. Two types of barracks, open bay and closed bay, were studied. The methods used and the results obtained were well described in the final report of Dr. Houser, the project Field Director.
The recruit population was divided geographically and administratively into two troops. Little close association occurred among recruits in these two troops. However, common classrooms, recreational facilities, dispensaries, and other meeting places created opportunity for close and frequent contact among the recruits within a troop. One of the troops was divided into two geographical areas: G and H. G area contained two squadrons and H area, three squadrons. The number of men per squadron varied according to the total troop strength, but at any given time the number of men in each squadron was similar as the result of rotational assignment of new recruits. Each squadron was composed of flights of 60 or 72 men (occasionally 80 men would be assigned to a flight). Each flight went through training as a unit, but transfers of men in and out of the flight because of missed training for a variety of reasons among them absence because of illness did occur. The training period was12 weeks. Each flight was housed by itself on a single floor of two-floored barracks. Double decked bunks were in use.
All barracks in G area were of the dormitory or open-bay type. The barracks in H area were identical in size and construction to those in G area except that individual rooms opening onto a central corridor had been constructed. Each room in these closed-bay barracks contained three double bunks. Because supporting pillars and clothes racks divided the open-bay barracks into units of three bunks each, the relative relationship of each man to any other in his flight was similar in the two types of barracks. The difference between the two barracks was that men in the closed bay occupied the three bunks in a closed space, whereas in the open-bay barracks men occupied three similarly located bunks in a space open to the entire barracks.
Comparison of the hospital admission rates of recruits from the two types of barracks showed no difference either in total rates for the entire training period of individual flights or in the time of training that hospital admission occurred. This was true not only during times of high rates of admission but also during interepidemic periods. When adenovirus infections, influenza B, and streptococcal infections were considered separately, no differences were observed between the two types of barracks. Maximum admission rates occurred during the 3rd and 4th weeks of training for ARD and during the 5th week for streptococcal infections. Influenza B admissions were influenced by the time of the epidemic rather than the time in training. Thus, under the conditions of training and barrack occupancy during the study, no advantage of one type of barrack over the other was apparent when hospital admissions for respiratory disease were considered.
When looking at floor space per man and cubic feet of air space per man, more crowding occurred among men occupying closed-by barracks. In an open-bay barrack, 72 men resulted in floor space of 60 ft2 and an air volume of 687 ft3 per man; the same number of men in the closed-bay barracks had 36 ft2 of floor space and 414 ft3 of air volume per man. These differences in floor space and air volume did
70
not appear important in the spread of respiratory disease under the conditions of this study. To test the effect of reducing intra room crowding by 50% while other factors in intra flight contacts remained the same, flights of men housed on two floors of barracks were compared with flights with the usual arrangement of a single floor. Such experiments in the open-bay barracks showed no differences for streptococcal and nonstreptococcal disease. However, in the closed-bay barracks streptococcal disease rates were less for the flights occupying two floors; no difference was noted in the admission rates for nonstreptococcal disease.
It was concluded that the two types of housing studied, closed bay and open bay, with differences in floor space and air volume per man, showed no difference in hospital admission rates for nonstreptococcal respiratory diseases, which were predominantly adenoviral and influenzal infections. Streptococcal disease appeared less likely to occur when the number of men per room was reduced; however, at the level of crowding normally present, the rooms did not result in a reduction of infection. Additional comparisons of the two types of housing were made in six pairs of flights. One of two flights that arrived on the base within a few days of each other was assigned to an open-bay barrack and the other was placed in a closed-bay barrack. Serum specimens were obtained every 1 or 2 weeks from each man; throat cultures were obtained two or three times per week; and direct questioning of each man in relation to respiratory symptoms was done two or three times per week. Analyses of data obtained in this manner were summarized as follows:
1. A fairly typical pattern of respiratory symptoms was present in the men of all flights. Within one or two days after arrival, coryzal symptoms were frequent and this pattern persisted for a few days. On about the tenth day, more severe symptoms began to appear. These were sore throat, cough, malaise, and feverishness. The men as a group were free of these symptoms after about the fourth week, and minor respiratory symptoms again were prominent for the remainder of training.
2. Units of five and six men occupying a single room in a closed-bay barrack were less likely to have illness introduced into the unit than were similar units in open-bay barracks, and there was a longer interval before introduction when it did occur in the closed-bay units.
3. Once illness was present in a closed-bay unit, there was no increased secondary attack rate among the men in the unit when compared to the open-bay units.
4. Although there was less risk of early acquisition of illness in the closed-bay units, the total risk during training was similar in the two types of barracks.
On the basis of these results, the investigators drafted a plan for the study of environmental conditions that influence the spread of respiratory pathogens in military populations, particularly recruit camps. Unfortunately, Sampson Air Force Base was closed, necessitating termination of the field studies. Dr. Houser`s report concluded with a summary of the research plan and brief protocols for three specific studies. The important factors to be considered were as follows:
1. Bed spacing or crowding;
2. Size of the population occupying a common living or dormitory area;
3. Communal gathering places within the barracks such as latrine and dayroom;
4. Presence or absence of barriers to limit person-to-person contact or to reduce droplet and droplet nuclei spread;
5. Sources of infection outside the barracks; and
6. Inanimate objects as intermediate sources of infection within barracks.
In addition to the above, certain basic factors in the epidemiology of respiratory disease were to be evaluated. These were the following:
1. The effect of environment - heat, humidity, ventilation - on the susceptible individual, on the infectious agent, and on the human source of infection;
71
2. Characteristics of the human source of infection;
3. Characteristics of the susceptible individual; and
4. Characteristics of the infectious agent.
The three protocols were for investigations of the following factors:
1. The effect of crowding on the spread of respiratory disease.
2. The influence on the spread of respiratory disease of reduced barrack contact between men by the use of rooms and cubicles.
3. The effect of distance between beds and duration of exposure on the spread of respiratory disease.
Details are available in Dr. Houser`s report. The issue of housing is still lively, as emphasized by the recent study by WRAIR investigators, who reported that the rates off ebrile ARD were significantly higher among trainees in modern (energy-efficient design and construction) barracks than in old bar racks. These results led to "the hypothesis that tight buildings with closed ventilation systems significantly increase risks of respiratory-transmitted infection among congregated, immunologically susceptible occupants."
Coccidioidomycosis
In 1944, CARD investigators assisted in studies of an outbreak of pulmonary disease that occurred in men who had spent time in an abandoned storm cellar on the military reservation at Camp Gruber, Oklahoma. Although etiologic studies failed to identify a causative agent at the time, the disease was later shown to have been histoplasmosis. Shortly thereafter, the CARD was to inherit from the Commission on Epidemiological Survey (CES) another mycotic infection (coccidioidomycosis) and Dr. Smith of California, who had contributed much to knowledge of the epidemiology of that infection, known locally as "California disease" or "San Joaquin Valley Fever."
Dr. Smith had trained in the laboratory of Dr. E. C. Dickson, a pioneer student of the fungus Coccidioides immitis at Stanford University School of Medicine, then located in San Francisco. The studies of Dr. Smith in the late 1930s had contributed to the recognition that the disease was frequently benign and that a high rate of infection occurred among newcomers to endemic areas. In 1940 and 1941, many newcomers arrived in he San Joaquin Valley when the Army Air Forces began construction of airfields for a year-round aviation training program. When the hazard posed to military personnel was called to the attention of the commanding officer of the West Coast Training Center, and in turn to the AFEB and the CES, a plan was developed for a study of coccidioidomycosis, including research into its epidemiology. This plan, approved by the AFEB in June 1941, called for the study to be centered in Dr. Smith`s laboratory in the Stanford University Department of Public Health and Preventive Medicine. He was assisted by Dr. Rodney R. Beard, then a member of that department (Dr. Beard subsequently became Director of the Commission on Environmental Hygiene and Chairman of the Department of Preventive Medicine at the new medical facilities at Stanford University in Palo Alto).
In collaboration with the Western Flying Training Command and Army Ground Forces, Drs. Smith and Beard and their associates arranged to skin test all new arrivals at Gardner, Lemoore, Merced, and Minter airfields and other bases in Southern California with coccidioid in. At Gardner Field, "dust was ankle deep and swirled in clouds over the fields." At Minter Field, 20% of all susceptible individuals were infected during the summer and fall of 1941. At the fourth meeting of the AFEB in November 1941, Dr. Smith reported that more than 2,000 men in the Ninth Service Command had been tested with coccidioid in. Men from the east and midwest were all negative; a few from western Texas, New Mexico, Arizona, and, of course, the San Joaquin Valley reacted. All soldiers with lesions of erythema nodosum at Camp Roberts were coccidioidin positive. Every 6 months, personnel previously coccidioid in negative were retested.
72
The same procedures were extended in 1943 to the California-Arizona maneuver area (the desert area of southeastern California and western Arizona) when a problem was recognized there. It was later concluded that southern and central Arizona were the most highly infected areas in the United States. In time, skin testing was extended to additional bases in California and Arizona, including a camp for prisoners of war in Florence, Arizona, where all tubercular prisoners of war were hospitalized at the Station Hospital. Ten tubercular prisoners were found to have been infected while hospitalized. Although the superimposed coccidioidal infections did not appear to affect the tuberculous infections adversely, the decision was made by authorities in Washington to transfer the prisoners to other hospitals to avoid any criticism of violation of policies governing hospitalization of prisoners of war.
Dr. Smith insisted that coccidioid in skin testing be coupled with accurate records. He required that all personnel previously coccidioid in negative who converted to positive at retest be recorded on standard "clinicoepidemiologic" forms and that blood be drawn from them for serologic tests. The results provided useful data regarding pathogenesis and prognosis. Of those infected,60% were asymptomatic; only 25% manifested sufficient clinical symptoms to be diagnosed. Erythema nodosum occurred in 24% of infected white females, in 4.3%of infected white males, but rarely in blacks. Dissemination occurred in approximately 1% of clinically manifest infections in white males and in 0.25%of all their infections. Disseminated infections occurred over 10 times as frequently in blacks, the most dangerous form being meningitis. Residual pulmonary cavitation, usually benign, occurred in 2% to 6% of subjects.
Coccidioid in, an antigen prepared from the mycelial phase of the fungus, was produced in Dr. Smith`s laboratory and distributed as a service of the CES. The first test site near Bakersfield was a "large tent equipped with an electric hot plate and an empty vegetable can for a sterilizer" and served as the dispensary; coccidioid in was then distributed to bases throughout the west, to Europe, North Africa, India, Australia, China, the Philippines, and South America. This eventually led to the detection of two new arid endemic areas: Lara, Venezuela, and Paraguayan Chaco. Dr. Smith has been credited with proposing that histoplasmosis might account for pulmonary calcifications in coccidioidin- and tuberculin-negative subjects and with suggesting to Dr. Carroll Palmer of the Public Health Service that the histoplasmin skin test be used to define endemic areas of histoplasmosis. He continued to provide coccidioidin to the armed forces after the war on behalf of CARD and each year made a point of reporting that the commercial value of the antigen distributed exceeded the cost of his contract by at least tenfold.
Coccidioidin is a weak immunogen, so repeated skin testing did not induce humoral antibodies. Disease did, and these antibodies were measured in simultaneous precipitin and quantitative complement fixation (CF) tests in Dr. Smith`s laboratory as another service function of the CES. Dr. Smith noted that the precipitin test was more useful early in the course of infection while the complement fixation test was more useful later, an observation subsequently explained by the demonstration that the former measures serum immunoglobulin M (IgM)and the latter measures serum immunoglobulin G (IgG) antibodies. Dr. Smith`s analysis of his meticulous records showed that the titer of complement fixation increased with the severity of infection. Less than one in 40 of patients with nondissemination disease had CF titers in excess of 1:16, whereas more than 50%of patients with disseminated disease and 95% of those with fatal lesions exceeded that level. The Stanford laboratory continued to function as a reference laboratory for all three services, performing over 100 tests per week until the 1960s. By this time, Dr. Smith had monitored the response of patients treated with intravenous amphotericin B and could report that 69% of 68 patients with nonmeningeal dissemination had favorable results. Improvement occurred more often (88%) in those who underwent a fourfold reduction in CF titer than in those who did not. The initial results in patients with meningitis were less encouraging; only 5 of 47 patients had a complete remission.
As for control measures, it was clear that the infection was acquired from soil containing the anthroconidia (spores) of the mycelial phase. Smith could attest to this from personal experience. His wife was infected by contact with his clothing after he transported highly infectious dirt from San
73
{kind=link}
Dr. Charles E. Smith was Professor of Preventive Medicine, Stanford University School of Medicine at San Francisco and subsequently Dean, School of Public Health, University of California at Berkley. He used the coccidioidin skin test to identify endemic areas of coccidioidomycosis that should be avoided during training exercises or where dust control was essential to prevention. He served as a member of both the CARD and the AFEB.
74
Benito. On the other hand, patients harboring spherules and endopores were not contagious. Appreciating the need to control dust at installations in endemic areas, at its annual meeting in 1944, the AFEB requested the CES to determine what more could be done. Before this, local dust control measures consisted of establishing grass areas and the construction of surfaced roads. A decision was made to try oiling areas without turf, such as playing fields and training grounds, where asphalt was not satisfactory. Highly refined oils were effective when applied to heavy, adobe-type soil butin effective when the soil was fine, loose silt. The most effective way to prevent infection was to avoid new construction and the holding of maneuvers in endemic areas.
Dr. Smith`s personal experience also gave him a great respect for the hazard of the laboratory. In the period between 1929 and 1945, the Dickerson/Smith laboratory was judged to be the source of about 20 infections with Coccidioides. When two visitors, including Dr. Smith`s son, were infected, culturing was restricted to a separate locked room. In 1946,infection of four monkeys one floor above the laboratory and in four individuals on all three floors of the building revealed contamination of the exhaust ventilating system. The ventilation louver of the transfer room was closed. Two infections in 1947 and an epidemic of five individuals in 1948 occurring on all three floors led to the discovery that the ventilating inlet louver was incompletely closed. The louver was sealed and a closed transfer chamber constructed. However, in 1949, as later reported to the AFEB, Dr. Smith discovered that his laboratory was still hazardous. Just after he had transferred stock cultures of C. immitis using all precautions, including the transfer chamber and chemical decontamination, "the natural air currents and ventilating system distributed the spores like the wind and dust storms of the endemic areas" throughout the medical school building.
Thirteen medical students, instructors, laboratory, and clerical personnel became ill, 12 two floors above on the third floor and 1 on the first floor. Asa result, Dr. Smith ceased handling any cultures on solid media. In 1950, he arranged to have the preparation of coccidioidin switched to facilities at Cutter Laboratories.
Drs. Smith and Pappagianis, now located at the School of Public Health in Berkeley, in collaboration with investigators of the Naval Biological Laboratory, also in Berkeley, and Dr. H. S. Lawrence of New York University (CSSD)continued studies of the immunological properties of coccidioidin. They found that repeated intradermal testing of negative reactors with coccidioidin alone did not ordinarily induce delayed sensitivity to the antigen. However, repeated intradermal testing of reactors with weak or latent sensitivity may effect ananamnestic delayed reactivity. Healthy subjects living in an area endemic forcoccidioidomycosis may exhibit a delayed allergy to coccidioidin in the absence of detectable serum complement-fixing antibody, and occasionally, serum antibody may be present in such subjects without delayed allergy to coccidioidin. They concluded that these findings suggest that the delayed type of allergic inflammatory response to coccidioidin need not necessarily be correlated with the presence or absence of serum antibody, an expression of another parallelism between fungal hypersensitivity and bacterial allergy of the tuberculin type.
In pursuit of the parallel with tuberculin allergy, the investigators found that generalized delayed sensitivity to coccidioidin can be transferred in human subjects with deoxyribonuclease (DNase)-treated leukocyte extracts obtained from sensitive donors. Attempts to transfer coccidioidin sensitivity with leukocyte extracts obtained from a negative donor were unsuccessful in eight of nine consecutive trials. Sensitivity to coccidioidin after transfer persisted up to15 months, in the absence of exposure to Cimmitis or repeated skin testing. Thus, the results of transfer of coccidioidin sensitivityb y this means paralleled those obtained in humans after the transfer of bacterial hypersensitivity with the use of extracts of specifically sensitive donor leukocyte extracts said by Dr. Lawrence to contain the elusive substance called "transfer factor."
Dr. Smith also collaborated with investigators at the National Biological Laboratory to test the efficacy of killed spherule vaccines in monkeys and mice. Multiple subcutaneous doses protected monkeys against progression of disease, but not infection, after respiratory challenge with arthrospores. Mice immunized intramuscularly showed an intranasal LD50of >3,000 arthrospores compared with approximately 50 in control animals. Vaccines prepared from mature spherules were superior to those prepared from immature spherules, consistent with the postulate that the mature cell wall is the primary locus of the immunogen. In continuation of these studies after his move to the University of
75
California School of Medicine at Davis, Dr. Pappagianis has attempted to identify subcellular components that confer protection. Purified antigens are desirable, for the spherule vaccine is moderately toxic. Furthermore, three doses of a killed spherule vaccine were shown to be ineffective in a trial conducted between 1980 and 1985 in 2,867skin-test-negative volunteers in California and Arizona.
Tuberculosis
The armed forces of the United States benefited greatly from the steady decline in the incidence of tuberculosis that occurred in the first half of the20th century in populations of industrial countries. Fewer and fewer recruits were exposed to tuberculosis in the United States before induction. However, rates did not decline as fast in the developing world, and recruits from these areas, particularly the Philippines, were at greater risk of prior infection and the subsequent development of active disease. Screening of recruits eliminated those with pulmonary lesions detectable by radiograph, but endogenous disease often did not become manifest until after months of service. Furthermore, personnel free of infection on entry as indicated by a negative tuberculin ran the risk of being infected in areas of the world where rates were high in the local population. The management of those who did become infected was markedly improved by the timely arrival of effective drugs; first, streptomyc in for therapy; then, isoniazid for both therapy and chemoprophylaxis.
CARD did not sponsor any research projects related to tuberculosis but was called on from time to time for advice on the various aspects of the problems outlined above. Most of the questions directed to the AFEB came in themid-1960s, stimulated particularly by the occurrence of epidemics traced by the Navy to dissemination of organisms aboard ship. One such outbreak had occurred on the destroyer U.S. S. Long beach in 1959. In August 1962, the Navy requested that the AFEB provide guidance regarding the use of baccillus Calmette-Gu?rin (BCG), a request stimulated in part by two strong proponents of BCG at Duke University, Dr. D. T. Smith, Professor of Microbiology and Chairman of the Department of Preventive Medicine, and Dr. Wilbert C. Davison, Professor of Pediatrics and founding dean. These colleagues had recommended to The Surgeon General and to members of Congress that BCG be given to all tuberculin-negative members of the armed forces. To address this recommendation and other concerns, CARD created a Committee on Tuberculosis in 1964, chaired by Dr. Gardner Middlebrook. Dr. Middlebrook had worked with Dr. Rene Dubose at the Rockefeller Institute to develop an improved medium for the growth of tubercle bacilli. He then moved to the National Jewish Hospital in Denver and later to the School of Medicine of the University of Maryland. Other members of the committee included Dr. Palmer, Public Health Service, Dr. James Hirsch, Rockefeller Institute, Dr. Arthur B. Robins, New York City Department of Health, and Dr. Elmer Becker, WRAIR.
The Committee on Tuberculosis recommended that BCG not be used by the military, emphasizing the value of the tuberculin skin test for detecting converters who can then be treated with isoniazid. Among other recommendations endorsed by the AFEB were that tuberculin-positive Filipino recruits be studied to determine the usefulness of isoniazid in preventing active disease and that more studies be made by the services to determine the conversion rates of personnel serving in potentially high-risk environments overseas.
The AFEB`s position on choosing to not use BCG was reaffirmed in 1969, when a recommendation for its use was again made, after additional outbreaks on three ships, to Dr. Louis M. Rousselot, Deputy Assistant Secretary(Health and Medical) by the Research Foundation of Chicago, the producer of Dr. Sol Ray Rosenthal`s BCG vaccine.
Q Fever
The last of the respiratory diseases to be considered by this review Q fever was an important airborne, especially dust-borne, cause of illness in the Mediterranean theater, and cultivation of the
76
causative rickettsial agent, Coxiellaburnetii proved to be far more hazardous than cultivation of C. immitis. Unknown to allied physicians at the time, Q fever existed outside of Australia. It was endemic in Bulgaria and Greece where German troops affected in 1943 referred to it as "Balkan grippe." Using blood from patients involved in an epidemic of "unusual" influenza in Athens in the winter of 1944, Dr. A. J. Caminopetros of the Pasteur Institute of Greece had established a febrile illness in guinea pigs readily transmitted by inoculation of infected blood.
In January 1945, an epidemic of 40 cases of pneumonitis occurred in one company of a battalion of British paratroopers who had come to Rome, Italy, from Athens. The men recalled exposure to dust in an abandoned silk mill used as abivouac. The initial description of this outbreak as one of "atypical pneumonia" was responsible for the first involvement of CARD. Dr. Dingle, Director, joined Lieutenant Colonel Gauld and Major Robbins of the 15th Medical General Laboratory in Naples to investigate the epidemic at the request of Brigadier E. R. Boland, Royal Army Medical Corps. Dr. Robbins (who subsequently shared a Nobel prize with Drs. John Enders and Thomas Weller for the growth of poliovirus in cell culture) was soon called on to assist in the study of a series of an outbreaks in Italy. Patients from two of these were seen at the15th Field Hospital, a medical evacuation unit located behind the U.S. II Corps in the Apennines North of Florence. Dr. Charles A. Ragan, Jr. (later, Professor of Medicine at Columbia University College of Physician and Surgeons) was Chiefo f the Medical Service.
Within 3 months after it was set up in December 1944, the 15th Field Hospital admitted 33 members of the Headquarters company, 339th Infantry, with febrile illnesses, and 20 additional patients from the same unit were seen in other 5thU.S. Army hospitals with similar symptoms. From the blood of one of the patients with pneumonitis a strain of Rickettsia characterized as Rickettsia burnetii laterrenamed Coxiella burnetii was isolated by inoculation into guinea pigs and subsequent transfer to chick embryoyolk sac (Henzerling strain). All convalescent sera from 53 patients contained complement-fixing antibodies to this strain.
A second outbreak occurred in April 1945, involving 269 members of the 3rdBattalion of the 362nd Infantry, 80 of whom were admitted to the 15th Field Hospital. The 900 men of the 3rd Battalion had been billeted in tents in the mountains north of Florence for rest and recuperation and attended training and recreational films in a dusty barn used as a makeshift cinema. No attempt was made to recover rickettsia from the dust. No specific rickettsial arthropod vectors were identified. High complement-fixing antibody titers to the Henzerlings train were found in civilians from the epidemic area. No person-to-person spread was recorded. Thus, a good case existed for dust-borne infection, to which the occurrence of 20 cases in personnel of the 15th medical laboratory lent strong support.
The disease contracted in the laboratory appeared to be somewhat more severe than that seen in the field; otherwise, the clinical picture in all outbreaks was similar. The men complained of headache, feverishness, and often pleuritic pain. Upper respiratory symptoms and signs were rare. Roentgeno grams of the chest showed patchy consolidation in almost all of the cases. The temperature ranged between 103? and 105? F and dropped by lysis, becoming normal in a week. Complications were not frequent, and convalescence was rapid. When sera from some of the patients were also tested with antigen prepared at the NIH from the rickettsiae of Q fever, they were found to contain complement-fixing antibodies, confirming the results obtained in Italy. The next involvement of CARD came on 1 June 1945, when it began an investigation of an outbreak of atypical pneumonia in the 717th Bomb Squadron, which had just returned to the United States from Italy. The transport WestPoint had debarked approximately 7,000 troops on 24 May, including the 379 men of the 717th Bomb Squadron. Seventeen cases of respiratory disease were admitted to the Station Hospital at Camp Patrick Henry, Virginia, from the Squadron on its arrival, and 38 on the following day. From 5 to 14 per day were admitted during the succeeding 5 days. Routine temperature and roentgenographic surveys helped to find more cases, 90% of whom had pulmonary infiltration. A total of 143 cases were hospitalized, constituting an attack rate of 38%. The men presented a rather uniform clinical picture, corresponding for the most part with that noted in Italy. A different feature was that many of the men complained of malaise and especially of nuchal aching. The white count was normal; the sedimentation rate was elevated. The fever was associated with only a slight increase in pulse rate. The most typical physical findings were
77
fine rales, usually heard at the end of inspiration and sometimes not elicited except on deep breathing or after coughing. No associated rash or splenomegaly was noted. Cough and chest soreness were infrequent. The roentgeno graphic lesions were widespread, irregularly distributed, and frequently peripheral. The patients recovered rapidly and usually experienced no post febrile asthenia. The uniform occurrence of the syndrome suggested that the disease was not primary atypical pneumonia but a separate entity.
Epidemiological studies were directed toward an elucidation of the place and time of infection and the manner and mode of transmission. The 717th Bomb Squadron was stationed for 17 months at Grotagile, near Taranto, Italy, along with the 716th, 718th, and 719th Bomb Squadrons, which together formed the 449th Bomb Group. Small service units also were present at the base. Operations at the base ceased approximately 1 May 1945, and on 13 May, the 717th moved as a unit to the Bagnoli staging area near Naples. On 15 May, this unit embarked and 9 days later arrived at Hampton Roads. The 716th, 718th, and 719th Squadrons departed at about the same time but staged at Taranto and were brought by a different ship to Boston.
The first case of illness in the 717th occurred two days after embarkation. The onset in 35 cases developed prior to the arrival of the WestPoint in the United States. The peak of the epidemic was at the time of arrival, and new cases continued through 6 June, 12 days after arrival. The absence of cases among other units aboard the transport strongly suggested that infection occurred before 13 May, when the Squadron staged at Bagnoli, because from then on constant intermingling with other organizations occurred. The explosiveness of the outbreak suggested a common source of infection or an exposure during a period of a few days to some common vector.
For this reason the hospital records at the Station Hospital, Camp Miles Standish, Massachusetts, were reviewed to determine the incidence and character of respiratory disease in the 716th, 718th, and 719th Bomb Squadrons, and Headquarters of the 449th Group. A total of 31 men from these organizations had been hospitalized, one of whom was diagnosed as having bronchopneumonia, one as lobar pneumonia of undetermined cause, one as acute gastroenteritis, and the rest as nasopharyngitis. Onsets of illness ranged from 20 to 22 May. Rales were reported in three cases, in two of which radiographic films of the chest were obtained; both showed pulmonary infiltration having the same characteristics observed in the patients from the717th Bomb Squadron. Additional evidence of the occurrence of illness in the 716th, 718th, and 719th Squadrons was gathered at the time of the rendezvous of the 449th Group for redeployment. A questionnaire revealed that each of the squadrons had experienced an epidemic of acute illness, the cases being clearly concentrated between 17 May and 3 June. Little question existed that the infections were acquired at Grotaglie; therefore, the incubation period was in the range of 10 to 20 days or longer. The source of the epidemic and its mode of spread were never clearly established.
Attempts to isolate rickettsiae from case subjects in the 717th Bomb Squadron were unsuccessful. Blood taken during fever was inoculated into chick embryos intravenously and into the yolk sac, into guinea pigs intraperitoneally and intramuscularly, and into mice intraperitoneally and intracerebrally. Blind passage yielded no agent. Therefore, two human volunteers and three baby chimpanzees were inoculated intramuscularly and intradermally; none developed fever or pulmonary infiltration, and no reactions were noted at the sites of inoculation. However, serologic identification of the outbreak was accomplished when it was shown that sera taken from patients during convalescence fixed complement in the presence of antigen prepared from Q fever rickettsiae and also contained agglutinins for an antigen prepared from the rickettsiae of Balkan grippe.
The Balkan grippe antigen was prepared at Fort Bragg from infected guinea pig blood transmitted from Dr. Camin petros in Athens via Major C. J. D. Zarafonetis of the USA Typhus Commission. Just when Dr. Zarafonet is picked up the tube of blood is not known. Dr. Woodward, also a member of the Typhus Commission, has reported that the tube was taken to Cairo and kept there for several days without refrigeration before being sent to General Bayne-Jones in The Surgeon General`s Office in Washington. After several days on the General`s desk, again without refrigeration, it was sent to the CARD laboratory in May 1945. The rickettsia in the tube were viable!
78
After Dr. Caminopetros` procedure, the agent was first established in guinea pigs. After 12 serial passages, the agent killed intraperitoneally inoculated guinea pigs at a dilution of 10-5. Some animals inoculated with lower dilutions died within 2 days. No characteristic gross pathological changes were found in infected guinea pigs. Recovered guinea pigs were not susceptible tore infection. The agent in plasma was able to be filtered through sintered glass filters that held back bacteria and grew in the yolk sac of embryonated hen`s eggs, killing the embryos in 4 to 6 days after inoculation. Impression smears of yolk sac stained with Macchiavello, Castaneda, or Giemsa stains showed minute pleomorphic organisms, sometimes in very large numbers. They varied in shape from rod like or even filamentous forms, to coccoid forms that were often difficult to see. Intracytoplasmic masses of organisms occurred in the enlarged spleens and livers of mice inoculated intracerebrally or intraperitoneally.
The antigen used in agglutination tests was prepared from infected yolk sacs. An ether-extracted, formalinized suspension of the ground yolk sacs was put through several cycles of low- and high-speed centrifugation and was made up in saline. Large numbers of rickettsiae were present in smears made from the antigen. Serum dilutions were made with 5% sodium chloride solution. The agglutination tests were incubated at 48?C for 3 hours, followed by 18 hours at4?C, before reading. The antigen was agglutinated in the presence of sera from recovered guinea pigs but not by sera from normal guinea pigs. Sera from many of the cases of atypical pneumonia in the British parachute troops studied by Drs. Gauld, Dingle, and Robbins also agglutinated the antigen, and as has been mentioned, sera from the 717th Bomb Squadron contained agglutinins. Sera from well persons and from 20 cases of undifferentiated respiratory disease at Fort Bragg had no agglutinins for the Balkan grippe antigen.
One of those who carried out the above procedures was Dr. Irving Gordon, then a young virologist, who has recalled the "thrill" he got "when Balkan grippe specimens, acquired after our troops took Greece, grew out rickettsiae detectable in Macchiavello stains of yolk sacs." Not so thrilling was the fact that Gordon became case no. 7 in a protracted laboratory outbreak of Q fever that involved 15 (31%) of 49 CARD employees and 1 visitor with onsets of illness between 30 July and 22 December 1945.
The first case occurred in a male technician about 3 months after work began with the agent at Fort Bragg. He used no precautions while autopsying infected animals and working with eggs. The number of eggs processed had increased in mid-July, with eggs being harvested every 3 to 7 days. The preparation of antigen from pooled yolk sacs included grinding and certification. Two other cases followed, with onsets on 10 and 15 August, after which all infected animals were killed and strict precautions introduced. The precautions were not strict enough, for cases continued to occur in individuals who were recorded as not having worn masks. One case occurred in a colonel who insisted on inspecting the laboratory. One of the last cases, no. 15, occurred in a secretary (Betsy Smith) who worked in the separate office building but had stood in the doorway of the animal room on several occasions. She experienced a severe illness followed by a relapse associated with infectious mononucleosis. As Mrs. William Ogletree living in Baltimore, she recalled white-coated attending physicians huddled in conversation in her hospital room and hearing one of them express concern that she might die. Fortunately, no one did. Not only did Dr. Gordon survive Q fever, he experienced an episode of influenza with pneumonitis and an attack of atypical pneumonia during his tour, all without reactivation of the tuberculosis that had interrupted his training just a few years before.
One other individual who worked in the office building and occasionally entered the serology laboratory became ill. This was Dr. Badger, the group`s biostatistician, who became case no. 11, much to his dismay. Thus, of 15 office workers, 2 (13%) became infected. Of the 34 laboratory workers, 13 (38%) became infected. The evidence pointed to the airborne route as the means of transmission. An agent that induced fever in guinea pigs was isolated from the blood of five of six patients studied during the acute phase of illness and from pleural fluid of the patient whose blood was negative. All of these guinea pigs developed agglutinins for the Balkan grippe strain, as did all 16 of the patients. None of the 31 members of the laboratory staff who remained well developed agglutinins.
After additional studies, including those by Dr. Norman H. Topping and his associates at the National Microbiological Laboratory, NIH, it was agreed that the Balkan grippe rickettsia was identical with the rickettsia of Australian Q fever, then known as R. burnetii. Within the year after the laboratory
79
outbreak at Fort Bragg, the NIH investigators in Bethesda, Maryland, experienced an explosive epidemic of 18 cases in February 1946, with the total number of cases reaching 47 by 31 May. Many of these cases occurred in employees in the same building who did not work directly with the agent. In contrast to the Fort Bragg cases, pneumonitis occurred in only 13 of the 45 patients studied; many of the other illnesses were mild. Penicillin, sulfadiazine, and transfusions of immune blood had no definite effect on the course of the disease. When antigens prepared from American and Italian strains of Rickettsia were compared, the highest serum titers were obtained with the "Italian Q antigen." Subsequently, the organism of Q fever was named Coxiellaburnetii in recognition of Dr. Harold R. Cox of the NIH Rocky Mountain Laboratory, who reported the isolation of the agent (called R. diaporica at the time) from ticks in 1938 while studying Rocky Mountain Spotted Fever.
A few years after the two laboratory outbreaks, the occurrence of Q fever in California established the importance of airborne spread in nature. In California, which did not require the pasteurization of milk, C. burnetii was shed in the milk of infected cattle, sheep, and goats, but the use of raw milk failed to account for many human cases. Dr. Lennette, who was to serve as a President of the AFEB, and his associates recovered C. burnetii from the dust-laden air of a dairy, sheep ranch, and goatery in California and proposed that many infections arose from the contaminated environment. Although not established then, it is probable that this was true of the epidemics in the Balkans and Italy during World War II.
Concurrent with the studies in California and for 15 years thereafter, experience at the Army Biological Laboratories, Fort Detrick, Frederick, Maryland, (now U.S. Army Medical Research Institute of Infectious Diseases [USAMRIID])emphasized the hazard of the laboratory. Fifty cases of Q fever occurred therebetween 1950 and 1965, only five of which resulted from known laboratory accidents. Sixteen others occurred in others working with rickettsiae who had no recognized accidents; 28 occurred in other employees, including many without known exposure. Immunization with the then-available vaccine (Formalin-killed rickettsial suspensions) did not prevent the disease nor obscure serologic diagnosis.
Since then, progress has been made in both treatment and prevention. Administration of tetracycline or chloramphenicol shortens the duration but is not as dramatically effective as with the other rickettsioses. Amore effective phase-1 vaccine is available for use in laboratory workers but must be administered only to those who skin-test negative to avoid adverse reactions. Investigators at both NIH and USAMRIID are seeking to develop an improved vaccine. None is yet available commercially; the inactivated whole-cellphase-1 vaccine can be obtained from USAMRIID.
OTHER DISEASES
Pretibial (Fort Bragg ) Fever
In the months just before CARD was activated and its laboratory established a t Fort Bragg, that base found its name attached to an acute febrile illness characterized by a bilaterally symmetrical rash located primarily on the anterior areas of the legs. Colonel Worth B. Daniels and H. A. Grennan called the disease "pretibial fever" when their first clinical description was published the following year, but Colonel Daniels chose "Fort Bragg Fever" as the title for his splendid chapter on the subject published by the Historical Unit, U.S. Army Medical Service 20 years later. Recent texts area bout equally divided or use the combination title above. Now that the etiology is known, at least one text recommends that all old names be dropped. It has seemed appropriate to use both in this historical account.
Between 29 July and 11 September 1942, 40 soldiers from a group quartered in the same area of the reservation were hospitalized at Fort Bragg. Colonel Daniels described the illness as follows:
80
The history was one of relatively sudden onset characterized by malaise, mild general aching, lumbar pain, severe frontal headaches, and postorbital pain. On the first or second day of symptoms, mild respiratory manifestations consisting of coryza, sore throat, pain and soreness in the chest, and cough occurred in 30 percent of the patients. The respiratory symptoms were not persistent and were never suggestive of primary respiratory involvement.... In about one-fourth of the cases, nausea and vomiting occurred, rarely accompanied by abdominal pain. Shaking chills or chilliness and fever developed. The fever was consistently spiking and frequently showed two or more peaks each day. Recurrent chills often accompanied the elevations. During the periods of temperature elevation, severe accentuation of the frontal and postorbital aching was experienced, but during the periods of lower temperature, the patients felt relatively well. The fever persisted for 2 to 8 days? averaging 5.4 days? with maximum elevations ranging from 99.8 to 105.6?F. In five patients, a transient elevation of temperatures, sometimes as high as 101.4?F, occurred from 2 to 7 days after the original febrile period. Stiffness of the neck accompanied headache in three patients, but examination of the cerebrospinal fluid revealed it to be normal: there was no noticeable relief of headache following lumbar puncture. Adenopathy was not remarkable. A firm spleen was palpable early in the disease in 95 percent of the patients. Splenomegaly persisted in some patients for as little as 5 days; in others, there was still noticeable enlargement after 2 weeks.
The most distinctive feature of the disease, however, was the appearance of an unusual rash on or about the fourth day of illness. In 60 percent (24) of the patients, this was bilaterally symmetrical and limited in distribution to the pretibial areas; in an additional 20 percent (8 patients), the pretibial areas were the primary site of the rash, and a few lesions were scattered elsewhere. Two patients had splotchy, generalized cutaneous manifestations including the anterior surface of both legs. One had a single lesion on the hand. In five cases, typical in all other respects, no rash was observed. Individual lesions consisted of an erythematous localized blush of irregular outline with ill-defined borders fading into the surrounding skin. These were often from 2 to 5 cm in their largest diameter, gradually coalescing with adjacent lesions. The lesions were raised, warmer than the surrounding skin, and sometimes slightly tender to touch. In some patients, the lesions vaguely resembled erythemanodosum. In two patients, the rash became diffusely distributed over the entire body, and in a few it appeared urticarial. Following the generalized type of rash, there was a residual pigmentation which persisted for about 2 weeks. None of the lesions were purpuric. In most instances, the cutaneous manifestations lasted 2 days, but they persisted longer in a few patients....
Leukopenia was noted sufficiently often to constitute a typical feature; it was present, in all except five patients, at some time during the acute illness. It developed most often between the third and the fifth day of illness. At the termination of the febrile period, the leukocytes again rose to normal, and in 14 patients a slight leukocytosis occurred.
The men were housed near a small stream and its tributaries. Some, but not all of the patients, had been swimming in several ponds, particularly McFadgen`s Pond, but no other local environmental factors were apparent. Ticks or other insect vectors were not incriminated. Because a search of the literature did not reveal a description of a similar clinical entity, here was a new disease presumably caused by an unknown infectious, but not contagious, agent acquired by unknown means.
This resulted in the formation of a three-man "Commission for the Study of an Unidentified Disease at Fort Bragg, NC" composed of Dr. Topping (National Microbiological Institute, NIH), Dr. John R. Paul (Director, Commission on Neutropic Virus Diseases, and Professor of Preventive Medicine at Yale University School of Medicine), and Major Cornelius B. Philip, SnC. They arrived on 2 September, reviewed the records, examined patients still in the hospital, and agreed that the illness was unknown to them. A survey of illness records in one of the involved regiments indicated that a number of febrile illnesses had not been classified as this new entity because no rash was apparent. Data on the movement of personnel suggested that the incubation period was 10 to 15 days or longer. Entomological observations provided no useful clues. A long list of possible diagnoses was considered; from available accounts, the correct diagnosis was not on the list. Blood was collected from acutely ill patients and frozen for transportation to the institutions of the ad hoc Commission members. All attempts to transmit the disease to a variety of animals, including humans, failed.
81
In the summer of 1943, another outbreak of a clinically identical disease ccurred at Fort Bragg. Lieutenant Tatlock, who had reported for duty with CARD on 1 July, collected blood from the last case of that year`s outbreak and injected approximately 5mL into each of five guinea pigs. After incubation periods of 3 to 5 days, three of these guinea pigs became febrile. After a few passages, the agent became lethal for guinea pigs, appearing predominantly intracytoplasmic in impression smears of the spleen. The organisms appeared as small pleomorphic bacillary forms, staining red by the Machiavello method and gram negative. They were larger than the known rickettsiae, as well as Francisella tularensis and Brucella, and were immunologically distinct from them. They grew fairly well in the yolk sac of the fertile hens egg but could not be cultivated on artificial media.
Recovered guinea pigs were found to be immune, with elevated levels of complement-fixing antibody to yolk sac antigen, but it was not possible to demonstrate complement-fixing or agglutinating antibodies in human sera. Dr. Tatlock reported the isolation of the agent, termed it "rickettsia-like "for descriptive purposes, and carefully pointed out that its origin was in doubt. In the light of Dr. Tatlock`s studies with another agent the following year, it was assumed that the "rickettsia-like" organisms had been latent in guinea pigs, and the matter rested for 35 years until the discovery of the true nature of the bacterium was to again cause confusion.
During July, August, and early September of 1944, there appeared for the third consecutive year at Fort Bragg a small epidemic (30 to 40 cases) of the disease. These cases occurred in the same limited areas of the post as during the preceding 2 years. From the freshly drawn blood of one of these patients, Dr. Tatlock, now a Captain, isolated a filterable pathogenic agent in guinea pigs that was different from the organism isolated the preceding year. The agent failed to grow on ordinary bacteriologic media either aerobically or anaerobically. It was filterable through a Corning fritted glass filter but failed to pass a single Seitz pad. It was inactivated by freezing, and no method of preserving in an infectious state was found other than serial passage of blood in guinea pigs. After intraperitoneal or intracerebral inoculation, an asymptomatic, febrile disease was produced in the guinea pig, resulting in solid immunity to reinoculation. The incubation period varied from 4 to 9 days, depending on the strength of the inoculum. Pathological changes were confined to the liver, where focal necrosis was found. No inclusion bodies were demonstrated. Transmission of the infection to other animal species was successful only in rabbits and Syrian hamsters, producing a lethal disease in the latter. The agent could be propagated in embryonated hen`s eggs and was maintained by passage in this host. Dr. Tatlock and his associates were now confident that this agent was av irus.
On 1 April 1945, Dr. Tatlock was ordered to Walter Reed General Hospital, Army Medical Center, for clinical duties as Chief of the Communicable Disease Section. He took the "virus" with him, maintaining it by passage and by? as was discovered? frozen storage in a skimmed milk medium. By this time, it was assumed that freezing had foiled the previous transmission attempts of the ad hoc Commission. One year later, with the encouragement of Lieutenant Colonel Smadel of WRAIR, Dr. Tatlock was ordered on detached duty to Cincinnati, Ohio, to undertake human transmission studies with the cooperation of Dr. Albert B. Sabin (Commission on Neurotropic Virus Diseases) and the staff of Longview State Hospital. The subjects were patients undergoing fever therapy at that hospital.
By this time, the agent had been through 80 passages in guinea pigs and 23 passages in embryonated eggs. The first group of three volunteers was injected with a 10% suspension of infected embryonated chick liver in saline, 3.0 mL intramuscularly and 0.4 mL intracutaneously. All three developed a short febrile illness beginning on the 9th day. Blood drawn for these patients was defibrinated, pooled, and injected into a second group of three subjects, 5.0 mL intramuscularly and 0.4 mL intracutaneously. All developed similar febrile illnesses after 11 to 14 days. A third group consisted of eight subjects: two normal, two recovered from sand fly fever, and four recovered from dengue. Seven of the eight developed febrile illnesses within 8 to 14 days; five developed rashes of varying extent, for the most part limited to the anterior and lateral surfaces of the legs. A few developed skin lesions on the pronator areas of the forearms. Of the total of 13induced cases, five showed a slight leucocytosis late in the incubation period followed by a slight leukopenia with a relative lymphocytosis beginning about the
82
third day of the febrile phase. Inoculation of hamsters showed that the "virus" appeared in the blood of the patients shortly before the onset of fever and disappeared rapidly thereafter.
Dr. Tatlock had reproduced pretibial (Fort Bragg) fever in humans by inoculating an agent that clearly was different from the previously described rickettsialike organism. Although CARD had adopted a policy of group authorship, Dr. Tatlock was the sole author of the article that described the recovery of the "rickettsia-like" organisms at Fort Bragg. He was also the sole author of the article that described the transmission studies on a" virus" from a patient with Fort Bragg fever (see list of publications). Thus, his name became linked to Fort Bragg and to two different agents. Afterward, when reference was made to "the Tatlock agent" and Fort Bragg fever, it wasn`t always clear which agent was meant. This identity problem was to cause confusion even after the true nature of both agents was determined. Characterization of the true etiologic agent was accomplished first.
One year after the volunteer studies in Cincinnati, Drs. Joseph L. Melnick and Paul (Commission on Virus and Rickettsial Diseases) of Yale University School of Medicine succeeded in transmitting the "virus" to chimpanzees with the use of a suspension of brains from hamsters infected with material provided by Dr. Tatlock. Virus was recovered from one of the first three animals to develop fever by transfer to another chimpanzee and from another by transfer to hamsters. A rash appeared on the skin and forearm of an inoculated animal. A hamster neutralization test demonstrated the development of antibodies during convalescence in four chimpanzees given "active virus." The agent was still considered to be a virus.
Then came the Korean War. A young Army physician, Captain John Hightower, who had been a Chief Medical Resident in Dr. Woodward`s Department of Medicine at the University of Maryland, was sent to Puerto Rico, where he saw a number of cases of leptospirosis. Later, when looking at the charts of patients with Fort Bragg fever with Dr. Joseph Smadel, he suggested leptospirosis as a possible diagnosis. However, when sera from patients with Fort Bragg fever were tested with antigens from Leptospiraicterohaemorrhagiae and L. canicola, the results were negative. Dr. Smadel did not give up.
On 22 August 1951, he wrote the following note to Major William S. Gochenour, Chief of the Department of Veterinary Microbiology at the Army Medical Service Graduate School, Walter Reed Army Medical Center (WRAMC),who had just augmented his collection of leptospiral strains:
Exp. Pre Tibial Fever
Question is could this disease be caused by one of the odd leptospira which would not cross with L. can. or icte. Would appreciate your testing these two pairs of very valuable sera against the various lepto spires. If any of the samples remain, please return.
The sera showed high titers of agglutinating antibodies against L. autumnalis. So did paired sera collected by Dr. Tatlock from six soldiers at Fort Bragg in 1944 and from three volunteers in Cincinnati in 1946, as did paired sera from the four chimpanzees shown by Drs. Melnick and Paul to have developed neutralizing antibodies to Dr. Tatlock`s "virus." A leptospiral organism was cultured from the 259th hamster passage, 365th total passage, of Dr. Tatlock`s second agent since its original isolation at Fort Bragg. Cross-agglutination tests showed it to be similar to L. autumnalis akiyami A, the cause of autumnal fever in Japan. No member of this group had been detected previously in the United States. In 1973, it was classified as L. interoganssera group autumnalis, serovar fort-bragg. It pays to store serum and other key specimens and to be persistent!
What of Dr. Tatlock`s first agent? It has turned out to be the earliest isolate of the Legionella species, a strain different from L. pneumophila, the cause of the epidemic of Legionnaires` disease in Philadelphia in 1976. Other isolates soon followed, including one from renal-transplant recipients in Pittsburgh who developed pneumonia. The Pittsburgh pneumonia agent was then shown by Dr. G.A. Hebert and associates to be identical to Dr. Tatlock`s rickettsialike organism, now named L. micdadei in recognition of Dr. Joseph McDade of the CDC who was the first to culture L. pneumophila. Because of Dr. Tatlock`s
83
linkage with Fort Bragg fever, the Pittsburgh pneumonia agent became mistakenly associated with that disease, and the literature about legionellosis began to include Fort Bragg fever as an example. This confusion stimulated Dr. Tatlock to publish an editorial in early 1982 in which he summarized the history outlined above and pointed out that the etiologic agent of Fort Bragg (pretibial fever) was not Legionellamiedadei but Leptospiraautumnalis.
With the understanding that civilian investigators supported by the commissions were working for the Army, which indeed they were, it seems appropriate to end this section with a quotation from the opening paragraph of Dr. Daniel`s chapter:
The recognition of Fort Bragg fever as a specific new disease entity and the ultimate proof of its etiology is a contribution of the U.S. Army Medical Department to the science of medicine. The disease was described by Army clinicians, studied by Army medical personnel with the assistance of Army-consigned consultants, transmitted to animals by an Army research worker, and finally proved as to etiology by an Army veterinarian and others .... The story of Fort Bragg fever indicates, too, the superior opportunities which were available to military medical personnel for clinical research. Larger groups of patients with the same disease are more often available for study in military installations than in civilian institutions. It is doubtful whether this disease would have been recognized as an entity had the outbreak occurred in an urban civilian community; there, each patient might have been cared for by a different physician and treated in a different hospital, whereas, on an Army post all were concentrated in one hospital under the care of a closely knit medical service.
Viral Gastroenteritis
Infectious gastroenteritis was the second most common cause of illness in the population of the Cleveland Family Study. It was considered "nonbacterial" in that no enteric bacterial pathogens were identified at the time. Although some of the illnesses possibly were attributable to enterotoxigenic Escherichia coli and other E. coli strains now known to be pathogenic, it is believed that most of the illnesses recorded were caused by enteric viruses. After elimination of gastrointestinal symptoms considered to be secondary to another illness or caused by some cause other than illness, a total of 4,057 cases were classified as infectious gastroenteritis. They accounted for 16% of all illness and occurred at an incidence rate of 1.52 cases per person per year.
The incidence of gastroenteritis fluctuated from year to year; unlike the incidence of respiratory disease, it did not decrease with time. The incidence was lower in both male and female infants under age 1 year than in older children. From age 1 through age 9 or 10 years, the incidence was relatively constant for both sexes. Schoolchildren had a higher incidence at ages 3 and 5 years, and rates were higher among preschool children who had siblings in school than among children of the same age who did not. As expected, the number of cases per year increased with increasing family size. Secondary attack rates varied from infancy through age 7 years, but no trend was discernable. Among these young children, approximately one in every five or six intrafamilial exposures to gastroenteritis resulted in recognizable illness. Children aged 8 years and older and adults had secondary attack rates that were almost 50% as great as those of younger children. The seasonal pattern was constant from year to year, with a sharp rise in October or November followed by a gradual decline during the winter and spring and a low incidence during the summer. Sequential cases of vomiting in a family during cold weather were reminiscent of the illness previously described as "Winter Vomiting Disease."
A detailed analysis of 1,104 cases that occurred during 1948 to 1950 developed a clinical description based on the frequency of the occurrence, severity, and duration of three major gastrointestinal symptoms? nausea, vomiting, and abdominal pain. Afebrile illnesses with only one major gastrointestinal symptom made up almost 50% of the total; among these, diarrhea was the most frequent symptom. Illnesses involving various combinations of two gastrointestinal symptoms occurred with ap-
84
proximately the same frequency as those in which all three were present. The proportion of illnesses that were febrile varied from 8% of the cases with diarrhea only to 28% of the cases in which all three gastrointestinal symptoms were present. The relative frequency of vomiting was fairly constant throughout childhood but was lower for adults. Diarrhea was recorded in approximately 66% of the cases in infants and young children. This symptom, however, was recorded in only 33% of such illnesses among children age 4 years or older, whereas it was present in about 74% of cases in adults. The most likely explanation for the difference in the frequency of occurrence of diarrhea in the various age groups was considered to be the failure of toilet-trained children to report the event. The relative frequency of abdominal pain increased progressively with age through early childhood, probably reflecting the increasing ability of the child to describe this symptom. Fever occurred less often among adults than among children. The illnesses of mothers and fathers were quite similar except for greater frequency of vomiting among mothers. The explanation for this difference was not apparent.
The onset of infectious gastroenteritis was usually abrupt. If vomiting or abdominal pain occurred during an illness, it usually began on the 1st day of gastrointestinal symptoms, whereas diarrhea began on the 2nd day or later in approximately 15% of all illnesses during which it was present. Fever of 100? For more was first recorded on the day after the onset of gastrointestinal symptoms or later in about 25% of the cases in which it occurred.
About 12% of cases consisted of a single episode of vomiting or one diarrheal stool. In only 6% of cases was the temperature 102?F or higher. This degree off ever was less common in older children than in those under age 5 years and was quite unusual in adults, being present in less than 2% of adult illnesses. In only 12% of cases did the individuals vomit four or more times in a single day; no consistent relation to age was noted. Four or more stools occurred in a single day in about 21% of all cases. This degree of diarrhea was more common in children under age 2 years and in adults than in older children.
The duration of infectious gastroenteritis was short in most instances. Fifty-nine percent of illnesses lasted 1 calendar day or less, and in only 12% did symptoms last more than 3 days. In summary, the clinical picture was that of a mild illness of abrupt onset and short duration. Almost 50% of the cases were afebrile illnesses consisting of only one major gastrointestinal symptom. It was unusual for an individual to vomit repeatedly, to have a large number of diarrheal stools in a single day, or to have high fever. Although early observations suggested that at least two types of gastroenteritis? a febrile and febrile? were occurring in the population and subsequent volunteer studies indicated the existence of more than one viral etiologic agent, it was not possible to identify or separate the two types epidemiologically. Epidemiologic analysis did, however, identify a "respiratory-gastrointestinal" syndrome where the associated respiratory and gastrointestinal symptoms were related more often than would be expected by chance. Whether this syndrome represented a distinct entity or the fact that gastrointestinal symptoms are more likely to be noticed and recorded when symptoms of respiratory disease a represent could not be determined.
The primitive cell culture systems then in use identified polioviruses and coxsackie viruses, but no viruses etiologically related to gastroenteritis could be cultivated. Accordingly, in January and February 1951,stool specimens were collected and processed with the view to reproducing the naturally occurring disease in volunteers. Bacteria-free supernate of a stool from a mother who experienced anorexia, nausea, abdominal pain, and diarrhea without feverishness induced mild symptoms in one of seven young adult males 56hours after ingestion. Supernate of stool from another mother who had headache, nausea, vomiting, abdominal cramps, and a temperature of 101?F but no diarrhea induced similar illnesses in four of eight young adult males 26 to 30 hours after ingestion. The afebrile, diarrheal disease resembled that successfully transmitted to volunteers by Drs. Gordon, H. S. Ingraham, and Robert F. Korns, who referred to the unidentified agent in stool filtrates as the Marcy strain. Japanese investigators had earlier induced gastroenteritis in volunteers after oral administration of bacteria-free fecal filtrates derived from diarrhea cases in the Niigata Prefecture. In later cross-challenge studies, the Niigata and Marcy strains were found to be related. No additional studies were done with the inocu-
85
lum from the afebrile family study case, but collaborative studies were undertaken by Dr. Jordan with Dr. Gordon, then Chief of the Virology Laboratory at the Division of Laboratories and Research, New York State Department of Health, in Albany, to compare the family study agent (FS1), which induced febrile illnesses, with the Marcy agent. The Director of the Division was Dr. Gilbert Dalldorf who had recently isolated the first strains of a new group of enteroviruses from the feces of patients with poliomyelitis in the nearby town of Coxsackie, New York.
FS inoculum consisted of unfiltered supernate of a 20% suspension of three loose stools from a case induced on first human passage in Cleveland. Marcy inoculum consisted of unfiltered diarrheal feces collected from a volunteer during the sixth human passage in New York. Inocula were freed of bacteria by centrifugation and addition of antibiotics; poliovirus was excluded by intracerebral inoculation of monkeys. The isolation unit established by Dr. Gordon at the New York State Vocational Institution, West Coxsackie, New York (a prison reformatory) was used for a series of experiments designed to compare FS and Marcy strains. In a cross-immunity experiment, two groups of volunteers in individual isolation were fed FS and Marcy inocula, respectively. Each group was reinoculated twice at approximately 2-weekintervals, first with homologous, then with heterologous, inocula.
Six of the seven men given 7 mL of Marcy inoculum had typical attacks of diarrheal disease. Only one of eight men given 2 mL of FS inoculum? the amount used for the first successful passage? had a definite illness; he developed a temperature of 101.8?F, nausea, anorexia, and headache after an interval of 24hours. Sixteen days later the men ingested the same inocula; however, 10 mL instead of 2 mL of FS were administered. The Marcy group remained well, but one of the FS group became ill. Cross immunity was tested 13 days after the second inoculation. Marcy inoculum induced diarrhea in seven of eight men, including two previously sick after FS inoculum. FS inoculum induced febrile disease in three of seven men, all convalescent from experimental Marcy gastroenteritis.
Illnesses induced with the FS inoculum differed from the afebrile Marcy disease. The average incubation period of experimental Marcy illness was60 hours, whereas that of the FS type was 27 hours. Fever was characteristic of the FS illness, constitutional symptoms were more marked, and the watery diarrhea of Marcy disease was lacking. It was believed that FS illness, like Marcy disease, represented an infection, because the feeding of10 mL of autoclaved supernate prepared from stools from 5 individuals to each of18 volunteers and the ingestion of 10 mL of autogenous stool supernate by 8subjects failed to produce such symptoms. Thus, evidence was obtained that at least two agents were responsible for nonbacterial gastroenteritis. At the time, neither disease could be associated serologically with enteric human orphan(ECHO) viruses, types 7, 8, 9, 11 and 12, or reovirus, type 1.
In recent years, a number of viruses have been shown to be causally related to gastroenteritis, most notably rotaviruses (at least four human serotypes), and the Norwalk group of viruses (at least six serotypes). Both agents were first described in 1972. Rotaviruses can be grown in cell culture; Norwalk viruses are identified only by electron microscopy. Clinically, Norwalk illnesses resemble the febrile FS1 illness and winter vomiting disease, but a clear-cut seasonality has not been apparent with known Norwalk-virus associated outbreaks. Both groups of viruses are transmitted by the fecal-oral route. In view of the postulated "respiratory-gastroenteritis" syndrome, it is of interest that throat garglings obtained from volunteers with experimentally induced rotavirus diarrhea failed to yield rotavirus. Similarly, nasopharyngeal washings from a volunteer with experimentally induced Norwalk illness failed to induce illness in three volunteers. However, an outbreak of Norwalk illness in a Toronto Hospital gave rise to the postulate that Norwalk-like virus could be transmitted by respiratory droplets since the implementation of strict enteric precautions infection failed to halt the spread of infection. A number of rotavirus vaccines have been developed and are undergoing efficacy trials.
Other viruses associated with diarrhea in children include several higher type adenoviruses and calici viruses. Unfortunately, the nature of the FS1 and Marcy agents will never be known, because neither Drs. Gordon or Jordan could retrieve appropriate inocula or sera 20 years later after moving to other institutions.
86
RABBIT EARS AND ENZYMES
This last section on scientific accomplishments does not deal with a specific disease but is included to illustrate that basic studies supported by the AFEB, while directed toward a particular disease, often resulted in observations that illuminated broad aspects of biology. Such was true of the research conducted by Dr. Thomas during those years when streptococcal infections were the responsibility of the CARD.
Dr. Thomas and his associates at the University of Minnesota studied the effects of cortisone on infection, the mechanism of the generalized Schwartzman reaction (GSR) and the pathogenesis of rheumatic fever. Blockade of there ticuloendothelial system by cortisone, thorium dioxide, trypan blue, or systemic streptococcal infections, before administration of endotoxin resulted in bilateral cortical necrosis of the kidneys. Fibrinoid necrosis of coronary arteries and valvular fibrinoid vegetations were produced in rabbits by intravenous injection of gram-negative bacterial endotoxin after infection with group A streptococci. It was also demonstrated that cortisone would reactivate latent group A streptococcal infections in rabbits as long as 3.5 months after the intravenous inoculation of the streptococcus. A preliminary study was made of an outbreak of acute glomerulonephritis associated with streptococcal skin infections in an Indian reservation in northern Minnesota. Details of this study will be found in the historical account of the CSSD.
After moving to New York University, Dr. Thomas reported that lesions indistinguishable from the GSR were induced in rabbits when a single intravenous injection of endotoxin was accompanied or followed by an injection of synthetic, heparinlike polymers. These reactions were produced by doses of polymer or of endotoxin that were without effect when given singly. Heparin, in doses known to protect rabbits against GSR, prevented reaction to the combined injection. Circulating fibrinogen disappeared after polymer-endotoxin injection, suggesting that lesions of GSR may be caused by the intravascular precipitation off ibrinogen by acidic polymers.
Dr. Thomas made a fascinating observation that an intravenous injection of crude papain caused the ears of rabbits to begin to collapse within 4 hours and collapse completely at 24 hours. Within 3 or 4 days after papain, the ears gradually resumed their normal form. Ear collapse was associated with depletion of the ear cartilage matrix and the disappearance of basophilia from the matrix. At the time, when the ears were restored to normal shape, the basophilic matrix reappeared in cartilage. Similar changes occurred in all other cartilage tissues, including bones, joints, larynx, trachea, and bronchi. When the arterial circulation to one ear was occluded for 15 minutes at the time of injection of papain, this ear was protected against collapse. Repeated injections of papain, over a period of 2 or 3 weeks, brought about immunity to the phenomenon of ear collapse. Cortisone prevented the return of papain-collapsed ears to their normal shape and rigidity. It was postulated that this reflected a capacity of cortisone to impede the synthesis or disposition of sulfated mucopolysaccharide in tissues.
Initially, the effect of crude papain could not be reproduced by crystallinepapa in protease or crystalline papain lysozyme. To be effective, crystallinepapain had first to be inactivated by thiol antagonists such as oxidation or sulfhydryl agents before administration. Crysteine-activated crystalline papain, when injected intravenously, produced little or no change in cartilage. The changes that occurred in cartilage after an injection of inactivated crystalline papain were indistinguishable from those produced by crude papain. Activation of crude papain by cysteine before injection resulted in loss of its capacity to produce in vivo changes in cartilage.
The progressive changes that took place in cartilage in vivo also occurred invitro in isolated rabbit ears removed shortly after an injection of crude papain or inactivated crystalline papain. In vitro ear collapse occurred rapidly at 37?C but did not occur at 4?C. Collapse was enhanced by exposing the cartilage to crysteine and prevented by exposure to iodoacetamide or p-chloromercuribenzoate. The direct action of crystalline papain on plates of normal cartilage in vitro resulted in the same gross and histological changes that were observed in vivo. The direct action was accelerated by crysteine and inhibited by iodoacetamide or p-chloromercuribenzoate. Dr. Thomas suggested that the reason for the
87
failure of activated papain to enter cartilage, after being injected intravenously, was that it probably reacted with a substrate in the blood, the assumption being that oxidized or otherwise inactivated papain was readily taken up by cartilage and converted there to its active form.
These interesting studies have not yet led to any practical therapeutic advances or public health applications, but the fact that Dr. Thomas was encouraged to pursue them reflects the encouragement extended by the AFEB to basic research and the flexibility of the Army Research and Development Command in supporting the AFEB`s recommendations. In the post-World War II years, a continuing increase in funding for biomedical research was provided by the NIH, the AFEB, and its commissions that sustained the laboratories of investigators who used such new technologies such as cell culture to develop new viral vaccines and those who were to trained the next generation of microbiologists and immunologists. When the AFEB was rechartered without commissions, certain groups considered the focus provided by a commission to have been so valuable as to the merit continuation in some form. The members of the CSSD established the Lancefield Society; those of the Commission on Rickettsial Diseases created the American Society for Rickettsicology and Rickettsial Diseases. Members of CARD contributed to a number of national and international groups that sought ways to reduce the morbidity and mortality of respiratory diseases. Thus, the influential work of CARD continued long after its last meeting in November 1972.
SUMMARY
During the World War II period, 1941 to 1946, approximately 75 civilian consultants, some temporarily in uniform, served four of the commissions of the AEB concerned with diseases transmitted by the respiratory route. Some individuals were members of more than one of these commissions, a practice that, along with periodic AFEB meetings, facilitated the exchange of information regarding the epidemiology and control of respiratory illnesses. As in previous wars, the burden of such illnesses was borne primarily by immunologically naive recruits. Studies during World War II defined three distinct acute respiratory illnesses: primary atypical pneumonia, ARD of military recruits, and the common cold; established the efficacy of a quadravalent pneumococcal polysaccharide vaccine; demonstrated that massprophylaxis with sulfadiazine controlled epidemics of meningococcal meningitis; showed that attempts to reduce the number of organisms in the air of barracks were of little value in reducing the incidence of illness spread by close personal contact; used the coccidioidin skin test to locate geographic areas of endemic coccidioidomycosis that should be avoided by training exercises or where dust control measures should be instituted or both; confirmed that a form of pneumonia first described in Australia (Q, or Query, fever) was the cause of epidemics in U.S. troops in the Mediterranean Theater; and recognized a new disease entity? pretibial (Fort Bragg) fever.
From 1946 to 1972, approximately 50 civilian scientists served as members or associate members of CARD under the AFEB. They assumed responsibility for the concerns of three short-lived commissions (Air-Borne Infections, Meningococcal Meningitis, and Pneumonia) and, for 3 years, the program of the Commission on Streptococcal Infections. Under four directors, studies during this quarter century described the epidemiology of common respiratory disease in a population of civilian families; detailed the behavior of sequential epidemics of H1N1 influenza and of the pandemic of H2N2 influenza (Asian) in the same population; used challenge studies in over 1,000 volunteers to demonstrate that nasal secretions from different donors with common colds contained different infectious agents; identified adenoviruses as the cause of ARD and developed an effective vaccine for the prevention of this important recruit disease; identified Mycoplasma pneumoniae as the cause of atypical pneumonia; cultivated a number of new viruses that can cause the symptoms of the common cold, the most important being over 100rhinovirus serotypes; encouraged the commercial production of a 23-valentpneumococcal polysaccharide vaccine; recognized that certain group A R-hemolyticstreptococci are nephritogenic;
88
Surprising Collapse of Rabbit Ears.
[Picture is copyrighted and is unavailable for viewing]
The surprising collapse of rabbit ears observed by Dr. Lewis Thomas following the intravenous injection of papain. A: before infection. B: 4 hours after. C: 24 hours after. D: 5 days after X 2/3. Reprinted with permission from the Journal of Experimental Medicine. 1956, Vol. 104, Plate 19. ? Rockefeller University Press.
89
demonstrated that more than one nonbacterial agent causes acute gastroenteritis; assisted military physicians in the management of epidemics of meningitis after meningococci became resistant to sulfadiazine and before Army scientists developed effective meningococcal vaccines; found no difference in hospital admission rates for respiratory infections (adenovirus, influenza B, streptococcal) between recruits housed in open-bay versus closed-bay barracks; applauded the demonstration by Army scientists in 1951 that the agent transmitted to guinea pigs in 1944 from a patient with Fort Bragg fever was a leptospira and, most importantly, provided a group of experts familiar with the military medical services and their preventive medicine officers, experts prepared to respond promptly to requests for advice and guidance and willing to undertake specific studies as needed.
It is not possible to determine the cost of these advisory and research activities to the federal government. The early, wartime budgets of the four commissions have been given, but data regarding the subsequent contracts sponsored by CARD are incomplete. A search of available archives has failed to provide a credible list of all investigators and their budgets, so the budgets have not been tabulated and totaled. The investigators and their institutions can be ascertained from the list of publications. Even if available, a sum of CARD contract budgets would be imprecise, because travel and meeting costs were charged to a central fund. Even during World War II, research budgets were supplemented by grants from foundations. Later, funds from other agencies, particularly the NIH, helped to sustain laboratories holding commission contracts under the auspices of the AFEB. Whatever the investment by the Department of Defense,: it is estimated that the prevention of illness and concurrent interruption of training schedules through the use of adenovirus vaccine alone have saved that much money, if not more.
90
MAXWELL FINLAND, M.D., RICHARD M. KRAUSE,M.D., AND
WILLIAM S. JORDAN, JR., M.D.
{kind=link}
Commission discussions are carried on in the civilian sector as Drs. Maxwell Finland, CARD and Distinguished Professor at Harvard; Richard M. Krause, Commission on Streptococcal and Staphylococcal Infections and Director of the National Institute of Allergy and Infectious Diseases; and William S. Jordan, Jr., CARD and Director of that institute`s Microbiology and Infectious Diseases Program attend a "Symposium on the Impact of Infections on Medical Care in the United States" at the National Institutes of Health in May 1978.
91
The last meeting of the Commission on Acute Respiratory Diseases, November 1972.
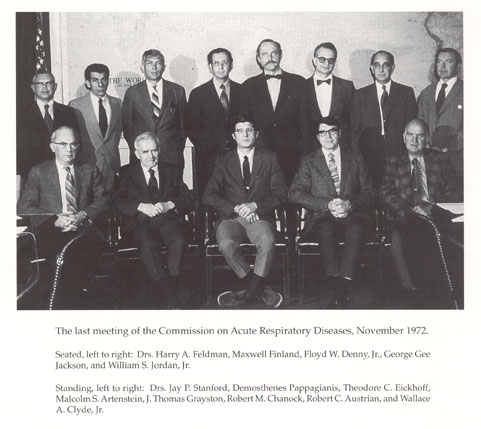{kind=link}
Seated, left to right: Drs. Harry A. Feldman, Maxwell Finland, Floyd W. Denny, Jr., George Gee Jackson, and William S. Jordan, Jr.
Standing, left to right: Drs. Jay P Stanford, Demosthenes Pappagianis, Theodore C. Eickhoff, Malcolm S. Artenstein, J. Thomas Grayston, Robert M. Chanock, Robert C. Austrian, and Wallace A. Clyde, Jr.
92
PUBLICATIONS
Commission on Acute Respiratory Diseases
1941-1943
Dingle, J. H., Abernethy, T. J., Badger, G. F. , Buddingh, G. J., Feller, A.E., Langmuir, A. D., Ruegsegger, J. M., and Wood, W. B. Primary atypical pneumonia, etiology unknown. War. Med. 1943, 3, 223-248.
Sharp, D. G., Taylor, A. R., McLean, I. W., Jr., Beard, D., Beard, J. W., Feller, A. E., and Dingle, J. H. Isolation and characterization of influenza virus B (Lee strain). Science 1943, 98, 307-308.
Taylor, A. R., Sharp, D. G., Beard, D., Beard, J. W., Dingle, J. H., and Feller, A. E. Isolation and characterization of influenza A virus (PR8 strain). J. Immunol. 1943, 47, 261-282.
Taylor, A. R., Sharp, D. G., McLean, I. W., Jr., Beard, D., Beard, J. W., Dingle, J. H., and Feller, A. E. Purification and character of the swine influenza virus. Science 1943, 98, 587-589.
1944
Beard, J. W., Sharp, D. G., Taylor, A. R., McLean, I. W., Jr., Beard, D., Feller, A. E., and Dingle, J. H. Ultracentrifugal, chemical and electron microscopic identification of the influenza virus. South. Med. J. 1944, 37, 313-320.
Commission on Acute Respiratory Diseases. Epidemiology of atypical pneumonia and acute respiratory disease at Fort Bragg, North Carolina. Am. J. Public Health 1944, 34, 335-346.
Commission on Acute Respiratory Diseases. Primary atypical pneumonia. Am. J. Public Health 1944, 34, 347-357.
Commission on Acute Respiratory Diseases. Endemic exudative pharyngitis and tonsillitis. Etiology and clinical characteristics. J. Am. Med. Assoc. 1944, 125, 1163-1169.
Commission on Acute Respiratory Diseases. Cold hemagglutinins in primary atypical pneumonia and other respiratory infections. Am. J. Med. Sci. 1944, 208, 742-750.
Dingle, J. H., Abernethy, T. J., Badger, G.F., Buddingh, G. J., Feller, A. E., Langmuir, A. D., Ruegsegger, J. M., and Wood, W. B., Jr. Primary atypical pneumonia, etiology unknown. (Parts I, II, and III.) Am. J. Hyg. 1944, 39, 67-128, 197-268, 269-336.
Kaplan, M. H. Nature and role of the lytic factor in hemolyticstreptococcal fibrinolysis. Proc. Soc. Exp. Biol. Med. 1944, 57, 40-43.
McLean, I. W., Jr., Beard, D., Taylor, A. R., Sharp, D. G., Beard, J. W., Feller, A. E., and Dingle, J. H. Influence of temperature of incubation on the increase of influenza virus B (Lee strain) in the chorioallantoic fluid of chick embryos. J. Immunol. 1944, 48,305-316.
Sharp, D. G., Taylor, A. R., McLean, I. W., Jr., Beard, D., Beard, J. W., Feller, A. E., and Dingle, J. H. Isolation and characterization of influenza virus B (Lee strain). J. Immunol. 1944, 48, 129-153.
Tatlock, H. A rickettsia-like organism recovered from guinea pigs. Proc. Soc. Exp. Biol. Med. 1944, 57, 95-99.
Taylor, A. R. Chemical analysis of the influenza viruses A(PR8 strain) and B (Lee strain) and the swine influenza virus. J. Biol. Chem. 1944, 153, 675-686.
Taylor, A. R., Sharp, D. G., McLean, I. W., Jr., Beard, D., Beard, J. W., Dingle, J. H., and Feller, A. E. Purification and character of the swine-influenza virus. J. Immunol. 1944, 48, 361-379.
1945
Commission on Acute Respiratory Diseases. Atypical pneumonia. Am. J. Med. Sci. 1945, 209, 55-58.
Commission on Acute Respiratory Diseases. An experimental attempt to transmit primary atypical pneumonia in human volunteers. J. Clin. Invest. 1945, 24, 175-188.
93
Commission on Acute Respiratory Diseases. The present status of the etiology of primary atypical pneumonia. Bull. N. Y. Acad. Med. 1945,2nd Ser. 21, 235-262.
Commission on Acute Respiratory Diseases. Transmission of primary atypical pneumonia to human volunteers. J. Am. Med. Assoc. 1945, 127, 146-149.
Commission on Acute Respiratory Diseases, Dammin, G. J., and Weller, T. H. Attempts to transmit primary atypical pneumonia and other respiratory tract infections to the mongoose. J. Immunol. 1945,50, 107-114.
Commission on Acute Respiratory Diseases, and Kaplan, M. H. A quantitative study of the fibrinolysin-antifibrinolys in reaction. Science 1945, 101, 120-122.
Commission on Acute Respiratory Diseases. Role of B-hemolyticstreptococci in common respiratory disease. Am. J. Public Health 1945, 35, 675-682.
Commission on Acute Respiratory Diseases. A study of a food-borne epidemic of tonsillitis and pharyngitis due to B-hemolyticstreptococcus, type 5. Bull. John Hopkins Hosp. 1945, 77, 143-210.
Commission on Acute Respiratory Diseases and the New York State Department of Health. The relation between epidemics of acute bacterial pneumonia and influenza. Science 1945, 102, 561-563.
Rammelkamp, C. H., and Kirby, W. M. M. Factors determining the dosage of penicillin in the treatment of infections. Bull. N. Y. Acad. Med. 1945, 2nd Ser., 21, 656-672.
1946
Commission on Acute Respiratory Diseases. The periodicity of influenza. Am. J. Hyg. 1946, 43, 29-37.
Commission on Acute Respiratory Diseases. The effect of double-bunking in barracks on the incidence of respiratory disease. Am. J. Hyg. 1946, 43, 65-81.
Commission on Acute Respiratory Diseases and Commission on Air-Borne Infections. A study of the effect of oiled floors and bedding on the incidence of respiratory disease in new recruits. Am. J. Hyg. 1946, 43,120-144.
Commission on Acute Respiratory Diseases. Acute respiratory disease among new recruits. Am. J. Public Health 1946, 36, 439-450.
Commission on Acute Respiratory Diseases. Hemagglutination byamniotic fluid from normal embryonated hen`s eggs. Proc. Soc. Exp. Biol. Med.1946, 62, 118-123.
Commission on Acute Respiratory Diseases. Association of acute pulmonary lesions with infections of the throat. Ann. Int. Med. 1946, 25, 473-487.
Commission on Acute Respiratory Diseases. Studies of streptococcal fibrinolysis. IV Clinical application of a quantitative antifibrinolysin test. J. Clin. Invest. 1946, 25, 352-359.
Commission on Acute Respiratory Diseases. The transmission of primary atypical pneumonia to human volunteers. I. Experimental methods. Bull. Johns Hopkins Hosp. 1946, 79, 97-108.
Commission on Acute Respiratory Diseases. Association of pneumonia with erythema multiforme exudativum. Arch. Intern. Med. 1946,78, 687-710.
Commission on Acute Respiratory Diseases. The transmission of primary atypical pneumonia to human volunteers. II. Results of inoculation. Bull. Johns Hopkins Hosp. 1946, 79, 109-124.
Commission on Acute Respiratory Diseases. The transmission of primary atypical pneumonia to human volunteers. III. Clinical features. Bull. Johns Hopkins Hosp. 1946, 79, 125-152.
Commission on Acute Respiratory Diseases. The transmission of primary atypical pneumonia to human volunteers. IV Laboratory studies. Bull. Johns Hopkins Hosp. 1946, 79, 153-167.
Commission on Acute Respiratory Diseases. Q fever: A foreword. Introduction to a series of papers dealing with Q fever. Am. J.Hyg. 1946, 44, 1-5.
Feinstein, M., Yesner, R., and Marks, J. L. Epidemics of Q fever among troops returning from Italy in the spring of 1945. I. Clinical aspects of the epidemic at Camp Patrick Henry, Virginia. Am. J. Hyg. 1946, 44, 72-87.
Commission on Acute Respiratory Diseases. Epidemics of Q fever among troops returning from Italy in the spring of 1945. II. Epidemiological studies. Am. J. Hyg. 1946, 44, 88-102.
94
Commission on Acute Respiratory Diseases. Epidemics of Q fever among troops returning from Italy in the spring of 1945. III. Etiological studies. Am. J. Hyg. 1946, 44, 103-109.
Commission on Acute Respiratory Diseases. Identification and characteristics of the Balkan grippe strain of Rickettsia burneti. Am. J. Hyg. 1946, 44, 110-122.
Commission on Acute Respiratory Diseases. A laboratory outbreak of Q fever caused by the Balkan grippe strain of Rickettsia burneti. Am. J. Hyg. 1946, 44, 123-157.
Gallenson, N. Hypertonic sodium chloride solution as serum dilutent in aqglutination tests with Ricksettsia burneti. Proc. Soc. Exp. Biol. Med. 1946, 63, 169-171.
Kaplan, M. H. Studies of streptococcal fibrinolysis. I. The dissimilarity of serum protease and trypsin as indicated bythe separate specificities of their kinases, fibrinolys in and enterokinase. J. Clin. Invest. 1946, 25, 331-336.
Kaplan, M. H. Studies of streptococcal fibrinolysis. II. The inhibition of streptococcal fibrinolysis by antifibrinolys in and antiprotease. J. Clin. Invest. 1946, 25, 337-356.
Kaplan, M. H., and Commission on Acute Respiratory Diseases. Immunological similarity of streptococcal antifibrinolysins. Proc. Soc. Exp.Biol. Med. 1946, 63, 50-53.
Kaplan, M. H., and Commission on Acute Respiratory Diseases. Studies of streptococcal fibrinolysis. III. A quantitative method for the estimation of serum antifibrinolys in. J. Clin. Invest. 1946, 25, 237-351.
1947
Commission on Acute Respiratory Diseases. Bacteriological findings in undifferentiated and other acute respiratory diseases. Medicine 1947,26, 465-484.
Commission on Acute Respiratory Diseases. Clinical patterns of undifferentiated and other acute respiratory diseases in army recruits. Medicine 1947, 26, 441-464.
Commission on Acute Respiratory Diseases. Experimental transmission of minor respiratory illness to human volunteers by filter-passing agents. I. Demonstration of two types of illness characterized by long and short incubation periods and different clinical features. J. Clin. Invest. 1947, 26, 957-973.
Commission on Acute Respiratory Diseases. Experimental transmission of minor respiratory illness to human volunteers by filter-passing agents. II. Immunity on reinoculation with agents from the two types of minor respiratory illness and from primary atypical pneumonia. J. Clin. Invest. 1947, 26, 974-982.
Commission on Acute Respiratory Diseases. Exudative tonsillitis and pharyngitis of unknown cause. J. Am. Med. Assoc. 1947,133, 588-593.
Commission on Acute Respiratory Diseases. Studies on streptococcal fibrinolysis. V. The in vitro production off ibrinolysin by various groups and types of beta hemolytic streptococci; relationship to anti fibrinolysin production. J. Exp. Med. 1947, 85,441-457.
Commission on Acute Respiratory Diseases. The role of Lancefield groups of beta-hemolytic streptococci in respiratory infections. N. Engl. J. Med. 1947, 236, 157-166.
Commission on Acute Respiratory Diseases in collaboration with Mickle, W. A., Jr. Studies on the causation of an unusual pulmonary disease at Camp Gruber, Oklahoma. Arch. Intern. Med. 1947, 80,203-204.
Dingle, J. H. Experimental studies of the "common cold" in human volunteers. Trans. Stud. Coll. Physicians Phila. 1947,15, 113-123.
Smith, C. E. Recent progress in pulmonary mycotic infections. Calif. Med. 1947, 67, 1-7.
Tatlock, H. Studies on a virus from a patient with Fort Bragg fever (pretibial fever). J. Clin. Invest. 1947, 26, 287-297.
1948
Commission on Acute Respiratory Diseases. Endemic influenza. Am. J. Hyg. 1948, 47, 290-296.
Commission on Acute Respiratory Diseases (in collaboration with Mickle, W. A., and Oliver, T. J.). Problems in determining the bacterial flora of the pharynx. Proc. Soc. Exp. Biol. Med. 1948, 69, 45-52.
95
Commission on Acute Respiratory Diseases. Studies of the 1943 epidemic of influenza A. I. Introduction II. Comparison of the clinical and laboratory characteristics of influenza A and undifferentiated acute respiratory disease (ARD). III. The reliability of immunological methods for the diagnosis of influenza. IV The antibody response to infection. V The distribution of influenza virus. VI. Epidemiological characteristics in varied types of military units and comparison with undifferentiated acute respiratory disease. VII. The relative frequency of recognized and inapparent infections, the relation between antibody titer and susceptibility, and the change in the antibody status of a selected population. VIII. General discussion and summary. Am. J. Hyg. 1948, 48, 253-349.
Commission on Acute Respiratory Diseases. Influenza B. Study of a localized outbreak preceding the 1945 epidemic. Am. J. Hyg. 1948, 47, 297-303.
Dingle, J. H. Common virus infections of the respiratory tract: Diagnosis and etiology. J. Am. Med. Assoc. 1948, 138, 1084-1088.
Heidelberger, M., MacLeod, C. M., and Dilapi, M. M. The human antibody response to simultaneous injection of six specific polysaccharides of pneumococcus. J. Exp. Med. 1948, 88, 369-372.
*Schoenbach, E. B., and Phair, J.J. Appraisal of the techniques employed for the detection of subclinical (inapparent) meningococcal infections. Am. J. Hyg. 1948, 47, 271-281.
Smith, C. E., Beard, R. R., and Saito, M. T. Pathogenesis of coccidioido mycosis with special reference to pulmonary cavitation. Ann. Int. Med. 1948, 29, 623-655.
1949
Austrian, R., and MacLeod C. M. Acquisition of M protein by pneumococci through transformation reactions. J. Exp. Med. 1949, 89, 451-460.
Austrian, R., and MacLeod, C. M. A type-specific protein from pneumococcus. J. Exp. Med. 1949, 89, 439-450.
Commission on Acute Respiratory Diseases. A comparison of the bacterial flora of the pharynx and nasopharynx. Am. J. Hyg. 1949, 50, 331-336.
Commission on Acute Respiratory Diseases. The single throat culture as an index of the bacterial flora of the respiratory tract. Am. J. Hyg. 1949,50, 168-174.
Dingle, J. H., Badger, G. F., Feller, A. E., Hodges, R. G., Jordan, W. S., Jr., and Rammelkamp, C. H., Jr. A study of respiratory infections in families. Trans Assoc. Am. Physicians 1949, LXII, 99-104.
Heidelberger, C. M., and Dilapi, M. M. Measurement and preservation of antibodies in human sera. J. Immunol. 1949, 61, 153-159.
Jordan, W. S., Jr. The infectiousness and incubation period of primary atypical pneumonia. Am. J. Hyg. 1949, 50, 315-330.
MacLeod, C. M., Heidelberger, M., Robinson, B., Dilapi, M. M., Walter, A. W., and Sutliff, W. D. The antibody response of rabbits to a single injection of type I pneumococci. J. Immunol.1949, 61, 179-183.
Rammelkamp, C. H., Jr. Badger, G. F., Dingle, J. H., Feller, A. E., and Hodges, R. G. Quantitative method for measuring staphylococcal anticoagulase. Proc. Soc. Exp. Biol. Med. 1949, 72, 210-213.
Randall, E., and Rantz, L. A. Stable, reduced, desiccated streptolysin "O." Proc. Soc. Exp. Biol. Med. 1949, 70, 414-416.
Robinson, R. L. Studies on the technique of isolating pneumococci from throat cultures by mouse inoculation. Am. J. Hyg. 1949, 50, 343-348.
Smith, C. E., Saito, M. T., Beard, R. R., Rosenberger, H. G., and Whiting, E.G. Histoplasmin sensitivity and coccidioidal infection. I. Occurrence of cross-reactions. Am. J. Public Health 1949, 39, 722-736.
1950
Denny, F. W., Wannamaker, L. W., Brink, W. R., Rammelkamp, C.H., Jr., and Custer, E. A. Prevention of rheumatic fever. Treatment of the proceeding streptococcic infection. J. Am. Med. Assoc. 1950, 143, 151-153.
96
Feller, A. E., Badger, G. F., Hodges, R. G., Jordan, W. S., Jr., Rammelkamp, C. H., Jr., and Dingle, J. H. The failure of antihistaminic drugs to prevent or cure the common cold and undifferentiated respiratory diseases. N. Engl. J. Med. 1950, 242, 737-744.
Feller, A. E., and Jordan, W. S., Jr. (1)Serologic studies of mumps employing complement fixation and agglutination-inhibition; (2) The relationship of complement-fixing and antihemagglutinating factors against the viruses of mumps and Newcastle disease. J. Lab. Clin. Med. 1950, 36, 360-368, 369-377.
Heidelberger, M., Dilapi, M. M., Siegel, M., and Walter, A. W. Persistence of antibodies in human subjects injected with pneumococcal polysaccharides. J. Immunol. 1950, 65, 535-541.
Heidelberger, M., MacLeod, C. M., Markowitz, H., and Roe, A.S. Improved methods for the preparation of the specific polysaccharides of pneumococcus. J. Exp. Med. 1950, 91, 341-349.
Jordan, W. S., Jr., and Albright, R. W. Liver function tests in infections mononucleosis. J. Lab. Clin. Med. 1950, 35, 688-698.
Jordan, W S., Jr., Badger, G. F., and Dingle, J. H. Immunological studies of pneumococcal pneumonia in patients treated with penicillin. J. Clin. Invest. 1950, XXIX, 161-168.
Loosli, C. G., Smith, M. H. D., Cline, J., and Nelson, L. The transmission of hemolytic streptococcal infections in infant wards with special reference to "skin dispersers." J. Lab. Clin. Med. 1950, 36, 342-359.
MacLeod, C. M., and Krauss, M. R. Relation of virulence of pneumococcal strains for mice to the quantity of capsular polysaccharide formed in vitro. J. Exp. Med. 1950, 92, 1-9.
Maroney, M., and Rantz, L. A. Electrocardiogram in 679 healthy infants and children. Pediatrics 1950, March, 396-407.
Rammelkamp, C. H., Jr., Badger, G. F., Dingle, J. H., Feller, A. E., and Hodges, R. G. Antigenicity of cell-free staphylococcal coagulase. J. Infect. Dis. 1950, 86, 159-163.
Rammelkamp, C. H., Jr., Hezebicks, M. M., and Dingle, J. H. Specific coagulases of staphylococcus aureus. J. Exp. Med. 1950, 91,295-307.
Smith, C.E., Saito, M. T., Beard, R. R., Kepp, R. M., Clark, R. W., and Eddie, B. U. Serological tests in the diagnosis and prognosis of coccidioidomycosis. Am. J. Hyg. 1950, 52, 1-21.
Stollerman, G. H., and Bernheimer, A. W. Inhibition of streptolysin S by the serum of patients with rheumatic fever and acute streptococcal pharyngitis. J. Clin. Invest. 1950, 29, 1147-1155.
Wannamaker, L. W., Denny, F. W., Rammelkamp, C. H., Jr., and Brink, W. R. Use of Maxted`s method for group classification of hemolytic streptococcai. Proc. Soc. Exp. Biol. Med. 1950, 73, 467-469.
1951
Brink, W. R., Rammelkamp, C. H., Jr., Denny, F. W., and Wannamaker, L. W. Effect of penicillin and aureomycin on the natural course of streptococcal tonsillitis and pharyngitis. Am. J. Med. 1951,10, 300-308.
Hahn, E. O., Houser, H. B., Rammelkamp, C. H., Jr., Denny, F. W, and Wannamaker, L. W. Effect of cortisone on acute streptococcal infections and post-streptococcal complications. J. Clin. Invest. 1951, 30, 274-281.
Heidelberger, M., MacLeod, C. M., and Dilapi, M. M. Antigenic potency in man of the specific polysaccharides of types I and Vpneumococcus and their products of alkaline degradation. J. Immunol. 1951,66, 145-149.
Heidelberger, M., MacLeod, C. M., Markowitz, H., and Dilapi, M. M. Absence of a prosthetic group in a type-specific polysaccharide of pneumococcus. J. Exp. Med. 1951, 94, 359-362.
Jordan, W. S., Jr., Albright, R. W., McCain, F. H., and Dingle, J. H. Clinical variations in primary atypical pneumonia. Am. J. Med. 1951,10, 3-020.
Marsh, R. R., and Tillotson, I. G. The cutaneous toxicity and therapeutic effectiveness of penicillin O. N. Engl. J. Med. 1951, 245,17-20.
Rantz, L. A., Maroney, M., and DiCaprio, J. M. Antistreptolysin O response following hemolytic streptococcus infection in earlychildhood. A.M.A. Archives Int. Med. 1951, 87, 360-371.
97
Sartwell, P E. Common respiratory disease in recruits. Am. J. Hyg. 1951, 53, 224-235.
Smith, C. E. Diagnosis of pulmonary coccidioidal infections. Calif.Med. 1951, 75, 385-391.
Wannamaker, L. W., Rammelkamp, C. H., Jr., Denny, F. W., Brink, W. R., Houser, H. B., Hahn, E. O., and Dingle, J. H. Prophylaxis of acute rheumatic fever, by treatment of the preceding streptococcal infection with various amounts of depot penicillin. Am. J. Med. 1951,10, 673-695.
1952
DiCaprio, J. M. Rantz, L. A., and Randall, E. Studies on streptococcal hyaluronidase and antihyaluronidase. A.M.A. Archives Int. Med. 1952, 89, 374-386.
Feller, A. E. Cold hemagglutinins: Effect of storage at -20?C.J. Lab. Clin. Med. 1952, 39(3), 440-442.
Feller, A. E., and Stevens, D. A. Sheep blood agar for the isolation of Lancefield groups of beta hemolytic streptococci. J. Lab. Clin. Med. 1952, 39(3), 484-491.
Houser, H. B., and Eckhardt, G. C. Recent developments in the prevention of rheumatic fever. Ann. Intern. Med. 1952, 37, 1035-1043.
Mandel, A., and Jordan, W. S., Jr. Ornithosis (psittacosis) in chickens and poultry workers. Am. J. Hyg. 1952, 55, 230-238.
Rammelkamp, C. H., Jr. Prevention of rheumatic fever. Bull.Rheum. Dis. 1952,11(7),13-14.
Rammelkamp, C. H., Jr., Wannamaker, L. W., and Denny, F. W. The epidemiology and prevention of rheumatic fever. Bull. N.Y. Acad. Med. 1952,28, 321-334.
Rammelkamp, C. H., Jr., Weaver, R. S., and Dingle, J. H. Significance of the epidemiological differences between acute nephritis and acute rheumatic fever. Trans. Assoc. Am. Physicians 1952, 65, 168.
Stevens, D. A. Studies on the technique of transporting throat swabs to the laboratory for the isolation of pneumococci. J. Lab. Clin. Med. 1952,39, 437-439.
1953
Badger, G. F., Dingle, J. H., Feller, A. E., Hodges, R. G., Jordan, W. S., Jr., and Rammelkamp, C. H., Jr. A study of illness in a group of Cleveland families. II. Incidence of the common respiratory diseases. Am. J. Hyg. 1953, 58, 31-40.
Badger, G. E, Dingle, J. H., Feller, A. E., Hodges, R. G., Jordan, W. S., Jr., and Rammelkamp, C. H., Jr. A study of illness in a group of Cleveland families. III. Introduction of respiratory infections into families. Am. J. Hyg. 1953, 58, 41-46.
Badger, G. F., Dingle, J. H., Feller, A. E., Hodges, R. G., Jordan, W. S., Jr., and Rammelkamp, C. H., Jr. A study of illness in a group of Cleveland families. IV The spread of respiratory infections within the home. Am. J. Hyg.,1953, 58, 174-178.
Badger, G. F., Dingle, J. H., Feller, A. E., Hodges, R. G., Jordan W. S., Jr., and Rammelkamp, C. H., Jr. A study of illness in a group of Cleveland families. V. Introductions and secondary attack rates as indices of exposure to common respiratory diseases in the community. Am. J. Hyg. 1953, 58, 179-182.
Brock, L. L., and Siegel, A. C. Studies on the prevention of rheumatic fever: The effect of time of initiation of treatment of streptococcal infections on the immune response of the host. J. Clin. Invest.1953, 32, 630-632.
Clark, E. J., and Houser, H. B. Comparative effects of 3 hydroxy-2-phenylcinchoainic acid (HPC) and aspirin on the acute course of rheumatic fever and the occurrence of rheumatic valvular disease. Am. Heart J. 1953, 45, 576-588.
Denny, E W., Jr., and Thomas, L. The demonstration of type specific streptococcal antibody by a hemagglutination technique employing tannic acid. J. Clin. Invest. 1953, 32, 1085-1093.
Denny, F. W., Jr., Wannamaker, L. W., and Hahn, E. O. Comparative effects of penicillin, aureomycin and terramycin on streptococcaltonsillitis and pharyngitis. Pediatrics 1953, 11, 7-14.
Dingle, J. H., Badger, G. E, Feller, A. E., Hodges, R. G., Jordan, W. S., Jr., and Rammelkamp, C. H., Jr. A study of illness in a group of Cleveland families. I. Plan of study and certain general observations. J. Hyg. 1953, 58, 16-30.
98
Dingle, J. H., Rammelkamp, C. H., Jr., and Wannamaker, L. W. Epidemiology of streptococcal infections and their non-suppurative complications. Lancet 1953, April 11, 736.
Ginsberg, H. S. Comparison of quantity of egg and mouse-adapted influenza viruses required to infect each host (20606). Proc. Soc. Exp. Biol. Med.1953, 84, 249-252.
Good, R. A., and Thomas, L. Studies on the generalized Schwartzman reaction. IV. Prevention of the local and generalized Schwartzman reactions with heparin. J. Exp. Med. 1953, 97, 871-888.
Jordan, W. S., Jr., Gordon, I., and Dorrance, W. R. A study of illness in a group of Cleveland families VII. Transmission of acute non-bacterial gastroenteritis to volunteers: Evidence for two different etiologic agents. J. Exp. Med. 1953, 98, 461-475.
Rammelkamp, C. H., Jr. Glomerulonephritis. Proc. Inst. Med. Chic.1953,19, 17.
Rantz, L. A., Maroney, M., and DiCaprio, J. M. Hemolytic streptococcal infection in childhood. Pediatrics 1953, 12, 5.
Smith, R. T., Thomas, L., and Good, R. A. Generalized Schwartzman reaction. V. Effect of intravenous injection of colloidal iron or carbon on response of rabbits to meningococcal toxin (20226). Proc. Soc. Exp. Biol. Med. 1953, 82, 712-715.
Thomas, L., Denny, F. W., Jr., and Floyd, J. Studies on the generalized Schwartzman reaction. III. Lesions of the myocardium and coronary arteries accompanying the reactional in rabbits prepared by infection with group A streptococci. J. Exp. Med. 1953, 97, 751-766.
Walker, S. H. The failure of antibiotic therapy in infectious mononucleosis. Am. J. Med. Sci. 1953, 226, 65-72.
Wannamaker, L. W., Denny, F. W., Jr., Perry, W. D., Rammelkamp, C. H., Jr., Eckhardt, G. C., Houser, H. B., and Hahn, E. O. The effect of penicillin prophylaxis on streptococcal disease rates and the carrier state. N. Engl. J. Med. 1953, 249, 1-7.
1954
?Catanzaro, F. D. J., Stetson, C. A., Morris, A. J., Chamovitz, R., Rammelkamp, C. H., Jr., Stolzer, B. L., and Perry, W. D. The role of the streptococcus in the pathogenesis of rheumatic fever. Am. J. Med. 1954, 17, 749-756.
Chamovitz, R., Catanzaro, F. J., Stetson, C. A., Rammelkamp, C. H., Jr. Prevention of rheumatic fever by treatment of previous streptococcal infections. N. Engl. J. Med. 1954, 251, 466-471.
?Denny, F. W., Jr. The prophylaxis of streptococcal infections. Strep. Infect. 1954, Chapter 13.
Dingle, J. H. The clinical pattern of streptococcal infection in man. Strep. Infect. 1954, Chapter 9.
Dingle, J. H., Ginsberg, H. S., Badger, G. F., Jordan, W. S., Jr., and Katz, S. Evidence for the specific etiology of "acute respiratory disease(ARD)." Trans. Assoc. Am. Physicians 1954, 67, 149-154.
Ginsberg, H. S. Formation of non-infectious influenza virus in mouse lungs: its dependence upon extensive pulmonary consolidation initiated by the viralinoculum. J. Exp. Med. 1954, 100, 581-603.
Ginsberg, H. S. Production of pulmonary lesions by influenza viruses in immunized mice. J. Immunol. 1954, 72, 24-29.
Gordon, L. E., Smith, C. E., Tompkins, M., Saito, M. T. Sensitivity of Coccidioides immitis to 2-hydroxystilbamidine and the failure of the drug in the treatment of experimental coccidioidomycosis. J. Lab. Clin. Med. 1954, 43, 942-945.
?Houser, H. B., Clark, E. J., and Stolzer, B. L. Comparative effects of aspirin, ACTH and cortisone on the acute course of rheumatic fever in young adult males. Am. J. Med. 1954, 16,168-180.
Jordan, W. S., Jr., and Oseasohn, R. O. The use of RDE to improve the sensitivity of the hemagglutination-inhibition test for the serologic diagnosis of influenza. J. Immunol. 1954, 72, 229-235.
Katz, S., Badger, G. F., Jordan, W. S., Jr., Rosenbaum, H.B., and Dingle, J. H. A study of illness in a group of Cleveland families. VI. Controlled study of reactions to oxytetracycline hydrocloride. N. Engl. J. Med. 1954, 251, 508-513.
Markowitz, H., and Heidelberger, M. Chemical constitution of the specific polysaccharide of type XVIII pneumococcus. J. Am. Chem. Soc. 1954,76, 1317-1319.
99
Markowitz, H., and Heidelberger, M. Chemical modifications of the specific polysaccharide of type III pneumococcus and their immunological effects. J. Am. Chem. Soc. 1954, 76,1313-1316.
Rammelkamp, C. H., Jr. Acute hemorrhagic glomerulonephritis. Strep. Infect. 1954, Chapter 14.
?Rammelkamp, C. H., Jr., Stetson, C. A., Krause, R. M., Perry, W. D., and Kohen, R. J. Epidemicnephritis. Trans. Assoc. Am. Physicians 1954, 67, 276-282.
?Rammelkamp, C. H., Jr., and Stolzer, B. L. The treatment and prevention of rheumatic fever. Pediatric Clin. North Am. 1954, 1, 265-274.
Smith, R. T., and Thomas L. Influence of age upon response to meningococcal endotoxin in rabbits. Proc. Soc. Exp. Biol. Med. 1954, 86,806-809.
?Stetson, C.A., Jr. The relation of antibody response to rheumatic fever. Strep. Infect. 1954,Chapter 15.
?Stolzer, B. L., Houser, H. B., and Clark, E. J. Comparative effects of aspirin, ACTH, and cortisone on the antistreptolysin "O" titer and gamma globulin concentration in rheumatic fever. J. Lab. Clin. Med. 1954, 44, 229-234.
Thomas, L., Smith, R. T., and Korff, R. V. Cold-precipitation by heparin of a protein in rabbit and human plasma. Proc. Soc. Exp. Biol. Med. 1954, 86, 813-818.
Thomas L., and Smith, R. T. Effect of cortisone on response to endotoxin in mature rabbits. Proc. Soc. Exp. Biol. Med. 1954, 86,810-813.
Tillotson, G., and Ginsberg, H. S. An antipyretic action of aureomycin. Inhibition of febrile response to influenza virus in rabbits. Proc. Soc. Exp. Biol. Med. 1954, 85, 192-197.
?Wannamaker, L. W. The epidemiology of streptococcal infections. Strep. Infect. 1954,Chapter 12.
1955
?Catanzaro, F. J., Brock, L., Chamovitz, R., Perry, W. D., Siegel, A. C., Stetson, C. A., Rammelkamp, C. H., Jr., Houser, H. B., Stolzer, B. L., Wannamaker, L. W., and Hahn, E. O. Effect of oxytetracycline therapy of streptococcal sore throat on the incidence of acute rheumatic fever. Ann. Intern. Med. 1955, 42, 345-357.
Chancey, R. L., Morris, A. J., Conner, R. H., Catanzaro, F. J., Chamovitz, R., and Rammelkamp, C. H., Jr. Studies of streptococcal prophylaxis comparison of oral penicillin and benzathine penicillin. Am. J. Med. Sci. 1955, 229, 165-171.
Denny, F. W., Jr., and Thomas, L. Persistence of group a streptococci in tissues of rabbits after infection. Proc. Soc. Exp. Biol. Med. 1955, 88, 260-263.
Dingle, J. H. Respiratory disease research. U.S. Armed Forces Med. J. 1955, 6, 1249-1264.
Dingle, J. H. Respiratory diseases caused by viruses. Mil. Med. 1955, 116, 252-258.
Dingle, J. H. The prevention of respiratory infections within families. Ann. Intern. Med. 1955, 43, 3.
Dingle, J. H., Ginsberg, H. S., Gold, E., Jordan, W. S., Jr., Katz, S., and Badger, G. F. Relationship of certain characteristics of the new respiratory viruses to the clinical and epidemiological behavior of non-bacterial pharyngitis. Trans. Assoc. Am. Physicians 1955, 67, 73-77.
Friedman, L., Smith, C. E., and Gordon, L. E. The assay of virulence of coccidioides in white mice. J. Infect. Dis. 1955, 97,311-316.
Ginsberg, H. S. Suppression of influenza viral pneumonia in mice by the non-specific action of xeros in. J. Immunol. 1955, 75,430-440.
Ginsberg, H. S., Badger, G. F., Dingle, J. H., Jordan, W. S., Jr., and Katz, S. Etiologic relationship of the RI-67 agent to "acute respiratory disease (ARD)." J. Clin. Invest. 1955, 34, 820-831.
Ginsberg, H. S., Gold, E., Jordan, W. S., Jr., Katz, S., Badger, G. F., and Dingle, J. H. Relation of the new respiratory agents to acute respiratory diseases. Am. J. Public Health 1955, 45, 915-922.
Gordon, L. E., Smith, C. E., and Wedin, D. S. Nystatin(mycostatin) therapy in experimental coccidioidomycosis. Am. Rev. Tuber. Pul. Dis. 1955, 72, 64-70.
Harford, C. G., Hamlin, A., and Parker, E. Electron microscopy of early cytoplasmic changes due to influenza virus. J. Exp. Med. 1955,101, 577-590.
100
Hilleman, M. R., Tousimis, A. J., and Werner, J. H. Biophysicalc haracterization of the RI (RI-67) viruses. Proc. Soc. Exp. Biol. Med. 1955,89, 587-593.
Hilleman, M. R., Werner, J. H., Adair, C. V., and Dreisbach, A. R. Outbreak of acute respiratory illness caused by RI-67 and influenza a viruses, Fort Leonard Wood, 1952-1953. Am. J. Hyg. 1955, 61,163-173.
Hilleman, M. R., Werner, J. H., Dascomb, H. E., and Butler, R. L. Epidemiology investigations with respiratory disease virus RI-67. Am. J. Public Health 1955, 45, 203-210.
Hilleman, M. R., Werner, J. H., Dascomb, H. E., Butler, R. L., and Stewart, M. T. Epidemiology of RI (RI-67) group respiratory virus infections in recruit populations. Am. J. Hyg. 1955, 62, 29-43.
Littell, A. S., and Smith, G. V. Interval between onsets of multiple cases of poliomyelitis in families. Am. J. Hyg. 1955, 61, 302-313.
McCorkle, L. P, Hodges, R. G., Badger, G. F., Dingle, J. H., and Jordan, W. S., Jr. A study of illness in a group of Cleveland families? VIII. Relation of tonsillectomy to incidence of common respiratory diseases in children. N. Engl. J. Med. 1955, 252, 1066-1069.
Rammelkamp, C. H., Jr. Prevention of acute nephritis. Ann. Intern. Med. 1955,43, 511-517.
?Rammelkamp, C. H., Jr. The natural history of streptococcal infections. Bull. N.Y. Acad. Med. 1955, 31,103-112.
Seal, J. R. Acute respiratory diseases in recruit training stations-etiology, prevention, and control. Mil. Med. 1955, 116, 265-277.
Siegel, A. C., Rammelkamp, C. H., Jr., and Griffeath, H. I. Epidemicnephritis in a school population. The relation of hematuria to group A streptococci. Pediatrics 1955, 15, 33-44.
Smith, C. E. Coccidioidomycosis. Ped. Clin. North Am. 1955, 2,109-125.
Stetson, C. A., Rammelkamp, C. H., Jr., Krause, R. M., Kohen, R. J., and Perry, W. D. Epidemic acute nephritis: Studies on etiology, natural history and prevention. Medicine 1955, 34, 431-450.
Thomas, L., Brunson, J., and Smith, R.T. Studies on the generalized Schwartzman reaction. VI. Production of the reaction by the synergistic action of endotoxin with three synthetic acidic polymers (sodium polyanethol sulfonate, dextran sulfate and sodium polyvinyl alcohol sulfonate). J. Exp. Med. 1955, 102, 249-261.
Thomas, L., Smith, R. T., and Korff, R. Studies on the generalized Schwartzman reaction. VII. The role of fibrinogen in the deposition of fibrinoid after combined injections of endotoxin and synthetic acidic polymer. J. Exp. Med. 1955, 102, 263-278.
1956
Dingle, J. H. Studies of respiratory and other illnesses in Cleveland (Ohio)families (summary). Proc. R. Soc. Med. 1956, 49, 259-260.
Feller, A. E., Furcolow, M. L., Larsh, H. W, Langmuir, A. D., and Dingle, J. H. Outbreak of unusual form of pneumonia at Camp Gruber, Oklahoma, in 1944. Follow-up studies implicating histoplasma capsulatum as the etiologic agent. Am. J. Med. 1956, 21, 184-192.
Fisher, T. N., and Ginsberg, H. S. The reaction of influenza viruses with guinea pig polymorphonuclear leukocytes. II. The reduction of white blood cell glycolysis by influenza viruses and receptor-destroying enzyme (RDA).Virology 1956, 2, 637-655.
Fisher, T. N., and Ginsberg, H. S. The reaction of influenza viruses with guinea pig polymorphonuclear leukocytes. III. Studies on the mechanism by which influenza viruses inhibit phagocytosis. Virology 1956,2, 656-664.
Friedman, L., Smith, C. E., Pappagianis, D., and Berman, R. J. Survival of Coccidioidesimmitis under controlled conditions of temperature and humidity. Am. J. Public Health 1956, 46, 1317-1324.
Friedman, L., and Smith, C. E. Vaccination of mice against Coccidioidesimmitis. Am. Rev. Tuber. Pul. Dis. 1956, 74, 245-248.
Friedman, L., Smith, C. E., Roessler, W. G., and Berman, R. J. The virulence and infectivity of twenty-seven strains of Coccidioidesimmitis. Am. J. Hyg. 1956,64, 198-210.
101
Ginsberg, H. S. Characteristics of the new respiratory viruses(adenoviruses). I. Qualitative and quantitative aspects of the neutralization reaction. J. Immunol. 1956, 77, 271-278.
Ginsberg, H. S. Characteristics of the new respiratory viruses(adenoviruses). II. Stability to temperature and pH alterations. Proc. Soc. Exp. Biol. Med. 1956, 93, 48-52.
Ginsberg, H. S., and Blackman, J. R. Reactions of influenza viruses with guinea pig polymorphonuclear leukocytes. I. Virus-cell interactions. Virology 1956, 2, 618-636.
Ginsberg, H. S., and Wedgwood, R. J. Inactivation of virus by the proper din system. Ann. N.Y. Acad. Sci. 1956, 66, Art. 2, 251-261.
Harford, C. G., Hamlin, A., Parker, E., and VanRavenswaay, T. Electron microscopy of HeLa cells infected with adenoviruses. J. Exp. 1956, 104, 443-454.
Harford, C. G., Hamlin, A., Parker, E., and VanRavenswaay, T. Globoid structures in the cytoplasm of rapidly growing HeLa cells. J. Biophys. Biochem. Cytology Suppl. 1956, 2, 347-350.
Heidelberger, M., and Adams, J. The immunological specificity of type II pneumococcus and its separation into partial specificities. J. Exp. Med. 1956, 103, 189-197.
Heidelberger, M., Adams, J., and Dische, Z. Fractionation of gum arabic by chemical and immunological procedures. J. Am. Chem. Soc. 1956, 78, 2853-3855.
Hodges, R. G., McCorkle, L. P, Badger, G. F., Curtiss, C., Dingle, J. H., and Jordan, W. S., Jr. A study of illness in a group of Cleveland families. XI. The occurrence of gastrointestinal symptoms. Am. J. Hyg. 1956, 64, 349-382.
Hoeprich, P D., Kent, G. T., and Dingle, J. H. Rickettsial pox. Report of aserologically proven case in Cleveland. N. Engl. J. Med. 1956, 254, 25-27.
Jordan, W. S., Jr. Human nasal cells in continuous culture. I. Establishment of two lines of epithelial-like cells. Proc. Soc. Exp. Biol. Med. 1956,92, 867-871.
Jordan, W. S., Jr., Badger, G. F., Curtiss, C., Dingle, J.H., Ginsberg, H. S., and Gold, E. A study of illness in a group of Cleveland families. X. The occurrence of adenovirus infections. Am. J. Hyg. 1956, 64, 336-348.
Jordan, W. S., Jr., Stevens, D., Katz, S., and Dingle, J. H.A study of illness in a group of Cleveland families. IX. Recognition of family epidemics of poliomyelitis and pleurodynia during a search for respiratory-disease viruses. N. Engl. J. Med. 1956, 254, 687-691.
MacLeod, C. M., and Roe, A. S. Effect of silicate on gram staining and viability of pneumococci and other bacteria. J. Exp. Med. 1956, 103, 453-463.
?Morris, A. J., Chamovitz, R., Catanzaro, F. J., and Rammelkamp, C. H., Jr. Prevention of rheumatic fever by treatment of previous streptococci infections. Effect of sulfadiazine. J. Am. Med. Assoc. 1956, 160, 114-116.
Pappagianis, C., Smith, C. E., and Kobayashi, G. S. Relationship of the invivo form of Coccidioidesimmitis to virulence. J. Infect. Dis. 1956, 98, 312-319.
Prouty, R. L., and Jordan, W. S., Jr. A family epidemic of psittacosis with occurrence of a fatal cause. A.M.A. Arch. Intern. Med. 1956, 98, 365-371.
?Rammelkamp, C. H., Jr. Streptococcalinfection in relation to rheumatic fever and nephritis. Trans. Stud. Coll. Physicians Phila. 1956, 23, 3.
Rammelkamp, C. H., Jr., and Lebovitz, J. L. The role of coagulase instaphylococcal infections. Ann. N.Y Acad. Sci. 1956, 65, 144-151.
Seibert, R. H., Jordan, W. S., Jr., and Dingle, J. H. Clinical variations in the diagnosis of psittacosis. N. Engl. J. Med. 1956, 254, 925-930.
Seibert, R. H., Williams, R. F., Jordan, W. S., Jr., Ginsberg, H. S., and Dingle, J. H. Epidemiological studies of psittacosis in Cleveland. Am. J. Hyg. 1956, 63, 28-37.
Smith, C. E. Analogy of coccidioidin and histoplasmin sensitivity. Public Health Monogr. 1956, 39(3), 173-178.
Smith, C. E., Saito, M. T., and Simons, S. A. Pattern of 39,500 serologic tests in coccidioidomycosis. J. Am. Med. Assoc. 1956, 160, 546-552.
102
Smith, R. T., Thomas, L., and Gellerman, D. G. The lethal effect of endotoxins on the chick embryo. J. Exp. Med. 1956, 104,217-231.
Thomas, L. Reversible collapse of rabbit ears after intravenous papain, and prevention of recovery by cortisone. J. Exp. Med. 1956,104(2), 245-252.
Thomas, L. The role of epinephrine in the reactions produced by the endotoxins of gram-negative bacteria. I. Hemorrhagicnecrosis produced by epinephrine in the skin of endotoxin treated rabbits. J. Exp. Med. 1956, 104, 865-880.
Wedgwood, R. J., Ginsberg, H. S., and Pillemer, L. The properdin system and immunity. VI. The inactivation of Newcastle disease virus by the properdin system. J. Exp. Med. 1956, 104, 707-725.
Zweifach, B. W., Nagler, A. L., and Thomas, L. The role of epinephrine in the reactions produced by the endotoxins of gram-negative bacteria. II. The changes produced by endotoxin in the vascular reactivity to epinephrine, in the rat mesoappendix and the isolated, perfused rabbit ear. J. Exp. Med. 1956, 104, 881-896.
1957
Boyer, G. S., Leuchtenberger, C., and Ginsberg, H. S. Cytological and cytochemical studies of HeLa cells infected with adenoviruses. J. Exp. Med. 1957, 105, 195-216.
?Denny, F. W., Jr., Perry, W D., and Wannamaker, L. W. Type-specific streptococcal antibody. J. Clin. Invest. 1957, 36, 1092-1100.
Dowling, H. F., Jackson, G. G., and Inouye, T. Transmission of the experimental common cold in volunteers. II. The effect of certain host factors upon susceptibility. J. Lab. Clin. Med. 1957, 50, 516-525.
Fisher, T. N., and Ginsberg, H. S. Accumulation of organic acids by HeLa cells infected with type 4 adenovirus. Proc. Soc. Exp. Biol. Med. 1957, 95, 47-51.
Ginsberg, H. S. Biological and physical properties of the adenoviruses. Ann. N.Y. Acad. Sci. 1957, 67, Art. 8, 383-391.
Harford, C. G., Hamlin, A., and Parker, E. Electron microscopy of HeLa cells after the ingestion of colloidal gold. J. Biophysic. Biochem. Cytol. 1957, 3, 749-756.
Jordan, W. S., Jr. The frequency of infection with adenoviruses in a family study population. Ann. N.Y. Acad. Sci. 1957, 67, Art. 9, 273-278.
Jordan, W. S., Jr. Failure to transmit human nonbacterial gastroenteritis to cats. Proc. Soc. Exp. Biol. Med. 1957, 94, 692-695.
Jordan, W. S., Jr., and Denny, F. W., Jr. Failure to transmit common cold to suckling hamsters. Proc. Soc. Exp. Biol. Med. 1957, 95, 651-653.
Katz, S., Jordan, W. S., Jr., Badger, G. F., and Dingle, J. H. Studies of complement-fixing and neutralizing antibodies against certain adenoviruses. J. Immunol. 1957, 78, 118-121.
Pappagianis, D., Smith, C. E., Saito, M. T., and Kobayashi, G. S. Preparation and property of a complement-fixing antigen from mucelia of Coccidioides immitis. Proceedings of the Symposium on Coccidiodmycosis, USPHS 1957, 57-63.
?Perry, W. D., Siegel, A.C., Rammelkamp, C. H., Jr., Wannamaker, L. W., and Marple, E. C. Transmission of group A streptococci. I. The role of contaminated bedding. Am. J. Hyg.1957, 66, 85-95.
?Perry, W. D., Siegel, A.C., and Rammelkamp, C. H., Jr. Transmission of group A streptococci II. The role of contaminated dust. J. Hyg. 1957, 66, 96-101.
Prince, A. M., Littell, A. S., and Ginsberg, H. S. Methods for quantitative bioassay of Ehrlich ascites tumor cells. J. Natl. Cancer Inst. 1957, 18, 487-506.
Prince, A. M., and Ginsberg, H. S. Immuno histochemical studies on the interaction between Ehrlich ascites tumor cells and Newcastle disease virus. J. Exp. Med. 1957, 105, 177-188.
Prince, A. M., and Ginsberg, H. S. Studies on the cytotoxic effect of Newcastle disease virus (NDV) on Ehrlich ascites tumor cells. I. Characteristics of the virus-cell interaction. J. Immunol.1957, 79, 94-106.
103
Prince, A. M., and Ginsberg, H. S. Studies on the cytotoxic effect of new castle disease virus (NDV) on ehrlich as cites tumor cells. II. The mechanism and significance of in vitro recovery from the effect of NDV J. Immunol. 1957, 79(2), 107-112.
Reen, B. M., Schalet, N., and Houser, H. B. Epidemic rheumatic fever. Problems in control at a recruit training base. U.S. Armed Forces Med. J. 1957, 8, 802-810.
Smith, C. E., and Saito, M. T. Serologic reactions in coccidioidomycosis. J. Chronic. Dis. 1957, 5, 571-579.
Smith, C. E., Saito, M. T., Campbell, C. C., Hill, G. B., Saslaw, S., Salvin, S. B., Fenton, J. E., and Krupp, M. A. Comparison of complement fixation tests for coccidioidomycosis. Public Health Rep.1957, 72, 888-894.
Smith, C. E., Pappagianis, D., and Saito, M. T. The public health significance of coccidioidomycosis. Public Health Bull. 1957, 575, 3-9.
Thomas, L., Zweifach, B. W., and Benacerraf, B. Mechanisms in the production of tissue damage and shock by endotoxins. Trans. Assoc. Am. Physicians 1957, 70, 54-63.
Wedgwood, R. J. The influence of antibodies on the activity of the properdin system. Transactions of the 6th Congress of the European Society of Haematology. 1957, 1003-1005.
1958
Boake, W. C. A study of illness in a group of Cleveland families. XVIII. Tobacco smoking and respiratory infections. N. Engl. J. Med. 1958, 259,1245-1249.
?Catanzaro, F. J., Rammelkamp, C. H., Jr., and Chamovitz, R. Prevention of rheumatic fever by treatment of streptococcal infections. II. Factors responsible for failures. N. Engl. J. Med. 1958, 259, 51-57.
Dowling, H. F., Jackson, G. G., Spiesman, I. G., and Inouye, T. Transmission of the common cold to volunteers under controlled conditions. III. The effect of chilling of the subjects upon susceptibility. Am. J. Hyg. 1958, 66, 69-65.
Everett, S. F., and Ginsberg, H. S. A toxinlike material separable from type5 adenovirus particles. Virology 1958, 6, 770-771.
Ginsberg, H. S. Characteristics of the adenoviruses. III. Reproductive cycle of types 1 to 4. J. Exp. Med. 1958, 107, 133-152.
Grieble, H. G., Jackson, G. G., Dowling, H. F., Seketa, D. H., and Anderson, T. O. The etiology of common respiratory infections in a civilian adult population. Am. J. Med. Sci. 1958, 235, 245-259.
Jackson, G. G., Dowling, H. F., and Anderson, T. O. Neutralization of common cold agents in volunteers by pooled human globulin. Science 1958, 128, 27-28.
Jackson, G. G., Dowling, H. F., Spiesman, I. G., and Boand, A. V. Transmission of the common cold to volunteers under controlled conditions. I. The common cold as a clinical entity. A.M.A. Arch. Intern. Med. 1958,101, 267-278.
Jordan, W. S., Jr., Badger, G. F., and Dingle, J. H. A study of illness in group of Cleveland families. XV. Acquisition of type-specific adenovirus antibodies in the first five years of life-implications for the use of adenovirus vaccine. N. Engl. J. Med. 1958, 258, 1041-1044.
Jordan, W. S., Jr., Badger, G. F., and Dingle, J. H. A study of illness in a group of Cleveland families. XVI. The epidemiology of influenza, 1948-1953. Am. J. Hyg. 1958, 68, 169-189.
Jordan, W. S., Jr., Denny, F. W., Jr., Badger, G. F., Curtiss, C., Dingle, J. H., Oseasohn, R., and Stevens, D. A. A study of illness in a group of Cleveland families. XVII. The occurrence of Asian influenza. Am. J. Hyg. 1958, 68, 190-212.
?Rammelkamp, C. H., Jr. The Lewis A. Conner memorial lecture. Rheumatic heart disease? A challenge. Circulation 1958, 17, 842-851.
Schalet, N., Reen, B. M., and Houser, H. B. A comparison of penicillin G and penicillin V in treatment of streptococcal sore throat. Am. J. Med. Sci. 1958, 235, 183-188.
Wedgwood, R. J. The influence of antibodies on the activity of the properdin system. Transactions of the 6th Congress of the European Society of Haematology 1957, 1003-1005.
104
Wedgwood, R. J. Concerning the nature of the properdin system. Pediatrics 1958, 22(5), 991-1000.
?(Wedgwood, R. J., and Pillemer, L. The nature and interactions of the properdin system. Int. J .Hematol. 1958, 20, 253-259.
1959
Bernstein, S. H., and Houser, H. B. Sensitivity reactions to intramuscular injection of benzathine penicillin. N. Engl. J. Med. 1959, 260, 747-751.
Boyer, G. S., Denny, F. W., Jr., and Ginsberg, H. S. Intracellular localization of type 4 andenovirus. II. Cytological and fluorescein labelled antibody studies. J. Exp. Med. 1959, 109, 85-96.
Boyer, G. S., Denny, F. W., Jr., and Ginsberg, H. S. Sequential cellular charges produced types 5 and 7 adenoviruses in HeLa cells and in human amniotic cells. J. Exp. Med. 1959, 110, 827-844.
Denny, F. W., Jr., and Ginsberg, H. S. Intracellular localization of type 4 adenovirus. I. Cellular fractionation studies. J. Exp. Med. 1959, 109, 69-83.
Ginsberg, H. S., and Dixon, M. K. Deoxyribonucleic acid (DNA)and protein alterations in HeLa cells infected with type 4 adenovirus. J. Exp. Med. 1959, 109(4), 407-422.
Hartford, C. G., Hamlin, A., and Rodermund, E. P. Some problems of electron microscopy in the study of virus-infected cells. Ann.N.Y. Acad. Sci. 1959, 81, 197-206.
Jackson, G. G., and Dowling, H. F. Transmission of the common cold to volunteers under controlled condition. IV. Specific immunity to the common cold. J. Clin. Invest. 1959, 38, 762-769.
Kaji, M., Oseasohn, R., Jordan, W. S., Jr., and Dingle, J. H. Isolation of Asian virus from extrapulmonary tissues in fatal human influenza. Proc. Soc. Exp. Biol. Med. 1959, 100, 272-275.
Katz, S., Badger, G. F., Denison, A. B., Denny, F. W., Jr., and Jordan, W.S., Jr. Search for illness due to adenovirus type 4 among college dormitory freshmen. Proc. Soc. Exp. Biol. Med. 1959, 101, 592-594.
Oseasohn, R., Adelson, L., and Kaji, M. Clinicopathologic study of thirty-three fatal cases of Asian influenza. N. Engl. J. Med. 1959, 260, 509-518.
Wedgwood, R. J. Immunity, infection, and properdin. Arch. Intern. Med. 1959, 104, 497-505.
Wedgwood, R. J. Measurement of the components of complement by the reagent titration technique. Zeitshrift fur Immunitatsforschung undExperimentelle Therapie 1959, 118, 358-367.
?Wedgwood, R. J., and Pillemer, L. The nature and interactions of the properdin system. ActaHaematol. 1959, 20, 253-259.
1960
Boyer, G. S., Denny, F. W., Jr., Miller, I., and Ginsberg, H. S. Correlation of production of infectious virus with sequential stages of cytologic alteration in HeLa cells infected with adenoviruses types 5 and 7. J. Exp. Med. 1960, 112, 865-882.
Dowling, H. F., Lepper, M. H., and Jackson, G. G. Important guides in the recognition of viral diseases of the respiratory and central nervous systems. Med. Clin. North Am. 1960, 44, 5-16.
?Hinz, C.F., Jr., Wedgwood, R. J., Todd, E. W., and Pillemer, L. The properdin system and immunity. XIV. The injection of human properdin into rabbits and the production of antibodies to properdin. J. Immunol. 1960, 85, 547-558.
Jackson, G. G., Dowling, H. F., Anderson, T.O., Riff, L., Saporta, J., and Turck, M. Susceptibility and immunity to common upper respiratory viral infections? The common cold. Ann. Intern. Med. 1960, 53, 719-738.
Jackson, G. G., and Dowling, H. F., Some common acute respiratory infections. World-Wide Abstracts of Gen. Med. 1960, 8-18.
Jackson, G. G., Dowling, H. F., and Mogabgab, W. J. Infectivity and interrelationships of 2060 and JH viruses in volunteers. J. Lab. Clin. Med. 1960, 55, 331-341.
105
James, W. E. S., Badger, G. F., and Dingle, J. H. A study of illness in a group of Cleveland families. XIX. The epidemiology of the acquisition of group A streptococci and of associated illnesses. N. Engl. J. Med. 1960, 262, 687-694.
Jordan, W. S., Jr. Activities of the Commission on Acute Respiratory Diseases. U.S. Armed Forces Med. J. 1960, 11, 1225-1229.
Jordan, W. S., Jr. Stability characteristics of Coe virus. Proc. Soc. Exp. Biol. Med. 1960, 103, 506-509.
Kunin, C. M., Emmons, L. R., and Jordan, W. S., Jr. Detection of cells of heterologous origin in tissue culture and their segregation by the use of differential media. J. Immunol. 1960, 85, 203-219.
Stonehill, R. B., Schalet, N., Fong, W. Y, Saltzman H., and Houser, H. B. Pulmonary ventilatory function in military recruits during health and acute viral respiratory disease including pneumonia. Am. Rev. Respir. Dis. 1960, 81, 315-320.
1961
Clyde, W. A., Jr. Demonstration of Eaton`s agent in tissue culture. Proc. Soc. Exp. Biol. Med. 1961, 107.
Clyde, W. A., Jr., Denny, F. W., and Dingle, J. H. Fluorescent-stainable antibodies to the Eaton agent in human primary atypical pneumonia transmission studies. J. Clin. Invest. 1961, 40, 1638-1647.
Denny, F. W., Jr., Ginsberg, H. S. Certain biological characteristics of adenovirus types 5, 6, 7 & 14. J. Immunol. 1961, 86, 567-574.
?Ginsberg, H. S. Biochemical alterations in adenovirus-infected cells. Persp. Virol.1961, 2, 58-68.
Ginsberg, H. S. Biological and biochemical basis for cell injury by animal viruses. Fed. Proc. 1961, 20, 656-660.
Ginsberg, H. S., and Dixon, M. K. Nucleic acid synthesis in types 4& 5 adenovirus-infected HeLa cells. J. Exp. Med. 1961, 113, 283-299.
Harford, C. G., and Hamlin, A. A method of electron microscopic autoradiography with tritium labeled cells in a magnetic field. Lab. Invest. 1961,10, 627-635.
Harford, C. G., and Hamlin, A. Electron microscopic autoradiography in a magnetic field. Nature 1961, 189, 505-506.
Hinz, C. F., Jr., Wedgwood, R. J., and Pillemer, L. The properdin system and immunity. XV Some biologic effects of the administration of zymosan and other polysaccharides to rabbits, and the presence of antibodies tozymosan in human and rabbit serum. J. Lab. Clin. Med. 1961, 57, 185-198.
?Jackson, G. G., Muldoon, R. L., Akers, L. W., Liu, O., Johnson, G. C., and Engel, C. Effect of N1,N1-anhydrobis-(?-hydroxyethyl) ? iguanide-hydrochloride on Asian influenza virus in volunteers. Antimicrob. Agents Chemother. 1961, 883-891.
Jordan, W. S., Jr. The mechanism of spread of Asian influenza. Am. Rev. Respir. Dis. 1961, 83(2), 29-35.
Kunin, C. M., and Jordan, W. S., Jr. In vitro adsorption of poliovirus by noncultured tissues. Effect of species, age, and malignancy. Am. J. Hyg.1961, 73, 245-257.
Smith, C. E., Pappagianis, D., Levine, H. B., and Saito, M. Humancoccidioidomycosis. Bacteriol. Rev. 1961, 25, 310-320.
Wilcox, W. C., and Ginsberg, H. S. Purification and immunological characterization of types 4 and 5 adenovirus-soluble antigens. Proc. Natl. Acad. Sci. U.S.A. 1961, 47, 512-526.
1962
Anderson, T. O., Riff, L. J. M., and Jackson, G. G. immunoelectrophoresis of nasal secretions collected during a common cold: Observations which suggest a mechanism of seroimmunity in viral respiratory infections. J. Immunol. 1962, 89, 691-697.
Clyde, W. A., Jr. A slide conveyor for use with the microtomecryostat. Stain Technol. 1962, 37, 189-192.
106
Gold, E., and Ginsberg, H. S. An inhibitor of adenoviruses in ox serum. J. Immunol. 1962, 88, 513-518.
Harford, C. G., Hamlin, A., Middelkamp, J. N., and Briggs, D. D., Jr. Electron microscopic examination of cells infected with reovirus. J. Lab. Clin. Med. 1962, 60, 179-193.
Jackson, G. G., Dowling, H. F., Akers, L. W., Muldoon, R. L., Van Dyke, A., and Johnson, G. C. Immunity to the common cold from protective serum antibody time of appearance, persistence and relation to reinfection. N. Engl. J. Med. 1962, 266, 791-796.
Jordan, W. S., Jr., Acute respiratory diseases of viral etiology. I. Ecology of respiratory viruses?1961. Am. J. Public Health 1962, 52, 897-902.
Jordan, W. S., Jr. Growth characteristics of respiratory syncytial virus. J. Immuno1. 1962, 88, 581-590.
Jordan, W. S., Jr. The Armed Forces Epidemiological Board activities of the Commission on Acute Respiratory Diseases, 1961. Mil. Med. 1962, 127, 191-194.
?Krause, R. M., Rammelkamp, C. H., Jr., Denny, F. W., Jr., and Wannamaker, L. W. Studies of the carrier state following infection with group A streptococci. I. Effect of climate. J. Clin. Invest. 1962, 41(3), 568-574.
Kunin, C. M. Virus-tissue union and the pathogenesis of enterovirus infections. J. Immunol. 1962, 88, 556-569.
McCorkle, L. F. A study of illness in a group of Cleveland families. XX. Blood groups O and A and the occurrence of certain minor illnesses. Am. J. Hyg. 1962, 75, 33-43.
Wheelock, E. F. The role of protein synthesis in the eclipse period of Newcastle disease virus multiplication in HeLa cells as studies with furomycin. Proc. Natl. Acad. Sci. U.S.A. 1962, 48, 1358-1366.
Wilcox, W. C., and Ginsberg, H. S. Effect of proflavine on the synthesis of adenovirus type 5, and associated soluble antigens. J. Bacteriol. 1962, 84, 526-533.
1963
Clyde, W. A., Jr. Hemolysis in identifying Eaton`s pleuropneumonia-like organism. Science 1963, 139(3549), 55.
Clyde, W. A., Jr. Studies on Eaton agent in tissue culture. Am. Rev. Respir. Dis. 1963, 88, 212-217.
Clyde, W. A., Jr. (Introduced by Floyd W. Denny, Jr.) Studies on growth of Eaton`s agent in tissue culture. Proc. Soc. Exp. Biol. Med. 1963, 112,905-909.
Clyde, W. A., Jr., and Denny, F. W., Jr. The etiology and therapy of atypical pneumonia. Med. Clin. North Am. 1963, 1201-1218.
Gwaltney, J. M., Jr., and Jordan, W. S., Jr. The present status of respiratory viruses. Med. Clin. North Am. 1963, 1155-1170.
Jackson, G. G., Muldoon, R. L., and Akers, L. W. Serological evidence for prevention of influenzal infection in volunteers by an anti-influenzal drug adamantanamine hydrochloride. Antimicrob. Agents Chemother. 1963, 703-707.
Jackson, G. G., Muldoon, R. L., Johnson, G. C., and Dowling, H. F. Contributions of volunteers to studies on the common cold. Am. Rev. Respir. Dis. 1963, 88, 120-127.
Jordan, W. S. The respiratory virus "explosion." Mil. Med. 1963,128, 219-223.
Kuhn, N. O., and Harford, C. G. Electron microscope autoradiography ofb acteria labeled with iodine-125. Science 1963, 141, 355-356.
Kuhn, N. O., and Harford, C. G. Electron microscopic examination of cytoplasmic inclusion bodies in cells infected with parainfluenza virus, type 2.Virology 1963, 21, 527-530.
Lefkowitz, L. B. Jr., Jackson, G. G., and Dowling, H. F. The role of immunity in the common cold & related viral respiratory infections. Med. Clin. North Am. 1963, 1171-1184.
Smith, M. R., Fleming, D. O., and Wood, W. B., Jr. The effect of acute radiation injury on phagocytic mechanisms of antibacterial defense. J. Immunol. 1963, 90, 913-924.
Wheelock, E. F. (Introduced by J. H. Dingle) Intracellular site of Newcastle disease virus nucleic acid synthesis. Proc. Soc. Exp. Biol. Med. 1963,114, 56-60.
107
Wilcox, W. C., and Ginsberg, H. S. Production of specific neutralizing antibody with soluble antigens of type 5 adenovirus. Proc. Soc. Exp. Biol. Med. 1963, 114, 37-42.
Wilcox, W. C., and Ginsberg, H. S. Structure of type 5 adenovirus. I. Antigenic relationship of virus-structural proteins to virus-specific soluble antigens for infected cells. J. Exp. Med. 1963, 118, 295-306.
Wilcox, W. C., Ginsberg, H. S., and Anderson, T. F. Structure of type 5 adenovirus. II. Fine structure of virus subunits. Morphologic relationship of structural subunits to virus-specific soluble antigens for infected cells. J. Exp. Med. 1963, 118, 307-314.
1964
Clyde, W. A., Jr. Mycoplasma species identification based upon growth inhibition by specific antisera. J. Immunol. 1964, 92, 958-965.
Dingle J. H., Badger, G. E, and Jordan, W. S., Jr. Illness in the Home: A Study of 25,000 Illnesses in a Group of Cleveland Families. Cleveland, Ohio: Western Reserve University Press, 1964, 398 pp.
Dolowy, W. C., and Muldoon, R. L. (Introduced by J. E. Kempf). Studies of germfree animals. I. Response of mice to infection with influenza A virus. Proc. Soc. Exp. Biol. Med. 1964, 116, 365-371.
Drips, W., Jr., and Smith, C. E. Epidemiology of coccidioidomycosis. J. Am. Med. Assoc. 1964, 190, 1010
Flanagan, J. F., and Ginsberg, H. S. Role of ribonucleic acid biosynthesis in multiplication of type 5 adenovirus. J. Bacteriol. 1964, 87, 977-987
Feldman, H. A., and Melnyk, C. In vitro susceptibility of sulfonamide-resistant meningococci to nalidixic and hydroxynalidixic acids. Antimicrob. Agents Chemother. 1964, 440-443.
Gwaltney, J. M., Jr., and Jordan, W. S., Jr. Rhinoviruses and respiratory disease. Bacteriol. Rev. 1964, 28, 409-422.
Jackson, G. G. Treatment of non pneumonic viral respiratory infections. Mod.Treat. 1964, 1, 877-888.
Jackson, G. G. Understanding of viral respiratory illnesses provided by experiments in volunteers. Bacteriol. Rev. 1964, 28, 423-430.
Jordan, W. S., Jr. The growth and structure of viruses. Mil. Med. 1964, 129, 497-501.
Kunin, C. M. Cellular susceptibility to enteroviruses. Bacteriol. Rev. 1964, 28, 382-390.
Miller, I. A study of illness in a group of Cleveland families. XXI. The tendency of members of a given family to have a similar number of common respiratory diseases. Am. J. Hyg. 1964, 79, 207-217.
Wheelock, E. F. Interferon in dermal crusts of human vaccinia virus vaccinations? possible explanation of relative benignity of variolation smallpox. Proc. Soc. Exp. Biol. Med. 1964, 117, 650-653.
Wheelock, E. F., and Sibley, W. A. Interferon in human serum during clinical viral infections. Lancet 1964, 22, 382-385.
1965
Carey, F. J., Kuhn, N. O., and Harford, C. G. Effects of anticellular serum on phagocytosis and the uptake of tritiated thymidine and uridine by HeLa cells. J. Exp. Med. 1965, 121, 991-1000.
Dajani, A. S., Clyde, W. A., Jr., and Denny, F.W. Experimental infection with mycoplasma pneumoniae (Eaton`s Agent). J. Exp. Med. 1965, 121, 1071-1086.
Gilead, Z., and Ginsberg, H. S. Characterization of a tumorlike antigen in type 12 and type 18 adenovirus-infected cells. J. Bacteriol. 1965, 90, 120-125.
Harford, C. G., and Hamlin, A. Electron microscopic radioautography of HeLa cells infected with adenovirus. J. Bacteriol. 1965, 89, 1540-1547.
Kenny, G. E., and Grayston, J. T. Eaton pleuropneumonia-like organism(mycoplasma pneumoniae) complement-fixing antigen: Extraction with organic solvents. J. Immunol. 1965, 95, 19-25.
Pappagianis, D., Lindsey, N. J., Smith, C. E., and Saito, M. T. (Introduced by S. S. Elberg.) Antibodies in human coccidioidomycosis: Immunoelectrophoretic properties. Proc. Soc. Exp. Biol. Med. 1965, 118, 118-122.
108
Rosenthal, M. S. Contamination of rhinovirus seed pools revealed in HEp2 cell suspension cultures. J. Gen. Microbiol. 1965, 38, 409-416.
Stanley, E. D., Muldoon, R. E., Akers, L,. W., and Jackson, G. G. Evaluation of antiviral drugs: The effect of amantadine on influenza in volunteers. Ann. N.Y. Acad. Sci. 1965, 130, 44-51.
Svec, K. H., and Dingle, J. H. The occurrence of rheumatoid factor in association with antibody response to influenza A2 (Asian) virus. Arthritis Rheum. 1965, 8, 524-529.
Wheelock, E. F. Interferon-like virus-inhibitor induced in human leukocytes by phytohemagglutinin, Science 1965, 149(3681), 310-311.
Wheelock, E. F., and Sibley, W. A. Circulating virus, interferon and antibody after vaccination with the 17-D strain of yellow-fever virus. N. Engl. J. Med. 1965, 273, 194-198.
1966
Alexander, E., Russell, M. D., Foy, H. M., Kenny, G. E.,Kronmal, R. A., McMahan, R., Clarke, E. R., MacColl, W. A., and Grayston, J. T. Pneumonia due to mycoplasma pneumoniae? its incidence in the membership of a cooperative medical group, N. Engl. J. Med. 1966,275, 131-136.
Bahrani, M., Boxerbaum, B., Gilger, A. P, Rosenthal, M. S., Teree, T. M., Generalized herpes simplex and hypoadrenocorticism? a case associated with adrenocortical insufficiency in a prematurely born male: Clinical, virologic, ophthalmological, and metabolic studies. Am. J. Dis. Child 1966, 111, 437-445.
Dowling, H. F. Human experimentation in infectious diseases. J. Am. Med. Assoc. 1966, 198, 997-999.
Edelman, R., and Wheelock, E. E Vesicular stomatitis virus replication inhuman leukocyte cultures: Enhancement by phytohemagglutinin. Science 1966,154, 1053-1055.
Feldman, H. A. Meningococcal disease 1965. J. Am. Med. Assoc. 1966,196, 391-393.
Feldman, H. A. Recent developments in the therapy and control of meningococcal infections. Dis. Mon. 1966, 1-31.
Foy, H. M., Grayston, J. T., Kenny, G. E., Alexander, E. R., and McMahan, R. Epidemiology of mycoplasma pneumoniae infection in families. J. Am. Med. Assoc. 1966, 197, 859-866.
Foy, H. M., Kenny, G. E., and Koler, J. Mycoplasma pneumonia in Stevens-Johnson`s syndrome. Lancet 1966, 550-551.
Gilead, Z., and Ginsberg, H. S. Comparison of the rates of ultraviolet inactivation of the capacity of type 12 adenovirus to infect cells and to induce T antigen formation. J. Bacteriol. 1966, 92, 1853-1854.
Gwaltney, J. M., Jr. Micro-neutralization test for identification of rhinovirus serotypes (31345). Proc. Soc. Exp. Biol. Med. 1966, 122, 1137-1141.
Gwaltney, J. M., Jr., Hendley, J. O., Simon, G., and Jordan, W. S., Jr. Rhinovirus infections in an industrial population. I. The occurrence of illness. N. Engl. J. Med. 1966, 275, 1261-1268.
Gwaltney, J. M., Jr., and Jordan, W. S., Jr. Rhinoviruses and respiratory illnesses in university students. Am. Rev. Respir. Dis. 1966, 93, Part 1, 362-371.
Harford, C. G., Hamlin, A., and Rieders, E. Electron microscopic autoradiography of INA synthesis in cells infected with vaccinia virus. Exp. Cell Res. 1966, 42, 50-57.
Jao, R. L., Rubenis, M., and Jackson, G. G. Isolation of mycoplasmapneumoniae from adults with respiratory infections. Arch. Intern. Med. 1966, 117, 520-526.
Kim, K. S., Clyde, W. A., Jr., and Denny, F. W. Physical properties of human mycoplasma species. J. Bacteriol. 1966, 92, 214-219.
Lefkowitz, L. B., Jr., and Jackson, G. G. Dual respiratory infection with para influenza and rhinovirus. The pathogenesis of transmitted infection in volunteers. Am. Rev. Respir. Dis. 1966, 93, 519-528.
Rice, R. P., and Loda, F. A roentgenographic analysis of respiratory syncytial virus pneumonia in infants. Radiology 1966, 87, 1021-1027.
Stanley, E. D., and Jackson, G. G. Viremia in Asian influenza. Trans. Assoc. Am. Physicians 1966, 74, 376-387.
Warren, K. S., and Dingle, J. H. A study of illness in a group of Cleveland families. XXII. Antibodies to Toxoplasma gondii in 40 families observed or ten years. N. Engl. J. Med. 1966, 274, 993-997.
109
Wheelock, E. F. Virus replication and high-titered interferon production inhuman leukocyte cultures inoculated with Newcastle disease virus. J. Bacteriol. 1966, 92, 1415-1421.
Wheelock, E. F. The effects of nontumor viruses on virus-induced leukemia in mice: Reciprocal interference between Sendai virus and Friend leukemia virus in DBA/2 mice. Proc. Natl. Acad. Sci. 1966, 55,774-780.
1967
Carey, F. J., and Pettengill, O. S. A time-lapse study of effects of anticellular antibody on membrane mobility and phagocytic activity of HeLa cells. J. Cell Biol. 1967, 33, 709-712.
Clyde, W. A., Jr., and Kim, K. S. Part VI. Mycoplasma from human respiratory and urogenital tracts, biophysical characterization of human mycoplasma species. Ann. N.Y. Acad. Sci. 1967, 143, Art. 1, 425-435.
Deeb, B. J., and Kenny, G. E. Characterization of mycoplasma pulmonis variants isolated from rabbits. I. Identification and properties of isolates. J. Bacteriol. 1967, 93, 1416-1424.
Deeb, B. J., and Kenny, G. E. Characterization of mycoplasma pulmonis variants isolated from rabbits. II. Basis for differentiation of antigenic subtypes. J. Bacteriol. 1967, 93, 1425-1429.
Edelman, R., and Wheelock, E. F. Specific role of each human leukocyte type in viral infections. I. Monocyte as host cell for vesicular stomatitis virus replication in vitro. J. Virol. 1967, 1, 1139-1149.
Feldman, H. A. Sulfonamide-resistant meningococci. Ann. Rev. Med. 1967, 18, 495-506.
Fernald, G. W., Clyde, W. A., Jr., and Denny, F. W., Jr. Factors influencing growth inhibition of mycoplasma pneumoniae by immune sera (32391). Proc. Soc. Exp. Biol. Med. 1967, 126, 161-166.
Fernald, G. W., Clyde, W. A., Jr., and Denny, F. W., Jr. Nature of the immune response to mycoplasma pneumoniae. J. Immunol. 1967, 98, 1028-1038.
Glezen, W. P., Clyde, W. A., Jr., Senior, R., Shaeffer, C.I., and Denny, F. W. Group A streptococci, mycoplasmas, and viruses associated with acute pharyngitis. J. Am. Med. Assoc. 1967, 202, 455-460.
Greenfield, S., and Feldman, H. A. Familial carriers and meningococcal meningitis. N. Engl. J. Med. 1967, 277, 497-502.
Gwaltney, J. M., Jr., Hendley, J. O., Simon, G., Jordan, W. S., Jr. Rhinovirus infections in an industrial population. II. Characteristics of illness and antibody response. J. Am. Med. Assoc. 1967, 202, 494-500.
**Heggie, A. D. Intrauterine infection in maternal rubella. J. Pediatr. 1967, 71, 777-782.
Inkley, S. R., and Oseasohn, R. O. A study of illness in a group of Cleveland families. XXIII. Ventilatory function in young adults a decade after repeated wheezing in childhood. Am. Rev. Respir. Dis. 1967, 96, 408-410.
Keck, C. W., and Rosenthal, M. S. The cytopathic effects of HGP virus and coxsackievirus B type 5 on HEp2 cells. J. Gen. Virol. 1967, 1, 239-242.
Lawrence, W. C., and Ginsberg, H. S. Intracellular uncoating of type 5adenovirus deoxyribonucleic acid. J. Virol. 1967, 1, 851-867.
Levine, A. J., and Ginsberg, H. S. Mechanism by which fiber antigen inhibits multiplication of type 5 adenovirus. J. Virol. 1967, 1, 747-757.
Muldoon, R. L., and Jackson, G. G. Antibody response in rabbits to antigenic stimulation during amantadine treatment (32359). Proc. Soc. Exp. Biol. Med. 1967, 126, 26-30.
Pappagianis, D., Levine, H. B., and Smith, C. E. Further studies on accination of human volunteer with killed coccidioides immitis. Coccidioidomycosis 1967, 201-210.
Pappagianis, D., Maibach, H., and Smith, C. E. Microscopic characteristics o fthe cutaneous reaction to coccidioidin in humans. Am. Rev. Respir. Dis. 1967, 95, 317-319.
Pappagianis, D., Smith, C. E., and Campbell, C. C. Serologic status after positive coccidioidin skin reactions. Am. Rev. Respir. Dis. 1967, 96, 520-523.
Simon, G., and Jordan, W. S., Jr. Infectious and allergic aspects of bronchiolitis. J. Pediatr. 1967, 70, 533-538.
110
Slotkin, R. I., Clyde, W A., Jr., and Denny, F. W. The effect of antibioticson mycoplasma pneumoniae in vitro and in vivo. Am. J. Epidemiol. 1967, 86, 225-237
1968
Beckman, B. L., and Kenny, G. E. Immunochemical analysis of serologically active lipids of mycoplasma pneumoniae. J. Bacteriol. 1968, 96, 1171-1180.
Clyde, W. A., Jr. An experimental model for human mycoplasma disease. Yale J. Biol. Med. 1968, 40, 436-442.
Dingle, J. H., and Langmuir, A. D. Epidemiology of acute respiratory disease in military recruits. Am. Rev Respir. Dis. 1968, 97, Part 2, 1-65.
Edelman, R., and Wheelock, E. F. Enhancement of replication of vesicular stomatitis virus in human lymphocyte cultures treated with heterologousanti-lymphocyte serum. Lancet 1968 (April 13), 771-775.
Edelman, R., and Wheelock, E. F. Specific role of each human leukocyte typein viral infections. II. Phytohemagglutinin-treated lymphocytes as host cells for vesicular stomatitis virus replication in vitro. J. Virol. 1968, 2, 440-448.
Gilead, Z., and Ginsberg, H. S. Characterization of the tumor-like (T) antigen induced by type 12 adenovirus. I. Purification of the antigen from infected kb cells and a hamster tumor cell line. J. Virol. 1968, 2, 7-14.
Gilead, Z., and Ginsberg, H. S. Characterization of the tumor-like (T)antigen induced by type 12 adenovirus. II. Physical and chemical properties. J. Virol. 1968, 2, 15-20.
Gwaltney, J. M., Jr., Hendley, J. O., Simon, G., and Jordan, W. S., Jr. Rhinovirus infections in an industrial population. III. Number and prevalence of serotypes. Am. J. Epidemiol. 1968, 87, 158-166.
Lepow, M. L., Balassanian, N., Emmerich, J., Roberts, R. B., Rosenthal, M.S., and Wolinsky, E. Interrelationships of viral, mycoplasmal, and bacterial agents in uncomplicated pneumonia. Am. Rev. Respir. Dis. 1968, 97, 533-545
Levine, A. J., and Ginsberg, H. S. Role of adenovirus structural proteins in the cessation of host-cell biosynthetic functions. J. Virol. 1968, 2,430-439.
Loda, F. A., Clyde, W. A., Jr., Glezen, W. P., Senior, R. J., Shaeffer, C. I., and Denny, F. W., Jr. Studies on the role of viruses, bacteria and M. pneumoniae as causes of lower respiratory tract infections in children. J. Pediatr. 1968, 72, 161-176.
?Pierce, W. E., Rosenbaum, M. J., Edwards, E. A., Peckinpaugh, R. O., and Jackson, G. G. Live and inactivated adenovirus vaccines for the prevention of acute respiratory illness in Naval recruits. Am. J. Epidemiol. 1968, 87, 237-246.
Rosenbaum, M. J., Deberry, P., Sullivan, E. J., Edwards, E.A., Pierce, W. E., Muldoon, R. L., Jackson, G. G., and Peckinpaugh, R. O. Characteristics of vaccine-induced and natural infection with adenovirus type 4in Naval recruits. Am. J. Epidemiol. 1968, 88, 45-54.
Saliba, G. S., Franklin, S. L., and Jackson, G. G. ECHO-11 as a respiratory virus: Quantitation of infection in man. J. Clin. Invest. 1968, 47,1303-1313.
Tremonti, L. P, Lin, J-S. L., and Jackson, G. G. Neutralizing activity in nasal secretions and serum in resistance of volunteers to parainfluenza virus type 2. J. Immunol. 1968, 101, 572-577.
Wheelock, E. F., Larke, R. P. B., and Caroline, N. L. Interference in human viral infections: Present status and prospects for the future. Prog. Med.Virol. 1968, 10, 286-347.
Wheelock, E. F., Schenker, S., and Combes, B. Absence of circulatingi nterferon in patients with infectious and serum hepatitis (32989). Proc.Soc. Exp. Biol. Med. 1968, 128, 251-253.
1969
Collier, A. M., Clyde, W. A., Jr., and Denny, F W. Biologic effects of mycoplasma pneumoniae and other mycoplasmas from man on hamster tracheal organ culture (34385). Proc. Soc. Exp. Biol. Med. 1969, 132, 1153-1158.
111
Fernald, G. W. Immunologic aspects of experimental mycoplasma pneumoniae infection. J. Infect. Dis. 1969, 119, 255-266.
Hackenthal, E. Distribution of keto-deoxyoctonic acid and sialic acid in N. meningitidis. J. Immunol. 1969, 102, 1099-1102.
Kenny, G. E. Serological comparison of ten glycolytic mycoplasma species. J.Bacteriol. 1969, 98(3), 1044-1055.
Lipman, R. P, and Clyde, W. A., Jr. The interrelationship of virulence, cytadsorption, and peroxide formation in mycoplasma pneumoniae (34061). Proc. Soc. Exp. Biol. Med. 1969, 131, 1163-1167.
Lipman, R. P., Clyde, W. A., Jr., and Denny, F. W. Characteristics of virulent, attenuated, and avirulent mycoplasma pneumoniae strains. J. Bacteriol.1969, 100, 1037-1043.
Mueller, R. E., Muldoon, R. L., and Jackson, G. G. Communicability of enteric live adenovirus type 4 vaccine in families. J. Infect. Dis. 1969, 119,60-66.
1970
Dowling, J. N., and Feldman, H. A. Quantitative biological assay of bacterial endotoxins. Proc. Soc. Exp. Biol. Med. 1970, 134, 861-864
Fernald, G. W., and Clyde, W. A., Jr. Protective effect of vaccines in experimental mycoplasma pneumoniae disease. Infect. Immun. 1970, 1, 559-565.
Gale, J. L., and Kenny, G. E. Complement dependent killing of mycoplasmapneumoniae by antibody: Kinetics of the reaction. J. Immunol. 1970, 104, 1175-1183.
Gwaltney, J. M., Jr. Rhinovirus inhibition by 3-substituted triazinoindoles(34642). Proc. Soc. Exp. Biol. Med. 1970, 133, 1148-1154.
Jao, R. L., Wheelock, E. F., and Jackson, G. G. Production of interferon in volunteers infected with Asian influenza. J. Infect. Dis. 1970, 121, 419-426.
Pappagianis, D. Epidemiology of coccidioidomyccsis. Proceedings of the International Symposium on Mycosis (Scientific Publication PAHO) 1970, 205, 195-200.
?Roberts, R. B. The interaction in vitro between group B meningococci and rabbit polymorphonuclear leukocytes, demonstration of type specific opsonins and bactericidins. J. Exp.Med. 1970, 126, 795-818.
Roberts, R. B. The relationship between group A and group C meningococcalpolysaccharides and serum opsonins in man. J. Exp. Med. 1970, 131, 499-513.
Velicer, L. F., and Ginsberg, H. S. Synthesis, transport, and morphogenesisof type 5 adenovirus capsid proteins. J. Virol. 1970, 5, 338-352.
1971
Caudill, R. G., Smith, C. E., and Reinarz, J. A. Coccidioidal meningitis. Am. J. Med. 1971, 49, 360-365.
Clyde, W. A., Jr. Immunopathology of experimental mycoplasma pneumoniae disease. Infect. Immun. 1971, 4, 757-763.
Clyde, W. A., Jr. Mycoplasma pneumoniae pneumonia. Mil. Med. 1971, 136, 20-22.
Collier, A. M., Clyde, W. A., Jr., and Denny, F. W., Jr. Mycoplasma pneumoniae in hamster tracheal organ culture: Immunofluorescent and electron microscopic studies (35313). Proc. Soc. Exp. Biol. Med. 1971, 136, 569-573.
Collier, A. M., and Clyde, W. A., Jr. Relationships between mycoplasmapneumoniae and human respiratory epithelium. Infect. Immun. 1971, 3, 694-701.
Denny, E W., Jr., Clyde, W. A., Jr., and Glezen, W. P. Mycoplasma pneumoniaedisease: Clinical spectrum, pathophysiology, epidemiology, and control. J. Infect. Dis. 1971, 123, 74-89.
Dowling, J. N., Sheehe, P. R., and Feldman, H. A. Pharyngeal pneumococcal acquisitions in "normal" families: A longitudinal study. J. Infect. Dis. 1971, 124, 9-16.
Eickhoff, T. C. In-vitro and in-vivo studies of resistance to rifampin in meningococci. J. Infect. Dis. 1971, 123, 414-420.
112
Eickhoff, T. C. Rifampin and meningococci: The price of prophylaxis. Mil.Med. 1971, 136(4).
Eickhoff, T. C. Sero-epidemiologic studies of meningococci infection with the indirect hemagglutination test. J. Infect. Dis. 1971, 123, 519-525.
Glezen, W. P., Loda, F. A., Clyde, W. A., Jr., Senior, R. J., Shaeffer, C. I., Conley, W. G., and Denny, F. W., Jr. Epidemiologic patterns of acute lower respiratory disease of children in a pediatric group practice. J. Pediatr. 1971, 78, 397-406.
Greenfield, S., Sheehe, P. R., and Feldman, H. A. Meningococcal carriage in a population of "normal" families. J. Infect. Dis. 1971, 123, 67-73.
Gwaltney, J. M., Jr. Virology of middle ear. Ann. Otol. Rhinol. Laryngol. 1971, 80, 365.
Pappagianis, D. Coccidioidomycosis. Immunological Diseases. 1971, 2nd Edition, 652-659.
Zweiman, B., Pappagianis, D., Maibach, H., and Hildreth, E. A. Effect of measles immunization on tuberculin hypersensitivity and in vitro lymphocytereactivity. Int. Arch. Allergy. Appl. Immunol. 1971, 40, 834-841.
1972
Collier, A. M. Pathogenesis of mycoplasma pneumoniae infection as studied in the human foetal trachea in organ culture. Pathogenic Mycoplasmas 1972, 25-27, 307-320.
Ensinger, M. J., and Ginsberg, H. S. Selection and preliminary characterization of temperature-sensitive mutants of type 5 adenovirus. J. Virol. 1972, 10(3), 328-339.
*Feldman, H. A. Meningococcal infections. Adv. Intern. Med. 1972, 18, 117-140.
Feldman, H. A. Some Recollections of the Meningococcal diseases. J. Am. Med. Assoc. 1972, 220(8), 1107-1112.
Fernald, G. W. In vitro response of human lymphocytes to mycoplasmapneumoniae. Infect. Immun. 1972, 5(4), 552-558.
Fernald, G. W., Clyde, W. A., Jr., Bienenstock, J. Immunoglobulin-containing cells in lungs of hamsters infected with mycoplasma pneumoniae. J. Immunol.1972, 108(5), 1400-1408.
Goldschneider, I., Lepow, M. L., Gotschlich, E. C. Immunogenicity of the group a and group c meningococcal polysaccharides in children. J. Infect. Dis. 1972, 125(5), 509-519.
Goldstein, E., Winship, M. J., and Pappagianis, D. Ventricular fluid and the management of coccidiodal meningitis. Ann. Intern. Med. 1972, 2, 243-246.
Hendley, J. O., Edmondson, W. P, Jr., and Gwaltney, J. M., Jr. Relation between naturally acquired immunity and infectivity of two rhinoviruses involunteers. J. Infect. Dis. 1972, 125(3), 243-248.
Hendley, J. O., Fishburne, H. B., and Gwaltney, J. M., Jr. Coronavirus infections in working adults. Am. Rev. Respir. Dis. 1972, 105, 805-811.
Kenny, G. E., Wentworth, B. B., Beasley, R. P., and Foy, H. M. Correlation of circulating capsular polysaccharide with bacteremia in pneumococcal pneumonia. Infect. Immun. 1972, 6(4), 431-437.
Pappagianis, D., Siato, M., and Van Hoosear, K. H. Antibody in cerebrospinal fluid in non-meningitic coccidiodomycosis. Sabouraudia 1972, 10, 173-179.
Werner, S. B., Pappagianis, D. H. I., and Mickel, A. An epidemic of coccidiodomycosis among archeology students in northern California. N. Engl. J. Med. 1972, 286(9), 507-512
Wilheim, J. M., and Ginsberg, H. S. Synthesis in vitro of type 5 adenoviruscapsid proteins. J. Virol. 1972, 9(6), 973-980.
Williams, R. B., III, and Gwaltney, J. M., Jr. Allergic rhinitis or virus cold? Nasal smear eosinophilia in differential diagnosis. Ann. Allergy 1972, 30, 189-194
1973
Calhoun, A. M., Jordan, W. S., Jr., and Gwaltney, J. M., Jr. Rhinovirus infections in an industrial population. V. Change in distribution of serotypes. Am.J. Epidemiol. 1973, 99(1), 58-64.
Clyde, W. A., Jr., and Thomas, L. A. Session III. Model systems, models of mycoplasma pneumoniae infection. J. Infect. Dis. 1973, 127, 817-822.
113
Collier, A. M., and Baseman, J. B. Organ culture techniques with mycoplasma. Ann.N.Y. Acad. Sci. 1973, 225, 277-289.
Collins, M., and Pappagianis, D. Effects of lysozyme and chitinasse on thespherules of Coccidioides immitis in vitro. Infect. Immun. 1973, 7, 817-822.
Fernald, G. W. Role of host-response in mycoplasma pneumoniae disease. J. Infect. Dis. 1973, 127, S55-S58.
Fernald, G. W., and Glezen, W. P. Humoral and cellular immune responses to an inactivated mycoplasma pneumoniae vaccine in children. J. Infect. Dis. 1973, 127, 498-504.
Glezen, W. P, and Denny, F. W. Medical progress, epidemiology of acute lower respiratory disease in children. N. Engl. J. Med. 1973, 288, 498-505.
Ibrahim, A. B., and Pappagianis, D. Experimental induction of energy to coccidioidin by antigens of Coccidioides immitis. Infect. Immun. 1973, 7, 786-794.
Merrill, C. W., Gwaltney, J. M., Jr., Hendley, J. O., and Sande, M. A. Rapid identification of pneumococci. N. Engl. J. Med. 1973, 288, 510-512.
Pappagianis, D., Vanderlip, J., and May, B. Coccidioidomycosis naturally acquired by a monkey, Cercocebus Atys, in Davis, California. Sabouraudia 11,1973, 52-55.
Werner, S. B., and Pappagianis, D. Coccidioidomycosis in northern California. An outbreak among archeology students near Red Bluff. J. Calif. Med. Assoc. 1973, 119, 16-20.
Commission on Air-borne Infections
1941-1943
Harris, T. N., and Stokes, J., Jr. Air-borne cross-infection in the case of the common cold. A further clinical study of the use of glycol vapors for air sterilization. Am. J. Med. Sci. 1943, 206, 631-636.
Lemon, H. M. A method for collection of bacteria from air and textiles. Proc. Soc. Exp. Biol. Med. 1943, 54, 298-301.
Loosli, C. G., Lemon, H. N., Robertson, O. H., and Appel, E.Experimental air-borne influenza infection. I. The influence of humidity onsurvival of virus in air. Proc. Soc. Exp. Biol. Med. 1943, 53, 205-206.
Moulton, S., Puck, T. T., and Lemon, H. M. An apparatus for determination of the bacterial content of air. Science 1943, 97, 51-52.
Puck, T. T., Robertson, O. H., and Lemon, H. M. The bactericidal action of propylene glycol vapor on microorganisms suspended inair. II. The influence of various factors on the activity of the vapor. J. Exp. Med., 1942, 78, 387-406.
Robertson, O. H., Bigg, E., Puch, T. T., Miller, B. F., and Baker, Z. Sterilization of Air by Means of Germicidal Aerosol Mists andVapors. Publication No. 17 of The American Association for the Advancemen tof Science, "Aerobiology." Washington, D.C.,1942, 271-280.
Robertson, O. H. Air-borne infection. Science 1943, 97, 495-502.
Robertson, O. H. Sterilization of air with glycol vapors. Harvey Lect. 1942-43,38, 227-254.
Robertson, O. H., Puch, T. T., Lemon, H. F., and Loosli, C. G. The lethal effect of triethylene glycol vapor on air-borne bacteria and influenza virus. Science1943, 97, 142-144.
Wise, H., Puck, T. T., and Stral, H. M. Rapid colorimetric method for the determination of glycols in air. J. Biol. Chem. 1943, 150, 61-67.
1944
Hamburger, M., Jr. Studies on the transmission of hemolytic streptococcus infections. I. Cross infections in army hospital wards. J. Infect. Dis. 1944,75, 58-70.
114
Hamburger, M., Jr. Studies on the transmission of hemolytic streptococcus infections. II. Beta hemolytic streptococci in the saliva of persons with positive throat cultures. J. Infect. Dis. 1944, 75, 71-78.
Hamburger, M., Jr., Puck, T. T., Hamburger, V G., Johnson, M. A. Studies on the transmission of hemolytic streptococcus infections. III. Hemolyticstreptococci in the air, floor dust, and bedclothing of hospital wards and the irrelation to cross infection. J. Infect. Dis. 1944, 75, 79-94.
Hamburger, M., Jr., Hilles, C. H., Hamburger, V G., Johnson, M. A., and Wallin, J. G. Ability of different types of hemolytic streptococci to produce scarlet fever. J. Am. Med. Assoc. 1944, 124 , 564-566
Hilles, C. H., and Hamburger, M., Jr. Experience with the slide agglutination and the capillary precipitin methods for typing hemolytic streptococci. J. Infect. Dis. 1944, 75, 265-270.
Lemon, H. M., and Wise, H. A flowmeter for use in air sampling procedures. Science 1944, 99, 43-44.
Lemon, H. M., Wise, H., and Hamburger, M., Jr. Bacterialcontent of air in Army barracks. Results of a study with special reference to dispersion of bacteria by the air circulation system procedures. Science 1944, 99, 43-44.
Puck, T. T., Wise, H., and Robertson, O. H. A device for automatically controlling the concentration of glycol vapors in the air. J. Exper.Med. 1944, 80, 377-381.
Robertson, O. H., Hamburger, M., Jr., Loosli, C. G., Puck, T. T., Lemon, H.M., and Wise H. A study of the nature and control of air-borne infection in army camps. J. Am. Med. Assoc. 1944, 126, 993-1000.
Robertson, O. H., Puck, T. T., Loosli, C. G., Hamburger, M., Jr., Lemon, H.M., and Wise, H. A new approach to the control of airborne infection. Trans. Assoc. Am. Physicians 1944, 58, 171-174.
1945
Hamburger, M., Jr., Puck, T. T., and Robertson, O. H. The effect of triethylene glycol vapor on airborne beta hemolytic streptococci in hospital wards. I. J. Infect. Dis. 1945, 76, 208-215.
Hamburger, M., Jr., Robertson, O. H., and Puck, T. T. The present status of glycol vapors in air sterilization. Am. J. Med. Sci. 1945, 209, 162-166.
Hamburger, M., Jr., Green, M. J., and Hamburger, V. G. The problem of the "dangerous carrier" of hemolytic streptococci. II. Spread of infection by individuals with strongly positive nose cultures who expelled large numbers of hemolytic streptococci. J. Infect. Dis. 1945, 77, 96-108.
Hamburger, M., Jr., Hurst, V, Robertson, O. H., and Puck, T.T. The effect of triethylene glycol vapor on air-borne beta hemolytic streptococci in hospital wards. III. The action of glycol vapors at low relative humidities. J. Infect. Dis. 1945, 77, 177-180.
Hamburger, M., Jr., Green, M. J., and Hamburger, V. G. The problem of the "dangerous carrier" of hemolytic streptococci. I. Number of hemolytic streptococci expelled by carriers with positive and negative nose cultures. J. Infect. Dis. 1945, 77, 68-81.
Harris, T. N., and Stokes, J., Jr. Summary of a 3-year study of the clinical applications of the disinfection of air by glycol vapors. Am. J. Med. Sci. 1945, 209, 152-156.
Loosli, C. G., and Robertson, O. H. Recent studies on the control of dust-borne bacteria by treatment of floors and bedclothes with oil. Am. J. Med. Sci. 1945, 209, 166-172.
Puck, T. T., Hamburger, M., Jr., Robertson, O. H., and Hurst, V. The effect of triethylene glycol vapor on air-borne beta hemolytic streptococci in hospital wards. II. The combined action of glycol vapor and dust control measures. J. Infect. Dis. 1945, 76, 216-225.
1946
Hamburger, M., Jr., and Green, M. J. The problem of the dangerous carrier of hemolytic streptococci. IV. Observations upon the role of the hands, of blowing the nose, of sneezing, and of coughing in the dispersal of these micro-organisms. J. Infect. Dis., 1946, 79, 33-44
115
Hamburger, M., Jr., and Lemon, H. M. The problem of the dangerous carrier of hemolytic streptococci. III. The chemotherapeutic control of nasal carriers .J. Am. Med. Assoc. 1946, 130, 836-841
Hamburger, M., Jr., Mattman, L. H., Grosch, D. S., and Hurst, V. Susceptibility to sulfadiazine of hemolytic streptococci recovered in army camps. Am. J. Med. 1946, 1, 23-27
Lemon, H. M., and Hamburger, M., Jr. Missed cases and contact carriers among nasal carriers of beta hemolytic streptococci. J. Immunol. 1946,54, 189-196
Loosli, C. G., Wise, H., Lemon, H. M., Puck, T. T., and Robertson, O. H. The oil treatment of bedclothes for the control of dust-borne infection. II. The use of triton oil emulsion (T-13) as a routine laundry procedure. Am. J. Hyg. 1946, 43, 105-119
Puck, T. T., Robertson, O. H., Wise, H., Loosli, C. G., and Lemon, H. M. The oil treatment of bedclothes for the control of dust-borne infection. I. Principles underlying the development and use of a satisfactory oil-in-water emulsion. Am. J. Hyg. 1946, 43, 91-104
Puck, T. T. The dispersal and control of triethylene glycol vapor for aerial disinfection. Industrial Hyg. Assoc. Quarterly 1946, 7(3), 10-16
Puck, T. T. and Wise, H. Studies in vapor-liquid equilibria. I. A new dynamic method for the determination of vapor pressures of liquids. J. Phys. Chem. 1946, 50, 329-339
1947
Hamburger, M., Jr. Transfer of beta hemolytic streptococci by shaking hands. Am. J. Med. 1947, II, 23-25.
Loosli, C. G. Dust and its control as a means of disinfection of air. Am. J. Public Health 1947, 37, 353-359.
Loosli, C. G., Smith, M. H. D., Gauld, R. L., Robertson, O.H., and Puck, T. T. Control of cross-infections in infants` wards by the use of triethylene glycol vapor. Am. J. Public Health 1947, 37, 1385-1398.
Puck, T. T. The mechanism of aerial disinfection by glycols and other chemical agents. I. Demonstration that the germicidal action occurs through the agency of the vapor phase. II. An analysis of the factors governing the efficiency of chemical disinfection of the air. J. Exp. Med. 1947, 85, 729-757.
Robertson, O. H. New methods for the control of air-borne infection with especial reference to the use of triethylene glycol vapor. Wis. Med. J. 1947, 46, 311-317.
Robertson, O. H., Loosli, C. G., Puck, T. T., Wise, H., Lemon, H. M., and Lester, W., Jr. Tests for the chronic toxicity of propylene glycol and triethylene glycol on monkeys and rats by vapor inhalation and oral administration. J. Pharmacol. Exp. They. 1947, 91, 52-76.
1948
Lemon, H. M., Loosli, C. G., and Hamburger, M., Jr. The transmission and control of respiratory diseases in army barracks. II. The spread of hemolytic streptococcal infections among enlisted personnel. J. Infect. Dis. 1948, 82, 72-85.
Loosli, C. G., Lemon, H. M., Wise, H., and Robertson, O. H. Studies on the transmission and control of respiratory disease within army barracks. I. Hemolytic streptococcal contamination of the environment. J. Infect. Dis. 1948, 82, 59-71.
1949
Hamburger, M., Jr., Lemon, H.M., and Platzer, R.F. The significance of nose to throat carrier ratios in the epidemiology of hemolytic streptococcal infection. Am. J. Hyg. 1949, 62, 99-104.
Wise, H. Dispersal of triethylene glycol vapor with aerosol bombs. Indust. Engin. Chem. 1949, 41, 633-635.
116
1951
Smith, M.H.D., Loosli, C.G., and Ritter, M.H. Outbreak of aerobacterinfection on infants` wards. Pediatrics 1951, 7, 550-562.
1952
Lemon, H. M., Loosli, C. G., Wise, H., and Puck, T. T. Transmission and control of respiratory disease in army barracks. III. The suppression of dust-borne bacteria by oiling floors and bedclothes. J. Infect. Dis. 1952, 90, 141-152.
Loosli, C. G., Lemon, H. M., Robertson, O. H., and Hamburger, M. Transmission and control of respiratory disease in army barracks. IV. The effect of oiling procedures on the incidence of respiratory diseases and hemolytic streptococcal infections. J. Infect. Dis. 1952, 90, 153-164.
1953
Hamburger, M., and Lemon, H. M. The failure of antistreptolysin to protect against streptococcal infection. J. Lab. Clin. Med. 1953, 42, 1, 140-144.
Commission on Meningcoccal Meningitis
1941-1943
Kuhns, D. M., and Feldman, H. A. Laboratory methods used in determining the value of sulfadiazine as a mass prophylactic against meningococcic infections. Am. J. Public Health 1943, 33, 1451-1465.
Kuhns, D. M., Nelson, C. T., Feldman, H. A., and Xuhn, L. R. The prophylactic value of sulfadiazine in the control of meningococcic meningitis. J. Am. Med. Assoc. 1943, 123, 335-339.
Miller, C. P., Becker, R. M., Schad, D., and Robbins, M. W. The effect o fheat on the toxic and antigenic properties of meningococcus. J. Infect. Dis. 1943, 73, 248-256.
Phair, J. J., Smith, D. G., and Root, C. M. The use of chicken serum in the species and type identification of neisseria. Proc. Soc. Exp. Biol. Med. 1943, 52, 72-73.
Schoenbach. E. B. The meningococcal carrier state. Med. Ann. Dist. Columbia 1943, 12, 417-420.
1944
Kabat, E. A., Kaiser, H., and Sikorski, H. Preparation of the type-specific polysaccharide of the type I meningococcus and a study of its effectiveness as an antigen in human beings. J. Exp. Med. 1944, 80, 299-307.
Miller, C. P. A note on the agglutination of meningococcus. Yale J. Biol. Med. 1944, 16, 519-528.
Miller, C. P, Breadenkopf, W. G., Peck, D., and Robbins, M. W. A survey of chronic meningococcus carriers in a semi permanent population. J. Infect. Dis. 1944, 74, 212-224.
Miller, C. P, and Schad, D. The resistance of meningococci to drying. J. Bacteriol. 1944, 47, 71-77.
Miller, C. P, and Schad, D. Germicidal action of daylight on meningococci inthe dried state. J. Bacteriol. 1944, 47, 79-84.
Phair, J. J., Schoenbach, E. B., and Root, C. M. Meningococcal carrier studies. Am. J. Public Health 1944, 34, 148-154.
Phair, J. J., and Schoenbach, E. B. The dynamics of meningococcal infections and the effect of chemotherapy. Am. J. Hyg. 1944, 40, 318-344.
117
1945
Kabat, E. A., Miller, C. P, Kaiser, H., and Foster, A. Z. Chemical studies on bacterial agglutination. VII. A quantitative study of the type specific and group specific antibodies in antimeningococcal sera of various species and their relation to mouse protection. J. Exp. Med. 1945, 81, 1-8.
Phair, J. J., and Schoenbach, E. B. The transmission and control of meningococcal infections. Am. J. Med. Sci.,1945, 209, 69-74.
Schoenbach, E. B., and Phair, J. J. The dissemination and control of meningococcal infections. J. Mt. Sinai Hosp. N. Y. 1945, 12, 624-636.
1946
Phair, J. J., Schoenbach, E. B., and Merrell, M. Chemoprophylaxis in the prevention of disease with special reference to meningococcal infections. I. A comparative study of the absorption, persistence and excretion of four sulfonamide compounds. Hum. Biol. 1946, 18, 171-203
1948
*Schoenbach, E. B., and Phair, J. J. Appraisal of the techniques employed for the detection of subclinical (inapparent) meningococcal infections. Am. J. Hyg. 1948, 47, 271-281.
Schoenbach, E. B., and Phair, J. J. The sensitivity of meningococci to sulfadiazine. Am. J. Hyg. 1948, 47, 177-186.
Commission on Pnuemonia
1944
Degara, P. F. A granular body characteristic of certain non-bacterial pneumonias of mice. Proc. Soc. Exp. Biol. Med. 1944, 56, 107-110.
Tillett, W. S., Cambier, M. J., and McCormack, J. E. The treatment of lobar pneumonia and pneumococcal empyema with penicillin. Bull. N.Y. Acad. Med. 1944, 2nd Ser. 20, 142-178.
1945
Christensen, L. R. Streptococcal fibrinolysis; a proteolytic reaction due to a serum enzyme activated by streptococcal fibrinolysin. J. Gen. Physiol. 1945, 28, 363-383.
Degara, P. F., and Furth, J. The relative susceptibility of normal and x-rayed mice of different stocks to pneumotropic viruses. J. Immunol. 1945, 50, 255-264.
1946
Heidelberger, M., MacLeod, C. M., Kaiser, S. J., and Robinson, B. Antibody formation in volunteers following injection of pneumococci or their type-specific polysaccharides. J. Exp. Med. 1946, 83, 303-320.
Hodges, R. G., and MacLeod, C. M. Epidemic pneumococcal pneumonia. I. Description of the epidemic. Am. J. Hyg. 1946, 44, 183-192.
Hodges, R. G., and MacLeod, C. M. Epidemic pneumococcal pneumonia. II. The influence of population characteristics and environment. Am. J. Hyg. 1946,44, 193-206.
Hodges, R. G., MacLeod, C. M., and Bernhard, W. G. Epidemic pneumococcal pneumonia. III. Pneumococcal carrier studies. Am. J. Hyg. 1946, 44,207-230.
118
Hodgers, R. G., and MacLeod, C. M. Epidemic pneumococcal pneumonia. IV. The relationship of nonbacterial respiratory disease to pneumococcal pneumonia. Am. J. Hyg. 1946, 44, 231-236.
Hodges, R. G., and MacLeod, C. M. Epidemic pneumococcal pneumonia. V. Final consideration of the factors underlying the epidemic. Am. J. Hyg. 1946,44, 237-243.
Walter, A. W., Schenkein, E. L., and Sutliff, W. D. Mouse-protective titers of sera of volunteers following injection of pneumococcior their type-specific polysaccharides. J. Exp. Med. 1946, 83,321-328.
1947
Heidelberger, M., MacLeod, C. M., Hodges, R. G., Bernhard, W.G., and Delapi, M. M. Antibody formation in men following injection of four type-specific polysaccharides of pneumococcus. J. Exp. Med., 1947,85, 227-230
1948
Degara, P. F., and Furth, J. Pneumonia produced by a meningo-pneumotropicvirus. Report of a fatal case, with observations on the interrelationship of psittacosis-like viruses. Arch. Pathol. 1948, 45, 474-493.
*Joint Report with Commission on Meningitis (Reprint Number 411).
?Joint sponsorship with Commission on Streptococcal and Staphacoccal Diseases.
?Joint sponsorship with Commission on Immunization.
?No reprints available and joint sponsorship with the Commission on Immunization.
?No reprints available.
**Joint sponsorship with the Commission on Viral Infection.
??Joint sponsorship with the Commission on Influenza.
119
SUPPLEMENTAL REFERENCES
Adenoviruses
Rowe, W. P, Huebner, R. J., Gilmore, L. K., Parrott, R. H., and Ward, T. G. Isolation of a cytopathic agent from human adenoids undergoing spontaneous degeneration in tissue culture. Proc. Soc. Exp. Biol. Med. 1953,84, 570-573.
Hilleman, M. R., and Werner, J. H. Recovery of new agent from patients with acute respiratory illness. Proc. Soc. Exp. Biol. Med. 1954, 85, 183-188.
Huebner, R. J., Rowe, W. P, Ward, T. G., Parrott, R. H., and Bell, J. A. Adenoidal-pharyngeal-conjunctival agents, a newly recognized grou pof common viruses of the respiratory system. N. Engl. J. Med. 1954, 251,1077-1086.
Hilleman, M. R. Prevention of acute respiratory disease in recruits by adenovirus (RI-APC-ARD) vaccine. Proc. Soc. Exp. Biol. Med. 1956, 92, 377-383.
Chanock, R. M., Ludwig, W., Huebner, R. J., Cate, T. R., and Chu, L-W. Immunization by selective infection with type 4 adenovirus grown inhuman diploid tissue culture. I. Safety and lack of oncogenicity and tests for potency in volunteers. J. Am. Med. Assoc. 1966, 195, 345-352.
Edmondson, W. P, Purcell, R. H., Gundelfinger, B. F., Love, J. W. P, Ludwig, W., and Chanock, R. M. Immunization by selective infection with type 4 adenovirus grown in human diploid tissue culture. II. Specific protective effect against epidemic disease. J. Am. Med. Assoc. 1966, 195, 453-459.
Buescher, E. L. Respiratory disease and the adenoviruses. Med. Clin. N. Am. 1967, 51, 769-779.
Top, F. H., Jr., Grossman, R. A., Bartelloni, P. J., Segal, H. E., Dudding, B. A., Russell, P. K., and Buescher, E. L. Immunization with live types 7 and 4adenovirus vaccines. I. Safety, infectivity, antigenicity, and potency of adenovirus type 7 vaccine in humans. J. Infect. Dis. 1971, 124, 148-154.
Top, F. H., Jr., Buescher, E. L., Bancroft, W. H., and Russell, P. K. Immunization with live types 7 and 4 adenovirus vaccines. II. Antibody response and protective effect against acute respiratory disease due to adenovirus type 7. J. Infect. Dis. 1971, 124, 155-160.
Collis, P. B., Dudding, B. A., Winter, P. E., Russell, P. K., and Bueschert, E. L. Adenovirus vaccines in military recruit populations: a cost benefit analysis. J. Infect. Dis. 1973, 128, 745-752.
Atypical/Mycoplasma Pneumonia
Cressy, N. L. "Primary atypical pneumonia." In "The Pneumonias" (chapt. XII). In Preventive Medicine in World War II. Vol. IV. Communicable Diseases Transmitted Chiefly Through the Respiratory and Alimentary Tracts, edited by E. C. Hoff. Washington, D.C.: Office of The Surgeon General, Department of the Army, 1958.
Reimann, H. A. An acute infection of the respiratory tract with atypical pneumonia; a disease entity probably caused by a filterable virus. J. Am. Med. Assoc. 1938, 111, 2377-2384.
Levin, S. The atypical pneumonia syndromes. J. Am. Med. Assoc. 1984, 251, 945-948.
Finland, M., and Dingle J. H. Virus pneumonias II. Primary atypical pneumonia of unknown etiology. N. Engl. J. Med. 1942, 227, 378-385.
Official Statement. Primary atypical pneumonia, etiology unknown. War Med. 1942, 2, 330-333.
Eaton, M. D., Meiklejohn, G., van Herick, W., and Talbot, J. C. Infectious agent from cases of atypical pneumonia apparently transmissible to cotton rats. Science1942, 96, 518-519.
Eaton, M. D., Meiklejohn, G., and van Herick, W. Studies on the etiology of primary atypical pneumonia: A filterable agent transmissible tocotton rats, hamsters, and chick embryos. J. Exp. Med. 1944, 79, 649-668.
Liu, C. Studies on primary atypical pneumonia. I. Localization, isolation, and cultivation of a virus in chick embryos. J. Exp. Med. 1957, 106,455-466.
120
Liu, C., Eaton, M. D., and Heyl, J. T. Studies on primary atypical pneumonia. II. Observations concerning the development and immunologic characteristics in patients. J. Exp. Med. 1959, 109, 545-556.
Chanock, R. M., Mufson, M. A., Bloom, H. H., James, W. D., Fox, H. H., and Kingston, J. R. Eaton agent pneumonia. J. Am. Med. Assoc. 1961, 175, 213-220.
Marmion, B. P, and Goodburn, G. M. Effect of an organic gold salt on Eaton`s primary atypical pneumonia agent and other observations. Nature 1961, 189, 247-248.
Chanock, R. M., Fox, H. H., James, W D., Bloom, H. H., and Mufson, M. A. Growth of laboratory and naturally occurring strains of Eaton agent in monkey kidney tissue culture. Proc. Soc. Exp. Biol. Med. 1960, 105, 371-375.
Chanock, R. M., Hayflick, L., and Barile, M. F. Growth on articial medium of an agent associated with atypical pneumonia and its identification as a PPLO. Proc. Natl. Acad. Sci. 1962, 48, 41-49.
Smith, C. B., Friedewald, W T., and Chanock, R. M. Inactivated Mycoplasmapneumoniae vaccine, evaluation in volunteers. J. Am. Med. Assoc. 1967, 199, 353-358.
Mogabgab, W J. Protective effects of inactive Mycoplasma pneumoniae vaccine in military personnel 1964-1966. Am. Rev. Respir. Dis. 1968, 97, 359-865.
Fernald, G. W., and Glezen, P. W. Humoral and cellular immune responses to an inactivated Mycoplasma pneumoniae vaccine in children. J. Infect. Dis. 1973, 127, 498-504.
Wenzel, R. P, Craven, R. B., Davies, J. A., Hendley, J. O., Hamory, B. H., and Gwaltney, J. M., Jr. Field trial of an inactivated Mycoplasmapneumoniae vaccine. I. Vaccine efficacy. J. Infect. Dis. 1976, 134, 571-576.
Common Cold/Rhinoviruses
Kruse, W. Die Erreger von Husten und Schnupfen Muench. Med. Woch. 1914, 61, 1547.
Dochez, A. R., Shibley, G. S., and Mills, K. C. Studies inthe common cold. IV. Experimental transmission of the common cold to anthropoid apes and human beings by means of a filtrable agent. J. Exp. Med. 1930, 52, 701-716.
Long, P. H., Doull, J. A., Bourn, J. M., and McComb, E. The etiology of acute upper respiratory infection (common cold). J. Exp. Med. 1931, 53,447- 470.
Andrewes, C. H. Adventures among viruses. III. The puzzle of the common cold. New Engl. J. Med. 1950, 242, 235-240.
Price, W. H. The isolation of a new virus associated with respiratory clinical disease in humans. Proc. Natl. Acad. Sci. 1956, 42, 892-896.
Pelon, W., Mogabgab, W. J., Phillips, I. A., and Pierce, W. E. Acytopathogenic agent isolated from Naval recruits with mild respiratory illnesses. Proc. Soc. Exp. Biol. Med. 1957, 94, 262-267.
Tyrrell, D. A. J., Bynoe, M. L., Hitchcock, G., Pereira, H.G., and Andrewes, C. H. Some virus isolations from common colds. I. Experiments employing human volunteers. Lancet 1960, 1, 235-237.
Hamparian, V. V., Ketler, A., and Hilleman, M. R. Recovery of new viruses(coryzavirus) from cases of common cold in human adults. Proc. Soc. Biol Med.1961, 108, 444-453.
Tyrrell, D. A. J. Rhinoviruses, a description. Science 1963, 141,152-153.
Rosenbaum, M. J., DeBerry, P., Sullivan, E. J., Pierce, W.E., Mueller, R. E., and Peckinpaugh, R. O. Epidemiology of the common cold in military recruits with emphasis on infections by rhinovirus types IA, 2 and two unclassified rhinoviruses. Am. J. Epidemiol. 1971, 93, 183-193.
Fox, J. P, Cooney, M. K., and Hall, C. E. The Seattle virus watch. V. Epidemiologic observations of rhinovirus infections, 1965-1969, in families with young children. Am. J. Epidemiol. 1975, 101, 122-143.
Bluestone, C. D. Symposium. Questioning the efficacy and safety ofanti-histamines in the treatment of upper respiratory infection. Pediatr. Infect. Dis. J. 1988, 7, 215-242.
121
Pneumococcal Pneumonia
Avery, O. T., and Heidelberger, M. Soluble specific substance of pneumococcus. J. Exp. Med. 1923, 38, 73-79.
Avery, O. T., MacLeod, C. M., and McCarty, M. Studies on chemical nature of substance inducing transformation of pneumococcal types, induction and transformation by a deoxyribonucleric acid fraction isolated from pneumococcus type III. J. Exper Med. 1944, 79, 137-158.
Austrian, R. The current status of bacteremic pneumococcal pneumonia. Reevaluation of an underemphasized clinical problem. Trans. Assoc. Am. Physicians 1963, 76, 117-125.
Austrian, R., and Gold, J. Jr. Pneumococcal bacteremia with special referenceto bacteremic pneumococcal pneumonia. Ann. Intern. Med. 1964, 60, 759-776.
Austrian, R. The development of pneumococcal vaccine. Proc. Am. Philos. Soc. 1981, 125, 46-51.
Schiemann, O., and Casper, W. Sind die Spezifisch Pracipitablen Substanzender 3 Pneumokokkentypen Haptene? Z. Hyg. Infektionskr. 1927, 108, 220-257.
Francis, T. J., Jr., and Tillett, W. S. Cutaneous reactionsin pneumonia. The development of type specific antibodies following the intradermal injection of type-specific polysaccharide. J. Exp. Med. 1930, 52, 573-585.
Finland, M., and Ruegsegger, J. M. Immunization of human subjects with the specific carbohydrates of Type III and the related Type VIII pneumococcus. J.Clin. Invest. 1935, 14, 829-832.
Ekwurzel, G. M., Simmons, J. S., Dublin, L. I., and Felton, L. D. Studies on immunizing substances in pneumococci. VIII. Report on field tests to determine the prophylactic value of a pneumococcus antigen. Public Health Rep. 1938,53, 1877-1893.
Heidelberger, M. Quantitative absolute methods in the study of antigen? antibody reactions. Bacteriol. Rev. 1939, 3, 49-95.
Austrian, R., Douglas, R. M., Schiffman, G., Coetzee, A. M., Koornhof, H. J., Hayden-Smith, S., and Reid, R. D. W. Prevention of pneumococcal pneumonia by vaccination. Trans. Assoc. Am. Physicians 1976, 89, 184-192.
Smith, P., Oberholzer, D., Hayden-Smith, S., Koornhof, H. J., and Hilleman, M. R. Protective efficacy of pneumococcal polysaccharide vaccine. J. Am. Med. Assoc. 1977, 238, 2613-2616.
Immunization Practices Advisory Committee. Pneumococcal polysaccharide vaccine. Morb. Mortal. Wkly. Rep. 1989, 38, 64-76.
Meningococcal Meningitis
Schwentker, F. F., Gelman, S., and Long, P H. The treatment of meningococcal meningitis with sulfanilamide. Preliminary report. J. Am. Med. Assoc. 1937, 108, 1407-1408.
Dingle, J. H., Thomas, L., and Morton, A. R. Treatment of meningococca lmeningitis and meningococcemia with sulfadiazine. J. Am. Med. Assoc. 1941, 116, 2666-2668.
Feldman, H. A. Meningococcal disease, 1965. J. Am. Med. Assoc. 1966, 196, 391-393.
Millar, J. W., Siess, E. E., Feldman, H. A., Silverman, C., and Frank, P In vivo and in vitro resistance to sulfadiazine in strains of Neisseriameningitidis. J. Am. Med. Assoc. 1963, 186, 139-141.
Alexander, C. E., Sanborn, W. R., Cherriere, G., Crocker, W.H., Jr., Edwald, P E., and Kay, C. R. Sulfadiazine-resistant group A Neisseriamenigitidis. Science 1968,
Feldman, H. A. Some recollections of the meningococcal diseases. The first Harry F. Dowling lecture. J. Am. Med. Assoc. 1972,220, 1107-1112.
Eickhoff, T. C. In-vitro and in-vivo studies of resistance to rifampin inmeningococci. J. Infect. Dis. 1971, 123, 414-420.
Weidmer, C. F., Dunkel, T. B., Pettyjohn, F. S., Smith, C.D., and Leibovitz, A. Effectiveness of rifampin in eradicating the meningococcalcarrier state in a relatively closed population, Emergence of resistant strains. J. Infect. Dis. 1971, 124, 172-178.
122
Goldschneider, I., Gotschlich, E. C., and Artenstein, M. S. Human immunity to the meningococcus. I. The role of humoral antibodies. J. Exp. Med. 1969, 129, 1307-1326.
Goldschneider, I., Gotschlich, E. C., and Artenstein, M. S. Human immunity to the meningococcus. II. Development of natural immunity. J. Exp. Med. 1969, 129, 1327-1348.
Gotschlich, E. C., Liu, T. Y, and Artenstein, M. S. Human immunity to the meningococcus. III. Preparation and immunochemical properties of the group A, group B and group C meningococcal polysaccharides. J. Exp. Med. 1969, 129, 1349-1365.
Gotschlich, E. C., Goldschneider, I., and Artenstein, M. S. Human immunity to the meningococcus. IV. Immunogenicity of group A and group Cmeningococcal polysaccharides in human volunteers. J. Exp. Med. 1969, 129, 1367-1384.
Gotschlich, E. C., Goldschneider, I., and Artenstein, M. S. Human immunity to the meningococcus. V. The effect of immunization withmeningococcal group C polysaccharide on the carrier state. J. Exp. Med. 1969, 129, 1385-1395.
Artenstein, M. S., Gold, R., Zimmerly, J. G., Wyle, F. A., Schneider, H., and Harkins, C. Prevention of meningococcal disease by group C polysaccharide vaccine. New Engl. J. Med. 1970, 282, 417-420.
Devine, L. F., Pierce, W. E., Floyd, T. M., Rhode, S. L., Edwards, E. A., Siess, E. E., and Peckinpaugh, R. P. Evaluation of group C meningococcal polysaccharide vaccine in marine recruits, San Diego, California. Am. J. Epidemiol. 1970, 921, 25-32.
Wahdan, M. H., Pizk, F., El-Akkad, A. M., El Ghoroury, A. E.,Hablas, R., Girgis, N. I., Amer, A., Boctar, W., Sippel, J. E., Gotschlich, E.C., Triau, R., Sanborn, W. R., and Cvjetanovic, B. A controlled field trial of serogroup A meningococcal polysaccharide vaccine. Bull. World Health Organ. 1973, 48, 667-673.
Makela, P. H., Kayhty, H., Weckstrom, P., Sivonen, A., and Renkonen, O. Effect of group A meningococcal vaccine in army recruits in Finland. Lancet 1975, 2, 883-886.
Control of Airborne Infections
Whayne, T. F. "Housing." In Preventive Medicine in World War II. Vol. II: Environmental Hygiene, edited by E. C. Hoff. Washington, D.C.: Office of The Surgeon General, Department of the Army, 1955.
Brundage, J. F., Scott, R. McN., Lednar, W. M., Smith, O. W., and Miller, R.N. Building-associated risk of febrile acute respiratory diseases in Army trainees. J. Am. Med. Assoc. 1988, 259, 2108-2112.
Coccidioidomycosis
Dickson, E. C. "Valley Fever" of San Joaquin Valley and fungus Coccidioides. Calif. West. Med. 1937, 47,151-155.
Smith, C. E. The epidemiology of acute coccidioidomycosis with erythemanodosum ("San Joaquin" or "Valley Fever"). Am. J. Public Health 1940, 30, 600-611.
Palmer, C. E. Geographic differences in sensitivity to histoplasm in among student nurses. Public Health Rep. 1946, 61, 475-487.
Smith, C. E. "Coccidioidomycosis." In Preventive Medicine in World War II. Vol. IV. Communicable Diseases, edited by E. C. Hoff. Washington, D.C.: Office of The Surgeon General, Department of the Army, 1958.
Winn, W. A. Coccidioidomycosis and amphotericin B. Med. Clin. North Am. 1963, 47, 1131-1148.
Pappagianis, D., Hector, R., Levine, H. B., and Collins, M. S. Immunization of mice against coccidioidomycosis with a subcellular vaccine. Infect. Immun.1979, 25, 440-445.
Pappagianis, D., and The Vaccine Study Group. Evaluation of the protective efficacy of the killed Coccidioides immitis vaccine inman. Abstract. 1986, 784. Inter science Conference on Antibiotics and Chemotherapy (ICAAC).
123
Q Fever
Robbins, F. C., and Ragan, C. A. Q fever in the Mediterrean Area, report of its occurrence in Allied troops. I. Clinical features of the disease. Am. J. Hyg. 1946, 44, 6-22.
Robbins, F. C., and Rustigian, R. Q fever in the Mediterranean Area, report of its occurrence in Allied troops. IV. A laboratory outbreak. Am. J. Hyg. 1946, 44, 64-71.
Spicknall, C. G. Huebner, R. J., Finger, J. A., and Blocker, W. P. Report of an outbreak of Q fever at the National Institutes of Health. I. Clinical features. Ann. Intern. Med. 1947, 27, 28-40.
DeLay, P. D., Lennette, E. H., and DeOme, K. B. Q fever in California. II. Recovery of Coxiella burnetii from naturally-infected air-borne dust. J.Immunol. 1950, 65, 211-220.
Johnson, J. E., III, and Kadull, P. J. Laboratory-acquired Q fever. A report of fifty cases. Am. J. Med. 1966, 41, 391-403.
Ascher, M. S., Berman, M. A., and Ruppaner, R. Initial clinical and immunologic evaluation of a new phase 1 Q fever vaccine and skin test in humans. J. Infect. Dis. 1983, 143, 214-222.
Pretibial (Fort Bragg) Fever
Daniels, W. B., and Grennan, H. A. Pretibial fever: An obscure disease. J. Am. Med. Assoc. 1943, 122, 261-365.
Daniels, W. B. "Fort Bragg" fever. In Internal Medicine in World War II. Vol. II. Infectious Diseases, edited by W. P. Havens, Jr.Washington, D.C.: Office of The Surgeon General, Department of the Army, 1963.
Melnick, J. L., and Paul, J. R. Experimental Fort Bragg fever (pretibial fever) in chimpanzees. Proc. Soc. Exp. Biol. Med. 1948, 67, 263-268.
Gochenour, W. S., Smadel, J. E., Jackson, E. B., Evans, L. B., and Yager, R.H. Leptospiral etiology of Fort Bragg fever. Public Health Rep. 1952, 67, 811-813.
Hebert, G. A., Thomason, B. M., Harris, P. P., Hicklin, M.D., and McKinney, R. M. "Pittsburgh pneumonia agent," a bacterium pheno typically similar to Legionella pneumophila and identical to the Tatlock bacterium. Ann. Intern. Med. 1980, 92, 53-54.
Tatlock, H. Clarification of the cause of Fort Bragg fever (pretibial fever)?January1982. Rev. Infect. Dis. 1982, 4, 157-158.
Viral Gastroenteritis
Zahorsky, J. Hyperemesis hiemis or the Winter Vomiting Disease. Arch. Pediatr. 1929, 46, 391-395.
Gordon, I., Ingraham, H. S., and Korns, R. F. Transmission of epidemic gastroenteritis to human volunteers by oral administration of fecal filtrates. J.Exp. Med. 1947, 86, 409-422.
Kojima, S., Fukumi, H., Kusama, H., Yamamoto, S., Suzuku, S., Uchida, T., Ishimaru, T., Oka, T., Kuretani, K., Ohmura, K., Nishikawa, F.,Fujimoto, S., Fujita, K., Nakano, A., and Sunakawa, S. Studies on the causative agent of the infectious diarrhea. Record of experiments on human volunteers. Jpn. Med. J. 1948, 1, 467-476.
Kapikian, A. Z., Flores, J., Hoshino, Y, Glass, R. I., Midthun, K., Gorziglia, M., and Chanock, R. M. Rotavirus, the major etiologic agent of severe infantile diarrhea may be controllable by a "Jennerian" approach to vaccination. J. Infect. Dis. 1986, 153, 805-822.
Leers, W. D., Kasupski, G., and Fralick, R. Norwalk-like gastroenteritis epidemic in a Toronto Hospital. Am. J. Public Health 1987, 77, 291-295.
Matson, D. O., Estes, M. K., Glass, R. I., Bartlett, A. V., Penaranda, M., Calomeni, E., Tanaka, T., Nakata, S., and Chiba, S. Human calicivirus-associated diarrhea in children attending day care centers. J.I nfect. Dis. 1989, 159, 71-78.
124
SECTION 1-APPENDIX 1
ADMINISTRATIVE CHRONOLOGY
27 December 1940
Lieutenant Colonel James S. Simmons transmitted letter prepared for the signature of Major General James C. Magee, The Surgeon General, recommending stablishment of a "Board for the Investigation of Influenza and Other Epidemic Diseases in the Army."
11 January 1941
Secretary of War authorized the establishment of "The Board for the Investigation and Control of Influenza and Other Epidemic Diseases in theArmy."
6 February 1941
First meeting of Board; Dr. Francis Blake, President; Commissions on Influenza, Meningitis, and Pneumonia among the first seven commissions proposed.Influenza Commission to include "related acute respiratory diseases."
27-28 February 1941
Second meeting of Board. Drs. John H. Dingle and Alto E. Feller listed among17 consultants for Commission on Influenza.
19 March 1941
Organizational meeting of Commission on Meningococcal Meningitis; Dr. Perrin Long, Director
May 1941
Commission on Pneumonia activated; Dr. Colin M. MacLeod, Director.
19-20 June 1941
Third meeting of Board. A new commission on Cross Infections in Hospitals proposed; Dr. Oswald H. Robertson, Director.
26 June 1941
Now eight commissions. Memorandum to The Adjutant General summarized the investigations that The Surgeon General had determined "are required by the respective commissions." Board approved plan for study of coccoidioidomycosis at Army air fields in San Joaquin Valley by Commission on Epidemiological Survey to be centered in laboratory of Dr. Charles E. Smith at Stanford.
1 July 1941
Central laboratory for Commission on Meningococcal Meningitis established at The Johns Hopkins School of Hygiene and Public Health under direction of Dr. John J. Phair.
21 October 1941
Commission on Cross Infections in Hospitals met to prepare a program of investigation and budget.
29-31 October 1941
Representatives of Board (Dr. A. R. Dochez) and of the Commissions on Influenza (Dr. Yale Kneeland, Jr.) and Pneumonia (Dr. MacLeod), plus Dr. Kenneth Goodner surveyed epidemic of atypical pneumonia at Camp Claiborne, Louisiana.
28-29 November 1941
Fourth Meeting of Board. Board approves Dr. MacLeod`s recommendation "that a team of investigators be sent to Camp Claiborne to investigate atypical pneumonia, etiology unknown."
9 December 1941
Dr. Dingle (Commission on Influenza) and Dr. W. Barry Wood, Jr. (Commission on Pneumonia) dispatched to Camp Claiborne.
January 1942
Group of investigators at Claiborne expanded by addition of Drs. G. John Buddingh and Feller (Commission on Influenza), Theodore J. Abernethy and James M. Ruegsegger (Commission on Pneumonia), Dr. Alexander D. Langmuir(epidemiologist), and George F. Badger (biostatistician) to form Commission for the Investigation of Atypical Pneumonia and Other Respiratory Diseases at Camp Claiborne.
125
12-13 May 1942
Fifth meeting of Board. Following report on atypical pneumonia by Dr. Dingle, Board recommended that provision be made for a year-round study of respiratory disease by a permanent commission. Commission on Tropical Diseases established; Dr. William A. Sawyer, Director.
19 July 1942
Dr. Blake, President of Board, Dr. A. R. Dochez, Board member, Brigadier General J. S. Simmons, administrator of Board, and Dr. Dingle consulted with Brigadier General. H. C. Coburn, Jr., Post Surgeon and Colonel Sanford W. French, Surgeon, Fourth Service Command at Fort Bragg, North Carolina.
24 July 1942
Board recommended to The Surgeon General that a Commission on Acute Respiratory Diseases (CARD) be established at Fort Bragg under the direction of Dr. Dingle.
1 August 1942
Commission on Acute Respiratory Diseases (CARD) activated. Initial members: Dr. Dingle, Director; Dr. Abernethy, Associate Director; Dr. Langmuir, Assistant Director; Drs. Badger, Feller, and Ruegsegger. Personnel were based temporarily at The Johns Hopkins School of Hygiene and Public Health.
15 August 1942
Decision made to establish a laboratory for CARD at the Station Hospital(later Regional Hospital) at Fort Bragg; ward building to be remodeled for this purpose.
19 October 1942
Activities of CARD centered at Fort Bragg.
31 August 1942
Dr. Phair succeeded Dr. Long as Director of Commission on Meningococcal Meningitis.
Late 1942
Allotment of 25 officers` ranks obtained by Preventive Medicine Division for assignment to the Board.
6-7 May 1943
Commission on Cross Infections in Hospitals renamed Commission on Air-Borne Infections (CABI); Dr. Robertson continued as Director.
November 1942-1943
Additional members added to CARD: Major Norman L. Cressy, Captain Hugh Tatlock, 1st Lieutenant. Elias Strauss and Drs. Charles H. Rammelkamp, Joseph W. Beard, and Irving Gordon. Dr. Beard remained at Duke University. Dr. Ruegsegger resigned for a commission in the Navy.
29 November 1943
CARD laboratory designated a Class IV installation under the Office of The Surgeon General.
November 1943
Military increment of officers for Board activities placed administratively under CARD at Fort Bragg.
29 November 1943
Laboratory established at Camp Carson, Colorado, by CABI, in collaboration with Commission on Hemolytic Streptococcal Infections.
July 1944
Work of Board military officers designated a miscellaneous War Department activity; allotment no longer charged to The Surgeon General.
November 1944
Laboratory at Camp Carson closed. Personnel and equipment moved to Madigan General Hospital, Fort Lewis, Washington.
August 1945
Army Medical Research and Development Board constituted to supervise and coordinate all research activities, including those of Army Epidemiological Board.
December 1945
Commission on Pneumonia terminated.
126
15 April 1946
Commission on Meningococcal Meningitis terminated.
15-16 April 1946
Eleventh meeting of Board. Commission on Environmental Hygiene directed to continue studies of Commission on Air-Borne Infections; CARD asked to incorporate activities of Commissions on Pneumonia and Streptococcal Infections.
30 June 1946
CARD Laboratory at Fort Bragg closed. Biological specimens transferred to School of Medicine, Western University, Cleveland, Ohio.
24 January 1949
Streptococcal Disease Laboratory established at Warren Air Force Base, Cheyenne, Wyoming, under direction of Dr. Rammelkamp.
21 February 1949
Secretary of Defense directed Secretary of the Army to assume responsibility for expanding the Board to reflect the needs of all three services.
26-27 February 1949
First formal meeting of revived Commission on Streptococcal and Staphlococcal(CSSD) Infections; Dr. William S. Tillett, Director.
2 March 1949
Secretary of the Army delegated responsibility for tri service coordination to The Surgeon General, Department of the Army.
19 April 1949
Name of Board changed to Armed Forces Epidemiological Board (AFEB).
29-30 September 1949
First annual meeting of AFEB.
8 October 1953
Secretary of Defense issued directive placing AFEB more firmly at Department of Defense level. This document became the "charter" for the AFEB.
January 1954
CARD established Laboratory on Housing and Illness at Sampson Air Force Base, New York; Dr. Harold B. Houser, Field Director.
1955
Dr. Feller succeeded Dr. Dingle as Director, CARD.
June 1956
Sampson Air Force Base closed. Records and biological specimens of Laboratory on Housing and Illness transferred to Upstate Medical Center, State Universityof New York at Syracuse.
1959
Members of CARD assisted in development of Virology Division at Naval Medical Field Research Laboratory, Camp Lejeune, North Carolina.
1959
Dr. William S. Jordan, Jr., succeeded Dr. Feller as Director, CARD.
1960
Members of CARD and Commission on Influenza began service on Adenovirus Committee, later designated Panel for Respiratory and Related Viruses, at the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), to develop specifications for standardized reagents.
1961
Members of CARD prepare a Manual of New Viruses Causing Respiratory Illnesses in Man. World Health Organization requests permission to reproduce.
1963
Committee on Meningococcal Infections formed, Dr. Harry A. Feldman, Chairman. Dr. Feldman consulted on outbreak at Naval Training Station, San Diego, California.
1963
Members of CARD and Commission on Influenza appointed to NIAID`s Board for Vaccine Development.
127
1964
Members of Committee on Meningococcal Infections consulted on outbreak at Fort Ord, California.
1967
Dr. Floyd W. Denny, Jr., succeeded Dr. Jordan as Director, CARD.
18 May 1971
Report of management survey of AFEB presented to AFEB and Commission Directors.
September 1971
Dr. George G. Jackson served as Acting Director for one year during Dr. Denny`s sabatical.
12 July 1972
AFEB and Commission Directors discussed management survey report.
1972
CARD explored the feasibility of developing a federally supported facility for vaccine research and development for certain vaccines that are not likely to be developed or marketed commercially.
18 December 1972
Report of Task Force to develop plan for a new advisory system for Army Medical Research and Development command submitted. New charter for AFEB adopted.
31 December 1972
All commissions terminated.
19 April 1973
First meeting of AFEB under new charter.
128
SECTION 1 APPENDIX 2
RESEARCH CHRONOLOGY
1941
A sharp increase in the number of cases of coccidioidomycosis was observed at military bases in southern California.
1942
Clinical, epidemiological, and etiologic studies of primary atypical pneumonia in military recruits at Camp Claiborne, Louisiana, confirmed it to be a common communicable illness, most likely caused by a new agent, probably a virus.
1942
An outbreak of a dengue-like illness with rash on legs (pretibial fever) was observed at Fort Bragg, North Carolina.
1942
Polysaccharides of types 1 and 2 pneumococci were shown to be immunogenic in humans.
1942
Investigators for Commission on Influenza repeated that an agent from cases of atypical pneumonia was transmissible to cotton rats and chick embryos.
1942
Pneumococci were identified as an important cause of pneumonia at the Army Air Base, later Army Air Force Technical School, Sioux Falls, South Dakota.
1943
A marked difference in the incidence of acute respiratory disease (ARD) between new recruits and seasoned soldiers was recorded during 3consecutive years at Fort Bragg. Atypical pneumonia was continuously present with a 10 to 1 ratio of respiratory admissions to cases of pneumonia.
1943
A clinical illness that manifested as nonstreptococcal endemic exudative pharyngitis and tonsillitis was recognized that, except for the presence of exudate, did not differ from cases of ARD.
1943
Influenza A and B viruses were purified and characterized as particles consisting of lipoprotein with associated nucleic acid of the desoxypentose type, with sizes by electron microscopy of 77.6 gm (A/PR8), 78.3 ?m(A/swine), and 97.3 ?m (B/Lee).
1943
Studies at Camp Carson, Colorado, showed that there were 28%fewer hospital admissions for upper respiratory infections among soldiers housed in oil-treated barracks than among soldiers housed in untreated barracks and 16%fewer admissions for streptococcal infections.
1943
A rickettsialike organism was isolated from three of five guinea pigs injected with blood from a patient with "Fort Bragg or Pretibial Fever." It was not affected by human convalescent sera. Over 30 years later, it was found to be the first isolate of Legionella species; named L. micdadei.
1943
Atypical pneumonia was transmitted to volunteers using as inocula unfiltered throat washings and sputa obtained from patients early in the course of characteristic disease.
1943
Illnesses produced by a foodborne epidemic of type 5streptococcus infection did not differ appreciably from sporadic or airborne cases of tonsillitis and pharyngitis caused by other types of streptococci at Fort Bragg.
1944
Titers of cold hemagglutinins in patients with atypical pneumonia were shown to be proportional to the severity of illness.
129
1944
Meningococcal carrier studies in an Army Medical Service Unit showed an average composite prevalence rate of 40%. Infections with at least one of several types were found in 92.9% of men during a 10-week study period. A single dose of 2 g of sulfadiazine reduced the carrier rate to zero without toxic reactions.
1944
Pretibial fever was recognized at Fort Bragg for the third consecutive year. A filterable agent was isolated in guinea pigs from the blood of one patient that differed from the Rickettsia-like agent previously isolated. This presumed "virus" was serially transmitted in guinea pigs; able to infect hamsters, rabbits, and chick embryos; and neutralized by convalescent sera.
1944
Atypical pneumonia was transmitted to volunteers using bacteria-free filtrates as inocula.
1944
Epidemic evidence pointed to a single common exposure in a storm cellar as the source of a severe outbreak of an unusual form of pulmonary disease at Camp Gruber, Oklahoma; subsequently (1947) shown to be histoplasmosis.
1944
Studies of epidemic influenza A at Fort Bragg and Camp Mackall, North Carolina, were complicated by the appearance of epidemic ARD. The two diseases could be differentiated serologically. The incidence of pneumococcal pneumonia increased sharply at Camp Mackall but not at Fort Bragg; the incidence ofatypical pneumonia remained constant.
1944
Members of the Commission on Influenza expanded their report on the isolation of a filterable agent ("Eaton agent") from cases of atypical pneumonia that could be propagated in chick embryos.
1944
Triethylene glycol vapor introduced into the air in scarlet fever wards reduced the number of (3 streptococci by 38% to 100%. The combination of vapor in air and dust control to floors and bedding resulted in a reduction of airborne streptococci of 93% when the wards were quiet and of 97% during bed-making periods.
1944
Oiling of floors and bedding at Fort Bragg effectively controlled the degree of bacterial contamination of air in treated barracks but had little or no effect on the incidence of hospitalized illness during the epidemic occurrence of ARD.
1945
Significantly lower incidence rates of respiratory disease were observeda mong men living in barracks equipped with double bunks than in control barracks. The procedures used in this study made possible the definition of distinct epidemiological patterns for influenza A, streptococcal pharyngitis, atypical pneumonia, and ARD.
1945
Vaccine containing pneumococcal polysaccharides types 1, 2, 5, and 7 greatly reduced the incidence of pneumococcal pneumonia at the Army Air Force Technical School, Sioux Falls, South Dakota.
1945
An epidemic illness among troops returning from Italy to Camp Patrick, Virginia, was identified as Q fever. The agent of "Balkan Grippe, "later shown to be Rickettsia (Coxiella) burnetii, caused a laboratory outbreak of Q fever.
1945
A strain of meningococcus type 1 was made resistant to sulfadiazine by serial passage through fertilized eggs containing increasing concentrations of drug.
1945
CARD proposed a theory to explain the periodicity of influenza epidemics.
130
1946
Presumed agent of pretibial fever induced a similar clinical picture in patients undergoing fever therapy and did so on three successive passages.
1946
Only 6% of cases among recruits hospitalized at Fort Bragg were due to streptococcal infections; 90% were group A, 4% group C, and 3% groupG.
1946
Two types of minor respiratory illness were demonstrated by transmission of filter passing agents to volunteers. One with a long (5 to 6days) incubation period (ARD) induced immunity to rechallenge; the other with a short (24 to 48 h) incubation period (common cold) induced no immunity tore challenge. Cross-immunity was not demonstrable with either filtrate.
1946
An outbreak of coccidioidomycosis occurred when spores from a laboratory were disseminated throughout a medical school.
1946
Four of 350 strains of meningococci were found to be resistant to 0.5 mg.% of sulfadiazine. Epidemics of meningitis could still be aborted or prevented by prophylactic use of sulfadiazine.
1947
Investigators for the Commission on Virus and Rickettsial Diseases showed that presumed "virus" of pretibial fever induced illness in chimpanzees; "viremia" was demonstrated by transmission to another chimpanzee and to young hamsters.
1947
Studies of respiratory disease at Fort Dix, New Jersey, initiated jointly with Commission on Influenza, confirmed occurrence of cyclesof ARD in recruits.
1947
Study of illnesses in a group of Cleveland, Ohio, families initiated.
1947
An investigator for the Commission on Immunization showed that fluorescein-labeled antibody can detect Eaton agent in bronchial epithelium of infected chick embryos. Sixty-seven percent to 92% of patients in several outbreaks of atypical pneumonia showed a rise of fluorescent-staining antibody during convalescence.
1948
The antibody response in humans after the injection of six type-specific pneumococcal polysaccharides was the same for each type as after the injection of fewer antigens.
1948
The mouse virulence of pneumococcal types 2, 3, and 7 was shown to correlate directly with the amount of specific polysaccharide synthesized.
1949
Study of streptococcal infections was initiated at For Francis E. Warren, Wyoming, under joint auspices of CARD and the CSSD.
1949
The "dangerous carrier" of R hemolytic streptococci was identified as a nasal carrier. Nasal carriers dispersed, on average, nearly100 times as many streptococci as throat carriers.
1949
Human subjects injected 3, 5 to 6, or 8 years previously with type-specific pneumococcal polysaccharide usually showed measurable and sometimes relatively high levels of antibody after the periods indicated. In instances in which an antibody had disappeared or remained low, reinjection of homologous polysaccharide usually caused antibody to reappear or to increase ,although rarely to the original maximum.
1949
Early penicillin therapy (relatively small doses) of pneumococcal pneumonia did not suppress the production of agglutinins or mouse protective antibodies.
1949
Three types of staphylococcal coagulase and anticoagulase were identified as being immunologically distinct.
131
1950
Nonbacterial gastroenteritis was found to be the second most frequent cause of illness in civilian families.
1950
Antihistamine drugs had no beneficial prophylactic or therapeutic effect on naturally occurring respiratory infections or on common colds transmitted to volunteers.
1950
It was demonstrated that rheumatic fever can be prevented by the treatment of exudative streptococcal pharyngitis or tonsillitis with penicillin.
1950
A case of poststreptococcal glomerulonephritis and hematuria in other members of a family of five provided the first clue that group A, type 12 streptococciare nephritogenic.
1951
The agent of pretibial fever was shown by Walter Reed Army Institute of Research (WRAIR) investigators to be similar to Leptospira autumnalis; it was subsequently designated Leptospira interrogans, serogroup Autumnalis, serovar fort bragg.
1951
Pneumococcal polysaccharides were shown to lack the capacity to induce a primary antibody response in rabbits.
1952
Rabbits immunized with pneumococcal whole-cell antigens were shown to respond to types 1 and 3 polysaccharides.
1952
Although there were fewer admissions for respiratory disease from oil-treated barracks than from control barracks, the differences in one study were not significant, and considerable numbers of hemolytic streptococcal infections continued to occur in oil-treated barracks.
1952
It was demonstrated that cortisone will reactivate group A streptococcal infections in rabbits as long as 3.5 months after intravenous inoculation of the bacteria.
1952
Stool supernates fed to volunteers induced two clinically different forms of gastroenteritis; no cross-immunity was demonstrated.
1953
Members of a group of Cleveland, Ohio, families experienced approximately 10illnesses per person per year, approximately 65% being common upper respiratory infections. Gastroenteritis was responsible for 15% of the total.
1953
Cytopathogenic agents isolated by NIH investigators from human adenoids and by WRAIR investigators from patients with acute respiratory disease at Fort Leonard Wood, Missouri, were shown to be multiple types of similar viruses; subsequently named adenoviruses.
1954
Twenty-eight percent of strains of meningococci were now resistant to sulfadiazine.
1954
The adenovirus isolated at Fort Leonard Wood (RI-67; type 4) was related etiologically to ARD illnesses induced in volunteers at Fort Bragg by tests with stored sera.
1954
A small epidemic of nonbacterial pharyngitis caused by adenovirus type 3 was documented in Cleveland, Ohio, families.
1955
Adenoviruses types 3, 4, and 7, particularly type 4, were shown to be the most important cause of ARD in military recruits.
1955
No adenovirus type 4 infections were identified at Army or Navy military academies.
132
1955
An investigator sponsored by the Commission on Immunization reported that the "virus" (Eaton agent) of atypical pneumonia could be demonstrated in the lungs of chick embryos by the use of fluorescein-labeled antibody.
1955
Lesions indistinguishable from the generalized Shwartzman reaction (GSR)occurred in rabbits when a single intravenous (IV) injection of endotoxin was accompanied or followed by an injection of synthetic, heparin-like, polymers.
1955
No differences were observed between men housed in open-bay or closed-bay barracks in hospital admission rates for adenovirus infections, influenza, and streptococcal infections.
1956
As measured by antibody acquisition, infection with adenovirus types 1 and 2 are common in the first 5 years of life, less so types 5 and 6. Children aged 1 to 18 years had no type 4 antibody.
1956
A Formalin-killed bivalent adenovirus vaccine developed by WRAIR, containing types 4 and 7, was effective in reducing the incidence of cases requiring hospitalization at Fort Dix.
1956
A Formalin-killed trivalent adenovirus vaccine (types 3, 4, and 7) reduced febrile respiratory illnesses at Great Lakes Naval Training Center, Illinois, by an estimated 50% to 75%.
1956
The level of complement-fixing antibodies in patients with coccidioidomycosis whose disease became disseminated remained elevated and indicated a poor prognosis.
1956
Experimental colds developed in approximately 35% to 40% of young adults following a single challenge with infectious secretion. Neither sex nor season altered susceptibility. The incubation periods were 24 to 72 hours. Illnesses were rarely associated with fever. Pooled human immune globulin was 65%affective in neutralizing two infectious secretions.
Gamma globulin in doses of 3, 6, 9, or 15 mL reduced hospital admissions fo racute nonstreptococcal disease. Illness, but not infection, caused by adenovirus types 4 and 7, was prevented. Later, doses of 5 to 15 mL again protected against adenovirus infections, but not against influenza A.
1956
Chilling of volunteers given infectious nasal secretions had no effect on th frequency of colds nor did the presence or absence of tonsils. Volunteers with an allergic history were slightly more susceptible (45% vs 31%), as were smokers(55% vs 34%).
1956
An IV injection of papain caused rabbit ears to collapse within 3 to 4 hours.
1956
A review of the longitudinal study of influenza in families showed that during influenza A (HlN1) epidemics in 1950, 1951, and 1953, viruses were isolated from 9% to 12% of individuals and from 25% of families. In 1950, the serologic attack rate was 15%; in 1951 and 1953, it was 25%.
1956
Inactivated bivalent types 4 and 7 adenovirus vaccine developed at WRAIR reduced hospitalized cases caused by these agents by 98% at Fort Dix.
1956
Growth of the first rhinoviruses in cell culture was reported by investigators at Hopkins (JH virus) and at Great Lakes Naval Training Station (2060 virus). The isolates were similar and became prototypes for type 1.
1957
Rechallenge of 55 volunteers with either JH or 2060 viruses resulted in 5% colds compared to 38% colds on first challenge.
1957
Experimental colds developed in approximately 35% to 40% of young adults following a single challenge with infectious secretion. Neither sex nor season altered susceptibility. The incubation periods were 24 to 72 hours. Illnesses were rarely associated with fever. Pooled human immune globulin was 65%affective in neutralizing two infectious secretions.
133
1957
A team composed of representatives of the Commission on Influenza, CARD, Navy, and the Pan American Health Organization visited laboratories in South America to assess their capacity to study the anticipated epidemic of Asian influenza before its arrival in the United States.
1957
An Influenza Study Group was organized by CARD and the Commissions on Influenza and Streptococcal Diseases to obtain early information on pandemic Asian (H 2N2) influenza. It reported that influenza in Santiago and Concepcion, Chile, during July and August was accompanied by a high rate of pulmonary complications and a twofold increase in deaths.
1957
The observation of Cleveland, Ohio, families that had been discontinued was reinstituted in September in anticipation of an epidemic due tot he new influenza A variant (H2N2). Infection occurred in 90% of families and in 47% of individuals. There were no fatal cases in the families.
1957
Asian influenza caused fulminant, fatal cases in the Cleveland, Ohio, community. Virus was isolated from the lung or trachea of 25 of 33 patients and from extrapulmonary organs in 3 of the 25.
1958
Review of volunteer experiments involving 1,034 subjects showed that installation of one of five infectious secretions obtained from patients with a common cold gave specific protection against the development of a cold when the same secretion was in stilled up to 45 weeks later, whereas there was no protection against a cold produced by any other secretion.
1959
Intravenous amphotericin B produced a favorable response in three-quarters of patients with progressive primary coccidioidomycosis and led to complete remission in 5 of 47 patients with meningitis.
1959
Tissue culture technology permitted the isolation of many new viruses from respiratory (parainfluenza types 1, 2, and 3; respiratory syncytial; coxsackie) and gastrointestinal (enteroviruses or enteric human orphan [ECHO] and reoviruses) tracts, creating a "viral smog."
1960
Fluorescent-stainable antibody responses to Eaton agent, measured in infected chick embryos, were detected in convalescent sera collected in 1944 from volunteers who developed atypical pneumonia during transmission experiments. Because volunteers who had no illness or minor illness also developed such antibody responses, proof of the etiologic role of Eaton agent could not be established.
1960
Studies of respiratory illnesses in recruits at the Marine Recruit Depot, Parris Island, South Carolina, using fluorescent-stainable antibody in Eaton agent-infected chick embryos showed that 68% of patients with atypical pneumonia developed evidence of infection versus 6% with no illness.
1960
Eaton agent was shown to be inhibited by gold salts and to grow as minute coccobacilli in chick embryos and tissue, leading to the conclusion that the agent is not a virus but a member of the genus Mycoplasma(pleuropneumonia-like organisms).
1961
Three soluable antigens were separated from cells infected with type 5 adenovirus: "early eluting" (type specific), "late eluting" (group specific), and "toxic," also group specific. The antigens were produced before infectious particles and were precursors of such particles.
134
1961
Of 68 coccidioidomycosis patients with nonmeningeal dissemination treated with amphotericin B, 68% had favorable results. Improvement occurred more often (88%) in those who underwent a fourfold reduction in CF titer than in those who did not (33%).
1961
It was shown that saline-soluble deoxyribonucleic acid (DNA) is produced as a requirement of adenovirus synthesis and is a precursor, if not a subunit, of the virus. The accumulation of "surplus" DNA and protein results in the formation of the nuclear inclusion bodies that are the hallmark of adenovirus-infected cells.
1962
Eaton pleuropneumonialike organism (PPLO) was recovered directly on agar from 12 of 13 serologically positive patients with atypical pneumonia. The isolates produced distinctive colonies on an agar-yeast extract-horse serum medium.
1963
Eaton PPLO was designated Mycoplasma pneumoniae.
1963
Types 4 and 7 adenoviruses grown in human embryonic kidney cell culture were shown to selectively infect the lower intestinal tract when virus was administered in enteric-coated capsules.
1963
Sulfadiazine failed to reduce carrier rates of meningococci among recruits at the San Diego Naval Training Center. Cases of meningitis continued to occurred spite mass prophylaxis.
1964
An epidemic of meningococcal meningitis at Fort Ord, California, was linked to cases that occurred first in the civilian community of California away from the base, rather than vice versa.
1964
Now 53 rhinovirus serotypes.
1964
Effectiveness of different lots of inactivated adenovirus vaccine, both aqueous and adjuvant, shown to vary in trials at Great Lakes Naval Training Station.
1964
Biosynthesis of ribonucleic acid after adenovirus infection was shown to be essential for production of virus-specific DNA, virus antigens, and infectious particles.
1964
Interferon was demonstrated in the dermal cells of vaccinia lesions of humans and in acute sera from 7 of 51 patients with clinical viral infections.
1964
Type 4 adenovirus grown in human diploid fibroblast cell culture was shown to selectively infect the lower intestinal tract, stimulate moderately high levels of neutralizing antibody, and not spread to susceptible contacts.
1964
Live type 4 adenovirus vaccine given to Marine recruits at Parris Island prevented type 4 infection when the recruits were transferred to Camp Lejeune, North Carolina, where type 4 infection was epidemic.
1965
Amantadine given 20 hours before challenge protected a volunteer with a low level of antibody against intranasal challenge with live influenza A virus.
1965
Fifty percent of civilian strains of meningococci were now resistant to 1mg?% or more of sulfadiazine. Penicillin treatment of meningitis was recommended.
1965
An inactivated M. pneumoniae vaccine prepared by NIH investigators induced resistance to multiplication of mycoplasma in the lung of vaccinated hamsters and was well-tolerated by 36 human subjects.
135
1966
Inactivated M. pneumoniae vaccine induced growth-inhibiting antibody in 10 of 19 volunteers who initially lacked this antibody; challenge with live M. pneumoniae-induced illness in 1 of 10men who responded to vaccine, in 7 of 9 men who did not respond, and in 10 of 13controls who lacked antibody.
1966
M. pneumoniae infections were detected in 36 of 114 families in Seattle, Washington. Transmission occurred in 23 of 36 families, with 84% of children and 44% of adults becoming infected. Tetracycline treatment did not abolish the carrier state.
1966
In a field trial of adenovirus type 4 vaccine conducted at Fort Dix by WRAIR investigators, suppression of type 4 virus fostered the emergence of type 7virus in the immunized population.
1966
Adult employees in an industrial population experienced an average of 2.3 respiratory illnesses per year during a 3-year period. Rhinoviruses accounted for 25% of the illnesses. Recurrent annual fall peaks of illness occurred during which rates of rhinovirus isolation exceeded 45%.
1966
A microneutralization test was developed for identification of rhinovirus serotypes.
1967
Neutralizing antibody responses were measured in 77% of paired serum specimens from patients with rhinovirus illness; only 5% had hemologous titers of eight or more in the acute phase of illness.
1967
Use of 73 different antisera then available successfully typed three-quarters of the rhinovirus isolates collected in Charlottesville, Virginia, over a 3-yearperiod. Forty-eight different types were identified; 61 strains were untyped. The most frequent isolate, type 14, was associated with only 8.4% of rhinovirus illnesses. Multiplicity of serotypes dimmed prospects for an effective vaccine.
1967
Only 3 of 59 male volunteers given a Formalin-killed spherule vaccine of Coccidioidesimmitis developed a serologic response.
1968
Continued observation of recurrent fall peaks of rhinovirus illnesses in families showed no demonstrable effect of school openings on peak illness rates in working adults with school children compared to those without schoolchildren.
1968
Studies of childless young married couples showed that enteric live adenovirus type 4 vaccine spread between partners without producing illness.
1968
Enteric live adenovirus type 4 vaccine given to mothers of 22 military families with children spread to only 1 of 8 nonimmune fathers and 1 of 64 children. In 26 similar families, vaccine virus given to a child spread to 3 of23 nonimmune parents and to 5 of 49 siblings but induced no illness.
1969
In a prospective study of military recruits at Fort Dix, investigators at WRAIR found that 51 of 54 cases of meningococcal meningitis were deficient in antibodies to homologous and heterologous strains of pathogenic meningococci. The group-specific polysaccharides of group A and group C meningococci were purified and shown to be excellent immunogens in six human volunteers.
1969
Navy investigators showed that group C meningococcal polysaccharide vaccine prevented the acquisition of group C meningococci by Marine recruits at San Diego, California. Three cases of meningococcal disease occurred among more than3,000 controls but none among a similar number of vaccinees.
1969
WRAIR investigators demonstrated that group C vaccine effected an 87%reduction in group C disease in 13,763 Army recruits at five basic training centers.
136
1969
In a hamster model of M. pneumoniae infection, previous infection precluded pneumonia in all animals, but parenteral vaccines were not protective despite high serum antibody titers.
1970
Hamsters immunized with a chemically induced, temperature-sensitive attenuated mutant of M. pneumoniae developed resistance to pneumonia only after intranasal infection. The level of serum antibody did not correlate with protection.
1970
A combined groups A and C meningococcal vaccine was shown to be immunogenicin greater than 90% of children 4 to 12 years of age.
1970
M. pneumoniae was isolated from 38% of recruits at Great Lakes in late summer.
1970
Simultaneous immunization of recruits at Fort Dix with both live adenovirus type 4 and type 7 vaccines during an outbreak of ARD caused by type 7 led to 96%suppression of type 7-associated ARD hospitalizations.
1971
At Great Lakes, meningococcal carrier rates, predominantly group Y, were as high as 70% during the winter of 1970 and 1971. Subsequently, group C became predominant at Great Lakes and Orlando Naval Training Stations.
1971
On 19 May the AFEB recommended that type 4 adenovirus vaccine be administered to recruits and advanced training personnel of all services and that type 7 be evaluated further for clinical effectiveness.
1971
Electron micrograph studies of hamsters showed that a differentiated portion of M. pneumoniae, consisting of an extension of the unit membrane c ontaining an electron dense core surrounded by a lucent space, serves as the means of attachment to host cell membrane.
1971
In a field trial among students at Lowry Air Force Base, Colorado, rifampin given orally in a daily dose of 600 mg for 4 days to 47 carriers of meningococciproved to be 94.7% effective in eradication of nasopharyngeal carriage. Four rifampin-resistant strains were identified during the follow-up period. Emergence and spread of resistant strains were also documented at Great Lakes and Camp Lejeune.
1971
During the peak month of influenza (A3/Hong Kong/68) activity at Lowry Air Force Base, serologic evidence of meningococcal infection was over five times as frequent among those who concurrently had serologic evidence of influenza infection than in those who did not. There was no such correlation with adenovirus infection.
1971
During an 8-year study of working adults in Charlottesville, Virginia, 4% of all colds and 8% of winter and spring colds were serologically related to infection with coronaviruses 229E and OC43.
1972
Routine administration of group C meningococcal polysaccharide vaccine was instituted for all incoming military recruits. Bivalent A and C vaccine was licensed for selective use in 1975 and administered to all recruits in 1979. Use of tetravalent (A, C, W-135, and 4) vaccine was instituted in 1982.
1972
Two doses of inactivated M. pneumoniae vaccine were administered 77 days apart to 12 antibody-negative and 6 antibody-positive children. Few or no rises in antibody titer were detected in those who were antibody negative and only minimal increases developed in those with preexisting antibody.
137
1973
On 13 September, the AFEB recommended that vaccine containing both adenovirus types 4 and 7 be administered by all three services to recruits and advanced training personnel.
![]()