



The Armed Forces Epidemiological Board
The Decade of the 1980s
Peacetime Activities Essential for the Maintenance of a Balanced Health Program in the Military Services
During the years 1979-1989, the military services and the Department of Defense`s Office of Health Affairs utilized the Board`s advisory capabilities for a number of critical medical issues that were of paramount importance to the military. Some of the most important problems ever encountered by the AFEB were discussed during this decade, including:
. Asbestosis
. Worldwide diseases and the rapid deployment force (RDF)
. Population-based forecasting models in health-care delivery systems
. Health standards for military personnel
. Health problems related to women in the armed forces
. Malaria
. Acquired immune deficiency syndrome (AIDS)
. Asplenia
. Health problems associated with the M2 Bradley Fighting Vehicle (BFV)
. Korean hemorrhagic fever
. Cardiovascular screening for military personnel age 40 and over
THE AFEB`S ROLE IN SETTING POLICY ON
ASBESTOS-RELATED HEALTH PROBLEMS
Beginning in 1977, Preventive Medical Officers at the Department of the Navy consulted with the Board in determining policy for asbestos-related health problems. During several Board meetings that year, exposure risk levels, the specificity of demographic factors, diagnostic criteria, possible contributing factors, prognosis, incidence, prevalence, and mortality were discussed.
Dr. Herschel Griffin, President of the Board, organized an ad hoc Subcommittee in 1977, in response to a request from the Deputy Assistant Secretary of Defense for Energy, Environment, and Safety, that the Board evaluate and coordinate all ongoing and proposed epidemiological studies of asbestos-related health problems. The Board was asked to advise on which other studies were needed, and on a subsequent statement of interest from the Chief of the Bureau of Medicine and Surgery, Department of the Navy, on the Board`s evaluation of the potential health hazards associated with the industrial uses
186
of asbestos. AFEB members Dr. Paul Kotin (Chairman), Dr. Anna Baetjer, and Dr. Norton Nelson served on the Subcommittee. Expert consultants to the Subcommittee were: Dr. George Jacobson, Chairman of the Department of Radiology, University of Southern California School of Medicine; Dr. Marvin Kuschner, Dean of the School of Medicine, State University of New York at Stony Brook; Dr. Marvin Schneiderman, Associate Director, Field Studies and Analysis, National Cancer Institute; and Dr. Irving Selikoff, Professor of Medicine, Mount Sinai School of Medicine.
Meetings were held on 29 September 1977 and 6 January 1978, in accordance with provisions of the Federal Advisory Committee Act and implementing directives, and were attended by a broad representation from the Department of Defense, the Veterans Administration, the Government Accounting Office, the National Institute of Occupational Safety and Health, the National Cancer Institute, the United States Public Health Service, organized labor, and other groups. During these meetings, representatives of the medical departments of the armed forces described their control programs and the potential for exposure to asbestos in the environment. The consultants to the Subcommittee presented briefings covering their areas of individual expertise, and the representative sof other groups were given the opportunity to comment.
The report, which was presented on 13 April 1978, with subsequent discussions on 13-14 April, showed that the consideration of asbestos-related health problems involves many issues besides those related to preventive medicine and occupational health. Engineering controls, contractual agreements, indemnifications, operational management, and command policies and prerogatives, all matters beyond the purview of the AFEB, were not addressed by the Subcommittee, although they do at times affect health policy.
The Subcommittee learned that Army and Air Force personnel have some potential for exposure to airborne asbestos fibers while repairing the brakes of vehicles, while replacing insulation and fire retardant materials, and during dental laboratory and clinic procedures. But the greatest potential exposure exists in the Navy, both from the standpoint of the numbers of personnel involved and from the high concentration of airborne asbestos fibers that may occur during insulation-handling operations in confined spaces aboard ships. The Navy`s policy was to confine the use of asbestos to an absolute minimum, and, in those situations in which substitute materials were inadequate, to impose strict handling procedures on its use. The report stated that compliance with Occupational Safety and Health Administration (OSHA) regulations would effectively control personnel exposure to asbestos, and that all three services have regulations implementing comprehensive industrial hygiene programs for this purpose. However, a serious breakdown in these controls can occur when work, such as asbestos "ripout" operations aboard ships undergoing shipyard overhauls, is contracted out for completion by commercial firms. These outside contractors may operate with untrained laborers and fail to comply with federal regulations for protecting either their own employees or those who may work in that area later. The report stated that it is essential that these contractor-operations be brought under the authority of line officers to mandate compliance with the regulations for protecting the contractors` personnel. This might be accomplished by writing compliance standards for personnel protection and industrial hygiene controls into contracts for this type of work.
Because of the serious impact of this matter on disease prevention, it was considered appropriate that the Subcommittee make an exception in this case and comment directly upon a management operational policy issue. The report stated that environmental exposure to asbestos is a national health hazard, and is not unique to the armed forces. The magnitude of the asbestos-related disease problem merits the establishment of a national program for (a) preventing exposure, (b) education and research, and (c) providing medical care for those afflicted with asbestos-associated diseases. It has been well established that exposure to this material entails increased risk of developing chest diseases and various cancers. However, many aspects of this risk remain poorly defined, such as those in the areas of temporal and
187
dose-response relationships, and further epidemiological and clinical assessments are needed to increase our understanding of these diseases.
The report further stated that the armed forces population could provide a useful arena for collecting needed data, as well as for developing practices and programs applicable to the population at large. Joint Department of Defense-Department of Health, Education, and Welfare research efforts are needed to provide information that may contribute to (a) better methods for preventing further exposures to personnel, (b) reducing the risk of developing asbestos-related diseases in those personnel who were exposed in the past, and (c) improving the medical care for those already afflicted with asbestos-associated disease. Current pilot studies being conducted at selected Naval shipyards are expected to establish feasible standards for medical and environmental surveillance programs, which will be applicable elsewhere However, the primary emphasis has been placed upon improving the controls for preventing personnel exposure and minimizing the adverse effects of exposures to asbestos in the past, without awaiting the results of further research.
The Subcommittee also learned that the Naval Environmental Health Center is developing a comprehensive registry of asbestos workers, in order to maintain the continuity of its medical surveillance program while it follows individuals for long time periods. In addition, a Naval Harmful Exposures Analysis Panel has been working to identify all job-related hazards, the populations at risk, and their geographic locations. This information is being used to target current medical and environmental surveillance resources toward specific environments and occupations and to justify the expansion of resources devoted to occupational health programs.
The Navy has taken measures to standardize their preemployment, periodic, and termination-of-employment medical examinations. This has helped to evaluate the effectiveness of environmental hygiene measures and to identify environmentally-associated diseases early, so that appropriate health care can be obtained. Similar routine medical surveillance programs are needed for all DoD personnel with occupational exposure to asbestos and other potentially harmful materials.
The Subcommittee report further stressed that rapid expansion of the knowledge of asbestos-related health problems is needed among health-care personnel, and that management, supervisors, and workers must be educated regarding the importance of complying with environmental control measures for preventing asbestos-associated diseases. The National Cancer Institute has developed programs for the education of health professionals and for alerting the public regarding the possible health effects associated with past exposure to asbestos.
After thoroughly discussing the information provided by the Subcommittee and the data derived from related commentaries, on 7 July 1978 the Board recommended the following to the three Surgeons General and the Assistant Secretary of Defense for Health Affairs:
a. That for all tasks having a potential for airborne distribution of asbestos fibers, the Department of Defense make immediate provisions to assure the mandatory, immediate, and continued compliance with measures for the protection of the environment and all personnel, whether DoD- or contractor-employed, from exposure to hazardous concentrations of airborne asbestos fibers.
b. That in contracts with commercial firms for tasks involving the fabrication, installation, repair, or removal of asbestos-containing insulation or fire-retardant materials or the repair [and the] relining [or both] of brakes, the Department of Defense make provisions which will assure the mandatory compliance with regulations for the protection of personnel and the environment from exposure to hazardous concentrations of airborne asbestos fibers.
c. That educational activities be implemented to make health-care professions cognizant of asbestos-related health problems, that regional consultation centers be established for assistance in clinical diagnosis, pathology, and reading of X rays, and that education
188
programs be established to inform project managers, supervisors and workers regarding the importance of compliance with all environmental control measures for prevention of asbestos-related disease. It is particularly important to inform employees who may have been exposed to hazardous levels of airborne asbestos fibers in the past that it is extremely hazardous for them to smoke.
d. That an asbestos-related disease registry be developed through consultation with existing disease registries; capabilities should be developed in conjunction with the guidelines developed by the American College of Radiology and the existing U.S. Mesothelioma Panel.
e. That the Navy appoint an officer and office, which will be administratively located in the existing Occupational Health Program, to be charged with overall responsibility for supervision of the Navy Asbestos Control Program and liaison with other involved federal agencies.
f. That sufficient information be provided to applicants for employment in areas having a potential for exposure to hazardous concentrations of airborne asbestos fibers to assure that they understand that cigarette smokers exposed to asbestos fibers experience a greatly increased risk (7-30 times greater) of developing lung cancer over that of asbestos workers who do not smoke. A special effort should be made to discourage smokers from accepting employment which may involve exposure to asbestos fibers.
g. That a continuing consultative advisory committee to the DoD be established, which will be composed of experts, both from within government and outside, in the fields of clinical diagnosis and therapy, epidemiology, biostatistics, environmental and occupational health, and industrial hygiene. This group could function as a Subcommittee of this Board until such time that it is considered operationally more appropriate to establish it as an independent advisory committee.
h. That the DoD coordinate with the DHEW and other involved agencies in promotion or research needed to provide information needed for improved occupational health capabilities.
The Board Assists the Navy Environmental Health Center in Norfolk
Not until November 1983 did Colonel Robert Nikowlewski, who was then the Board`s Executive Secretary, receive a request from the Commanding Officer of the Navy Environmental Health Center (NEHC) for members of the Navy Asbestos Medical Surveillance Program (AMSP) to present a report on the progress of their endeavor, which had begun in 1977-78. The AMSP had specifically requested that the Board`s Subcommittee provide recommendations not only for data analysis but also to consider disability criteria, research priorities, and a review of major program changes. Members of the AFEB review subcommittee were Drs. Culver, Densen, Jablon, Kurland, Legters, Nelson, Thompson, and me.
The Navy`s program, which described the identification of civilian and military personnel who were possibly exposed to asbestos, and the forms of data collection in histories, physical findings, and chest X rays, was presented by Lt. Commander P. G. Bray, MC, USNR, with comments from Captain J. Edwards, Captain J. Calcane, and others. The areas that the Subcommittee raised for consideration included:
. Specification of asbestos-exposure risk levels
. Specification of demographic factors
. Possible contributing and confounding factors
189
. Diagnostic criteria for asbestos-related diseases
. Measurement of the frequency of such diseases, including their (a) incidence, (b) prevalence, and (c) mortality
. Prognostic factors
. Future modification of the data-collection instruments, based on the reliability of each item in the data-collection questionnaire
In the interim before the next meeting of the AFEB, Dr. Kurland, Colonel Nikolewski, and I (who was President of the Board) visited NEHC in Norfolk, Virginia, for further discussion. Dr. Nelson, a member of this small ad hoc group, was unable to make this trip. At its meeting on 28 February 1984, the AFEB accepted the findings of the Subcommittee and recommended the following:
1. A panel of experts should be selected by the Navy, either as full-time employees or by contract, to develop skeleton tables designed to provide essential data on prevalence, incidence, prognosis, and data reliability. Priorities should be assigned to these tables, in relation to their relevance to such a design, so as to provide a more effective future program. Modification of the data collection instruments may be necessary.
2. The Board would, if requested, be willing to identify for the Navy suggested names for this panel of experts and would participate with the advisory panel as a consultant group to effect timely solutions to this multifaceted program.
On 23 April 1984, the Commanding Officer of NEHC requested that the AFEB assist them in identifying a group of experts from which an advisory panel for NEHC might be selected. The Board was also asked to define the minimal and optimal numbers of panel members by speciality, such as clinical medicine, epidemiology, biostatistics, occupational health, and industrial hygiene.
Dr. Leonard Kurland chaired the AFEB Subcommittee and solicited the names of experts who might serve on the advisory board for the Navy. In addition to the medical disciplines reflected in the list of potential nominees, the Board. agreed unanimously at its meeting on 24 August 1984 to also consider including recognized authorities in the medical specialties of industrial hygiene, pulmonology, and occupational medicine. It was further suggested that the Navy`s selection of panel members preferably reflect only those individuals who had not been involved in pending or recently completed, medically related, federally funded asbestos contract studies. At this same meeting, the AFEB recommended:
that, upon selection and activation of the Asbestos Surveillance Panel by the Navy Medical Service, the Board would, if requested, serve as the scientific oversight review for proposed plans, policies, and programs outlined by the panel in keeping with the overall goals and objectives of the United States Navy Occupational and Environmental Medicine Programs.
The NEHC Advisory Panel met in Norfolk, Virginia, in January1986. Members Frank Townsend and William Harlan, and Colonel Robert A. Wells attended this meeting. (By this time, Dr. Townsend had succeeded Dr. Kurland as Chairman of the ad hoc Committee, and Colonel Wells had succeeded Colonel Nikolewski as the Board`s Executive Secretary.) During the meeting, a number of questions related to asbestos and its associated health problems were discussed. These involved detailed scientific issues and required responses by capable authorities. The questions were presented to the President of the AFEB for the Board`s consideration. I commented that these types of questions should be presented to the Navy`s Panel of Experts on Asbestosis, since Board members were not sufficiently informed on
190
LEONARD T. KURLAND, M.D., M.P.H.
An honor graduate of the University of Maryland School of Medicine and the Harvard School of Public Health, Len Kurland first distinguished himself in the clinical, pathogenical, and epidemiological aspects of neurology. He did the pioneering work on motor neurone diseases, in particular on amyotrophic lateral sclerosis. He is now Professor of Epidemiology at the Mayo Graduate School of Medicine, which has developed a model system on records, medical data collection, and statistical analysis.
Len is a hardworking and dedicated Board member who has assisted in developing ambulatory and hospital data-collection systems for the military services. He has also helped devise guidelines for population forecasting and statistical evaluation of such difficult problems as the Guillain-Barr? syndrome. On several occasions, he has invited the Board`s ad hoc Subcommittees to meet in Rochester.
191
Seated, left to right: B. Dwight Culver, M.D.; Paul M. Densen, D.Sc.; Theodore E. Woodward, President of the Board; Abram S. Benenson, M.D.; Gordon N. Meiklejohn, M.D.; and Herschel E. Griffin, M.D.
Standing, left to right: Richard D. Remington, Ph.D.; Leonard T. Kurland, M.D.; William R. Harlan, M.D.; William S. Spicer, Jr., M.D.; Frank B. Engley, Jr., Ph.D.; Frank M. Townsend, M.D.; Seymour Jablon; Samuel D. Thompson, Ph.D.; Ronald C. Shank, Ph.D.; Richard H. Hornick, M.D.; William S. Jordan, Jr., M.D.; Llewellyn J. Legters, M.D.; and Colonel Robert F. Nikolewski, BSC, USAF, Executive Secretary.
192
Armed Forced Epidemiological Board and Committee Directors
21-22 June 1984
Seated, left to right: Benjamin D. Culver, M.D.; Norton Nelson, Ph.D.; Theodore E. Woodward, M.D., President of the Board; Paul M. Densen, D. Sc.; William S. Jordan, Jr., M.D.; Herschel E. Griffin, M.D.; and Gordon N. Meiklejohn, M.D.
Standing, left to right: Llewellyn J. Legters, M.D.; Samuel D. Thompson, Ph.D.; William R. Harlan, M.D.; Richard B. Hornick, M.D.; Ronald C. Shank, Ph.D.; Leonard T. Kurland, M.D.; Frank M. Townsend, M.D.; Abram S. Benenson, M.D.; Saul Krugman, M.D.; and Colonel Robert F. Nikolewski, BSC, USAF, Executive Secretary.
193
Frank Townsend graduated from Tulane University School of Medicine, and trained for several years in clinical medicine. He took his graduate training in pathology at Washington University School of Medicine in St. Louis. Dr. Townsend has been one of the pillars of the University of Texas Medical School at San Antonio. He has contributed to various fields of pathology; a major contribution of lasting importance was his extensive evaluation of wounds following airplane accidents.
Frank Townsend brought a mature judgment to the Board in the fields of medicine and pathology. He was particularly helpful in developing the Board`s recommendation to the Department of the Navy regarding the asbestosis problem, as well as in the formulation of sensible guidelines for the control of HIV infections.
194
such issues to render an authoritative response. The Board reaffirmed that it would always provide scientific oversight for proposed plans, policies, and programs as outlined by the expert panel.
On 7 February 1986, J. J. Bellanca, Commanding Officer of NEHC, transmitted the following letter of appreciation to the AFEB:
1. This is to express my appreciation for the helpful support of the Armed Forces Epidemiology Board (AFEB). This distinguished group has provided my command and the Naval Medical Command welcome support for our Asbestos Medical Surveillance Program.
2. 1 would especially like to recognize the contributions of two AFEB Board Members, first Dr. Kurland, and later Dr. Townsend, in helping us to form an expert advisory panel. This advisory panel, presently consisting of Dr. Phil Enterline, Dr. Ed Gaensler, Dr. Marcus Key, and Dr. Jerome Wiot, has analyzed our efforts and made detailed suggestions concerning data and procedures. These will be of significant value to protected Navy personnel, the medical community, and the Navy.
3. Finally, I wish to thank Colonel R. A. Wells, Executive Secretary of the Armed Forces Epidemiologic Board and all who have cooperated with him to provide us with an excellent and expert forum for solving critical epidemiologic problems regarding asbestos medical surveillance. (It should be added that Colonel Nikolewski merits equal appreciation.)
4. Please convey my sincere thanks to all concerned. We move on with increased confidence in our mission as a result of the support rendered by the Armed Force Epidemiologic Board.
During this decade of discussion of the problems related to asbestosis, the AFEB kept abreast of current developments. Preventive Medicine Officers and others in authority informed the Board of new developments, such as the relationship between mesothelioma and lung cancer, from data provided by the Armed Forces Institute of Pathology (AFIP). Demographic data including the incidence, prognosis, and mortality of asbestosis, and better means of its roentgen detection, were also presented to the Board.
THE AFEB`S ROLE IN ASSISTING THE MILITARY
ON PROBLEMS RELATED TO INFECTIOUS DISEASES
IN THE EVENT OF RAPID DEPLOYMENT
Periodically and without fail, the Board entered into discussions with the three military services (through their Preventive Medicine Officers and intramural military investigators) regarding combat readiness, rapid deployment, and infectious diseases. Drs. Abram Benenson and Charles Rammelkamp represented the AFEB at a workshop on the preventive strategy regarding the threat of infectious diseases to rapid deployment. The report o? that workshop and subsequent pertinent correspondence follows:
This workshop, held at WRAIR on 14-15 July [1981], was attended by representatives of all the services involved in the Rapid Deployment Force (RDF), the Preventive Medicine Officers of all three services, and experts on the various diseases that had been selected for discussion.
The purpose of the workshop was to (a) define infectious disease threats to the RDF given the projected scenarios for its deployment; (b) obtain an update on the epidemiology, preventive strategies and needed research and intelligence for each disease; and (c)identify policy requirements to effectively protect the RDF from these disease threats.
The area of concern was Southwest Asia; each disease was considered from the point of view of the threat to military operations in that area. Specific diseases and items considered were:
Hepatitis. Maj. Stanley M. Lemon, MC, WRAIR, reviewed the potential problem of hepatitis. He discounted hepatitis B as a problem unless there is sustained deployment and sexual contacts are affected. While only 22% of our troops have antibodies against hepatitis A, non-A non-B hepatitis is seen as the major threat in view of several
195
water-borne outbreaks which had occurred in India in 1955, 1977 and 1979 without development of antibodies against HAV. Based on these antibody studies, Dr. Lemon feels that outbreaks previously considered to have been due to hepatitis A were really due to non-A non-B infections. In 1978, French Forces [deployed to] Chad had non-A non-B hepatitis; those given IG were protected.
Research requirements include: definition of the characteristics of hepatitis in the region concerned, agent identification and characterization, the effectiveness of IG in preventing hepatitis, and, long-term, development of a vaccine against hepatitis A.
Malaria. Col. Craig J. Canfield, MC, WRAIR, presented malaria as a serious and severe threat. Problems are related to vector control inadequacies and the lack of a drug in the TO&E for chloroquine-resistant falciparum malaria. Resistance is anticipated to be a potential problem in view of the westward spread across Asia of resistant strains; half the cases in the area could be expected to be due to Plasmodium falciparum. Malaria vaccine, when available, would be strongly indicated for small independently operating units. The question was raised why to give chloroquine/primaquine combination in chemoprophylaxis in view of concern of G6-PD deficient individuals. No rationale was elicited from any of the participants for including primaquine in the field chemoprophylactic.
Leishmaniasis. Lt. Col. Charles N. Oster, MC, WRAIR, discussed leishmaniasis. Leishmania tropica, with dogs as the reservoir, is the urban problem; Le. major, with a rodent reservoir, is the rural problem. The latter can be controlled by eliminating rat burrows by deep (half meter) plowing of camp site areas and creating a ten-meter concrete barrier. [This hardly sounds practical. A.S.B.]DEET hopefully would be an effective repellent (but see below under sandfly fevers). USSR and Israel use a vaccine made of living Le. major organisms, based on experiences in which 50% of Israeli soldiers developed lesions in a six-month period at Jericho and 50% of Germans in Saudi Arabia developed the disease. Le. donovani, the cause of visceral leishmaniasis, has a rodent and canine reservoir, and can be a serious problem with high mortality without lengthy therapy. Research requirements are to determine the local epidemiology and potential attack rates, the effectiveness of the control measures on the specific vectors involved, the need for an effective therapy (only pentostam, a pentovalent antimonial, is now available in the United States on an IND) and the question of development of a vaccine.
Dengue. Col. William H. Bancroft, MC, WRAIR, discussed the potentially serious threat to military operations should dengue appear. This is related inversely to the effectiveness of anti-mosquito measures. Research requirements are to establish whether vector mosquitoes are present in the area and their habitat. The need for vaccination against dengue was discussed since vaccines against at least two of the four types are now potentially available. The value of carefully monitoring fevers of unknown origin for the initial appearance of dengue among troops was discussed, as well as serum surveys of the indigenous population to assess their past experience with this group of viruses.
Sandfly Fever, Rift Valley Fevers, and Congo/Crimean Hemorrhagic Fever. Lt. Col. Clarence J. Peters, MC, USAMRIID, felt that the problem in sandfly fever lies in the unknown effectiveness of standard repellents against local sandflies, as well as whether insecticide resistance has appeared. Research requirements include the determination of the effectiveness of antiviral drugs against this particular virus. As far as vaccines are, concerned, the multiple types of sandfly fevers complicate this potential long range solution. Rift Valley Fever-the potential effect of this virus was manifested in the recent 1977 epidemic in Egypt. While an effective vaccine has been developed, only sufficient material for 100,000 individuals is now available; this was prepared at the Swiftwater plant. Considerable discussion followed on policies for selecting vaccine recipients, particularly since the RDF contemplates staging areas in East Africa. Congo/Crimean Hemorrhagic Fever, a tick-borne disease, is expected to be prevalent throughout the entire area. Very little precise information is available concerning this disease entity in the potential area of operations.
Diarrheal Disease. Myron M. Levine, M.D., University of Maryland, presented the very serious problem of diarrheal disease. He reviewed the transmission through food and water of the various agents; by person-to-person spread of shigellae and 27-millimicronviruses; possibly by respiratory droplets of the rotavirus and the 27millimicron agent; and by flies as the vector of shigellae. Chemoprophylaxis was discounted as inappropriate or inadvisable; immunogenic protection provides the greatest hope.
Active work is underway with a pilus vaccine which would protect against colonization factor 1 and colonization factor 2; these are found in one-third of LT+/ST+ Escherichia coli infections but unfortunately are present in only 8-15% of LT-/ST+. Promising results are coming from work with oral vaccines with attenuated non-toxigenic strains such as E 1292/75 (2A). From the therapy point of view, early treatment with trimethopim-sulfasoxasole is
196
recommended; antibiotic resistance, especially against tetracycline, is as frequent as 40% in some areas. Research requirements include definition of the incidence and etiology of diarrheal diseases which might affect military personnel operating in the area; evaluation of the use of new oral vaccines versus enterotoxigenic E. coli and shigellae. An effective live vaccine against Shigella flexneri 2a is now produced by Yugoslav laboratories in Belgrade and Zagreb; this requires several doses and produces immunity lasting for twelve months at which time a single booster dose is required; three percent vomit after the first dose.
Rickettsial Diseases. Joseph V. Osterman, M.D., WRAIR, discussed Q fever and Boutonneuse fever (caused by R. conorii) as actual problems; epidemic and possibly murine typhus are expected to occur at a low incidence. Prevention would be based on avoiding the vector. Lice are resistant to DDT and lindane but Abate is still effective. For tick control, there is a question of the effectiveness of DEET as a repellent. For immunization against epidemictyphus, 1,000,000 doses of strain E and 400,000 doses of an inactivated vaccine are available. There is no vaccine for Boutonneuse fever. For Q fever, only 1,000 doses of phase-2 and 18,000 doses of phase-1 vaccine are available. Chemoprophylaxis was discussed with concern that weekly Doxacycline dosage would result in persistent rickettsial infections. Research requirements include definition of the frequency and types of rickettsial infections occurring in the area, the clearance by human testing of phase-1 Q fever vaccine, thed etermination of antigenic variation and vaccine development against R.conorii; the evaluation of appropriate antibiotic regimens for chemoprophylaxis, and entomological study for R. conorii vectors.
Schistosomiasis. Maj. John Boslego, MC, USUHS, focused on prevention by avoidance of contaminated vectors, locating foci of contamination, appropriate water treatment and protective clothing. The effectiveness of hexachlorophene as an anti-penetrant versus its neurotoxicity hazard was discussed. Col. David E. Davidson, VC, WRAIR, discussed potential immunization with irradiated cercariae which is many years off. He reviewed the drugs available for the specific schistosomal types and their adverse reactions. Of concern is the development of drug resistance against some of these agents by Schistosomamansoni in Brazil. Several potentially available agents are not licensed in the USA. Among anti-penetrants, hexachlorophene using a 0.1-0.3% alcoholic solution was 90-100% effective on mice; the anti-penetrant activity lasted for five days and resisted water soaking for four hours. Other drugs are under evaluation as anti-penetrants, including 4-aminoquinolines and a moscanate.
Rabies. William G. Winkler, DVM, Centers for Disease Control, stressed the importance of animal bites in this disease, despite four documented cases acquired by aerosol transmission, two cases from tissue (corneal) transplants, and a potential for infection by ingesting the virus. The human diploid cell vaccine has proven to be stable; pre exposure immunization with three doses given at days 0, 7, and 21, or 28 should seriously be considered. The limiting factor is the price of $42.50 per dose and the only licensed vaccine at the moment is French-made (Merieux); this has a low incidence of systemic reactions with 1 in 625 developing fever and headache. Research problems involved are those related to the demonstration of the carrier state in dogs in Ethiopia; the demonstration by monoclonal antibody studies that strains of virus differ immunologically raises the question whether the vaccine is uniformly effective; and the limited availability of rabies immune globulin which is only supplied by Cutter Laboratories and only 12,000 doses are presently available.
Respiratory Diseases. Lt. Col. R. M. Scott, MC, WRAIR, felt tha tthe greatest potential respiratory disease problem would be an antigenic shift in Influenza A and he reminded the group of the potential value of amantadine should such an event occur.
Vector Control. Col. M. Moussa, MSC, OTSG, pointed out that we have inadequate information on the identity and characteristics of the vectors in the area, of their repellent and insecticide sensitivities, and inadequate resources with which to control vectors. The Russians have reported that the anophelines in northern Iran are not repelled by DEET nor are the ticks. Studies of acceptability of repellents have shown that 60% of troops prefer to use a commercial preparation rather than the standard item, and 30% of those exposed prefer to use none. The equipment available to the RDF for area control of vectors is either non-functional, or obsolete with no replacement parts. He painted a very grim picture.
Rapid Viral Diagnosis. Karl M. Johnson, M.D., USAMRIID, discussed the techniques available for rapid viral diagnosis of specific pertinent agents, and the need for the development of appropriate technology to give operating units the ability to rapidly identify viral agents to permit appropriate preventive measures.
Practical Consideration of Airborne Corps Preventive Medicine. Col. D. C. Tsoulos, MC, Surgeon XVIII Airborne Corps, discussed his problems as operational senior medical officer, with inadequate preventive medicine
197
Phil Russell received his B.A. in Biology from The Johns Hopkins University in 1954, and his degree in Medicine from the University of Rochester School of Medicine in 1958. He trained in medicine at North Carolina Memorial Hospital in 1959, and at the University of Maryland Hospital from 1961 to 1964. At Maryland, he excelled as a house officer; he gained experience in infectious diseases in Baltimore and at Maryland`s Tropical Disease Medical Center in Lahore, Pakistan.
Phil Russell had an exemplary record in Bangkok, Thailand, where he served as Chief of Virology at the U.S. Army component of the South East Asia Treaty Organization. He was Director of the Virology Department at WRAIR; from 1979 to 1983, he was Commandant of WRAIR, which was followed by his appointment as Commanding General of Fitzsimmons Army Medical Center. In August 1986, he assumed command of the United States Army Medical Research and Development Command.
Phil Russell has distinguished himself as a virologist with notable contributions in the field of arbovirus infections, particularly those of dengue fever and the encephalitides. He maintained a close association with the Armed Forces Epidemiological Board and its Commissions prior to 1972. It was appropriate that Phil Russell was elected President of the American Society of Tropical Medicine and Hygiene. In 1979, he was the Joseph E. Smadel Lecturer and the awardee of the Infectious Diseases Society of America.
198
After he graduated from Cornell University Medical College in 1937, Bud Benenson trained at Bellevue Hospital, New York, and entered the U.S. Army Medical Corps in 1940. From then until 1962, he progressed through the ranks to Colonel, and served at Tripler General Hospital; the Medical Field Service School at Carlisle, Pennsylvania; the Fourteenth Field Hospital, Korea; the Army Medical Service Graduate School; the Second Army Area Medical Laboratory at Fort George G. Meade; the Tropical Research Medical Laboratory at San Juan, Puerto Rico; USAMRIID at Fort Detrick, Maryland; and WRAIR at Walter Reed. His medical service embraced the fields of microbiology, virology, immunology, epidemiology, and tropical medicine. He made important contributions to cholera research in Dacca, Pakistan. The Jefferson Medical College of Thomas Jefferson University, the University of Kentucky College of Medicine, and the Gorgas Memorial Laboratory and the School of Public Health in San Diego have all had the advantage of his academic contributions.
Bud Benenson has served the Board and many of its Commissions, and he directed the AFEB`s Commission on Immunization for a number of years. He is an infectious-disease authority whose fundamental background is excellent, whose memory of historical findings is uncanny, and whose ability to correlate the old with the new is impressive. Bud now heads the Board`s Subcommittee on Infections, a public service which merely highlights his long list of contributions to the AFEB.
199
personnel, supply and logistics problems, obsolete equipment, and no diagnostic capabilities within Corps. Food supply is based on 90 days C-rations which probably will result in eating from unauthorized sources. In the Bright Star exercise (Egyptian desert) 75% of the officers developed diarrhea. Education on personal protective measures is essential and must be simple; field sanitation now depends on non-medical personnel, with no Disease Surveillance and Control Teams, which are essential. Vaccines will be needed for unconventional troops who might operate where no medical support could be provided.
Research Requirements. Col. Philip K. Russell, MC, WRAIR, reviewed and summarized the research requirements which include the need for field research to define the epidemiology of major threats including the incidence and distribution of the diseases; the antigenicity and drug sensitivity of agents involved; the biology, distribution and insecticide sensitivity of vectors. Present efforts are underway at NAMRU-3 on schistosomiasis, Rift Valley fever, [and] Crimean/Congo hemorrhagic fever vectors. In the Army laboratory in Kenya, leishmaniasis, trypanosomiasis, [and]vector taxonomy and biology are under investigation. Under rapid diagnosis, the methods, reagents and equipment must be designed; doctrine for deployment and field use in disease control and treatment need definition; [and] selected agents, such as arboviral, rickettsial and BW threat agents, [must be] defined. Specific research requirements under hepatitis include the development of a vaccine against HAV and basic knowledge of non-A non-B; under malaria, drug development and vaccine development; under schistosomiasis, increased information on anti-penetrants; under leishmaniasis, agent and vector taxonomy, immunology, chemotherapy; under dengue, quadravalent vaccine; under Rift Valley fever, ecology, vaccine improvement and development; under diarrheal disease, shigella vaccine, E. coli pilus vaccine; under rabies, validation of intradermal vaccination.
Preventive Medicine Policy and the RDF. Col. George E. T. Stebbing, MC, OTSG, summarized the present status and future needs of the preventive medicine policy and the RDF. Major stress must be placed on the personal responsibility for health, and area sanitation. Preventive medicine units must be defined into segments which constitute C-130 plane local units. Policy decisions must be made on the use of IG against hepatitis; the use of vaccine against HBV; chemoprophylaxis against malaria and the change from the emergence of resistant plasmodia; determination of where Rift Valley fever exists and to whom vaccines should be given; the use of pHisohex as an anti penetrant for schistosomiasis; chemoprophylaxis for diarrheas; and to whom should pre-exposure rabies vaccination be given. Decisions on actions will be limited by what the command will permit; the type and amount of equipment will be dependent on transport facilities.
Concluding Remarks. Col. Philip E. Winter, MC, who chaired the meeting, pointed out the need to establish priorities and at the moment he ranked in order: diarrhea, leishmania, and the need to define procurement, acquisition, and R & D requirements. To monitor priorities, a committee was appointed consisting of Col. Winter, Col. Russell, Col. Stebbing, Col. Tsoulos, Maj. Prier, (Chief, Department of Epidemiology, Division of Preventive Medicine at WRAIR) and the Director of the U.S. Army Military Intelligence Information Agency.
It is anticipated that the AFEB will be involved in developing some policy decisions. It is advantageous that Dr. Rammelkamp and I had the opportunity to understand the background.
Abram S. Benenson, M.D.
Director, Gorgas Memorial Laboratory
Dear Bud:
First, I wish to thank Rammel and you for having attended the ad hoc meeting on rapid deployment in relation to infectious disease threats. Your report was comprehensive and the Board profited by receiving this important information. During the recent meeting, the question of simplification of vaccine schedule for the Armed Forces was a topic of discussion. Apparently, this is now the time for an objective review of this important matter. To this end, I wish to appoint an ad hoc committee of the Board to cope with this matter. You are the logical one to chair this group and I hope that you will take it on. The persons whom I suggest for membership are to receive copies of this letter with the hope that they will serve. If you wish to have other persons meet with you, this can certainly be arranged. Bill Tigertt comes to mind as one who might be very helpful.
200
If you concur, I believe that the group might meet on February 3, the day before the full meeting of the Board. As you know, this meeting will be held at WRAIR and I see no reason why the preventive medicine officers of the three services could not attend.
Also, Bud, I am going to ask you to serve on the ad hoc committee to consider the long-term effects of multiple immunizations. On this one, I will expect Bill Beisel to do a lot of the leg work. He has a long-term memory of the problem since he has been stationed at USAMRIID and has access to numerous important details. Let me thank you for all that you have accomplished for the good of the AFEB. Indeed, I feel the same way about everyone who takes time from [their] very busy schedules to assist the Board in its various activities.
Sincerely yours,
Theodore E. Woodward, M.D.
President, AFEB
Colonel Philip K. Russell
Commandant
Walter Reed Army Institute of Research
Washington, D. C. 20012
Dear Phil,
You are well familiar with the workshop on Infectious Disease Threats and its relation to Rapid Deployment which was held at WRAIR on July 14-15, 1981. Bud Benenson and Charles Rammelkamp kindly participated in this conference as representatives of the AFEB. Based on the character of the brief minutes which Bud Benenson prepared,
I gather that the workshop was productive and also open to various important questions. Thank you for allowing the Board to be represented, and be assured that we wish to be of service whenever possible. Do you think it appropriate and possible for you or a designated person to inform the Board of certain important matters which pertain to Infectious Diseases and their Prevention? The specific items of consideration are briefly mentioned below, and I am asking Bill Jordan if he will cover these matters as far as the NIH is concerned. Bill and Rammel have raised these points with which I fully concur. They are:
1. What aspects of early diagnosis of Infectious Diseases and control measures are being pursued by WRAIR or USAMRIID?
2. What information can be provided regarding the stockpile of essential drugs and vaccines?
3. What are the names of the civilian agencies or University-oriented laboratories that are working in the field of early diagnosis of Infectious Diseases and their prevention? In this regard, it would be useful to learn of the sources of support for the specific studies.
It would be very useful if Bill Jordan, as well as you, could provide us information regarding these matters at the time of the next meeting of the Board. Time can be found in the agenda for this important information. It is essential that the Board be so informed so that its advice, when solicited, can be oriented in the right direction. Hopefully, this is not too much to ask.
Sincerely,
Theodore E. Woodward, M.D.
cc: William S. Jordan, Jr., M.D.
Charles H. Rammelkamp, Jr., M.D.
Abram S. Benenson, M.D.
Captain Charles W. Halverson
201
THE AFEB SUPPORTS THE OVERSEAS RESEARCH LABORATORIES
During World War II, laboratories for special research were established at various geographic sites. The U.S. Navy established its Naval Medical Research Unit Number 2 (NAMRU-2) on the island of Guam. Later, the Department of the Navy inaugurated similar units in Cairo, Manila, Jakarta, and elsewhere. Special laboratories sponsored by WRAIR were established in Kuala Lumpur in 1948, and in Bangkok in 1959. These and other Overseas Laboratories enjoyed a record of excellence in medical research that was of vital importance to the Department of Defense.
Congress questioned the need for the Overseas Laboratories and discussed placing their research programs, which were located in foreign countries, under civilian sponsorship using contractual agreements. Another possibility was to eliminate them. When the Board heard this, it devoted several meetings in 1979 and 1980 to this critical issue. Dr. Reuel A. Stallones, Dean of the University of Texas School of Public Health and a former AFEB member, served as a consultant to a special Defense Department committee charged to pursue the matter. On 6 May 1980, Dr. Stallones sent me the following letter:
Dear Ted:
While serving as consultant to the Department of Defense on the proposed closure or change of sponsorship of the military overseas medical research laboratories, a number of issues emerged which were of special interest to me personally, and which do not fit well into a formal report. Since the suggestions involve the Armed Forces Epidemiological Board, I thought a submission directly to the Board would be the most useful step. The suggestions presuppose that the laboratories will continue to function under their present sponsorship, which is by no means assured.
1. Oversight. Significant value would accrue if a formal advisory board were established to provide continuing consultation on the mission and performance of the laboratories. The Armed Forces Epidemiological Board is an obvious locus for such a function. Evidently the ommitment should be more than casual, and should entail frequent visits to the laboratories.
2. Integration. The report entitled "New Directions in International Health Cooperation," submitted to President Carter in 1978 by Dr. Peter Bourne, noted that the military laboratories could be expanded to become centers for regional training in clinical tropical medicine. This leads to the need for serious consideration of regional organization of military research, generally. Presently NAMRU-2 (Manila and Jakarta), AFRIMS (Bangkok), and USAMRU (Kuala Lumpur) represent a very strong base for coordinated research and training efforts in Southeast Asia and the Western Pacific. NAMRU-3 (Cairo) and USAMRU (Kenya) could serve as the foci for regional programs in North Africa and the Middle East, and in Central Africa. Notably lacking is a strong research base in Latin America, for the U.S. Army presence in Brazil is modest. Perhaps the Armed Forces Epidemiological Board could take the lead in proposing expansion and integration of the DOD overseas medical research programs, with a view to achieving a globally balanced strategy. These notions were not originated by me, but arose in a number of conversations of different groups. However, I have not had an opportunity to review these suggestions with anyone else, and therefore I am sending them to you without presuming to represent others` views.
I am sending copies of this letter to Dr. John Moxley and Dr. Phillip Winter, since their responsibilities relate to the subject. Thank you for listening.
Yours sincerely,
Reuel A. Stallones, M.D., M.P.H.
The Board`s reaction and the action that it took in regard to this important matter are described in the following letter, dated 3 June 1980,which I sent to the Secretary of Defense. The response, dated 30 June 1980, is from Walter B. La Berge, the Principal Deputy Undersecretary of Defense.
202
REUEL ARTHUR STALLONES, M.D., M.P.H.
Stony accomplished many things following his internship, service as a battalion surgeon, and service as as a Preventive Medicine Officer and epidemiologist in the military. He taught preventive medicine at the University of California at Berkeley. At the University of Texas School of Public Health in Houston, where he was Professor of Epidemiology, Stony also assumed the duties of that school`s first Dean in 1968. Under his leadership, master`s and doctoral degrees in science, public health, and a wide range of fields related to public health were inaugurated and awarded.
Despite his heavy academic responsibilities during this period, Stony contributed in full measure as a member of the AFEB, never swaying from his belief that military and civilian medicine were comparable in certain of their objectives. His wisdom and perception helped the Board in its relationships with the military, and his role in maintaining the security of the Department of Defense`s Overseas Research Laboratories was appreciable.
203
SUBJECT: Department of Defense Overseas Medical Research Laboratories
The Honorable Harold Brown
Secretary of Defense
Room 3E880 Pentagon
Washington, D. C. 20301
Dear Mr. Secretary:
The Armed Forces Epidemiological Board (AFEB) expresses its concern over the proposal that military medical research laboratories in foreign countries be reduced in their scope, eliminated or placed under civilian management by contractual arrangements. The Board devoted portions of its last two meetings to discussion of this important matter. Its considered judgement is that such action would lead to an unacceptable reduction in military operational and research capability. Any savings to our government in terms of expenditures for personnel and operational costs would be trivial in comparison with the loss.
Board members feel obligated to voice their concern in view of the AFEB mission "to provide timely advice and recommendations concerning operational programs, policy development and research needs for the prevention of disease and injury and the promotion of health." Its competence to do so lies not only in its forty years of institutional involvement with military medical research programs, but also in the long personal and productive experience of several of its current members who have been active either in the direct operation of, or as consultants to, military medical research in supporting laboratories either in the United States or abroad.
These scientists are recognized authorities in various health fields.
The requirement for maintaining the overseas laboratories is unquestioned. It is essential that the Department of Defense maintain them in order to meet its known and anticipated military operational requirements pertinent to diseases and other adverse health risks peculiar to foreign environments. The United States must keep abreast of all indigenous disease or health threats such as malaria, scrub typhus, encephalitis, hemorrhagic fever, environmental changes and others wherever and whenever they may directly affect the ability of U.S. forces to function effectively. Certain of the essential functions of overseas military medical research laboratories are:
a. Research. Development of new knowledge and the resultant technologic and control programs depend directly on the long-term commitment of scientific investigation directed to problems which occur naturally in a particular country. American forces encountered malaria, scrub typhus, dengue and other disorders throughout the Southwest Pacific Islands, Indochina and Asia when troops functioned in the field. Many of these threats are unsolved and remain military problems.
b. Training. To maintain a cadre of experts and develop new competence in medical conditions to which military forces are exposed overseas, it is essential to maintain, improve and develop both facilities and scientific personnel before there is an operational necessity. Examples of the importance of medical research and our abysmal lack of capability occurred when American troops encountered scrub typhus, malaria and dengue fever in the Pacific Islands, drug-resistant falciparum malaria in Vietnam or highly fatal hemorrhagic fever in Korea. These are glaring examples. The threat of Rift Valley fever in the Middle East and virus infections, such as Lassa Fever or Marburg, and Ebola virus infections in Africa are current major threats to military security. Much progress has been made through research conducted in overseas military laboratories, and there is now a coordinated program directed to development of means of control throughout the military system. It is unlikely that any civilian institution would direct its interest to these unsolved problems simply because they are peculiar to the military mission.
c. Surveillance. There is no question of the value of foreign military medical laboratories and their ability to collect and cull the type of important epidemiologic information which is essential for long-term planning and determination of predictability. Military necessity makes it essential that experts be informed of military needs through their strategic placement throughout the world. They must be constantly involved in collection and interpretation of relevant data. The first isolation of the Asian strain of influenza virus in 1957 was in a military installation located in Asia. It is fundamental to the security of the United States that military medical laboratories be broadly conceived and developed world-wide. It is true that these laboratories would profit from better integration; it is quite unlikely that any civilian agency would have the interest, enthusiasm and broad capability to conceive, develop and integrate such programs. There is alack of military research presence in Latin America which merits early and serious consideration. The question may be logically raised why the military services should direct the overseas research programs. Experience through decades makes it abundantly clear that the required
204
capability and interest exists only in the military system. In no way does this derogate the outstanding contributions made by career civilian DOD scientists who have worked productively in these laboratories. These scientists have contributed to the planned and relevant military research problems designs and programmed for these laboratories. Factors which forcefully favor military sponsorship are:
a. Continuity. To insure continuity of capability it is essential to have management by, and involvement of, career military personnel who can alternate their tours of duty between domestic and foreign laboratories that are engaged in research on common mission oriented problems. These are problems unique to the military.
b. Responsiveness to Problems. The ability to respond to military demands is more direct and flexible when scientific facilities are under military command responsibility. Sponsorship by the contract mechanism is so awkward and clumsy as to preclude rapid change in response to military needs. The result can be costly delays.
c. Availability o f Key Scientific Personnel. There is a serious limit to the availability of highly qualified civilian scientists who would work in a civilian controlled laboratory overseas. There are striking examples of gross failure of civilian agencies to recruit personnel and to develop and maintain health care systems when placed in strategic overseas areas. This cannot be said of those established medical laboratories which continue to be productive and viable in Asia and the Middle East.
d. United States Presence. The presence of medical military laboratories in allied foreign countries has favored our national policy particularly when there has been a long-term experience in that country. In spite of political pressures and diplomatic strains, the host governments have maintained their favor in our medical laboratories. It is doubtful that civilian managed laboratories on a short-term basis could develop or enjoy this relationship.
e. Lasting Power. The record is conspicuously clear that the grant or contract mechanism has been devoid of lasting effect when civilian laboratories have been established in foreign countries. Centers have been sponsored by the USPHS, the Center for Disease Control, and NIH. USAID has sponsored other programs. The International Centers for Medical Research and Training were established in 1960 in five foreign countries by five civilian institutions. All but one of these have been phased out. The emergence of nationalism and increased anti-colonialism have shifted from free study U.S. programs to collaborative partnerships with visiting and local scientists who work on problems of mutual interest. Projects such as the NIH- and AID-sponsored Cholera Research Laboratory have been internationalized with an independent Board of Directors.
Attention must be paid to this historical record. It is unlikely and unrealistic to expect any civilian U.S. contractor to maintain any installation comparable to the current overseas military laboratories. The contracting agency would lack the welcome which is extended to the military by a friendly government. A private contractor, whether a University or institutional group, would encounter difficulties in maintaining proper relationships with civilian and governmental agencies in host countries. At times, the civilian agencies are considered competitive in contrast to relationships established by a Department of Defense activity.
The AFEB concludes and makes the following recommendation with strong conviction: That the United States military continue to operate laboratories in selected foreign countries for: (1) the development of new knowledge relative to the military mission; (2) the maintenance and development of a core of military personnel with appropriate scientific capability and expertise; and (3) the surveillance of medical problems as they relate to military needs.
These objectives require maintenance of medical laboratories that are promptly responsive to Department of Defense coordination and mission requirements, some of which can change without warning. These needs cannot be met satisfactorily by contracting such functions and responsibilities to a civilian agency, nor is it reasonable to assume that continuity or reliability of performance can be assured under such sponsorship.
Not only does the AFEB urge the maintenance of the currently existing programs, but it recommends that the military mission be better planned and programmed on a more logical and comprehensive world-wide system, i.e.,[that] DOD overseas medical research programs be designed to achieve a globally balanced strategy. For example, there is no strong research base in Central or Latin America, a hemisphere which is most important to the United States.
The Board is willing and enthusiastic in its desire to assume an advisory role.
Sincerely,
Theodore E. Woodward, M.D.
President, Armed Forces Epidemiological Board
205
Dear Dr. Woodward:
This is in reply to your letter of 3 June to the Secretary of Defense concerning the overseas medical research laboratories.
The proposal to close or contract for the operation of these laboratories did not arise within the Department of Defense. We have been afforded an opportunity to raise further arguments in rebuttal.
To this end we have recently concluded a study of the laboratories, their value to the Department of Defense and the feasibility of contracting-out their operation. I understand that the Board has been briefed by my staff on the progress of this study.
The study report concludes that the laboratories are a valuable and productive resource and that contracting for their operation would be infeasible and, in any case, counter-productive.
Unless you object, we will include the Board`s views with the study report, so they may be considered by those who will make the final decision on the issue.
Thank you for your thoughtful and constructive comments.
Sincerely,
Walter B. LaBerge
Principal Deputy [Undersecretary of Defense]
The Board responded that it would be pleased to have its views used to support the issue at hand. Ultimately, the Overseas Laboratories were maintained under the administrative responsibilities of their sponsoring military service. Hence, the Board was able to render counsel and advice that helped lead to a favorable decision.
Later, in 1980, a fortuitous opportunity permitted the Board to interact directly in investigative activities with an Overseas Laboratory. Dr. Stephen L. Hoffman, of the U.S. Naval Medical Research Unit No. 2 (NAMRU-2), Jakarta Detachment, informed me in a letter that a particularly severe form of typhoid fever, with associated shock and high fatality despite specific chemotherapy, prevailed in Jakarta. The mortality rate was said to far exceed that in other areas where typhoid fever was known to be endemic. It was clear from his letter that Dr. Hoffman was well-informed regarding the various pathophysiological abnormalities associated with typhoid, and he asked for suggestions for any indicated therapeutic approach. Corticosteroids had first been used in typhoid patients as early as 1950, under AFEB sponsorship, but I told Dr. Hoffman that proof of their efficacy had never been established, in spite of the fact that steroid treatment in severely ill typhoid patients was generally used. Excerpts from this 1980 correspondence follow:
7 July 1980
Dear Dr. Woodward:
As a consultant and investigator at the infectious diseases hospital in Jakarta, Indonesia, I see 5 to 10 new patients per week with bacteriologically confirmed typhoid fever (our lab). Of particular interest to me is the fact that many of these generally young (15-35 years),relatively well nourished patients with no underlying diseases present with severely abnormal states of consciousness. While appropriately 80% of the patients are apathetic on admission, 40% of the total number of patients have disorders ranging from delirium, which is often agitated, to obtundation, stupor, and coma. Most of them have fever outside the hospital for 7 to 10 days treated with oral antibiotics (often chloramphenicol). Although several patients have been in shock, most of them have adequate blood pressures, systemic perfusion and urinary output as well as no evidence other than abnormal mental states to suggest inadequate oxygenation, and no evidence clinically of DIC. Laboratory testing in this setting has thus far been inadequate but most patients tested have had normal electrolytes as well as uniformly negative cerebrospinal fluid examinations. The mortality rate in this group is approximately 10%, with those presenting in coma or with convulsions faring the worst. However, most recover slowly, but completely, with mental status returning to normal
206
approximately seven days after temperatures have returned to normal....
Enclosed is a tentative outline of how we will be approaching this group as well as a control group with typhoid and normal mental status. This is a fairly standard approach and I would appreciate hearing from you as to your ideas on the pathogenesis of this disorder as well as ways that we might approach the study of it....
Sincerely yours,
Stephen L. Hoffman, M.D.
Head, Department of Clinical Investigation and Epidemiology
NAMRU-2
24 July 1980
Stephen L. Hoffman, M.D.
Head, Department of Clinical Investigation and Epidemiology
U.S. Naval Medical Research Unit No. 2 Detachment
APO San Francisco 96356
Dear Dr. Hoffman:
Thank you for your letter of 7 July 1980 in which you bring out some of the opportunities which you have in connection with problems relating to patients with typhoid fever. I gather that your experience is voluminous to say the least.
There are some important problems which relate to pathogenesis of typhoid fever and its management which are unsettled. Some of these issues can only be settled or only partially settled in an area where there is a heavy influx of patients. It sounds to me as if you are experiencing some good old-fashioned virulent typhoid fever.
Would it be possible to obtain skin biopsy sections of the rose spot of typhoid?
Would it be possible to pass a cantor (gastric duodenal tube) tube in some patients, collect bile and/or perform a biopsy o fthe upper small intestine? We have found these procedures harmless but informative, particularly when immune-fluorescence techniques are used.
Do you think the number of patients is sufficient for a careful alternative study of two effective therapeutic regimens? Would this type of treatment be acceptable on the condition that the wo forms of treatment are regarded as comparable? One of these techniques would probably involve the use of corticosteroids along with an antibiotic, etc.
It is presumed that specimens of serum could be collected for special blood studies such as fractionation of amino acids and endotoxin assay, etc. Also, studies of lymphocyte transformation are important.
Let me hear from you about the above. Actually, you stimulated my interest when you raised the question of developing a collaborative study.
Sincerely yours,
Theodore E. Woodward, M.D.
Dr. Hoffman and his associate, Dr. Narain Punjabi, with advice from Dr. Sheldon E. Greisman of the University of Maryland faculty, developed a plan of study on recommended high doses of dexamethasone. The protocol was approved through the usual channels. Funds to conduct the study, beyond those available to NAMRU-2, were raised from Parke Davis and Company. The clinical study was completed in Jakarta with highly successful results, which Dr. Hoffman and his associates reported and published. (Hoffman, SL; Punjabi, NH; Kumala, S; Moechtar, A; Pulungsih, SP; Rivai, A; Rockhill, RC; Woodward, TE; and Loedin, AA. Reduction of mortality in chloramphenicol-treated severe typhoid fever by high-dose dexamethasone. New Eng. J. Med. 310: 82-88, 1984.)
207
The AFEB and the Annual Meetings of the Overseas Commanders
This clinical investigative activity prompted me to visit NAMRU-2 in Jakarta several times during my visits to other DoD Overseas Laboratories in Bangkok and Kuala Lumpur. The Overseas Commanders in 1982 were: Commander Patrick Carney, in Jakarta; Lt. Colonel Michael Gross, in Kuala Lumpur; and Colonel Michael Benenson at AFRIMS, in Bangkok. I also visited the NAMRU facility in Cairo, where Captain Ray Watten was Commander.
During these visits, it was obvious to me that relevant research, very important for the military mission, was being conducted in all units. Furthermore, in several of the units, Army and Navy Department scientists were working collaboratively with civilian scientists. After my discussions with the investigators overseas, it became clear to me that better collaboration and communication between individual Overseas Laboratories and the base laboratories in the United States would serve a useful function.
To this end, in 1982, I transmitted this concept to Maj. General Garrison Rapmund, Commander of the Army`s Research and Development Command, and to Captain James F. Kelly, Commander of the Navy`s Research and Development Command. Colonel Philip Russell, Commandant of WRAIR, was also consulted. A suggestion was made to hold workshop meetings at WRAIR, or other appropriate sites, in the early winter when the Commanders of the Overseas Laboratories and other laboratory personnel regularly attended the meetings of the American Society of Tropical Medicine. These meetings would provide a forum for the Overseas Laboratory personnel to meet and discuss scientific matters and to determine, whenever possible, how joint efforts, the avoidance of duplication, and suggestions for new leads might better promote relevant military research in the overseas sites.
Meetings of the Overseas Commanders have been held annually since 1982. Much progress has been made in coordinating their research and in developing better understanding of their mutual problems. Steps have been taken to allow working personnel at all levels to discuss both scientific matters and administrative difficulties during workshop conferences. Maj. General Rapmund; Maj. General Philip Russell; Captain Kelly, USN; Colonel Frank Top; and Colonel Fred Tyner, as well as the Overseas Commanders, have contributed to the success of these meetings.
A comprehensive meeting of the Overseas Laboratory Commanders was held at WRAIR on 1 December 1988. The programs of the various laboratories were thoroughly described by each Overseas Commander or associated staff personnel. Discussions were directed at coordinating and expanding specific research projects, with the aims of avoiding duplication and expanding new knowledge. The agenda for that meeting appears on page 208.
On 2 December, the Commanders and other overseas personnel visited the WRAIR and NAMRI laboratories. Maj. General Philip Russell, Commander of the U.S. Army Medical Research and Development Command, sent me the following letter, dated 30 December 1988:
Dear Dr. Woodward:
Thank you for your participation in this year`s Overseas Laboratory Commanders Conference. Your presence at these gatherings is always welcomed by both Army and Navy field commanders. It did not escape my notice that this was the seventh in a series of these conference since they were begun at your suggestion in 1981. These meetings are another tangible benefit resulting from the involvement of the Armed Forces Epidemiological Board in the infectious disease research program of the three Services. The interaction between the Board and our researchers in the field has been extremely valuable to us, both in terms of program direction and in terms of stimulating and guiding our young research scientists. Several of our young officers have remarked to me how much they have valued your visits to the overseas laboratories. Your continued involvement in our program, and the involvement of other members of the Board, is always welcome. Best regards.
Sincerely yours,
Philip K. Russell, Major General, Medical Corps, Commander
208
|
The Agenda of the 1 December 1988 Meeting Walter Reed Army Institute of Research 0800 Registration 0830 Welcome: Col. C. Fred Tyner, Director, WRAIR 0840 Introduction: Capt. J. Woody, CO, Navy MRDC 0850 Introduction: Maj. Gen. P. Russell, CDR, USAMRDC 0900 Army Infectious Disease Program: Col. D. Robinson 0930 Navy Infectious Disease Program: Capt. L. Laughlin 1000 Break 1020 AFRIMS (Thailand): Col. F. Sodetz 1050 USAMRU-M (Malaysia): Col. G. Lewis 1110 NAMRU-2 (Philippines): Capt. J. Coolbaugh 1130 NAMRU-2 DET (Indonesia): Cdr. F. Paleologo 1150 USAMRU-ROK (Korea): Col. K. Dixon 1210 Lunch 1330 NAMRU-3 (Egypt): Capt. M. Kilpatrick 1400 USAMRU-K (Kenya): Col. C. Roberts 1420 Break 1440 NAMRI-DET (Peru): Cdr. R. Buck 1500 USAMRU-B (Brazil): Maj. (P) McGreevy 1520 Break 1540 HIV: Col. E. Tramont 1600 HIV Discussion 1610 General Discussion 1630 Cash Bar, Officers` Club (WRAMC) 1800 Catered Dinner (Barbecue) WRAIR
|
The fortieth anniversary meeting of USAMRU (Malaysia) was held at WRAIR on 24 February 1988. Members of the AFEB, WRAIR, USAMRIID, NIH, and invited guests attended. The meeting`s agenda illustrates not only the important military medical research that has been conducted at USAMRU during the past forty years, but also the close collaboration between the AFEB and the DoD Overseas Laboratories. That agenda follows:
209
|
The Agenda of the 24 February 1988 Meeting 0900 Welcome: Col. F. Tyner 0905 40th Anniversary Celebration-Introduction: Maj. Gen. P. K. Russell I. Scientific Achievements-The University of Maryland Period 1948-1962 0915 First Specific Treatment for Scrub Typhus and Other Infections: Dr. T. E. Woodward 0945 Typhoid Fever and Chemoprophylaxis of Scrub Typhus: Dr. H. L. Ley, Jr. 1015 Fevers of Unknown Origin: Dr. P. A. Webb 1035 Break 1050 Medical Ecology: Dr. R. Traub 1140 Encephalitis: Dr. P. Paterson 1150 Discussion 1200 Lunch II. Scientific Achievements-The Post-Maryland Period 1300 The Ecology of Scrub Typhus: Maj. Gen. G. Rapmund 1320 Forest Ecology: Dr. I. Muul 1340 Doxycline Prophylaxis: Col. M. Groves 1400 Current Studies: Lt. Col. G. Lewis 1420 Discussion III. International Cooperation 1430 Collaborative Studies with the Institute for Medical Research: Dr. R. Traub 1440 Collaborative Studies with The Commonwealth Force: Dr. C. Dulake 1500 Volunteers, Then and Now Discussion: Dr. B. Elisberg 1520 Break IV. The Joseph E. Smadel Lecture 1530 Introduction of Dr. C. L. Wisseman, Jr.: Dr. B. Elisberg 1535 Epidemic Typhus: Dr. C. L. Wisseman, Jr. 1630 Adjourn V. Evening Program 1700 Gather for Dinner 1800 Dinner 1900 Introduction of Speaker: Maj. Gen. P. K. Russell 1915 Collaborative Efforts between the University of Maryland and the U.S. Army: Dr. T.E. Woodward
|
In fulfilling its advisory role, the AFEB has helped support and coordinate the activities of the Department of Defense`s Overseas Laboratories. This help has often taken the form of establishing an informal working relationship with a qualified academic center whenever that was appropriate to the program`s mission. Not the least of this support has been the AFEB`s assistance in recruiting key personnel.
210
{kind=link}
Bill Tigertt was closely affiliated with the AFEB and several of its Commissions during his distinguished military career. With the advantages of his remarkable experiences in laboratory medicine and his accurate bibliographic memory, Bill applied his capability in pursuit of those infectious-disease problems that he confronted. He gained broad experience in tropical diseases in New Guinea and the Philippines as Director of the 26th Army Laboratory and at the 406th General Laboratory in Tokyo. Malaria, other parasitic diseases, and enteric infections were rampant. Later, under his guidance as Commander of the U.S. Army Medical Unit at Fort Detrick (later USAMRIID), many of the problems of pathogenesis, pathophysiology, and control of viral and rickettsial diseases were clarified He held the rank of Brigadier General when he retired from the Army Medical Corps.
Bill was the principle force behind the thrust to find better prophylactic and chemotherapeutic controls of malaria. He collaborated closely with the Commission on Epidemiological Survey, and was a member of the AFEB`s Commissions on Malaria, Virus Diseases, and Parasitic Diseases.
211
THE DENSEN REPORT
The Board has always responded to requests by the respective Surgeons General and the Office of Health Affairs in the Department of Defense on standards and procedures related to health care, health standards, and data-collection systems. Several ad hoc committees and task forces addressed these health issues for the Board. Dr. Paul Densen, a leader in this field and a dedicated Board member, kindly responded to my request that he prepare a chronology of these proceedings and an historical commentary. The document that he produced, which is of significant historical importance, follows. It deals with the AFEB`s activities related to physical standards, frequency of examinations, population-based forecasting, epidemiological methods in the health-care delivery system, the ambulatory care data base, readiness-related issues, and the health care of women in the armed forces.
The AFEB, The Setting of Health Standards, and the Application of Epidemiological Concepts
to the Study of the Health of the Armed Forces:
A Chronology and Commentary
Background
Late in 1978 the Armed Forces Epidemiological Board was formally reorganized into three subcommittees:1
a. The Subcommittee on Disease Control
b. The Subcommittee on Environmental Health
c. The Subcommittee on Health Maintenance Systems
The establishment of the Subcommittee on Health Maintenance Systems constituted an expanded area of activity for the Board. While its concerns inevitably overlap those of the other two subcommittees, the designation of a separate subcommittee represented specific recognition of the importance of dealing with individual disease entities and environmental hazards. At the same time, it was recognized that central to the concern of all three subcommittees must be the development of an appropriate data base to aid in the early detection of departures from health, provide management with the tools for resource analysis, and furnish epidemiological information on the distribution of health and disease in the Armed Forces which ould serve as a point of departure for more detailed research efforts. In brief, the Subcommittee was to provide "scientific evaluations and recommendations concerning:
a. The assessment of those physical, nutritional, behavioral, hereditary and other characteristics of individuals and populations which are associated with chronic disease and disability.
b. Those programs which can be implemented to prevent or decrease lost time duty for Armed Forces personnel, and
c. Those epidemiological and management techniques applicable to the design of more efficient health service programs, particularly with regard to preparations for varied operational contingencies."
The activities under this charge follow:
Activities
Periodic Medical Examinations. In March of 1975, Col. Robert T. Cutting, M.D., Chief, Health and Environmental Division, DOD, requested the AFEB to review the scope of the periodic medical examination [(PME)] in the Armed Forces. The usefulness of the examination was in question and the shortage of medical manpower dictated that the entire policy be reviewed.
In response to Dr. Cutting`s request, Dr. Lennette, President of the Board at the time, appointed an ad hoc study team which made its report in March of 1976.2 The report included a suggested procedure for review of the PME and resulted in the appointment of a Subcommittee with Dr. Paul Densen as chairman to review the subject in detail. The Subcommittee held its first meeting in January, 1977 and submitted its report to the Board at its February meeting
212
Paul Densen has had a distinguished career as a counselor and administrator of health services, particularly as they relate to health care, community health planning, and health needs. He is the doyen of health-care consultants in the United States and is called upon by national groups with problems in this field.
The AFEB was fortunate to have attracted Paul Densen as a member in 1975. At that time, shortly before the Board broadened its interests in the field of infectious diseases, Paul Densen brought a sorely needed brand of expertise, and chaired the Board`s Subcommittee on Health Maintenance. Urgent, longstanding problems were frequently presented to the Board by the Surgeons General of the three services and the Office of Health Affairs. Paul assisted the military services in their planning for health care, health standards, and population forecasting, and particularly the special problems associated with the delivery of health care to large groups. Members of the Subcommittee performed in-depth studies, visited many military installations, and made exhaustive, objective recommendations regarding health care and statistical analysis. These were of inestimable value to the Department of Defense, and Paul Densen deserves the lions share of the credit. Always responsive, he never failed to accept a request and carry the problem through to its solution.
213
Dick Remington is a product of the University of Montana and the University of Michigan. After receiving his doctorate at Michigan, he served with Dr. Thomas Francis as an epidemiologist in that outstanding School of Public Health. Later he served as the Dean of the School of Public Health at Michigan.
The Board was fortunate to attract Dick Remington as a member. A practical and wise epidemiologist, he has helped solve various problems that were posed by the three medical services. His contributions have included recommendations pertaining both to data collection for ambulatory medical care systems and to population forecasting of the need for current and future procedures pertinent to inpatient and outpatient services. He has also worked on problems associated with acquired immune deficiency syndrome, particularly in developing practical guidelines for disease control.
214
in 1979.3 The Board approved the report and forwarded its recommendations to the Assistant Secretary of Defense (Health Affairs) and the Surgeons General in March of the same year.4
A number of detailed recommendations were made, the gist of which was that the PME, as then constituted, be abandoned. In its place it was proposed that a minimal health examination be integrated into the general medical program, the content and frequency of which were specified in the report. The report emphasized that the minimal health examination should serve to place examinees into risk groups and that the frequency and content of subsequent examinations should be governed by the nature of the risk. Manpower considerations were discussed and recommendations made as were recommendations for improving the management and monitoring of the program.
Subsequent to the Board`s report, a number of changes were made in the medical examination standards which move the procedure in the direction recommended by the Board.
In 1973, regulations required medical examinations every four years for Army personnel aged 19 through 39, every two years from ages 39 through 49, and annually thereafter. Since 1980, following the Board`s report, examinations are required every five years from ages 20 through 60, and annually thereafter. General officers are examined annually regardless of age.
The principle that the examination should serve to place individuals into risk groups and that subsequent examinations should be dictated by the nature of the risk has been adopted. For personnel over forty, procedures such as rectal examinations, cardiovascular screening, mammography and Pap smears have been instituted. Recently, the Army has initiated health risk appraisals which place the individual into risk groups based upon replies to a check list. A computer scans the check list and calls for further examination if the individual is identified as having a high risk life style.
The original stimulus for review of the PME was its low yield as then constituted with resultant inefficient use of scarce manpower. The extent to which the changes described have improved the situation should be examined periodically and the findings made available to the Board.
The risk-correlated approach to health maintenance has been particularly evident in a long-standing collaboration between the Air Force and the Army. The Navy, while not formally involved, has expressed keen interest. However, as far as is known at this writing, a coordinated, tri-service approach to a health examination program is still in the future.
Population-Based Forecasting. In 1973, at the direction of the President, a Military Health Care Study (MHCS)5 was undertaken charged with, among other things, making "appropriate recommendations for modifications to improve the Military Health Services Systems." The 1975 report of this study called particular attention to the lack of reliable information on the size and characteristics of the population eligible to receive benefits from the system and on the patterns of utilization of the system by the eligible population. The report "recommended that DOD adopt a planning process for CONUS which is based primarily on the demographics of the population to be served."
In response to this recommendation, the Office of Program Planning and Policy Analysis (OPPA) was established in 1980 in the Office of the Assistant Secretary of Defense, Health Affairs. One of the tasks assigned to OPPA was to develop population-based forecasting models designed to permit appraisal of the impact of policy changes on the Military Health Care System both in the direct care of service personnel and in the care of dependents. In November of 1980 Dr. John H. Moxley, III, then ASDA(HA), requested the AFEB to assess the "structure, accuracy and potential usage" of the population-based forecasting models being developed by the OPPA and asked that Dr. Densen participate in this assessment.6
Dr. Densen submitted his report to the Board in September of 1981. The Board approved the report and forwarded the recommendations to the ASD(HA) and the Surgeons General in the following month.7There were three overall recommendations:
1. The population-based forecasting activities of the OPPA should continue to be supported.
2. The activities of the OPPA in this area should be integrated with the medical statistics activities of the three services.
3. The ASD(HA) should request the AFEB to conduct and report on annual review of the population-based forecasting activities of the OPPA.
The last of these recommendations warrants some elaboration. The report dealt at some length with the potential uses of the information being developed by OPPA, pointing out that the need to know the population exposed to risk
215
pervades almost every management, policy and research activity undertaken by the Armed Services. Over the years the AFEB has repeatedly had occasion to comment upon the lack of such information, as indeed did the Military Health Care Study and as have outside consultants such as the Rand Corporation. The recommendation for an annual review was designed to ensure that the issue receive the attention its importance warrants. The recommendation also sought to provide an educational device for all parties concerned.
So far as is known no action on this recommendation has been taken to date.
In 1984 the functions of the Office of Program Planning and Policy Analysis were assumed by Dr. Mestrovich and his staff at the Defense Medical Systems Support Center (DMSSC). Population data by age, sex, beneficiary and geographical regions continue to be collected through the DEERS program. Responsibility for analyses and distribution of the data have been assigned to Norma St. Clair in Dr. Mestrovich`s office.
Although the availability of such population estimates represents a considerable advance over the previous situation, bringing these data together with numerator data in a systematic manner to form prevalence and/or incidence rates for the three Services is still sporadic. In view of the numerous recommendations in this regard which have been made over the years, this is deplorable and deserving of greater attention. One approach to developing such rates is embodied in the interim recommendation of the Ambulatory Care Data Requirements Work Group discussed below.
Epidemiological Methods in the Health Care Delivery System. At a meeting of the Board in September of 1980, Dr. Eric Gunderson presented a report on the Navy program on epidemiological models and management and clinical services in health care systems. Dr. Woodward placed discussion of this report on the agenda for the meeting of the Board in September of that year.
The Gunderson report provoked lively discussion which emphasized the need to bring together numerator and denominator information as a basis for epidemiological examination of the health of the Armed Forces and to provide the tools necessary for more effective management of the health care programs of the three services.
Following this meeting, Dr. Woodward appointed a Task Force with the charge "to better define and develop a program aimed at formulating epidemiological methods in the clinical health delivery system which will utilize all services and benefit all services in a manner which is peculiar to their needs."8 This initial Task Force was chaired by Dr. Herschel Griffin who was later succeeded by Dr. Richard Remington when the former`s term on the Board ended. In April of 1982, the Task Force submitted two resolutions to the Board which were forwarded to the ASD(HA) and the Surgeons General. One of these recommended "that as soon as possible(reports on health service utilization, occurrence of disease and other health indicators) include, in addition to counts, rates based on denominator data reflecting populations at risk." The other resolution expressed the Board`s willingness to assist in a planned annual review of the Office of Health Policy, Planning and Systems.
Subsequent to the April 1982 report, the Task Force received on-site briefings on the Navy Occupational Health Information System (San Diego), the Army Outpatient Information Test System (Brook Army Medical Center) and the Air Force`s Outpatient Computerized Occupational Health Program (Brooks AFB, Texas). These briefings culminated in a report to the Board at its March 1982 meeting containing several recommendations which were approved and forwarded in the usual manner.
After noting that the development of health care related information by the three Services was [impressive] and deserving of support, it was further recommended that "expansion of the informal dialogue occurring among the three services should be encouraged with each service developing its own phased implementation plan to provide a longitudinal health record on military personnel and their dependents." Referring to the information systems being developed by the Services another recommendation stressed that a "minimum requirement of these systems should be a capability to compare populations at risk with populations receiving care(matching numerator and denominator data)." Again, it was indicated that "the AFEB would like to be a contributing participant in the evolution of health care information systems...."
Following the Remington report there appears to have been organized in the Office of the Assistant Secretary of Defense(Health Affairs) a Health Studies Task Force with Colonel Redman as its chief. The Task Force undertook a study whose objectives were to:
1. Assess the utility and
2. The feasibility of transferring individual inpatient data to the Health Affairs Data Management Information System [DMIS] and then
3. To develop a mechanism to interface this data with other data modules in DMIS.
216
In June of 1984, the Task Force issued a draft report in which it was concluded it was both useful and feasible to transfer "archive copies of the Services individual inpatient data systems to the Data Management Information System of the OASD(HA)."
[The] June 1984 draft report of the Task Force may be considered a follow-up on the Remington report designed to provide DOD with the kind of information needed for the effective management of its health care program. The Task Force continues to function on a contingency basis (see the discussion below on readiness) under the direction of Lt. Colonel Antoinette Hagey. Contemporary issues have included smoking, nutrition, cardiovascular screening and cholesterol testing.
Ambulatory Care Data Base. A major part of the resources of the Military Health Care System (MHCS) is devoted to providing ambulatory care services to military personnel and their dependents. Yet, as pointed out in the Health Studies Task Force draft report "complete individual ambulatory utilization experience among the population is not now (1984) being collected by the services."10
The lack of ambulatory care information is not due to failure to recognize the problem. Almost every review of the health care programs of the three services for the past twenty years or so has noted the advantages to be gained from the availability of such information from the clinical, epidemiological and administrative points of view. Indeed, as noted in the Remington report, individual installations in each of the Services have striven to address the issue and at its 1985 Fall meeting, the Board heard a presentation on the development of an Ambulatory Care Data Base at Fort Sam Houston. This effort was begun as an Army initiative in 1982 by LTCs Terry Misener and John Coventry.
The search for a practical approach to the development of ambulatory care data continues. In September of 1966 an Ambulatory Care Data Requirements Work Group with Norma St. Clair as coordinator was organized as part of the Composite Health Care Systems, which in turn is part of the Defense Support Systems reporting directly to the ASD(HA) on database issues. Ms. St. Clair presented the plans of the Work Group to the AFEB in October of the same year and subsequently Dr. Densen attended one of the meetings of the Group and received Minutes of other meetings.
This effort received a setback in May of 1987, when Surgeon General Becker indicated that the Army was "preparing to discontinue testing the Ambulatory Care Data Base" because it could not "afford the cost (about $400,000 per year) nor manpower spaces (17) to continue ACDB collection efforts."11 The Surgeon General did indicate that apart from cost considerations the system was judged to be a success.
In its report at the end of May 1987, the Work Group made a number of recommendations.12 After stressing that the recommendations were designed so as not to place additional reporting burdens on the personnel of the individual installations and that they should not be implemented until a fully automated support system is available, the report urged that the ambulatory care data set developed by the Work Group should be "incorporated in the Composite Health Care System (CHCS) as the ambulatory care reporting requirement." The "Work Group focused on the facility level requirements for data that enhance the delivery of quality healthcare." It noted, however, that the "data requirements of the facility level are of a different nature from the requirements of the higher levels of management."
The Work Group was asked to recommend an interim solution for system-wide data collection until the CHCS capability became available. It noted that a system now exists that "records patient encounters without a data collection burden on facility personnel. This system provides support to clinic administrative personnel. An interface with DEERS could provide demographic data that could be combined with encounter information. This capability would provide basic data on encounters by clinical area and patient demographics."
The availability of such information would provide management with information on the variation in patterns of utilization among the individual installations which could serve as a basis for further inquiry as to the reasons for the variation. Unusually high or low utilization patterns may indicate more efficient deployment of resources or more effective ways of providing care or the opposite. In any case, management would have a powerful but too infrequently used tool available based on already existing data collection procedures.
In view of the many recommendations over the years to develop ambulatory care information, the AFEB should vigorously support the Work Group`s recommendation that certain existing procedures for collecting encounter information "be proliferated (and) combined with a DEERS interface" to stablish an interim data collection system.
This interim data collection procedure would be in accord with the recommendations of the Remington report referred to above and [consistent]with a suggestion made by Dr. Densen to Norma St. Clair that the development
217
of administrative data not wait entirely upon the clinical information desired at the facility level.
Readiness-Related Issues. The ability of the Armed Forces to combat disease in the field has always been a matter of major concern to the medical staffs of the three Services. It was not until World War II that battle casualties exceeded losses from disease. The worldwide deployment of Armed Forces personnel, even in the absence of overt armed conflicts, makes the issue of continuing concern to the DOD.
In March of 1984 the ASD(HA), Dr. Mayer, requested the Board to examine the quantity and quality of the existing worldwide reporting systems for epidemiological data with particular attention to the information on the incidence and prevalence of disease. He also asked that the Board review the availability and quality of epidemiological data for various potential trouble spots in the world and recommend the preventive measures best suited to prepared the Armed Forces to deal with health problems in these areas.13
Dr. Woodward asked Dr. Densen to form an ad hoc subcommittee to prepare a reply to Dr. Mayer`s request. With considerable help from representatives of the three Services, a draft report was presented at the September 1984 meeting of the Board. Lively discussion ensued and a number of constructive suggestions were made. The final report was sent to Dr. Mayer in the following month.14
After pointing out that information on the health problems likely to be encountered by Armed Forces personnel outside CONUS was available from a number of sources, but that this information was not collated and disseminated to the field in the most useful fashion, the Board recommended that:
1. The disease reporting systems of the three Services be reviewed with the objective of providing relevant medical intelligence information to the Armed Forces Medical Intelligence Center (AFMIC).
2. A physician-epidemiologist be assigned to AFMIC who, among other duties, should rank the diseases present in order of military importance with concomitant preventive measures to deal with them.
3. The physician-epidemiologist should be a regular contributing participant at all Board meetings.
Following this report, a non-medical epidemiologist was added to the staff of AFMIC and he attended Board meetings. More recently an Air Force Colonel, who is a physician with training in epidemiology, has been assigned to AFMIC. He attended his first AFEB meeting in February of 1988 as the AFMIC representative.
At the September 1987 meeting of the Board, the AFMIC Executive Officer, Lt. Colonel John Weske, discussed the problems encountered in rank ordering the reportable diseases according to military importance. He reported that a meeting on the subject was planned within the next ninety days with the object of clearly delineating the goals of the effort and possible options and solutions, as well as a time table for achieving the goals. This topic is on the agenda for the Fall of 1988 AFEB meeting.
With regard to preparing Armed Forces personnel to deal with health problems in troubled areas, the Board stressed that unless information "reaches the field commander in a manner which clearly provides an assessment of risk and indication of action to be taken, its usefulness is limited. It is in this area of interpretation and translation into practical recommendations that the Armed Services appear to be somewhat deficient. To remedy this deficiency, the Board made recommendations designed to prepare medical personnel to maintain the readiness of troops under combat conditions and to facilitate large area surveillance in order to identify potential hazards as well as to aid in diagnoses. Among these were the following[recommendations]:
1. The combat casualty course be expanded to include aspects of preventive medicine and expansion of the Army Course in Tropical Medicine at Walter Reed to provide practical field and laboratory experience in tropical medicine.
2. A continuing medical education course be required for all military physicians. Physicians with appropriate preventive medicine training be assigned to units deployed to existing trouble spots.
3. In the preparatory phase for troop deployment provision should be made for field laboratories in the operational area early in the deployment schedule.
218
As of this writing, training in preventive medicine is conducted on a contingency basis as is related pre deployment planning. Operations plans are previewed for infectious diseases in accordance with guidelines developed in the Academy of Health Sciences Preventive Medicine Officer`s short course. Whether this includes provision for field laboratories is not known at this point.
Upon receiving the recommendations in these two reports, Dr. Mayer prepared amemorandum15 to the Assistant Secretaries of the Army, Navy and Air Force(M&RA and MRA&D) and to the Assistant to the Chairman, Joint Chiefs of Staff stating that he intended to implement the recommendations of the Board and soliciting comments. If the actions proposed by Dr. Mayer are indeed implemented a good start will have been made toward overcoming the deficiencies noted in the Board`s report. In any event, the Board should follow developments in this area closely.
Women in the Armed Forces. Dr. Mayer, in the memorandum of March 27, 1984, asked the Board to examine the constraints and likely consequences of the increasing participation of women in the Armed Forces.
It proved impossible to answer Dr. Mayer`s question directly because of the lack of high quality data on the health problems of women in the Armed Forces. This problem had been noted previously in another context by the Office of the Assistant Secretary of Defense (Manpower, Reserve Affairs and Logistics). In a review of women in the military published in October 1981,16 it was stated that "a complete understanding of the relative costs and productivities of military men and women is hampered by missing, outdated or inconsistent data." This conclusion was found to apply as well in the area of health affairs.
Given this lack of adequate and reliable data, the Board`s recommendations were directed at remedying this deficiency, so that in the future the nature and size of the health problems of women in the military would be more precisely understood and therefore more effectively addressed.
Particularly lacking were measures on childbirth and pregnancy-related conditions presented in such a form as to make possible comparisons with the civilian sector and to permit meaningful interpretation of trends. An eloquent presentation of the problem was made by a service obstetrician (Col. Sa`adah) at the Fall meeting of the Board. In its report the Board recommended that:
the statistical data on childbirth and pregnancy-related conditions be revised so as to be directly comparable to reports of the National Center for Health Statistics.
The data should present trends in annual birth rates, with and without complications of pregnancy, details as to pregnancy outcomes in terms of parity, trimester of pregnancy first seen, etc., in order to provide information on the health of both mother and child and lay a better foundation for the estimates of resource requirements.
The discussion at the Fall meeting of the Board emphasized the need for a much broader base of information about the health status and utilization patterns of women in the Armed Services than existed at the time. After again noting the absence of out-of-hospital utilization data and reiterating its prior recommendations to develop such data, the Board recommended that:
the Office of the ASD(HA) consider developing a prospective five-year cohort study of women, beginning when they are inducted, to determine their utilization of health services, [to] examine the relation[ship] between health status and occupation, and [to] evaluate the factors contributing to separation from the Armed Services.
This recommendation is in accord with the general recommendation of the Remington report that a longitudinal health record be established on military personnel and their dependents.
Following the transmission of these recommendations to Dr. Mayer`s office, Col. Redman of that office was asked to examine their feasibility. He concluded that "it is feasible to have the Services` maternal and natal statistics be collected, completed and reported in a manner comparable to current national and state guidelines" and recommended that the services be directed to "to incorporate all elements of birth certificate information not now collected through their medical records coding into the Individual Patient DataSystems.17
So far as can be determined at this writing, little or nothing has been done to develop the needed data though as Col. Redman noted, it is feasible to do so. This is a shameful state of affairs and the Board should exert its influence whenever and wherever it can to remedy the situation.
Col. Redman also reported the cohort study to be feasible and recommended that it be undertaken.18
219
In Retrospect
In carrying out its assignment as defined in the original charge to the Subcommittee on Health Maintenance, the Board has followed the basic epidemiological principle of endeavoring to define the population exposed to risk and relating events of interest to that population (relating the numerator to the denominator).
Considerable progress has been made by the Services in the understanding of this principle and its application to the health care program. The Board`s recommendations in this area have been considerably advanced by the revitalization of the Office of the Assistant Secretary of Defense, Health Affairs, under Dr. John Moxley, III, and his successor, Dr. William E. Mayer. Both of these individuals fully appreciate the principle and they have endeavored to make the Office the focal point for the "population-based health information system "envisioned in the Remington report. As noted in the foregoing, there is much yet to be done but the will to do it is there.
To insure continued programs, it would be desirable to improve communication between the Board and the Services in two respects:
1. The Board is most effective in helping to improve the health maintenance efforts of the Services when it is in a position to bring its expertise to bear in the "gleam in the eye" stage of a proposal. It is at this stage that epidemiological and statistical concepts are most efficiently woven into the design of a proposed project or program.
As early as possible the Board`s comments should be solicited when proposals are put forward to the ASD(HA) officer or to the respective Offices of the Surgeons General.
2. More systematic follow-up of the Board`s recommendations should be instituted. The Executive Secretary should be asked to determine what action has been taken on the recommendations and to report to the Board at periodic intervals.
Paul M. Densen
June 1988
Footnotes
1. Reorganization memorandum of 11/6/78.
2. Report of ad hoc Study Team for Review of Scope of PME in the Army. AFEB76-3, March 15, 1976.
3. Report of the Subcommittee on Health Maintenance of the AFEB, Feb16, 1979.
4. Recommendations on the Scope of the PME in the Armed Forces, DASG-AFEB79-3, 27 Mar 1979.
5. U.S. Dept. of Defense, Dept. of Health, Education & Welfare, Office of Management & Budget: Report on the Military Health Care Study, Washington, D.C. US GPO, Dec 1975.
6. Memo from Dr. Moxley to Executive Secretary AFEB regarding Review of Population-Based Forecasting Models, 5 Nov 80.
7. Memo to ASD(HA) and Surgeons General: Recommendation Regarding an Assessment of Population-Based Forecasting Models of the Office of Planning and Policy Analysis 26 Oct 1981 and Report to Board by PMO dated September 2, 1981.
8. Letter of 9/25/80 from Dr. Woodward to Dr. Griffin requesting that the latter serve as Chairman of the Task Force.
9. Memo to ASD(HA) and the Surgeons General, 21 April 1983, DASG-AFEB 83-3. Recommendations on Epidemiological Methods in the Military Health Care Delivery System.
10. Draft Report Diagnostic Data for Health Planning and Policy Development Health Studies Task Force OASD(HA) Burgess and Redman, June 1987.
11. Memo from General Becker to ASD(HA) re: Ambulatory Care Data Base, 1 May87.
12. Recommendations of the Ambulatory Care Data Requirements Work Group, 29 May 1987. Ms. Norma St. Clair (Chair).
13. Memo from Dr. Mayer to AFEB regarding Readiness Related Topics for AFEB examination.
14. Board memos to Dr. Mayer on Readiness: DASG-AFEB 85-1, 85-2,85-3, 29 October 1984.
15. Memo from Dr. Mayer to Assistant Secretary (M&RA) to Assistant to Chairman, Joint Chiefs of Staff, 14 May 1985.
16. Background Review-Women in the Military, Office Assistant Secretary of Defense. (Manpower, Reserve Affairs and Logistics, Chapter VII, p. 97, Oct 1981).
220
17. Feasibility of Upgrading the Services` Maternal and Natal Statistics Reporting Systems, Col. R. A. Redman, Health Studies Task Force OASD(HA) 10 May, 1985. (Vol III).
18. Feasibility of a Cohort Study on the Health Needs of Women in the Services, Col. Redman, Health Studies Task Force OASD(HA), 15 May 1985. (Vol III).
THE CONTINUING PROBLEM OF MALARIA
In their regular reviews to the Board on the incidence of specific illnesses among military personnel, the Preventive Medicine Officers of the three services regularly reported on the prevalence of malaria in troops deployed to tropical areas. On 16 May 1985, Colonel Manmohan V. Ranadive, Chief of Preventive Medicine in the Office of the Surgeon General of the Army, presented the following memorandum and questions to the AFEB:
MEMORANDUM FOR
EXECUTIVE SECRETARY, ARMED FORCES EPIDEMIOLOGICAL BOARD
SUBJECT: Chemoprophylaxis Against Chloroquine-Resistant Malaria: Question to the Armed Forces Epidemiological Board
BACKGROUND
1. In January, 1985, the U.S.P.H.S. recommended that travelers to Chloroquine-resistant P. falciparum (CRPF) regions in Asia or South America take Fansidar in addition to Chloroquine ONLY if they remained overnight in rural areas (reference 1). Travelers to east and central Africa were recommended to take Fansidar and Chloroquine due to the intense transmission of malaria.
2. Since Fansidar became available in the U. S. in 1982, 20 cases (six fatal) of severe adverse reactions including erythema multiforme, Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported; 19 of these cases were also taking Chloroquine weekly. In April 1985, U.S.P.H.S. revised their earlier recommendations (reference 2). For short-term travel (3 weeks or less) to CRPF-areas in Africa, only Chloroquine was recommended, and Fansidar was to be taken ONLY if a febrile illness consistent with malaria developed while on the trip. Long-term travel would require a careful assessment of the need for both medications prophylactically, taking into account the degree of exposure and the likelihood of contracting infection.
3. Malaria chemoprophylaxis was not routinely recommended for visitors to urban centers of Asia (to include China, Indonesia, Malaysia, the Philippines and Thailand), or for those who would have only daylight exposure to rural areas. Individuals having considerable outdoor exposure to rural areas of Thailand, where widespread resistance to both Chloroquine and Fansidar has been reported, would require special evaluation. Since [the] malaria risk in South America was primarily in rural areas and in specific urban areas only, routine prophylaxis was not recommended. Chloroquine prophylaxis was also recommended for travelers to the Indian subcontinent, Papua New Guinea, Irian, Java, the Solomon Islands, and Vanatu.
4. Due to the large numbers involved in a military deployment, reliability in taking medications at the appropriate time, and limited medical care in isolated areas, the U.S.P.H.S. guidelines are not necessarily applicable in the military setting.
QUESTIONS
1. In view of recent U.S.P.H.S. guidelines and the fact that military personnel on overseas deployments will often be at greater risk of contracting malaria than tourists, is Chloroquine and Fansidar prophylaxis in combination indicated for military members deployed in CFPF areas?
2. Since many CFPF areas are so highly endemic for vivax malaria, terminal Primaquine prophylaxis will also be indicated. What is the best prophylaxis schedule using the three drugs that will be associated with the least serious adverse effects?
3. What precautions or medical procedures should be followed to minimize the occurrence of serious adverse effects from prophylactic medications?
221
REFERENCES
1. Adverse reactions to Fansidar and updated recommendations for its use in prevention of malaria. MMWR 33(51): 713-714. 4 January 1985.
2. Revised recommendations for preventing malaria in travelers to areas with chloroquine-resistant Plasmodium falciparum. MMWR 34 (14):185-190, 195. 12 April 1985.
During the spring meeting of the AFEB on 6-7 June 1985 the Subcommittee on Infections and the Board discussed the malaria problem again and formulated the following recommendations:
MEMORANDUM FOR
THE ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS)
THE SURGEON GENERAL, DEPARTMENT OF THE ARMY
THE SURGEON GENERAL, DEPARTMENT OF THE NAVY
THE SURGEON GENERAL, DEPARTMENT OF THE AIR FORCE
SUBJECT: Interim Recommendations Concerning Chemoprophylaxis of Chloroquine Resistant Plasmodium falciparum (CRPF) Malaria
1. The Chief, Preventive Medicine, Directorate of Professional Services, Office of the Army Surgeon General, prepared the attached background information report and specific questions to the Armed Forces Epidemiological Board (AFEB) as a result of reported adverse reactions to Fansidar (MMWR 33 (51): 713-714, 4 January, 1985) and concomitant revision of the United States Public Health Service (USPHS) earlier recommendations (MMWR 34 (14):185-190, 195, 12 April 1985: Centers for Disease Control, DQ-CPS, Advisory Memorandum no. 80, 24 April 1985).
2. In answer to the first question, regarding whether or not Chloroquine and Fansidar in combination is indicated for military members deployed to CRPF areas, the AFEB recognizes the differences in intensity of military and civilian exposures and the multiple variables that might be associated with such possible military exposure. For these reasons, the Board believes it is inappropriate at this time to recommend a single course o faction that would be applicable to all possible deployment scenarios. Therefore, the Board would propose that decisions concerning malaria chemoprophylactic regimens for deployed individuals and groups be based on consideration off alciparum malaria endemicity, present knowledge regarding patterns of drug resistance of falciparum parasites in the regions, military mission, size of forces and medical support available to these forces. Therefore, within this general framework, the Board offers the following interim recommended guidance predicated mainly on the size of the forces:
a. For individuals and small groups of up to twelve personnel, (i.e., special military detachments), the Centers for Disease Control guidelines, as published in the Morbidity and Mortality Weekly Report, Vol. 34, No. 14, April 12, 1985, should be followed.
b. For sizeable deployments of more than twelve personnel (including units of battalion size or larger) to Chloroquine resistant Plasmodium falciparum (CRPF) areas, a development of a blanket policy applicable to the entire force should be made, predicated on all available information. Regimens that might be considered, depending on the respective circumstances, should include:
(1) Standard Chloroquine prophylaxis plus Fansidar and terminal Chloroquine and Primaquine.
(2) Standard Chloroquine prophylaxis plus Mefloquine and terminal Chloroquine and Primaquine.
3. With regards to the best prophylaxis schedule in CRPF areas which are highly endemic for vivax malaria, the Board makes the following observations:
Fansidar prophylaxis, in a regimen with Chloroquine and Primaquine, will be associated with hemolytic reactions in those persons with Glucose-6-PhosphateDehydrogenase (G6PD) enzyme deficiency. This risk,
222
however, must be viewed in the context that vivax malaria continues to be the most common form of malaria acquired by military personnel. The disease, although mild, relatively speaking, may remove the individual from duty for up to five to seven days. Thus, the expense of hospitalization of these individuals, coupled with the important risk that the disease potentially may not be recognized by civilian or military physicians, adds to the disease morbidity. Therefore, viewed in the context of benefit and associated risk, the Board recommends that:
a. Based on recognized epidemiological factors, Fansidar should be continued for one week after leaving the country. The combination of Chloroquine (300 mg) and Primaquine (45 mg) should be combined for a total of eight weeks, one tablet per week. b. Mefloquine appears to show great promise as a therapeutic and prophylactic agent in the treatment of malaria, particularly in CRPF areas. Additional valuable experimental data can be obtained by using it in combination with Chloroquine in regions where CRPF and Fansidar-resistance are present. Recommended experimental dosage should be 180 mg weekly, so as to obtain adequate perspective data. This drug should be highly prioritized in its approval and certification by the Food and Drug Administration (FDA). Further, the FDA needs to be made aware of its identification as an important alternative drug for civilian personnel presently receiving Fansidar.
4. With regards to precautions and medical procedures to be followed so as to minimize the occurrence of serious adverse effects from prophylactic antimalarial medications, the Board provides the following guidance and recommendations:
a. Adverse effects utilizing Fansidar prophylaxis can be minimized through dissemination of information to all medical personnel as to the significance of a generalized rash and the danger of continuing this drug if the rash is considered to be drug-induced. Commanders of all units under Fansidar prophylaxis should be advised as to the importance of having any members of their command exhibiting generalized rash seen by medical personnel.
b. Individuals receiving terminal Primaquine therapy should be advised as to the possible side effects of the medication (i.e., dark urine suggesting hemolysis) and the need to promptly seek medical attention. G6PD testing would be [highly] desirable so as to provide the opportunity to give necessary warning to those who are at highest risk of Primaquine-induced hemolysis.
c. Data collection concerning attack rates after termination of Chloroquine chemoprophylaxis and the severity of illness among those who develop the disease would be helpful in deciding whether Primaquine treatment is necessary. The United States Public Health Service could obtain this data from civilian travelers.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D., President, AFEB
Robert F. Nikolewski, Colonel, USAF, BSC, Executive Secretary
REFERENCES
1. Pearlman, E. J., et al.: Chemo suppressive field trials in Thailand. IV: The suppression of Plasmodium falciparum and Plasmodium vivax parasitemias by Mefloquine. (WR 142, 490, A 4-Quinoline Methanol). Am. J. Trop. Med. Hyg. 29: 1131-1137, 1980.
2. Dixon, K. E., Pitaktong, U., Phintuyothin, A.: Clinical trial of Mefloquine in the treatment of Plasmodium vivax malaria. Am. J. Trop. Med. Hyg. 34: 435-437, 1985.
3. World Health Organization. Advances in Malaria Chemotherapy. Tech. Rep. Ser. 1984: 711, WHO Geneva.
223
THE BOARD`S ROLE IN ASSISTING THE MILITARY
TO DEFINE ITS POLICY REGARDING
ACQUIRED IMMUNODEFICIENCY SYNDROME
AND EXPOSURE TO HUMAN T-LYMPHOTROPIC VIRUS TYPE III
During his tenure as Executive Secretary, Colonel Robert Nikolewski often reminded me that the Board needed an important new issue to enhance its image. The problems of acquired immunodeficiency syndrome (AIDS) and human T-lymphotropic virus type III (HTLV-III) filled that need. At the end of the Board`s 6 June 1985 meeting, when new business was discussed, Lt. Colonel John Herbold, USAF, then in the Office of Health Affairs, asked, out of the blue, "What does the Board have to recommend for the military regarding AIDS?" What a question! We thought that we had escaped any difficult or controversial problems to consider as action items at this meeting! I was the President of the Board at that time, and I advised Dr. Herbold that the Board did not respond to verbal requests, and that all such queries should be submitted in writing through the proper channels. That was on 6 June 1985. Never has the system witnessed such rapid transit of a set of provocative questions; they reached the AFEB office from the Office of Health Affairs on 10 June 1985-a record. The memorandum for the Board, dated 10 June 1985, from J. Jarrett Clinton, M.D., Deputy Assistant Secretary of Defense, follows:
SUBJECT: HTLV-III Antibody Positivity
As introduced at the June 6 meeting of the Subcommittee on Disease Control, request the Board address the issue of the public health significance of HTLV-III antibody positivity.
Specifically, what guidance can the Board provide regarding the appropriate implementation of public health surveillance and control measures? Given the spread of HTLV-III infection outside previously identified high-risk groups, what studies should the services conduct and what data should be gathered to better define the natural history of and potential military importance of this infectious agent in active-duty populations? Given the comprehensive health care system of the Armed Forces, a closed system, how might our concerns and approaches differ from those of the civilian sector?
Your considered deliberation of this critical issue is requested.
The AFEB has traditionally responded expeditiously when major health problems involve both the military and the public. Accordingly, a special meeting of the Board`s Subcommittee on Infectious Diseases was convened at WRAIR on 9 August 1985. The offices of Health Affairs and the respective Surgeons General were bombarded with comments and questions from all sources. These offices were soon spared the nuisance of so many inquiries when the word got out that the AFEB was to direct its attention to AIDS. Neither Colonel Nikolewskin or I nor our secretaries logged the number of calls, but they were numerous. Heads of various lay groups, gay rights groups, and the press called. The Board received demands for allocations of speaking times and placement on the agenda of the pending August meeting. The Board`s meetings are, by law, open sessions. I assured the head of the gay rights movement that he would receive agenda time; I asked him to limit his discussion to one-half hour, and to limit the number of persons who would attend the meeting with him because space was limited. We gave no specific answers to questions, and the calls were finally diverted to the proper public relations officer at the Department of Defense. There were many disruptions, but 9 August soon arrived.
224
I awakened with the chickens that morning, got an early start from Baltimore in order to beat the beltway traffic, and arrived at WRAIR at 0730, well ahead of the meeting. Outside the meeting room were two large and impressive military guards. Unaware as to why they were there, I had them relocated to another floor. I thought that those attending the meeting, particularly the press, might have adverse reactions to seeing armed guards. It was not clear in advance whether the meeting would be orderly and informative or disorderly and controversial, since the public, through the press, was polarized at this time. Soon Conference Room 3092 was packed-a record-with extra chairs and standing room only.
The agenda for that meeting follows, and the roster of Board member, military personnel, invited guests, and press representation is on page 225. (To my knowledge, this was the first time that the press had ever attended a meeting of the AFEB.)
|
AGENDA ARMED FORCES EPIDEMIOLOGICAL BOARD 9 August 1985 0900-0915 Welcome, Introduction of Members and Visiting Consultants 0915-1000 Military Medical Issues Regarding HTLV-III-LAV Disease 1000-1030 Presentation, National Gay Task Force 1030-1045 Department of Defense Blood Bank Program 1045-1145 Preventive Medicine Officers` Report
Comments 1145 Discussion
|
The meeting was orderly. Colonel Edmund Tramont reviewed the current knowledge regarding AIDS. Mr. Jeffrey Levi, Director of the National Gay Task Force, raised the human rights issues of confidentiality and ethical practices. I informed Mr. Levi that the AFEB comprised some of the most ethical and well-informed scientists, epidemiologists, and clinicians in this country, and that questions and recommendations would be directed toward protecting the individual. He was assured that the Board`s recommendations would be in the best interests of both the military and the public.
The meeting`s main purpose was fulfilled by providing important information on the effectiveness and limits of HTLV-III antibody testing and clarifications of problems relating to the protection of the
225
blood supply. Clinical descriptions of the disease syndrome, the means of classifying phases of the AIDS spectrum, the incidence of the disease, the known methods of spread of the virus, and the current and anticipated incidences were also elucidated.
Another principal function of the meeting was to allay the suspicion, misinformation, and incrimination which seemed to have polarized the public. The stage was set for the Board to gather its data, to crystallize its understanding of the problem, and to fulfill its mission at its fall meeting, planned for 11-13 September 1985. At this meeting, various other agenda items would be discussed, and the Board`s final recommendations regarding the AIDS problem would be formulated.
Roster of Participants
9 August
AFEB Members:
Theodore E. Woodward, M.D. Board President
William S. Jordan, Jr., M.D. Board Member
William R. Harlan, M.D. Board Member
Frank M. Townsend, M.D. Board Member
Samuel D. Thompson, Ph.D. Board Consultant
Robert F. Nikolewski, COL, USAF, BSC Executive Secretary
Robert A. Wells, COL, USA, MSC Executive Secretary (Designate)
Invited Consultants:
Abram S. Benenson, M.D. San Diego State University
Saul Krugman, M.D. New York University Medical Center
Also Attending:
Thomas M. Geer, GB, USA, MC Director, Professional Services, DASG
Philip K. Russell, BG, USA, MC Commander, Fitzsimmons Army Medical Center
Harold Jaffe, M.D. Centers for Disease Control AIDS Section, Epidemiology
and Treatment
Roger Dodd, M.D. American Red Cross Laboratory, Bethesda
Harry W. Haverkos, M.D. National Institutes of Health
Jim Hill, Ph.D. National Institutes of Health (representing Dr. Fauci)
Alfred J. Saah, M.D. National Institutes of Health
Manmohan Ranadive, COL, USA, MC Preventive Medicine Officer, USA
Ernest Takafuji, LTC(P),USA, MC Disease Control Consultant (DASG)
William B. Mahaffey, CAPT, MC, USN Preventive Medicine Officer, USN
Alfred K. Cheng, COL, USAF, MC Preventive Medicine Officer, USAF
Edmund C. Tramont, COL, USA, MC Chief of Microbiology, WRAIR
A. J. Polk, LTC, USA, MSC Department of Defense Blood Program
T. R. Cuthbert, COL, USA Office Secretary of Defense (MRA&L)
John R. Herbold, LTC, USAF, BSC Health Affairs
Michael Murphy, LTC,USA Public Relations, Department of Army
Dave Russell, MAJ, USA Public Relations Office, Chief of Public Affairs,
Department of the Army
Tansill Johnson Public Relations, DASG
Jeffrey Levi National Gay Task Force
Mathilde Krim National Gay Task Force
Reporters Representing the Following:
Army Times, The New York Times, Chronicle Broadcasting, Pentagram, The Washington Times, The Advocate, Washington Stripe, The Washington Post, U.S. Medicine, and The Washington Blade.
Prior to the September meeting, the Department of the Army, on 15 August 1985, and the Department of Defense`s Office of Health Affairs, on 9 September 1985, had presented specific memoranda and questions for the Board`s consideration. These questions provided a structure for the Board`s response,
226
particularly after the current knowledge of AIDS had been been clarified and discussed. These new memoranda, and the agenda and attendance roster for the 11-13 September meeting, follow:
MEMORANDUM FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
SUBJECT: Questions for the Armed Forces Epidemiological Board on HTLV-III Infections in the Military
1. At the recent meeting of the Armed Forces Epidemiological Board (AFEB) Subcommittee on Infectious Diseases held on 9 August 1985, the respective services were requested by Dr. Theodore Woodward, Chairman of the AFEB, to submit specific questions pertaining to HTLV-III infections and AIDS to the Board that could be addressed at its September meeting.
2. In response to that request, the following questions are provided:
a. Based on current level of understanding, what is the significance of a positive Western blot-confirmed antibody test for HTLV-III infection?
b. Are individuals who are antibody-positive at increased risk of having more severe reactions to live virus vaccines? What would their immunological response be to live and killed vaccines?
c. With the requirement to continue vaccinating military members against smallpox, is routine HTLV-III antibody screening of basic trainees (and other new entrants into the military) prior to receiving smallpox vaccine medically justified? Should prior screening be performed before administration of any other live virus vaccines?
d. Should the Army be involved in the collection of medical data and the conduct of epidemiological studies on HTLV-III infections?
3. Your assistance with these difficult questions is greatly appreciated.
FOR THE SURGEON GENERAL:
Ernest T. Takafuji, M.D., Lt. Colonel, MC
for:
Manmohan V. Ranadive, M.D.
Colonel, MC, Chief, Preventive Medicine Consultants Division
MEMORANDUM FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
SUBJECT: HTLV-III Antibody Positivity
In our June 10, 1985 memorandum to the Armed Forces Epidemiological Board, we requested advice on broad public health issues of HTLV-III antibody positivity in the military. Your specific attention to the following questions in the context of the original request will assist this office in the development of policy guidelines:
1. Should personnel on active duty be screened for HTLV-III antibody?
2. What steps should be taken with respect to active duty personnel who screen confirmed positive for HTLV-III antibody?
3. Should confirmed HTLV-III antibody positive individuals, identified through screening of potential active duty accessions, be permitted to join th e military services?
4. What public health risk does a confirmed HTLV-III antibody positive individual pose in the military operational setting?
5. What public health risk does a confirmed HTLV-III antibody positive individual pose in the military community setting?
J. Jarrett Clinton, M.D.
Deputy Assistant Secretary [of Defense] (Professional Affairs & Quality Assurance)
227
|
AGENDA ARMED FORCES EPIDEMIOLOGICAL BOARD Wednesday, 11 September 1985 1300-1700 Select Immunodeficiency Diseases Thursday, 12 September 1985 0830-0845 Armed Forces Medical Intelligence Center Current Update 0845-1200 Select Immunodeficiency Diseases (Continued) 1300-1345 Germ Cell Tumors of the Testicle Among Aircraft Repairmen 1345-1400 Questions 1400-1445 Review of the U. S. Army Ambulatory Care Data Base 1445-1500 Questions 1500-1600 Preventive Medicine Officer Reports Friday, 13 September 1985 0800-1100 Overview and Summary |
228
Roster of Participants
12 September
AFEB Members:
Paul M. Densen, D.Sc.
Carol J. Johns, M.D.
William S. Jordan, Jr., M.D.
Richard Hornick, M.D.
Samuel Thompson, Ph.D.
Saul Krugman, M.D.
Theodore E. Woodward, M.D.
Abram S. Benenson, M.D.
AFEB Staff.
Lt. Col. Robert A. Wells, Ph.D., MSC, USA
Col. Robert F. Nikolewski, BSC, USAF
Jean P. Ward, DAC
Military Preventive Medicine Officers and DoD Staff:
Col. Alfred K. Cheng, MC, USAF
Col. Robert G. Self, MC, USAF
Lt. Col. John Herbold, BSC, USAF
Capt. William B. Mahaffey, MC, USN
Col. Manmohan Ranadive, MC, USA
Capt. Vernon D. Schinshi, MSC, USN
Cdr. John R. Stockwell, USPHS
Attendees:
Lt. Col. Fred A. Cecere, MC, USA
Col. Richard N. Miller, MC, USA
Lt. Col. Terry R. Misener, ANC, USA
Capt. Kenneth F. Wagner, MC, USN
Lt. Col. George E. Crawford, MC, USAF
Col. William H. Bancroft, MC, USA
Lt. Col. Ernest Takafuji, MC, USA
Col. Thomas E. Bowen, MC, USA
Lt. Cdr. Alan M. Ducatman, MC, USN
Lt. Col. Donald Burk
Capt. John McNeil, MC, USA
Capt. Mark S. Davis, MC, USN
Maj. John F. Brundage, MC, USA
Maj. Benedict M. Diniega, MC, USA
Capt. Jeffrey. D. Gunzenhauser, MC, USN
Maj. Robert R. Redfield; MC, USA
Col. William H. Wolfe, MC, USAF
Lt. Col. James W. Kirkpatrick, MC, USA
Capt. Douglas M. Stetson, MC, USMC
Col. Edmund C. Tramont, MC, USA
James R. Allen, M.D.
13 September
AFEB Members:
Theodore E. Woodward, M.D.
Frank Townsend, M.D.
Abram S. Benenson, M.D.
Samuel Thompson, Ph.D.
Richard Hornick, M.D.
William S. Jordan, Jr., M.D.
Carol J. Johns, M.D.
Leonard Kurland, M.D.
William R. Harlan, M.D.
Senior DoD Staff and Representative of the Surgeon General:
William Mayer, M.D.
Jarrett Clinton, M.D.
Maj. Gen. Monte B. Miller, MC, USAF
AFEB Staff:
Lt. Col. Robert A. Wells, MSC, USA
Col. Robert Nikolewski, BSC, USAF
Jean P. Ward, DAC
Military Preventive Medicine Officers and DoD Staff:
Col. Alfred K. Cheng, MC, USAF
Col. Manmohan Ranadive, MC, USA
Capt. William Mahaffee, MC, USN
Lt. Col. John R. Herbold, BSC, USAF
Col. Robert G. Self, MC, USAF
Cdr. John R. Stockwell, USPHS
Attendees:
Cdr. Mark L. Dembert, MC, USN
Lt. Cdr. Alan M. Ducatman, MC, USNR
Cdr. Mark S. Davis, MC, USN
Lt. Col. James W. Kirkpatrick, MC, USA
Lt. Col. Terry R. Misener, ANC, USA
Lt. Col. Fred A. Cecere, MC, USA
James R. Allen, M.D.
Lt. Col. George Crawford, UC, USAF
Col. William H. Wolfe, MC, USAF
The Board Formulates Its Resolutions on AIDS
Further discussions were held during evening sessions. Specific answers and recommendations to the questions relating to AIDS were formulated. On the morning of 13 September, Dr. William E. Mayer, Assistant Secretary of Defense for Health Affairs, and his Deputy, Dr. J. Jarrett Clinton, arrived at Parson`s Island by helicopter. I presented the Board`s answers to their specific questions and our recommendations to Dr. Mayer. He commented, after expressing his thanks, "We can live with that." The final report was presented to the Office of Health Affairs and the respective Surgeons General on 17 September 1985, and follows:
229
MEMORANDUM FOR
THE ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS)
THE SURGEON GENERAL, DEPARTMENT OF THE ARMY
THE SURGEON GENERAL, DEPARTMENT OF THE NAVY
THE SURGEON GENERAL, DEPARTMENT OF THE AIR FORCE
SUBJECT: Human T-Lymphotrophic Virus Type III (HTLV-III)Antibody Positivity
1. At the request of the Assistant Secretary of Defense, Health Affairs, the Armed Forces Epidemiological Board (AFEB)members, consultants and respective military medical service representatives met11 through 13 September 1985 to consider a set of questions on the above subject(Enclosures 1 and 2).
2. The AFEB traditionally has conceived its mission to be that of rendering advice to the end of ensuring the maintenance of a healthy, effective military service which is ready at all times for rapid deployment. It believes that HTLV-III infections should be addressed in the military services as any other infectious or contagious disease. In this regard it is noteworthy that its similarities to hepatitis B are striking in many respects. The primary objective of the Board must be to protect the health of the individual and simultaneously to prevent the spread of infection to other personnel within the Armed Forces.
3. The Board makes its recommendations relevant to HTLV-III antibody positivity in the light of its evaluation of the current state of knowledge of this complex disease. The Board is well aware of the present threat and of the potential for greater threat based on the comprehensive assessment of several factors to include: (a) the risks to the infected individual incident to military service, (b) the risk of transmission of illness to non-infected personnel, (c) the impact of infected individuals on the function of their unit, and (d) the safety of the blood supply.
4. The recommendations of the Board may be subject to change at such time as the natural history of HTLV-III infection becomes more clear. Under these conditions, pertinent and longitudinal studies would be appropriate. Under ideal circumstances the screening of all active duty military personnel for HTLV-III antibody and hepatitis B antigen could be advisable. However, such screening is unnecessary based on information currently available relative to the threat of illness to others or the limitations of personnel to perform their duties. Moreover, the prospect of screening all active military members for HTLV-III antibody at this time is not envisioned as feasible-not only because of the logistical and economical requirements, but especially because of the limited availability of trained personnel and medical resources. The qualifying criterion is simply that it is unknown whether an individual with HTLV-III will progress to active illness. Future studies of the natural history of the syndrome should help clarify this important matter.
5. Based on a thorough review of available information and subsequent discussion, the Board makes the following recommendations:
a. All active duty personnel pending reassignment to overseas permanent duty stations should be screened for the presence of HTLV-III antibody. If these individuals are found to be positive by ELISA and by an appropriate confirmatory test, the service member should be medically evaluated to determine the status of his or her infection
This is appropriate to allow identification of those at high risk for progression of infection and at high risk from exotic diseases before an extended overseas tour.
b. Individuals who are antibody positive but manifest no evidence of progressive clinical illness or immunological deficiency may be considered for worldwide duty. All antibody positive persons should receive a comprehensive and immunological evaluation at least annually. They should be counseled on risks of transmission and be designated as blood-donor ineligible. Military personnel with progressive clinical illness or immunological compromise should be referred to a medical evaluation board for a determination of fitness for worldwide duty.
c. New candidates for active duty identified as HTLV-III antibody positive (two ELISA and confirmatory tests) at the time of induction will be rejected from military service. The candidate will be advised to consult his or her personal physician.
230
This judgment is based on the possibility that such antibody positive persons may have an increased potential to develop the Acquired Immune Deficiency Syndrome-particularly when they are given required live biologic vaccines, when they are exposed to or are infected with agents such as the Plasmodium of malaria or are subjected to other biological or physical stresses. It is conceivable that future testing and medical evaluation may show that individuals with positive antibody alone may be healthy and therefore should not be ultimately precluded from consideration for military service.
6. Current evidence indicates that HTLV-III is transmitted to others by blood transfusion from an infected person by the injection of infected blood products or by intimate contact with an infected person. The risk of transmission of HTLV-III is not completely understood and requires further evaluation. However, day-to-day association with infected persons by close household contacts does not pose a threat to the uninfected individuals. There are hundreds of instances where adults or children living with persons with AIDS or positive for HTLV-III antibody have themselves failed to become infected or antibody positive. The same situation has been observed regarding medical contacts with known patients. Moreover, health professionals who have experienced needle puncture with needles contaminated with materials from AIDS patients have very rarely developed illness or serologic evidence of infection. Specifically, only one such case has been reported at present. The Board, therefore, makes the following recommendation relative to military operational settings:
Environmental contacts in military operational settings such as tanks, submarines, and aircraft are not regarded as significant risks for infection by HTLV-III. In accordance with United States Public Health Service recommendations, personnel who are HBG a and/ or HTLV-III antibody positive should be designated as unsuitable as blood donors.
7. Although generally there is no perceptible risk of transmission by non-sexual person-to-person contact, there are other concerns which are relevant within the military/community setting. The following recommendations by the Board are intended to address these issues:
a. Service planning on contingency blood samples should take the potential for HTLV-III infection into account. The periodic screening of all military personnel is not recommended due to excessive screening costs weighed against low risk and the inability to ensure the absence of infectivity by random testing. However, the Board recommends that donated blood be screened to detect HTLV-III antibody and Hepatitis-B antigen wherever a significant number of blood units are to be processed.
b. Although personnel pending overseas assignment are recommended for the highest screening priority, those currently serving at an overseas duty station may also be candidates for screening. Such screening should be accomplished in a prioritized fashion, with the highest priority to those assigned at locations with a high risk of endemic disease or with minimal medical capability.
c. The Board recommends that additional education be provided on techniques to minimize the transmission of this infection in order to reduce unfounded fears regarding the etiology and epidemiology of the disease.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert A. Wells, Ph.D.
Lt. Colonel (P), USA, MSC
Executive Secretary
231
The Secretary of Defense Establishes Policy
Acting without delay, Secretary of Defense Caspar W. Weinberger transmitted the following memorandum and policy procedures, dated 24 October 1985:
MEMORANDUM FOR
SECRETARIES OF THE MILITARY DEPARTMENTS
CHAIRMAN, JOINT CHIEFS OF STAFF
ASSISTANT SECRETARY OF DEFENSE (FM&P)
ASSISTANT SECRETARY OF DEFENSE (RA)
ASSISTANT SECRETARY OF DEFENSE (PA)
ASSISTANT SECRETARY OF DEFENSE (HA)
ASSISTANT SECRETARY OF DEFENSE (LA)
GENERAL COUNSEL
SUBJECT: Policy on Identification, Surveillance, and Disposition of Military Personnel Infected with Human T-Lymphotropic Virus Type III (HTLV-III)
The following policy is established relative to infection of military members with Human T-Lymphotropic Virus Type III (HTLV-III).This initial policy is intended to reflect current knowledge regarding the natural history of this disease, the risks to the infected individual incident to military service, the risk of transmission of disease to noninfected personnel, the effect of infected individuals on the function of the unit, and the safety of the blood supply. These policies are adopted as interim guidance which shall be reviewed within one year. This review shall assess developments in the medical management of HTLV-III infections, information obtained through longitudinal epidemiologic studies of the natural history of HTLV-III infection, and the effects of this interim guidance on force management. Appropriate changes to DOD directives shall be promulgated within 30 days of the conclusion of this review.
A. Accession
Applicants for enlisted service shall be screened for exposure to HTLV-III at the Military Entrance Processing Station or the initial points of entry to military service. Candidates for officer service shall be screened for exposure to HTLV-III during their pre-appointment of pre-contracting physical examinations. Individuals confirmed as HTLV-III antibody positive (Food and Drug Administration-approved enzyme immunoassay (EIA)serologic test and, if positive, a positive immunoelectrophoresis test (Western blot) are not eligible for military service. The rationale for this policy is[that:]
. the condition existed prior to service,
. the Department avoids potential medical costs and the possibility that the individual shall not complete his or her service commitment,
. clinical evidence indicates that pre-AIDS patients may suffer adverse and potentially life-threatening reactions to some live virus immunizations administered at basic training,
. an antibody positive individual is not able to participate in battlefield blood donor activities or other blood donation programs, and
. presently, there is no way to differentiate between antibody positive individuals who will progress to clinical disease and antibody positive individuals who will remain healthy.
B. Disease Surveillance
1. Active duty and reserve component military personnel shall be screened for the presence of HTLV-III antibody. Generally, implementation should be in the following priority order:
. individuals serving in, or subject to deployment on short notice to areas of the world with a high risk of endemic disease or with minimal existing medical capability,
232
. individuals serving in, or pending assignment to, all other overseas permanent duty stations,
. individuals serving in units subject to deployment overseas,
. other individuals or units deemed appropriate by the respective military department such as medical personnel involved in the care of HTLV-III infectious patients, all remaining individuals in conjunction with routinely scheduled periodic physical examinations.
2. Individuals who are confirmed to be antibody positive shall be medically evaluated to determine the status of their infection and the potential adverse consequences to the individual of serving in a particular geographic region. The Assistant Secretary (Health Affairs) shall convene a Tri-Service medical working group to develop a standardized clinical protocol to ensure consistent evaluation and staging of each patient at all military medical treatment facilities.
3. The medical assessment of each exposure to and/or case of HTLV-III infection shall include an epidemiological assessment of the potential transmission of HTLV-III to close personal contacts and family of the patient. This information is vital to provide appropriate preventive medicine counseling and to the continued development of scientifically based information regarding the natural history and transmission pattern of HTLV-III. Therefore, the occurrence of HTLV-III infection shall not be used as a basis for punitive action against an individual.
4. Each military medical service shall conduct ongoing clinical evaluations of each antibody positive individual`s health status at least annually, provide appropriate preventive medicine counseling to individual patients, provide public health education materials to the beneficiary population, conduct longitudinal [studies], and prepare internal reports to facilitate timely review and reassessment of current policy guidelines.
C. Retention
1. Individuals who are antibody positive but manifest no evidence of progressive clinical illness or immunological deficiency([based on] physical and laboratory assessment, demonstration of ability to respond to immunizations, and ability to mount a protective immune response to immunizations or exposure to naturally occurring pathogens) shall be retained. The Service Secretaries, in order to protect the health and safety of infected individuals and of other military persons, may limit assignment of such individuals with respect to the nature and location of the duties performed in accordance with operational requirements.
2. All antibody positive persons shall receive a comprehensive clinical and immunological evaluation at least annually. Each individual shall be counseled on the risks of disease transmission, methods of prevention, and informed that they are ineligible to donate blood.
D. Separation
1. Individuals who are infected with HTLV-III and demonstrate progressive clinical illness shall be referred for medical evaluation for a determination of fitness for continued service in accordance with Title 10 United States Code Section 1201, et seq.
2. Individuals who are infected with HTLV-III and are found not to have complied with preventive medicine counseling for individual patients may be separated for the convenience of the Government.
3. Separation for the convenience of the Government or for misconduct based upon evidence other than HTLV-III infection is unaffected by this policy memorandum.
E. Safety of the Blood Supply
DOD Military Blood Program Office policies and Food and Drug Administration guidelines shall be followed by the Military Departments` Blood Programs and by civilian blood agencies collecting blood on military installations. In the event that units of blood shall not be screened for infectious agents prior to transfusion (contingency or battlefield situations),the DOD Military Blood Program Office in coordination with the Military Departments shall provide guidance to operational units to ensure that potential donors have been screened.
F. Limitations on the Use of Information
1. Results obtained from laboratory tests for HTLV-III performed under this memorandum and information concerning personal drug use or consensual sexual activity disclosed by a Service member as part of an epidemiological assessment under this memorandum may not be used against the Service member in actions under the Uniform Code of Military Justice, in a Line of Duty determination, or on the issue of characterization in separation
233
proceedings. Such information may not be used as the basis for separation of the service member except for (a) separation based upon physical disability, or (b) separation for the convenience of the Government after a hearing before a board of officers and approval by the Secretary or an Assistant Secretary of the Service concerned.
2. The limitations in paragraph F.1. do not apply to:
(a) The introduction of evidence for impeachment or rebuttal purposes in any proceeding in which the evidence of drug abuse or relevant sexual activity (or lack thereof) has been first introduced by the Servicemember; (b) Disciplinary or other action based on independently derived evidence.
Caspar W. Weinberger
The Secretary of Defense
Enclosure (References)
References
(a) Armed Forces Epidemiological Board Memorandum, 17 September 1985, Human T-Lymphotropic Virus type III (HTLV-III)Antibody Positivity.
(b) Deputy Secretary of Defense Memorandum, 30 August 1985,HTLV-III Testing.
(c) Assistant Secretary of Defense (Health Affairs)Memorandum, 14 August 1985, Standardization of Reporting Requirements for Blood Collection Agencies on Military Installations.
(d) Assistant Secretary of Defense (Health Affairs)Memorandum, 17 July 1985, Military Implementation of Public Health Service Provisional [sic].
(e) DoD Military Blood Program Office Memorandum, 13 March1985, Military Implementation of Public Health Service Provisional Recommendations.
(f) Department of Defense Directive 6200.1, April 27 1973,Policy Concerning the Venereal Disease Control Program of the Armed Forces.
(g) Department of Defense Directive 1332.18, September 9,1968, Separation from the Military Service by Reason of Physical Disability.
(h) Title 10 United States Code Section 1201, etseq.
Despite the difficult logistical adjustments, the three military services persevered, collaborated, and applied their personnel and resources to effect the Board`s recommendations. The Assistant Secretary of Defense for Health Affairs expressed his appreciation to the Board in the following letter, dated 5 December 1985:
Dear Dr. Woodward:
I wish to commend and thank the Board for its assistance in addressing issues of critical importance regarding the emergence of Human T-lymphotropic Virus Type III infections among military personnel. To assist the Department of Defense in maintaining a current and balanced approach on this issue, I request that the AFEB establish a standing committee on HTLV-III infection that would evaluate and comment on current DOD initiatives and programs from the perspective of prevention, epidemiologic assessment, and risk management. Your continued support and valuable insight are greatly appreciated. I look forward to meeting personally with you and whomever you appoint to discuss the details of the AFEB`s continuing work on this disease.
Sincerely yours,
William Mayer, M.D.
The AFEB Responds to Requests from the Department of Defense
In keeping with Dr. Mayer`s request, a standing AFEB Subcommittee on HTLV-III Infections was appointed, with the following membership: Abram S. Beneson, Chairman, and William S. Jordan, Jr., Frank M. Townsend, and me. Later, Walter H. Dowdle, Richard B. Hornick, and Llewellyn J. Legters also
234
{kind=link}
Dr. Mayer, a psychiatrist, became the Pentagons top medical advisor in December 1983, when he was appointed Assistant Secretary of Defense for Health Affairs. He served in both the Army and the Navy Medical Corps and, following the Korean War, he conducted a special study for the Army on prisoners of war. He served as Director of the California State Department of Health while Ronald Reagan was Governor, and was head of the Alcohol, Drug Abuse, and Mental Health Administration in the Department of Health and Human Services while he was also on active duty in the Public Health Service Commissioned Corps.
Dr. Mayer and his very able Deputy, Dr. Jarrett Clinton, soon made it clear that they wished to work with the Armed Forces Epidemiological Board and the respective military services. Problems of great importance that intimately involved the Board came under intense discussion during their administration, some of which were: acquired immune deficiency syndrome; asbestosis; agent orange; cardiovascular screening for military personnel age 40 and older; safety considerations of the M2 Bradley Fighting Vehicle; military health standards; and population-based epidemiological forecasting.
235
joined. On September 25, 1986, J. Jarrett Clinton, M.D., Deputy Assistant Secretary of Defense, addressed the following letter of request to the AFEB:
Dear Dr. Woodward:
The Department of Defense has initiated a policy review of our current HTLV-III program guidance. As you recall, our initial guidance was promulgated after recommendations were provided by the AFEB. The assistance of the AFEB throughout this past year has been instrumental in our ability to maintain a steady course in addressing the myriad problems associated with this disease in a scientific and medically sound manner.
It would be most helpful if the AFEB would address the following questions at your October meeting:
(a) What is the significance of a p24 band alone? Should DoD maintain a dichotomized, positive/ negative standard or should laboratory results be reported as positive, negative, or indeterminate? Should laboratory results report the band patterns and explanation of results to the attending physician?
(b) Is periodic testing of the total force medically indicated? If so, how frequently? Does the current DoD recommended order of priority for cohort screening of military personnel for HTLV-III infection maximize the dual objectives of protecting individual health and minimizing transfusion associated transmission in contingencies? Could the total force screening effort currently being undertaken by the Military Services be effectively integrated into existing procedures such as pre-enlistment physical examinations, medical qualification for overseas assignment or assignment to rapid deployment units, and in conjunction with scheduled periodic physical examinations?
(c) For which high risk patient populations, if any, should military medical facilities offer or require HTLV-III screening (for example STD clinics, prenatal clinics, surgical or all hospital inpatients)?
(d) Given the rationale for HTLV-III screening of military personnel, should we require population-based screening of DoD civilian employees, either within the United States or overseas?
(e) What restrictions, if any, should be placed on health care workers who are HTLV-III antibody positive? If an HTLV-III infected health care worker continues to work, does the patient have a right to know about the health care worker`s status, even if the risk of transmission is negligible?
We appreciate your attention to these difficult issues.
Additionally, any guidance regarding other aspects of this disease that you deem appropriate would be most welcome. I am looking forward to joining you at the meeting.
Sincerely,
J. Jarrett Clinton, M.D.
Deputy Assistant Secretary
(Professional Affairs & Quality Assurance)
cc: Surgeons General
Executive Secretary, AFEB
The Subcommittee on AIDS and the Board discussed the sequestions at its fall 1986 meeting, and transmitted the following recommendations on Human Immunodeficiency Virus (HIV) infections-note that the policy on the name of the virus has been changed to HIV from HTLV-III-to DoD`s Office of Health Affairs on 10 November 1986:
SUBJECT: Recommendations on Human Immunodeficiency Virus (HIV)Infection
1. At the request of the Assistant Secretary of Defense, Health Affairs, the Armed Forces Epidemiological Board (AFEB),military medical service representatives and appropriate members of the civilian medical community met 16-17 October 1986 to consider a set of questions on the above subject (Enclosure 1).
236
{kind=link}
Walter Dowdle received his B.S. degree from the University of Alabama in 1955, his M.S. degree from Alabama in 1957, and his doctorate in Microbiology from the University of Maryland in 1960. Most of Dr. Dowdle`s experience has been at the Center for Disease Control in Atlanta, where he has served as Director of the Center for Infectious Diseases. He has published broadly in the field of infectious diseases on pneumonia, herpetic infections, influenza, and HIV infections.
Dr. Dowdle joined the AFEB in 1986, bringing his considerable epidemiological experience to help unravel the complicated relationship between HIV infection and its impact on health care in the military.
237
{kind=link}
Lew Legters graduated from the State University of New York at Buffalo School of Medicine, and served as a house officer in general medicine before he joined the Army Medical Department, where he developed his capabilities in epidemiology and preventive medicine. He maintained close contact with the AFEB during his tenure as the Army`s Chief of Preventive Medicine from 1975 to 1977. During his service years, Lew was always well-informed on the incidence of diseases, and could easily separate out matters of consequence. His reports to the Board were always concise and informative.
Lew became Chairman of the Department of Preventive Medicine at the Uniformed Services University of the Health Sciences School of Medicine, where he developed an effective epidemiological unit that applies its expert services in geographic sites of medical and military importance. Lew has served the Board as an actively participating member; his advice greatly assists the Subcommittee on Infectious Diseases. He is one of the few career officers who has maintained a close association with the Board after his retirement from the service.
238
{kind=link}
After he trained at The Johns Hopkins School of Medicine, Dick Hornick worked as a medical officer in infectious diseases at USAMRIID. Then, for two decades, he conducted innovative research on the development and application of viral, rickettsial, and bacterial vaccines at the University of Maryland School of Medicine. He helped develop the strong Division of Infectious Diseases there, which he directed until 1979, when he was named Chairman of the Department of Medicine at the University of Rochester School of Medicine.
Dick served as a member of the AFEB`s Commissions on Epidemiological Survey and Enteric Diseases. Later he was appointed to the Board, where he provided support for the Subcommittee on Infectious Diseases. Dick`s contributions to our knowledge of typhoid fever, other enteric infections, tularemia, and rickettsial diseases, and in particular to their control by vaccines and the development of a better understanding of their pathogenesis, have benefited our whole society.
239
2. a. With regard to the question of the significance of a solitary p24 band of the bands in the Western blot test which are characteristic of AIDS infection, and the preferred contents of the laboratory report, the Board recognized that Western blot preparations vary insensitivity and may produce false positive reactions. A solitary p24 band in a Western blot test cannot be regarded as definitive. While it may indicate an early stage of infection with HIV, it may be a false positive reaction; i.e. a true negative. Thus the Board recommends that:
A solitary p24 band should be regarded as neither positive nor negative, but as an intermediate result requiring further testing of the serum sample by more definitive procedures such as testing by the solid phase ELISA with recombinant antigen or by the radio-immunoprecipitation assay. This testing should permit a report of a positive or negative test for antibodies against HIV; rarely the testing might result in indeterminate findings requiring a new serum specimen for repeating testing.
b. To answer the question whether periodic screening of the total force is medically indicated, the Board considered the issues involved in the problem of AIDS among military personnel. The current program of mass screening will identify those in the Armed Forces who are presently infected with the human immunodeficiency virus (HIV); the exclusion of recruits who are serologically positive assures that no infected individuals are added to the active duty pool. The periodic medical evaluation of those active duty personnel who were found to be seropositive will assure that the military population is fully fit for duty insofar as AIDS is concerned, except that these individuals, and the much larger number of carriers of the hepatitis B virus, must be appropriately identified by "dogtag" or other device as disqualified from serving as blood donors.
Repeating total force screening would detect those active duty personnel who have developed new infections, and would provide important epidemiological information. The latter can be more economically obtained by testing appropriate numbers of active duty personnel selected randomly from various segments, geographic and otherwise. Findings of the current screening may suggest groups of epidemiological importance.
For detection of new cases, screening would best be integrated into existing medical encounters such as medical qualification for overseas assignment, assignment to rapid deployment units, and periodic physical examinations. The transmission of AIDS is very similar to that of syphilis; it is primarily transmitted sexually and also by exchange of blood (by needles shared among intravenous drug users and, before the tests became available, by blood transfusion); control of AIDS would be best effected by using the methods successful in controlling syphilis. These methods were based on identifying infected individuals and tracing the contacts from whom they may have acquired or to whom they may have transmitted their infections, and appropriately managing all who proved to be infected.
While there is now no proven effective drug for treatment of AIDS, the epidemic can be controlled by preventing further spread. This involves counseling the seropositive individuals on the techniques and need for the practice of "safe sex." For those who were involved in intravenous drug abuse, drug rehabilitation and impressing on the infected drug addict the danger he poses to others if he persists in his drug habits and shares syringes and needles with others.
The Board recommends that:
Following completion of the present total force screening, further HIV detection should be applied on a selective basis. Subsequent HIV screening for the military forces should be integrated into existing procedures such as pre-enlistment examinations, medical qualification for assignment overseas or to rapid deployment units, and in conjunction with scheduled periodic examinations. Major military medical facilities should acquire the expertise to carry out the serologic tests for screening for infection. Quality control measures must be reinforced to insure the validity of results.
c. With respect to the question to which high risk patient populations should HIV screening be required or offered, it is to be noted that the four-year interval between periodic physical examinations of those in the 20-30 age group, among whom the prevalence of sero positivity has been found to be highest, is too long a period to adequately protect the health of the individual or the safety of emergency-required blood for transfusion. This interval can be shortened by serological screening for HIV when the individual is admitted to a hospital or receives other medical care, with consideration of how recently the last serological screening had been performed. Because
240
they fall into high risk groups, testing should be required on those who attend drug rehabilitation or STD clinics because of the likelihood that infection with HIV may have occurred concurrently; testing should be repeated 2-3 months later if a negative test is reported since serological positivity may not have developed yet. Because of the threat to the newborn child, and because infected service members may be found among the contacts of a seropositive woman, screening is advisable for those attending prenatal clinics. Serological testing should be performed in the laboratories of major medical facilities; the technology for HIV testing is much simpler than the Wassermann test which is routinely performed in larger hospitals and regional laboratories. To assure a high level of performance, quality assurance testing will be required.
The Board therefore recommends that:
HIV testing should be a requirement for all military personnel admitted to a military hospital unless a test has recently been performed. It should be required of all personnel admitted to clinics for sexually transmitted diseases (STD) and drug rehabilitation; tests should be repeated in two to three months if negative on first testing. HIV screening is advisable for patients in prenatal clinics. Major medical facilities should acquire the expertise to carry out the appropriate serological tests; quality control measures must be enforced to insure the validity of results.
d. Regarding the question on the screening of DOD civilian employees either within CONUS or overseas, the Board considered the indications for screening civilian employees of the Armed Forces. Within CONUS,DOD has no medical responsibility for civilian employees; however, overseas the sick civilian becomes the responsibility of the military medical system. A seropositive individual going overseas might be assigned to duty in an isolated area with poor access to medical care; should clinical manifestations of AIDS such as pneumonia develop, the welfare of the individual would be jeopardized. From the point of view of the service, the seropositive civilian employee has an increased likelihood of becoming a burden to the medical system, and the probability of completing the contracted tour of duty is reduced. Therefore, the Board recommends that:
Testing for HIV should be included in any medical clearance procedures now in use prior to assignment of civilian personnel overseas.
e. With reference to the question on restrictions on HIV-infected health care workers, the Board recommends that:
HIV-positive health care workers who are otherwise healthy may continue to provide health care, conducting themselves in accordance with the guidelines published by the U.S. Public Health Service in Morbidity and Mortality Weekly Report, Vol. 35, No. 14, dated 11 April 1986, "Recommendations for Preventing Transmission of Infection with HTLV-III/LAV during Invasive Procedures." (Enclosure)
3. The Board commends the services for developing a working staging system for AIDS. The Board also suggests that the methods of reporting data related to AIDS prevalence and incidence be presented in a standard format and that specific rates be stated to permit inter service comparisons.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President
Robert A. Wells, Ph.D.
Colonel, USA, MSC
Executive Secretary
241
The Neuropsychiatric and Secondary-Infection Aspects of AIDS
During each of its meetings, the Subcommittee on Infections and the Board always discussed some aspect of the HIV infection problem. On 5February 1988, John F. Mazzuchi, Ph.D., who succeeded Dr. Clinton as Acting Deputy, Assistant Secretary of Defense for Health Affairs, presented the following memorandum to the AFEB for its consideration:
MEMORANDUM FOR ARMED FORCES EPIDEMIOLOGICAL BOARD
SUBJECT: Human Immunodeficiency Virus (HIV) and Implications for Military Service
Human Immunodeficiency Virus (HIV) infection continues to be a serious concern for the military. Preliminary information on the progression of HIV infection, the neuropsychiatric aspects of HIV infection and their potential effect on job performance, and risks of secondary infection, such as coccidiomycosis, in HIV infected soldiers raises some questions.
1. Is there sufficient epidemiological evidence to support the hypothesis that military service accelerates progression of HIV infection? In other words, is the rate of progression greater than would be expected incomparable HIV infected civilian populations?
2. Is there sufficient medical evidence to demonstrate neuropsychiatric impairment at levels.-,great enough to warrant excluding HIV seropositive military personnel, based solely on seropositivity, from military occupations requiring a high level of alertness, correct judgement, and precise motor skills?
3. Is there sufficient epidemiological evidence to demonstrate that HIV seropositive military personnel are at increased risk of developing disseminated coccidiomycosis when assigned to, living in, or traveling to geographical areas endemic for coccidiomycosis when compared to military personnel not infected with HIV?
It is requested that the Board address these questions during its February meeting.
After discussion and consideration, the Subcommittee on HIV Infections and the Board transmitted the following memorandum to the Office of the Assistant Secretary of Defense for Health:
In response to the memorandum from the Office of the Assistant Secretary of Defense on 5 February 1988, the AFEB considered the data presently known about asymptomatic infections with the human immunodeficiency virus (HIV).Based on the excellent presentation, the AFEB states:
1. There is insufficient epidemiological evidence presently available to support the hypothesis that military service accelerates the progression of HIV infection.
2. There is insufficient medical evidence to demonstrate that individuals who are HIV antibody positive, but asymptomatic, experience neuropsychiatric impairment in excess of HIV antibody negative personnel. Until more reliable data are available, the following AFEB recommendation[applying] to neuropsychiatric abnormalities [that] might result from various medical illnesses, including HIV infection, is made:
If mental depression or other neuropsychiatric states occur in any serviceman [or servicewoman] assigned to a stressful or occupationally sensitive position, that person is to have [a] full medical evaluation and [be] returned to that sensitive position only after shown to be functionally fit for duty.
3. While there is sufficient epidemiological evidence to demonstrate that patients with clinically manifest AIDS (those with depressed T4 cells, etc.) are at increased risk of developing disseminated coccidiomycosis when exposed to Coccidiodis immitis, there is not sufficient evidence to indicate greater susceptibility to infection or dissemination in those individuals in the WRAIR Groups 1 & 2.
I had participated in the meetings of the Subcommittee on HIV Infections and the Board, but did not fully concur with all of the recommendations. I had expressed my opinions to members of the Board, and
242
decided to submit a personal letter to Dr. Mayer, the Secretary of Defense for Health Affairs. That letter, dated 9 March 1988, follows:
Dear Dr. Mayer:
The AFEB recently held its winter meeting at WRAIR and devoted considerable time for discussion of the AIDS problem in the Military Services. This discussion culminated in a series of responses to important questions which had been presented to the Board. These responses and recommendations have been transmitted to your office under separate cover.
Often, answers to delicate medical problems are not as precise as they might be simply because there is insufficient data upon which are commendation is based. During the recent meeting, Doctor Mazzuchi and Lt. Col. Peterson reiterated that your office wished to have the recommendations and answers based solely on scientific evidence which was to form the basis for, and conclusions reached, by the Board and its panel of experts.
These answers to the specific questions are now in your hands. It was my privilege to participate in these discussions and to help formulate the recommendations as submitted. However, my personal view is at slight variance with those recommendations, which viewpoint is not fully shared by all members of the Board.
To my mind, there are factors other than those which are directly related to medical or psychoneurological abnormalities. These factors can transcend the known facts and can well relate to functional capability. To be sure, there are currently conflicting data as to whether a person with AIDS, in its early stages, has clearly measurable abnormalities of the central nervous system which would predictably interfere with his or her functional capacity in a high risk or sensitive position. Those factors that transcend this point of reference relate to day-to-day considerations of anxiety, stress, and tension, which clearly relate to function. These human reactions may develop after any catastrophic human event, of which AIDS is a representative example. In contemporary society, the social reaction to this horrible disease influences not only the victim but some of those who are associated with that unfortunate person. Clearly, there are members of society newly placed in contact with an AIDS patient who might react inappropriately to the threat of acquiring AIDS. This is true even though there is no evidence that casual contact relates in anyway to transmission of the virus. These are the weaknesses of human behavior. The threat regarding aberrant behavior may pertain to the victim as well as the one who is associated with that victim.
Any physician who has practiced medicine or psychiatry with a disturbed patient in the confidence of his sick room has witnessed abnormal behavioral traits repeatedly, which have influenced function, even though that person would test negatively to the available scientific measurements.
Until society has fully sifted out and accepted the troublesome and conflicting facets of this dread virus disease, my view is simply that those persons in the military service who are clearly identified as having HIV infection should not be assigned to high risk and sensitive positions. Examples of such high risk and sensitive positions might be the piloting of an airplane, directing the activities of an air traffic station, a high security position and similar occupations. Perhaps with the passage of time, these viewpoints may be found to be obtuse. It seems to me that with the current state of knowledge and uncertainty, better judgment favors the aforementioned consideration.
Sincerely yours,
Theodore E. Woodward, M.D.
President, Armed Forces Epidemiological Board
The Resolution Concerning Confidentiality
In all of the discussions pertaining to AIDS, the Board, collaborating with the military, had continually expressed the need to maintain confidentiality to the highest degree possible. During its February 1986 meeting in San Antonio, the Board had formulated the following resolution:
The AFEB is pleased that its recommended guidelines directed to the means of restriction of spread and control of [HIV] infection within the Armed Forces was favorably received by the Office of Health Affairs of the DoD. The Board maintains its original opinion that
243
{kind=link}
Following her graduation from The Johns Hopkins University School of Medicine and her residency in medicine at its hospital, Carol Johns joined the faculty of that institution. As an exceptionally well-qualified clinician, she chose pulmonary diseases, and in particular, Beck`s sarcoid, for her research interest. Carol has contributed importantly to the clinical and basic knowledge of this strange granulomatous disease. In Baltimore, she is called upon as a consultant in many difficult medical problems.
She served her alma mater, Wellesley College, as its Acting President, and she graciously joined the AFEB as a member despite her heavy academic responsibilities. She has brought a balance to the Board in matters relating both to internal medicine and to the particular needs of women in the Armed Forces.
244
Armed Forces Epidemiological Board and Commission Directors
6-7 June 1985
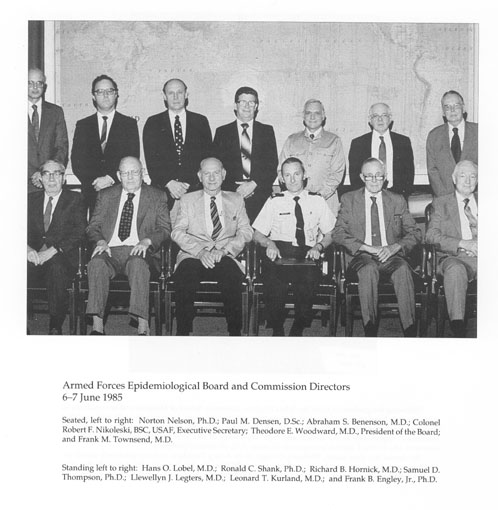{kind=link}
Seated, left to right: Norton Nelson, Ph.D.; Paul M. Densen, D.Sc.; Abraham S. Benenson, M.D.; Colonel Robert F. Nikoleski, BSC, USAF, Executive Secretary; Theodore E. Woodward, M.D., President of the Board; and Frank M. Townsend, M.D.
Standing left to right: Hans O. Lobel, M.D.; Ronald C. Shank, Ph.D.; Richard B. Hornick, M.D.; Samuel D. Thompson, Ph.D.; Llewellyn J. Legters, M.D.; Leonard T. Kurland, M.D.; and Frank B. Engley, Jr., Ph.D.
245
Armed Forces Epidemiological Board and Committee Directors
San Antonio, Texas
13-14 February 1986Seated, left to right: Dr. Frank B. Engley, Jr.; Dr. William E. Jordan, Jr.; Dr. Carol J. Johns; Dr. Theodore E. Woodward, President of the Board; Major General Floyd W. Baker, Commanding General, Health Service Command; and Dr. Paul M. Densen.
Standing, left to right: Dr. Leonard T. Kurland; Dr. Llewellyn J. Legters; Dr. Abram S. Benenson; Colonel Robert A. Wells, MSC, USA, Executive Secretary; Dr. Richard B. Hornick; Dr. Frank M. Townsend; and Dr. Saul Krugman.
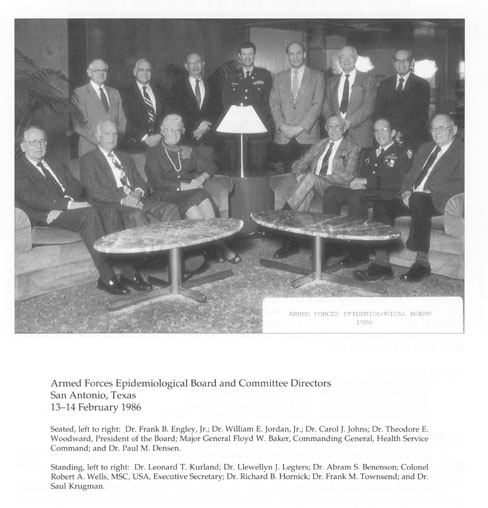{kind=link}
246
the preservation of individual confidentiality be maintained if the program is to succeed. The Board commends the Military Services for the plan to perform a longitudinal evaluation of those persons who now show the presence of [HIV] antibody. Only in this way will it be possible to understand the natural history of this disease which, to this point, has been uniformly fatal once active signs of infection occur. The valuable data which will accrue from a long-term study will provide valuable information of inestimable importance to the Military Services and to the public at large. The governmental policy should be designed so as to insure that all types of accurate medical and epidemiologic information is obtained. In the interrelationships with [HIV-]infected persons, the data collection must allow free communication between the infected service member and the health care provider. Free interchange of reliable information must not be stifled. If there is misunderstanding, lack of confidence and the fear that an adverse policy reaction will penalize or embarrass those involved, no reliable epidemiologic data will accrue. Under such adverse conditions, service members will be motivated to deny or withhold such relevant risk factors as homosexual behavior or drug abuse. An atmosphere of trust will greatly assist in acquisition of reliable epidemiologic information; otherwise, a scientific and accurate study is not possible. Added to the need of insuring an accurate scientific evaluation is the obligation to protect the rights of the individual, an undeniable right.
THE HEALTH PROBLEMS OF ASPLENIC PERSONS
In 1985, another potentially serious medical problem was presented to the Board by the Commander of the Navy Medical Command. Specifically, the Board was requested to determine the immunization requirements for three categories of as plenic persons: congenital as plenics, those whose spleens were removed before they entered the service, and those who had undergone splenectomy following their induction into active duty. After much discussion and review of the pertinent medical literature, the Subcommittee on Infections and the Board formulated the following memorandum and recommendations, dated 25 September 1985:
MEMORANDUM FOR:
THE ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS)
THE SURGEON GENERAL, DEPARTMENT OF THE ARMY
THE SURGEON GENERAL, DEPARTMENT OF THE NAVY
THE SURGEON GENERAL, DEPARTMENT OF THE AIR FORCE
SUBJECT: Immunization of A splenic Personnel
1. At the request of the Commander, Naval Medical Command, Washington, D.C., the Armed Forces Epidemiological Board (AFEB)members and consultants considered a set of questions on a splenic military personnel during the Fall Meeting of the Board at Parson`s Island, Maryland.
2. Although asplenic individuals have been shown to produce lower levels of antibody in response to some antigenic stimuli than those with intact spleens, they withstand common infectious agents including viruses as well. However, asplenic individuals may fail to control infections by encapsulated bacteria such as Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae. Vaccines for these infections are available. In addition, blood protozoal infections(malaria, babesiosis) may not be resisted as well as by the normal host. The post splenectomy sepsis syndrome, however, is a rare event.
3. It has been reported that significantly higher antibody titers against pneumococci develop if vaccine is
247
administered to traumatized persons before splenectomy[rather] than afterwards. There is an antibody response in either instance.
4. The Board recommends [that]:
a. All personnel known to be asplenic should receive one dose of pneumococcal polyvalent vaccine. A second dose need not be given.
b. It should be established that all asplenic persons have received quadrivalent meningococcal vaccine upon entry into the service. If not, this vaccine should be given.
c. Vaccine against Influenza B should be administered to all asplenic individuals.
d. Active duty personnel who require splenectomy should be given the pneumococcal and H. influenzae vaccine prior to removal of the traumatized spleen, if feasible.
e. Asplenic persons should be counselled regarding the importance for them to comply with all anti-malarial measures, especially those related to the use of prophylactic drugs.
f. In areas where babesiosis is prevalent, anti-tick measures should be employed.
g. No restrictions on deployment are necessary for asplenic personnel.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert A. Wells, Ph.D.
Lt. Colonel (P), USA, MSC
Executive Secretary
The Department of the Army raised several additional questions regarding a newly recognized gram negative bacteria known as Dysgonic Fermenter Type 2 (DF-2) in splenectomized individuals. The Subcommittee on Infections and the Board, after discussion and review, submitted the following memorandum, dated 23 September 1987, in answer to the questions presented:
MEMORANDUM FOR
THE ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS)
THE SURGEON GENERAL, DEPARTMENT OF THE ARMY
THE SURGEON GENERAL, DEPARTMENT OF THE NAVY
THE SURGEON GENERAL, DEPARTMENT OF THE AIR FORCE
SUBJECT: Recommendations on Infections with Dysgonic Fermenter Type 2 in Splenectomized Individuals
1. At the request of the Department of the Army Surgeon General, the Armed Forces Epidemiological Board (AFEB) considered at its 7-8 September 1987 meeting a request for recommendations for the problems posed by the serious infections by Dysgonic Fermenter-2 (DF-2) experienced by asplenic individuals following dog and cat bites.
2. Concerning restrictions to be placed on duty assignments of splenectomized individuals which involve contact with dogs and cats, the Board recommends that:
Splenectomized individuals not be newly assigned to duties involving significant exposure to dogs and cats. Those presently assigned or previously trained in animal care should be informed of the risks involved in case of bite and the need for immediate appropriate wound treatment and chemoprophylaxis.
3. With regard to the request for special precautions, if any, following animal bites, the Board recommends that:
248
Appropriate cleansing of the wound be performed with debridement, if necessary, together with an appropriate antibiotic such as Amoxicillin and clauvanic acid (Erythromycin or Tetracycline if the individual is penicillin-sensitive). The need for a booster dose of tetanus must be considered.
4. Concerning guidance to be provided splenectomized pet owners, the Board recommends that:
Splenectomized individuals who own pets should be advised of the hazard of serious infections which may follow bites from cats and dogs. They should be informed of the necessity to seek medical care and chemoprophylaxis, even if the bite is slight.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert A. Wells, Ph.D.
Colonel, USA, MSC
Executive Secretary
THE BOARD ASSISTS THE DEPARTMENT OF DEFENSE
IN FORMULATING POLICY REGARDING THE
HEALTH RISKS ASSOCIATED WITH THE M2 BRADLEY FIGHTING VEHICLE
On 6 November 1986, Maj. General Robert H. Buker, MC, the Deputy Surgeon General, in a memorandum to the President of the AFEB, requested that selected members of the Board and other appropriate authorities be convened to discuss and review health hazard issues associated with the M2 Bradley Fighting Vehicle. An ad hoc group of the Board had reviewed this subject at USAMRIID just the day before, on 5 November. Brig. General Philip Russell chaired the meeting, which I attended with AFEB members Norton Nelson and Ronald Shank, and Executive Secretary Robert A. Wells. Colonel Joel Gaydos and Lt. Colonel Hugh McAlear provided the technical information. It was decided at this meeting to convene a special group of national authorities as soon as possible.
Accordingly, a meeting was held at WRAIR on 6 January 1987. The civilian authorities who participated in this meeting were Drs. Arthur Dubois, Gareth Green, and Roger McClellan, in addition to the Board members and technical authorities aforementioned. The thorough discussions provided sufficient information and reliable data. The ad hoc Committee formulated the following memorandum and recommendations, dated 2 February 1987,which were approved by the Board and submitted to the Surgeon General of the Army:
MEMORANDUM FOR
THESURGEON GENERAL, DEPARTMENT OF THE ARMY
SUBJECT: Recommendation on the Potential for Health Risks of the Bradley Fighting Vehicle (BFV)
1. The Armed Forces Epidemiological Board (AFEB)met to consider the enclosed set of questions pertaining to the health risks o fthe BFV. In order to respond to the request, Board members Dr. Norton Nelson, Dr. Ronald Shank and Dr. Theodore Woodward met with Dr. Arthur Dubois, Dr. Gareth Green and Dr. Roger McClellan. Drs. Dubois, Green and McClellan, as well as Drs. Nelson and Shank are all known, recognized authorities in the fields of toxicology and pulmonary function. Two complete briefings and meetings were held, the first at USAMRDC on 5 November 1986 and the second at WRAIR on 6January 1987. All of the known data pertaining to the BFV were
249
presented and thoroughly reviewed with similar and knowledgeable officers of the Department of Defense and WRAIR with LTC Yancy Phillips as briefing officer.
2. At the outset it was recognized that the combat environment is inherently hazardous. It was likewise clear that given a potentially lethal armored-combat scenario, transient environmental exposure to agents such as fire suppressing chemicals and their pyrolysis products may well represent a reasonable preference over the obvious alternative. This professional advisory group, as any such group, faced an enormous challenge in interpreting the data provided as background to the questions being addressed. Compounding the challenge was the necessity for extrapolating from these data those segments which appeared to have meaningful relevance to the potential health risks of the crew and passengers of the BFV during combat and beyond. An additional task was that of evaluating and prioritizing numerous simultaneous variables within the BFV regarding both the supporting test data and the supposition of events occurring on the battlefield. It was in this manner that the group considered the data and their implications and rendered its recommendations. It should also be noted that these recommendations represent the best possible advice from facts and projections currently available. These recommendations are forwarded with the understanding that as advice, they will be considered for application, modification or rejection as deemed appropriate.
3. Regarding the question on the Halon fire suppression system, it is obvious that the immediate risk within the BFV is fire. Supporting hard copy and film data convincingly showed that the Halon system is an effective firefighting system which will serve the immediate needs of the BFV occupants. Emphasis for the group`s consideration focused on the associated decomposition and oxidation by-products of this system and their potential for toxicity. The Board makes the following recommendation:
The application of the Halon automatic fire suppression system poses an acceptable alternative risk to the occupants of the BFV at this point in time. Continuing efforts should be made to further reduce fire-extinguishing time. Concurrent reexamination of evacuation procedures and those related to personal protection (masking) and ventilation are highly encouraged.
4. With reference to question b-vaporific effects: It was noted that considerations regarding fuel and ammunition were not included in this issue. Following extensive deliberation, the Board feels that:
the vaporific effect does not appear to represent an unreasonable health risk to soldiers in the BFV outside the spall zone.
5. Regarding question c-measurement endpoints: Extensive effort was expended in reviewing underlying BFV test data with consideration of both the underlying questions being addressed and the structuring of the tests. It was the consensus of the group that the studies currently underway will produce valuable information regarding health risks related to nonfragment hazards. In addition, the Board provides the following guidance:
Physical and chemical measurement end points are appropriate with the exception that there should be a review of all sampling flow rates and times with reference to the analytical methods and instrumentation being used to assure they are matched to anticipate exposure constituents and concentrations. In addition, particle size distribution studies should be conducted as well as studies of gas particle interactions.
6. With reference to question d-laboratory animal research: The consensus was that the studies cited represent an excellent starting point for the generation of valuable data. The basic problem is estimating the response to complex mixtures of gases and particles rather than the response to single gases. Thus, the general impression was that these tasks should be structured to mimic the anticipated exposure scenarios as much as possible in the interest of generating useful information in a timely manner. The proposed research will not completely resolve uncertainties relating to health risks from Halon degradation products as found in actual BFV fires. However, they can considerably improve the evaluation of actual risk. Specifically, the Board recommends that:
More emphasis should be placed on field and laboratory stimulation of actual conditions as defined by field studies. Both laboratory and field studies will require the use of animals. Questions to be resolved should include the extent of interaction between gases,
250
{kind=link}
Norton Nelson directed the Institute of Environmental Medicine at New York University from 1954 to 1980. He was recognized as one of this country`s authorities on environmental pollution, air quality, toxic hazards, and safety evaluation. In view of the many problems involving the environment, the AFEB would not have functioned so efficiently as an advisor to the military without Dr. Nelson`s wise counsel. During the years that the Board had a commission system, Norton Nelson spearheaded our understanding of, and the guidelines needed to control, the problem of substance abuse in the military. His work on asbestosis, pesticides, other pollutants, and toxic products related to housing development gave the Board help that was instrumental in saving the government significant financial sums.
251
the particle-effect on dose-delivery to lung tissues, and other issues related to the mode of action of Halon degradation products.
7. Regarding question e-eardrum rupture: The review suggested that ear injury can reduce immediate and future individualeffectiveness, although this may be difficult to distinguish from motivational factors. Following a review of the data, the group endorsed the position that:
By itself eardrum rupture is not likely to cause significant acute disability. Further studies should be conducted in the areas of blast-associated structural and functional disturbances to the inner ear, the shielding effects of hearing protectors, and operational liability of hearing loss for military tasks.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert A. Wells, Ph.D.
Colonel, USA, MSC
Executive Secretary
KOREAN HEMORRHAGIC FEVER
During the summer of 1987, the Departments of the Army and Navy presented the AFEB a series of questions pertaining to the methods of preventing and managing Korean hemorrhagic fever (KHF). Various field operations, including the exercise "Bear Hunt" in the Republic of Korea, had resulted in the development of hemorrhagic fever among military personnel. Korea is highly endemic for this disease. Captain Norman A. Dean, MC,USN, Officer in Charge, Navy Environmental and Preventive Medicine Unit No. 6, Pearl Harbor, Hawaii, had previously prepared a comprehensive report of a hemorrhagic fever outbreak. Dr. Dean reported that among ten severely ill patients fever, fatigue, thrombocytopenia, proteinuria, nausea, and vomiting had occurred in all of them. Diarrhea and myalgia were present in eight patients, and conjunctival injection in five.
After careful study and discussions with the Army and Navy officers who had participated in these field exercises, the Subcommittee on Infections and the Board transmitted the following memorandum and recommendations, dated 23 September 1987:
MEMORANDUM FOR
THE ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAIRS)
THE SURGEON GENERAL, DEPARTMENT OF THE ARMY
THE SURGEON GENERAL, DEPARTMENT OF THE NAVY
THE SURGEON GENERAL, DEPARTMENT OF THE AIR FORCE
SUBJECT: Recommendations on Korean Hemorrhagic Fever
1. The Armed Forces Epidemiological Board (AFEB)considered the problems posed by Korean Hemorrhagic Fever (KHF) with renal syndrome in Korea during its meeting of 17-18 September 1987. These problems were referred to the AFEB by the Surgeons General of the Army and Navy. With respect to appropriate environmental control measures, the AFEB noted that identification of the Apodemus mouse as a reservoir of the etiological Hantaan virus indicates the need to minimize man-mouse contact for the control of this disease. Definitive recommendations cannot be made without additional bionomics of this animal species. The establishment of a planned research laboratory should provide the needed information. Until then, the analogies of some epidemiologic characteristics to those of scrub typhus suggest the best approach.
252
2. Concerning questions on semi-permanent bivouacs or camps in areas endemic for KHF, the Board recommends that:
Bivouac or camps preferably should not be located at any site known to have been a focus of infection for this disease. The Corps of Engineers should prepare a site by first clearing the entire campsite by flame-burning and bulldozing, including the preparation of a wide perimeter extending beyond the bivouac area. The construction of a concrete or gravel base for each tent is advised to prevent rodent harborage. It is essential that all known rodent control measures, including sanitary measures for solid waste, be continually applied. Qualified officers should make regular inspections of the campsite to ensure application of these preventive measures.
3. The environmental control measures instituted in the garrison setting in addition to maintenance of high level of rodent control activities will necessitate behavioral activities by all personnel which minimize the presence of rodents. The Board recommends that:
Continual rodent control measures be strictly applied by all personnel including rodent-proofing of waste food and food scraps, and management of solid wastes (rubbish, etc.) to eliminate harborages. Continual live trapping should be performed with virus studies of the trapped Apodemus mice if facilities for this are available.
4. With regard to personal protective measures for individuals residing in highly endemic areas, the Board states that:
The data presently available do not provide any evidence that there is need for decontamination of individual or unit equipment.
5. In responding to the query on medical evaluation of suspected and confirmed cases of KHF, the Board notes that:
It is desirable that diagnostic competence for the early identification of KFH be available in readily accessible units. Medical competence to treat seriously ill patients, including the capacity for renal dialysis, should be provided. Medical professionals, including contract physicians, who understand the serious complications of the disease, are required to treat such patients. This includes the knowledge and capability to apply measures to combat hypovolemic shock and renal failure. Army and Navy hospital commanders should apply these principles with a clear understanding that transport of seriously ill patients after the first few days is ill advised. Thus, evacuation should only be carried out when the required professional competence cannot be arranged; proper handling of the patient depends on very early diagnosis, and evacuation should be accomplished at sea-level cabin pressure to the closest site where appropriate professional care can be provided.
6. As requested by the Navy Surgeon General, the AFEB reviewed field guidance on KHF made by the Navy Environmental and Preventive Medicine Unit No. 6 (NEPMU-6) on 29 June 1987. The Board states that:
It concurs with the recommendations made in the guidance rendered by NEPMU-6. Concerning the preparation of the campsite, this would preferably be addressed more aggressively as indicated in Paragraph 2 above.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert A. Wells, Ph. D
Colonel, USA, MSC
Executive Secretary
253
{kind=link}
Scott Halstead qualified in medicine at Columbia University College of Physicians and Surgeons, and was a house officer in medicine in New York at Bellevue Hospital. He was commissioned in the U.S. Army Medical Corps in 1958, and compiled a distinguished record at the 406th General Laboratory, the U.S. Army SEATO Medical Research Laboratory in Bangkok, Thailand, and WRAIR. His work embraced the field of virology, and he made major contributions to the understanding of dengue hemorrhagic fever and the immuno pathogenesis of shock in this epidemic viral disease.
Scott contributed to the Commission on Viral Diseases, specifically in arboviruses. He has been Associate Director and Acting Director of the Health Sciences Division of the Rockefeller Foundation while serving simultaneously as a member of the AFEB.
254
Armed Forces Epidemiological Board and Committee Directors
16-17 April 1987
{kind=link}
Left to right: Leonard T. Kurland, M.D.; Walter R. Dowdle, Ph.D.; Samuel D. Thompson, Ph.D.; Frank B. Engley, Jr., Ph.D.; Ronald C. Shank, Ph.D.; Richard B. Hornick, M.D.; William R. Harland, M.D.; Frank M. Townsend, M.D.; Llewellyn J. Legters, M.D.; and Colonel Robert A. Wells, Ph.D., MSC, USA, Executive Secretary.
Left to right: Carol J. Johns, M.D.; Abram S. Benenson, M.D.; Theodore E. Woodward, M.D., President of the Board; Paul M. Densen, D.Sc.; and William S. Jordan, Jr.; M.D.
255
On 26 May 1989, Lt. Colonel James Le Duc briefed the Board on the current status of Hantaan virus infection and KHF. He recalled that during 1951 and 1952, many medical scientists with capabilities in virology, epidemiology, and clinical medicine worked with military medical officers in Korea on the hemorrhagic fever-renal syndrome. The Board had formed a Hemorrhagic Fever Commission, which was directed by Dr. Joseph E. Smadel and Dr. Marshall Hertig. In spite of intensive research, the Commission did not find the viral cause of this hemorrhagic disease. Not until two decades later did a Korean scientist, Dr. Ho Huang Lee, identify the causative agent.
Dr. Le Duc described the serological results of the lyophilized serum samples that Dr. Smadel had arranged to have collected and stored at WRAIR twenty years earlier. Commission workers had taken pains to collect acute (early) and late (convalescent) serum. IgM and IgG assays were tested for Hantaan virus infection and urban-rat-associated Seoul virus with the plaque-reduction neutralization test and enzyme and antibody-capture immunoassays.
Most of the sera from the 245 patients tested showed anti-Hantaan virus antibodies; IgM titers reached their maximal levels within the first few days of illness. IgG titers rose more slowly and reached their maximal level sduring the second week of illness. Measurement of IgM specific antibodies appeared to be the method of choice for early diagnosis of Hantaan virus infections.
In the United States, Dr. Le Duc has collaborated with Dr. James Childs and his associates at The Johns Hopkins School of Public Health on a surveillance of Hantaan virus infection in Baltimore rats. Adult rats taken in urban Baltimore neighborhoods showed evidence of the infection in as much as 50percent of some populations. Attempts are being made to equate hemorrhagic fever virus infection in patients with significant proteinuria, hypertension, and a history of cerebrovascular accidents. The primary focus of the study was inner-city black patients. The thesis under consideration is whether Hantaan virus infections are responsible for a portion of the patients who have chronic renal disease and hypertension. Investigators found that persons who tested seropositive for Hantaan virus fell into the group with chronic renal disease, hypertension, and cerebrovascular accidents. Since acute infection has not been detected in such patients, it is conceivable that subacute infection could lead to chronic renal disease.
AFEB CONTRIBUTION TO
CARDIOVASCULAR SCREENING OF
SOLDIERS AGED 40 AND OLDER
On 26 October 1987, Brig. General James H. Rumbaugh, MC, transmitted a memorandum on behalf of the Surgeon General of the Army to the President of the AFEB. That memorandum follows:
SUBJECT: Review of the 40 and Over Cardiovascular Screening Program
1. The Army revised its Physical Fitness Program in June 1981 to require soldiers 40 years of age and older to take the semi-annual PT test, from which they had been excused since WWII. To prevent exercise-related deaths, a cardiovascular screen is administered as part of the periodic physical examination which is done every 5 years. The screen is a multiphase evaluation; a risk-factor analysis, a cardiology consult and exercise tolerance test, nuclear studies and coronary angiography, and a fourth phase of medical o surgical treatment.
2. Clearance before entrance into the Army`s physical training and testing program is required of all soldiers 40 years of age and older. Clearance may occur during any phase; progressively smaller numbers enter phases II, III, and IV.
3. The Army has screened over 100,000 active-duty soldiers. The data are contained in a computer registry at The Armed Forces Institute of Pathology (AFIP), Washington, DC. The Chief of Staff of the Army intends to extend
256
this program to the 152,000 over-40 members of the Reserve Components, National Guard, and Army Reserve.
4. A Blue Ribbon Panel of Medical Experts endorsed the program design and objectives during a meeting at Walter Reed in December 1986. I also desire the AFEB to conduct its own comprehensive analysis of the Army`s 40 and Over Cardiovascular Screening Program as to its scientific validity and value to the Army. If you can undertake this task, please advise me of the time and resources required to accomplish it. Members of my staff and AFIP will assist you. POC for further information is Colonel Manmohan V. Ranadive, MC.
FOR THE SURGEON GENERAL:
James H. Rumbaugh
Brigadier General, MC
Director, Professional Services
After consulting with appropriate authorities, the Board formed the ad hoc Subcommittee for the Study of Cardiovascular Screening of Soldiers Aged 40 and Over, which would review the Army`s Cardiovascular Screening Program (CVSP) and provide guidance on soldiers aged 40 and older. It met on 27 January 1988 at the Mayo Clinic, in the splendid facilities of the Mayo Foundation in Rochester, Minnesota. Dr. Leonard Kurland was the host for the meeting. A delightful dinner in the Mayo Foundation Residence for Fellows, the former residence of Dr. Charles Mayo, was served. After dinner, I gave a short talk about the AFEB, emphasizing its early history, the founders, and their contributions.
The ad hoc Subcommittee comprised: William P. Castelli, Director of the Framingham Heart Studies; Roland N. Shamburek; L. Thomas Sheffield; David Ballard; and Thomas E. Kottke.
Board members who participated were: William R. Harlan, Chairman of the ad hoc Committee; Leonard Kurland; Lewellyn Legters (who was unable to attend);Robert A. Wells, Executive Secretary; and me. Military representatives who participated were: Lt. Colonel William FitzGerald, USA, MSC; Colonel James R. Hickman, Jr., USAF; Colonel Manmohan V. Ranadive, USA, MC; and Major Jerel Zoltick, USA, MC.
The questions that the Surgeon General of the Army had posed to the Board were contained in the following 1987 memorandum:
MEMORANDUM FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
SUBJECT: Questions on Cardiovascular Screening of Soldiers Age40 and Over
1. Does the available data collected in the 40 and over Cardiovascular Screening Program (CVSP) justify continuation of the program for active duty populations and its extension to the reserve component?
2. Has the CVSP prevented exercise-related sudden death or decreased mortality and/or morbidity from coronary artery disease?
3. If the CVSP has merit in previously sedentary populations, should it be continued in active duty populations now engaged in varying degrees of exercise just when they reach age 40?
4. Does the data justify repeating CVSP every 5 years?
5. If the CVSP should be continued, how can the screening criteria be modified to decrease the number of false positives requiring Phase II screen?
6. If the data collected since the inception of the CVSP in 1981 are not adequate to answer some of the above questions, how should the data collection be modified or what additional data can be collected to answer these questions in the future?
7. Should the existing physical fitness standards be changed? E.g., should over-50 populations be exempted from the APFT test or should these standards be relaxed to make it safer?
257
{kind=link}
Bill Harlan was first affiliated with the AFEB in 1974, when he served on an ad hoc Committee while he was Professor of Medicine at Duke University School of Medicine. At this time, he was actively involved as an advisor to the American Heart Association. That ad hoc group, which was appointed by Herschel Griffin when he was President of the AFEB, made key recommendations regarding the desired weight and blood pressure measurements for military personnel. Most recently, Bill chaired the ad hoc Committee on Cardiovascular Screening for Soldiers Age 40 and Older. This significant report was rendered on 7 April 1988, and for this work, the AFEB is in his debt.
258
COLONEL
MANMOHAN V. RANADIVE, MC, USA
Director, Health and Fitness Division
{kind=link}
LIEUTENANT GENERAL
QUINN H. BECKER, MC, USA
The Surgeon General
{kind=link}
259
8. Should the present program of screening for detection of asymptomatic significant coronary artery disease be replaced by a program of screening for coronary risk factors and risk factor modification?
9. Is there a medico-legal (or standard of practice) requirement to provide state-of-the-art cardiovascular disease screening program every five years just because an organization requires individuals to undergo mandatory physical fitness testing every six months?
10. In the present CVSP an individual with two or three risk factors (smoking, high cholesterol, etc.) can pass the treadmill test and be cleared to take the APRT. Does the program give this individual a false sense of security and would getting clearance on the treadmill test act as a disincentive for this individual to change risk factors?
FOR THE SURGEON GENERAL
Manmohan V. Ranadive
Colonel, Medical Corps
Director, Health & Fitness Division
The ad hoc Subcommittee members reviewed extensive data and experiences in the Army, Air Force, foreign military services, and the U.S. civilian sector pertinent to the questions at hand. The primary focal points for discussion were(a) whether CVSP has prevented exercise-related sudden death, and (b)whether the screening program has decreased overall morbidity and mortality from coronary disease.
Screening for occult coronary artery disease was initially developed to evaluate personnel 40 years of age and older, to reduce fatal and non-fatal coronary events as those personnel increased their physical activity for the mandated Army Physical Fitness Test (APFT). An observational study by Zoltick, et al., which analyzed 188 cardiovascular deaths in the Army since 1981,indicated that screening did not successfully identify those who had fatal episodes when coronary artery disease was the primary cause of death.(References for these studies include Zlotnick, J. M., McAllister, H. A., and Bedynek, J. L., Jr. The United States Army Cardiovascular Screening Program. J.L. Cardiac Rehab. 4: 530-535, 1984; Whitney, E. J. and Boswell, R. N. Cardiovascular Risk Modification: A Multidisciplinary Approach. Military Medicine 151: 473-477, 1986; and Hatsell, C. P. and Gaughan, D. L. USAF Health Evaluation and Risk Tabulation Program. Military Medicine 148:122-126, 1983.) Although the relative risk of a fatal cardiovascular event was less for those "cleared" by CVSP, over half of the deaths occurred in those "cleared to take the APFT." Air Force studies of flight personnel over 40 years of age have found similar difficulties in identifying occult coronary heart disease without performing invasive studies. Parenthetically, a review of a British study of the physical fitness training and testing programs suggested that coronary deaths were not increased significantly during exercise. After all available data were considered, the ad hoc Subcommittee concluded that there was no evidence to suggest that cardiovascular morbidity and mortality had decreased as a result of the screening program of soldiers aged 40 and over. At its 7 April 1988 meeting, the AFEB heard Dr. Harlan`s report of the ad hoc subcommittee. After thorough discussion, the Board approved the following memorandum on cardiovascular screening, and transmitted it to the Surgeon General of the Army:
1. There is no need to screen personnel who have been previously active, have passed the Army Physical Fitness Test (APFT),and who continue to exercise regularly and vigorously without symptoms, solely because they have reached the age of 40 years.
2. The panel reviewed the requirements for expanded studies of the program in weighing options for enhanced clarification and improvement of the program. [The AFEB recommends that:]
An in-depth evaluation of the effect of the Cardiovascular Screening Program (CVSP) on exercise-related death should be conducted. This should include a comparison of death rates before the initiation of the program with those during the program, and to the extent
260
possible, the circumstances surrounding events. A study on age-specific, cause-specific death rates (not necessarily exercise-related) before and during the program should be performed. Collection of this baseline would seem essential in determining the effectiveness and the quality control of the program.
3. The current multi-phase approach used in CVSP was reviewed to identify more efficient and effective approaches to risk screening and interventions. A concern with primary screening criteria has been the high false-positive referral rates for subsequent cardiovascular consultations. It was determined that personal and family medical history, e.g., regarding blood pressure, coronary disease, diabetes, smoking, etc., is often poorly completed and/or poorly scored and probably not sufficiently specific to be useful. [The AFEB recommends that:]
Emphasis be placed on the most reliable of conventional risk factors combined with follow-up counseling and intervention and instructional guidelines for behavior modification. Appropriate coronary risk factor analysis should be continued during routine periodic medical examinations. Emphasis must be placed on improving the measurement of total serum cholesterol and HDL cholesterol with standardization using Centers for Disease Control (CDC) criteria. Other risk factors should include blood pressure measurement and a review of daily smoking status. A total cholesterol to HDL ratio of 6.0 or greater, or the presence of 3 combined risk factors, namely, cigarette smoking (10 cigarettes or greater a day), a blood pressure of 160/90 or above, and a serum cholesterol greater than 250 mg/dl suggest an individual may be at significantly greater cardiovascular risk. Based on these criteria, it was felt that the number of such soldiers requiring Phase II cardiovascular evaluation and treadmill testing should be small. Phase II screening with treadmill exercise for any other criteria is not indicated.
4. Individuals who have significantly abnormal treadmill tests, as described below, should be referred for cardiac catheterization without nuclear studies.
a. Criteria for significantly abnormal treadmill tests:
(1) = less than 2 mm ST horizontal or downslope depression at 0.08 msec at 60% or less age adjusted maximal workload (generally greater than = 8 METs or 27 ml/kg/min).
(2) ST depression remains abnormal longer than 2 minutes post exercise.
(3) = less than 1 mm ST depression accompanied by chest pain.
(4) blunted blood pressure with = less than 1 mm ST depression with early exercise at greater than 80% maximum workload.
b. Nuclear testing should be reserved only for those individuals who have treadmill tests that cannot be adequately interpreted by conventional criteria because of abnormal resting ECG; e.g., LBBB, abnormal ST or T wave changes.
c. Individuals with abnormal treadmill tests who do not fall into either of the above two categories would receive no further diagnostic cardiovascular tests. They should be given counseling for risk factor reduction and individualized exercise prescription. [The AFEB recommends that:]
Asymptomatic active persons with risk factors do not need treadmill testing every five years but should be followed with counseling and intervention to correct unhealthy behavior, and, if they are already exercising, encouraged to continue a regular aerobic exercise program.
5. A review was conducted of APFT standards among soldiers of different age groups. It is understood that given current testing requirements within the Army, most soldiers should have remained relatively active under age 50, and should be able to safely participate in physical activities commensurate with the current APFT requirements. After consideration of these factors, the Board recommends that:
The APFT standards be relaxed for soldiers over 50 years of age, more importantly to protect individuals excercising in this age group, an individualized exercise program
261
should be part of the screening program and their duties should be less physically demanding.
6. In evaluating the overall Army CVSP, it was felt that certain general parameters should be altered or eliminated. The current program does not serve as an incentive for behavioral change that would modify risk factors or increase physical activity. In fact, clearance by CFSP may falsely reassure the individual that behavioral change is not needed to be considered healthy and thus lead to continuance of unhealthy lifestyles. The Board recommends that:
A medical screening program for risk-factor detection and modification be developed as the most promising means of improving health and decreasing the risk of coronary related episodes. An individually graded exercise (2-3 times weekly) with pulse monitoring is prescribed to increase the physical activity and aerobic capacity of all soldiers, particularly those over the age of 40. The current design of the 40-and-over CVSP appears not to serve as an incentive to modify life-endangering behavior into healthier lifestyles. There is no compelling rationale for continuing the current CVSP in active duty soldiers or to extend it to the reserve component.
FOR THE ARMED FORCES EPIDEMIOLOGICAL BOARD
Theodore E. Woodward, M.D.
President, AFEB
Robert Wells, Ph.D.
Colonel, MSC, USA,
Executive Secretary
When he retired as Surgeon General of the Army in June 1988, Lt. General Quinn H. Becker expressed his appreciation to the Board for its assistance in helping to solve some of the aforementioned issues:
Dear Dr. Woodward:
With the approach of my retirement, I want to thank you for your service as President of the Armed Forces Epidemiological Board (AFEB).
You have played a key role in many critical decisions of great importance to the Army and its sister services. Your contributions have involved an array of multi-billion dollar issues including Acquired Immunodeficiency Syndrome (AIDS), Asbestosis, Agent Orange, Cardiovascular Screening and the M2 Bradley Fighting Vehicle. Both your professional knowledge and your leadership are greatly revered by others including myself. I depart my post knowing that our nation is in good hands thanks to your talented and patriotic service to the Board.
Warm regards.
Sincerely yours,
Quinn H. Becker
Lt. General, U.S. Army
The Surgeon General
![]()