



Chapter 22
Medical Causes of Acute Renal Insufficiency
William J. Stone, M.D., James E. Hanchett, M.D., and James H. Knepshield, M.D.
Section I. Acute Renal Insufficiency From Falciparum Malaria
William J. Stone, M.D., James E. Hanchett,M.D., and James H. Knepshield, M.D.
During the 4 years between July 1965 and June 1969, 40 patients with ARI (acute renal insufficiency) caused by falciparum malaria were cared for in the three dialysis centers in the Asian war area (in Saigon; at Clark Air Force Base, Republic of the Philippines; and at Tachikawa Air Force Base, Japan). The pathogenesis, clinical features, and management of those cases are presented here.
MATERIALS AND METHODS
Forty-two cases of ARI caused by falciparum malaria comprise this study. Only patients with a positive blood smear for Plasmodium falciparum were considered. The patients ranged in age from 18 to 42 years, with an average of 22 years. Forty of these patients were members of the U.S. Armed Forces serving in Vietnam. Except in the cases of two soldiers on leave in the United States when symptoms began, initial evaluation and treatment were carried out in a number of hospitals throughout Vietnam. Results of laboratory tests reported were determined by standard methods. Percent parasitemia was calculated by a direct count of parasitized RBC.
Percutaneous renal biopsy was performed on six patients by Schreiner`s (1963) technique. The tissue was fixed in formaldehyde solution (formalin) and stained with hematoxylin and eosin for light microscopy. Immunofluorescent studies by the method of Lange et al. (1966) were performed on heart, lung, and kidney tissue obtained from one patient at postmortem examination. Necropsy results of 10 of the 12 American servicemen who died were reviewed.
The definition of ARI was a sudden daily rise in levels of BUN (blood urea nitrogen) and serum creatinine in the absence of volume depletion and obstruction of the renovascular or collecting systems following an acute illness in patients with no prior history of renal disease. Oliguria (less than 500 ml of urine
_______
This section is a revised version of the following article by the authors (1972): Acute renal insufficiency due to falciparum malaria. Arch Int. Med 129:620-28 (© 1972, American Medical Association).
484
per 24 hours) was usually present. All hemo dialyses were performed under regional heparinization, using a twin-coil dialyzer (Kolff-Travenol).
RESULTS
Table 98 summarizes the clinical data obtained from the 42 patients included in this study, and table 99 gives the laboratory admission data. Thirty-six patients were oliguric; 6 were not. The average duration of symptoms before ad mission to a dialysis unit was 8 days. All patients manifested anemia; the majority-36 (86 percent)-showed significant hemolysis.
In 31 of the 42 patients, a parasite index was calculated on the basis of the blood smear obtained on admission to the original hospital. Twenty-two of 31(71 percent) had at least 10-percent parasitemia. Eight (36 percent) of these had 60 to 90-percent parasitemia. The parasite index, as shown in table 100, tended to be lower in survivors than in fatal cases.
Hyperkalemia was found in only five patients (12 percent of admissions). In contrast, severe azotemia with evidence of hypercatabolism (BUN: creatinine ratio >10) was the rule, as had been noted previously (Brooks et al. 1967; Jackson and Woodruff 1962). Hepatic dysfunction was seen in nearly all patients. Roentgenograms of the chest were abnormal in 23 of 42 (55 percent), with findings ranging from small infiltrates to extensive opacification of lung fields. Seven of 11 patients tested had a coagulation disorder suggesting a consumption
485
coagulopathy (table 101). Several other patients manifested a bleeding diathesis but had insufficient coagulation tests to establish a definite diagnosis.
486
Except for one patient (patient 24) who contracted his disease in 1965 (before the widespread recognition of chloroquine-resistant P. falciparum), all patients received quinine sulfate or quinine hydrochloride, administered orally or parenterally. Prompt clearing of parasitemia occurred in all patients receiving quinine. Other antimalarial agents employed were pyrimethamine, primaquine phosphate, chloroquine phosphate, sulfisoxazole, sulfadoxine, and dapsone. Large doses of corticosteroids were usually given to patients manifesting symptoms of cerebral malaria or respiratory distress associated with pulmonary edema or hemorrhage. Management of renal failure consisted of restriction of protein, sodium, potassium, and water intake alone (10 patients); peritoneal dialysis (6 patients); and hemodialysis (23 patients). The average duration of oliguria was 8 days, with a range of 1 to 19 days. An average of four hemodialyses were performed on the patients requiring dialysis. Peritoneal dialysis was employed when patients showed less severe catabolic changes. Three patients died before dialysis could be initiated.
Of the 42 patients included in this study, 12 died. All were oliguric and had at least one and usually both of the other potentially lethal complications (cerebral and pulmonary) of falciparum malaria. Eight patients (67 percent) who died had severe pulmonary involvement which was believed to be the primary cause of death in six (50 percent) (fig. 90). Eleven (92 percent) had cerebral
487
malaria, which was considered the main cause of death in four (33 percent). One patient died of a massive upper gastrointestinal tract hemorrhage in association with marked thrombocytopenia and hypoprothrombinemia. Another died of gram-negative bacteremia secondary to peritoneal contamination at the time of peritoneal dialysis. No deaths resulted from uremia or hyperkalemia.
Among the 30 survivors, 1 (3 percent) had severe pulmonary involvement while 11 (37 percent) had moderate to severe cerebral malaria. Twenty of the survivors required some form of dialysis. All patients without oliguria lived, and none required dialysis therapy. The incidence of complications was much less in nonoliguric patients.
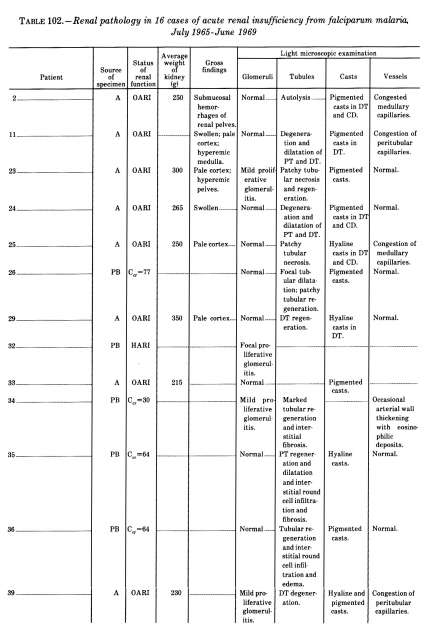
The renal pathologic findings in 10 necropsies and 6 percutaneous biopsies are summarized in table 102. At necropsy, the kidneys were enlarged with pallor of the cortex and hyperemia of the medulla. Findings on microscopic examination of both biopsy and necropsy material were similar. Evidence of a mild glomerulitis consisting of slightly increased cellularity was observed in eight (20 percent) of the specimens. Tubular changes included degeneration and dilatation of the proximal and distal nephron, patchy necrosis, and occasional interstitial
488
{kind=link}
489
round cell infiltration and edema. Most sections showed pigmented casts, particularly in the distal nephron. Striking medullary capillary congestion was seen in 30 percent of the cases (fig. 91). Immunofluorescent studies on renal tissue for immunoglobulins IgG, IgA, IgM, and β1C were negative in one patient studied.
DISCUSSION
Acute renal insufficiency has been recognized in many medical conditions, including thermal burns, gram-negative bacteremia, crush injury, and transfusion reaction, and following administration of certain drugs. It was commonly referred to as acute tubular necrosis in the past. Recovery is usual if the patient can be maintained by dialysis and other supportive measures during the oliguric phase. Renal histopathology during the acute period does not reflect the severe functional derangement seen (Finckh, Jeremy, and Whyte 1962; Olsen and Skjoldborg 1967; Brun and Munck 1957).
Many observations point to a similar situation occurring in ARI caused by falciparum malaria. Oliguria and subsequent diureses are common. Nonoliguric ARI has been noted less frequently (Sitprija et al. 1967).
Pathologic findings in the kidneys of patients with ARI caused by falciparum malaria have been mild to minimal. Spitz (1946) found evidence of glomerular involvement in 18 percent of 50 fatal cases of falciparum malaria during World War II. Light microscopic findings in these glomeruli consisted of
490
"generalized ischemia, enlargement and increased cellularity of the glomerulus, hyperchromatism and swelling of the endothelium, and occasionally thickening of the basement membranes." Pigmented casts were found in the distal nephrons of more than half of the cases; however, only 14 percent demonstrated tubular necrosis or degeneration. Proximal tubules were dilated and filled with proteinaceous fluid.
Maegraith and Findlay (1944; Maegraith 1944) found few RBC`s in glomerular capillaries, "anemia" of the cortex, and congestion of the medulla. They suggested that a vasoconstrictive process produced the renal insufficiency.
491
Sitprija and coworkers (1967) studied three patients with nonoliguric ARI caused by heavy P. falciparum infestation. There was no evidence of intravascular hemolysis. Renal biopsies showed normal glomeruli and only focal vacuolization of proximal tubules. Six patients from Central Africa with falciparum malaria and ARI demonstrated similar minimal changes consisting of tubular degeneration and casts on renal biopsy (Dukes, Sealey, and Forbes 1968).
Burdick reviewed three renal biopsies from patients with oliguric ARI caused by falciparum malaria. Light microscopy was normal. However, on electron microscopy he found moderate focal basement membrane thickening and small membrane-limited vacuoles within the basement membrane which may have been artifacts. Jackson and Woodruff (1962) reported on the renal findings in three cases of severe P. falciparum infection and renal failure. They found tubular necrosis of varying degree, and tubular casts, but no glomerular involvement.
Rosen and coworkers (1968) studied renal biopsy specimens of six soldiers with "blackwater fever" from falciparum malaria, three of whom were oliguric. Pathologic changes included casts, tubular atrophy, and focal fibrosis. Two of the six cases had glomerular abnormalities consisting of epithelial inclusions and hyalinization.
Review of our necropsy and biopsy material supports the concept that the morphologic changes in the kidney in no way explain the excretory defect. Nearly all glomeruli appeared normal. The observed tubular abnormalities were mild and had focal distribution.
Glomerulonephritis of the immune complex type can occur in certain types of malaria. Deposition of immunoglobulins IgG and β 1 C in glomeruli has been demonstrated by fluorescent antibody technique in rhesus monkeys infected with P. cynomolgi (Ward and Conran 1966) and in humans with P. malariae infestation (Kibukamusoke 1968; Allison et al. 1969). The nephrotic syndrome resulting from a proliferative glomerulonephritis has been described in three cases of falciparum malaria acquired in Vietnam (Berger, Birch, and Conte 1967). Unfortunately, immunologic techniques were not applied to these biopsies. However, glomerulonephritis as a cause of oliguria and azotemia is rare in falciparum malaria in comparison with ARI. Four cases in the current study showed evidence of a mild glomerulitis on biopsy. To the authors` knowledge, none subsequently developed the nephrotic syndrome or chronic renal insufficiency. In the only specimen studied for renal deposition of immune complexes, no IgG or 1C was demonstrated.
The similarity between the clinical courses of these patients and of those previously reported on is striking (Jackson and Woodruff 1962; Reid, Goldsmith, and Wright 1967; Canfield et al. 1968; Donadio, Whelton, and Kazyak 1968). A significant interval between the onset of symptoms and the institution of appropriate therapy was typical. Marked anemia and parasitemia were usually present. Cerebral, hepatic, and pulmonary involvement frequently complicated the initial period, particularly when treatment was delayed. A bleeding tendency was evident. The patient had severe toxic and catabolic reactions. Acute renal insufficiency could be readily managed if peritoneal dialysis or hemodialysis
492
facilities were available.
None of the patients in this study died of renal failure. However, the other complications of severe infestation with P. falciparum are less amenable to therapy and cause a significant mortality. Of the 12 fatalities, 6 died primarily of pulmonary involvement and 4 of cerebral involvement. All those who died had either pulmonary or cerebral complications and usually both. Initial delays in diagnosis and treatment may have contributed to the development of these lesions.
In the early period (1965-66) before a dialysis facility was established in Vietnam, patients requiring dialysis were flown to Japan or the Philippines. This critical delay of at least 12 hours may have contributed to the inordinate mortal ity (50 percent) observed in these patients. The later mortality (14 percent) probably reflects the value of early treatment (chart 29).
Similar delays have been recorded in the deaths from falciparum malaria in the U.S. civilian community. A low index of suspicion has been the single most troublesome factor. On therapeutic and epidemiological grounds, it is imperative that the diagnosis of malaria be sought in all individuals with unexplained febrile illnesses who return from endemic malarial regions.
493
Intravenously administered quinine hydrochloride was the cornerstone of therapy in severe P.falciparum infection. The usual daily dosage had to be decreased to 600 mg in the presence of oliguria to prevent toxic blood levels of quinine (Donadio, Whelton, and Kazyak 1968). This was given in 500 ml of dextrose solution over 24 hours and was continued for 10 to 14 days. Blood quinine levels were determined at regular intervals and the electrocardiogram was monitored for signs of toxic reaction (widened QRS complexes). In the absence of renal insufficiency, the recommended treatment regimen for falciparum malaria was the simultaneous initiation of quinine sulfate, 1,950 mg daily for 10 days; pyrimethamine, 25 mg twice daily for 3 days; and dapsone, 25 mg daily for 28 days (USARV Reg.) Sulfisoxazole, 500 mg four times daily for 5 days, was substituted for dapsone on occasion.
In treating patients with ARI from falciparum malaria, it was our practice to delay administration of pyrimethamine, dapsone, and sulfisoxazole until the recovery period. The dialysance of these drugs was not known, and recurrences of parasitemia did not occur when administration was delayed until the diuretic phase.
Section II. Acute Renal Insufficiency in Other Medical Disorders
James H. Knepshield, M.D., and William J.Stone, M.D.
A review of the records of the 629th Medical Detachment (Renal) reveals 12 medical causes of renal failure resulting in admission to the unit. Distribution of cases by cause was as follows:
Falciparum malaria - 13
Hemolytic anemia - 12
C-4 plastic explosive - 4
Chloroquine ingestion with overdose - 1
Heat stroke - 1
Hemolytic-uremic syndrome - 1
Serratia pneumonia - 1
Letptospirosis - 1
Acute glomerulonephritis - 4
Chronic glomerulonephritis with acute decompensation - 4
Goodpasture’s syndrome - 1
Interstitial nephritis, phenacetin abuse - 1
Hemolytic anemic states ranked second in frequency as a cause of acute renal failure. Considering the large population receiving malaria chemoprophylaxis, the actual number of severe hemolytic reactions was small. Acute infections added to the potential for hemolytic reaction among patients with G6PD (glucose-6-phosphate dehydrogenase) deficiency.
Acute renal insufficiency in a G6PD-deficient patient with viral hepatitis, who subsequently recovered, was described by Salen and coworkers (Salen et al. 1966). Drug-induced hemolysis, which had been well described since the early
494
1950`s, produced severe degrees of hemolytic anemia uncomplicated by renal failure. In view of the frequency with which this red cell enzyme deficiency has been reported throughout the world, it is surprising that renal failure has not been more common.
The deployment of large numbers of American troops to Southeast Asia exposed individuals with the enzyme deficiency to the hemolyzing agent primaquine, as well as dapsone (diaminodiphenylsulfone) in some geographic sectors. The quantity of these drugs taken for routine chemoprophylaxis (primaquine, 45 mg base once per week; dapsone, 25 mg per day) was well below the amounts that have produced clinically overt hemolysis in most WD-deficient black American subjects; however, this was not always true in the white soldier (Carson and Frischer 1966).
Two cases of acute renal failure in G6PD-deficient black American troops in South Vietnam were reported. Massive intravascular hemolysis in these patients was not induced by the antimalarial agents or by other drugs per se but was associated with unsuspected rickettsial infections. One patient had scrub typhus and the other, murine typhus (Whelton, Donadio, and Elisberg 1968).
A review of 3 years` experience in Vietnam with acute renal insufficiency (table 103) shows that 31 percent of admissions were for medical causes. There was an overall survival rate of 79 percent in the medical group treated during that period.
Section III. Toxic Effects Following Ingestion of C-4 Plastic Explosive
James H. Knepshield, M.D., and William J. Stone, M.D.
Composition C-4, the most common plastic explosive used by field units in Vietnam, is a mixture of four potentially toxic substances: RDX (cyclonite), 91 percent; polyisobutylene, 2.1 percent; motor oil, 1.6 percent; and di(2-ethylhexyl) sebacate, 5.3 percent. Figure 92 shows the chemical structure for the major com-
_______
This section is taken from the following article: Stone, W. J.; Paletta, T. L.; Heiman, E. M.; Bruce, J. I.; and Knepshield, J. H. 1969. Toxic effects following ingestion of C-4 plastic explosive. Arch. Int. Med 124: 726-30 (© 1969, American Medical Association).
495
ponent, RDX, a colorless crystal which is highly insoluble in water (0.0076 g/100 g solvent at 25°C) (DA-TM). Because C-4 is a malleable solid, burns without explosion, and is relatively insensitive to impact or friction, it can be easily transported and stored without undue precautions (fig. 93). A blasting cap is employed as a detonator. C-4 may even be used as a field cooking fuel when other sources of heat are unavailable. However, when it is ingested or inhaled in significant quantities, by either accident or intent, a dramatic clinical picture develops within a few hours. Generalized seizures, gross hematuria, severe nausea and vomiting, muscle twitching, and mental changes occur.
It was common knowledge among the field troops in Vietnam that the ingestion of a small quantity of C-4 produces a "high" similar to that produced by alcohol. The exact frequency of ingestion of the material was not known; however, several serious intoxications from this agent were seen in every major military hospital in the Republic of Vietnam. Toxic effects of C-4 have also involved the civilian community in the United States. Inhalation of the dust was incriminated when factory workers who handled and packed the explosive experienced convulsions (Merrill 1968). C-4 is a potential health hazard in the
496
United States because of its availability on many military installations, although rigid control of its use makes this unlikely.
The six male patients summarized here had toxic effects from C-4 severe enough to warrant hospitalization (table 104). Their ages ranged from 20 to 35 years, with an average of 24 years. The estimated quantity of ingestion in three of the patients was 25 to 180 g (average 77 g). Data for two of the patients are from Merrill`s report (1968).
497
TABLE 104.- Symptoms and signs of six patients with C-4 intoxication
All patients were admitted to the hospital for the management of generalized seizures. When initially seen, most were conscious but stared into space confusedly. They were restless and unpredictable and required restraints. At frequent intervals, generalized seizures lasting 1 to 2 minutes occurred. Between seizures, the state of consciousness varied from coma to lethargy. Other prominent symptoms and signs were severe neuromuscular irritability with muscular twitching and hyperactive reflexes, myalgias, frontal headaches, nausea, vomiting, gross hematuria, and fever. Within 48 hours, the patients were able to answer simple questions and follow directions, but orientation, concentration, recall, and memory for recent and remote events were impaired. After 1 week, the sensorium cleared; however, remote memory continued to be defective with spotty recall for both personal experiences and well-known facts. Follow up indicated that mental capacity had returned to normal in about 1 to 2 months. Neuromuscular irritability, gastrointestinal symptoms, hematuria, and fever abated within 48 hours. Headaches persisted for 1 to 3 weeks.
The abnormal laboratory findings are summarized in table 105. Within 2 weeks, all the abnormal values returned to normal except for the hematocrit in one patient and urinary protein excretion in another.
During the first week following ingestion of C-4, muscle, liver, and renal biopsies were performed on a patient with an elevated SGOT (serum glutamicoxaloacetic transaminase) (354 units) and moderate azotemia with microscopic hematuria. Although the muscle biopsy was normal, muscle injury was still considered most likely because the patient complained of myalgias and muscle tenderness. Only a small portion of the latissimus dorsi was examined. The absence of hepatomegaly and of abnormal findings in the liver function studies and liver biopsy effectively excluded liver involvement. Renal biopsy showed minimal changes consisting of mild vacuolization of the proximal tubules most likely caused by mannitol therapy. There was transient hematuria and azotemia. Although a glomerulitis could also account for these abnormalities, the absence of glomerular changes by light and electron microscopy in the renal biopsy obtained 5 days after the ingestion made this diagnosis improbable. The early ad-
498
TABLE 105. - Laboratory data of patients with C-4 intoxication
ministration of mannitol may have modified the course of acute tubular necrosis in this patient. Prerenal azotemia was excluded because congestive heart failure and volume depletion were not present in any of the six patients. Additionally, a bone marrow aspiration was performed on the patient because of persistent normochromic, normocytic anemia. The findings of erythroid hypoplasia and a normal marrow iron content were consistent with toxic depression of the erythroid series. Mild anemia was found in three other patients.
Two abnormalities persisted in the patient who had ingested the largest quantity of C-4. At the time of evacuation on the 30th hospital day, anemia (hematocrit 33 percent) and loss of memory for recent events were still present. The patient`s clinical course suggests that larger quantities may cause serious complications that persist for an extended period. The ingestion of a small quantity of C-4 (a few grams) is unlikely to produce any serious long term adverse effects.
The management of C-4 intoxication consisted of early gastric lavage; maintenance of an airway and prevention of aspiration of gastric contents; control of seizures with anticonvulsants; monitoring of hourly urine volume to detect acute renal insufficiency at its onset; and maintenance of normal fluid and electrolyte balance. In the presence of oliguria, a test dose of 25 g of mannitol or 200 mg of furosemide was given. If diuresis did not ensue, an acute renal insufficiency regimen was instituted. Because of its chemical structure and solubility characteristics, aqueous hemodialysis or peritoneal dialysis cannot remove significant quantities of RDX, which is presumed to be the cause of the toxic effects of C-4. The other constituents of composition C-4 are large molecules in low concentrations and are probably nontoxic in the quantities ingested. RDX is lipid-soluble; therefore, it is probably selectively accumulated in the central nervous system and body fat similarly to thiopental and glutethimide. This suggests that hemodialysis using soybean oil or cottonseed oil in the bath might be beneficial in the critically ill patient. No patient with C-4 intoxication in this study required dialysis.
499
REFERENCES
Allison, A. C.; Houba, V.; Hendrickse, R. G.; De Petris, S.; Edington, G.M.; and Adeniyi, A. 1969. Immune complexes in the nephrotic syndrome of African children. Lancet 1: 1232-38.
Berger, M.; Birch, L. M.; and Conte, N. F.1967. The nephrotic syndrome secondary to acute glomerulonephritis during falciparum malaria. Ann. Int. Med 67:1163-71.
Brooks, M. H.; Malloy, J. P.; Bartelloni, P.J.; Tigertt, W. D.; Sheehy, T. W.; and Barry, K. G.1967. Pathophysiology of acute falciparum malaria. I. Correlation of clinical and biochemical abnormalities. Am. J. Med. 43: 735-44.
Brun, C., and Munck, 0. 1957. Lesions of the kidney in acute renal failure following shock. Lancet 1: 603-7.
Burdick, C. 0. Electron microscopical investigation of renal disease of the military forces in the Far East. In 406th Medical Laboratory Professional Report, U.S. Army Medical Command(Japan), July 1965-June 1966, pp.335-47.
Canfield, C. J.; Miller, L. H.;Bartelloni, P. J.; Eichler, P.; and Barry, K. G. 1968. Acute renal failure in Plasmodium falciparum malaria. Arch. Int. Med 122:199-203.
Carson, P. E., and Frischer, H. 1966.Glucose-6-phosphate dehydrogenase deficiency and related disorders of the pentose phosphate pathway. Am. J. Med 41:744-61.
DA-TM-Department of the Army. 1955.Militaryexplosives. Technical Manual (TM) 9-1910, pars. 55,66.
Donadio, J. V., Jr.; Whelton, A.; andKazyak,L.1968. Quinine therapy and peritoneal dialysis in acute renal failure complicating malarial haemoglobinuria. Lancet1: 375-79.
Dukes, D. C.; Sealey, B. J.; and Forbes, J.I. 1968. Oliguric renal failure in blackwater fever. Am. J. Med. 45: 899-903.
Finckh, E. S.; Jeremy, D.; and Whyte, H. M.1962. Structural renal damage and its relation to clinical features in acute oliguric renal failure. Quart. J. Med.31: 429-46.
Jackson, R. C., and Woodruff, A. W.1962. The artificial kidney in malaria and blackwater fever. Brit. M. J. 5289:1367-72.
Kibukamusoke, J. W. 1968. Malariaprophylaxis and immunosuppressant therapy in management of nephrotic syndrome associated with quartan malaria. Arch. Dis. Child. 43: 598-600.
Lange, K.; Treser, G.; Sagel, I.; Ty,A.; and Wasserman, E. 1966. Routine immunohistology in renal diseases. Ann. Int. Med. 64: 25-40.
Maegraith, B. 1944. Blackwater fever anuria. Tr.Roy. Soc. Trop. Med & Hyg. 38: 1-23.
Maegraith, B. G., and Findlay, G. M.1944.Oliguria in blackwater fever. Lancet 2: 403-4.
Merrill, S. L. 1968. Ingestion of an explosive material,compositionC-4: A report of two cases. USARVM. Bull (USARV Pam 40-8), March-April, pp. 5-11. Copy inJoint Medical Library, Office of the Surgeons General.
Military explosives, Department of the Army Technical Manual. See DA-TM.
Olsen, T. S., and Skjoldborg, H.1967.Thefine structure of the renal glomerulus in acute anuria. Acta path. et. microbiol. scandinav. 70: 205-14.
Reid, H. A.; Goldsmith, H. J.; and Wright, F.K.1967. Peritoneal dialysis in acute renal failure following malaria. Lancet 2: 436-39.
Rosen, S.; Hano, J. E.; Inman, M. M.; Gilliland, P. F.; and Barry, K. G. 1968. The kidney in blackwater fever. Light and electron microscopic observations. Am .J. Clin. Path. 49:358-70.
Salen, G.; Goldstein, F.; Haurani, F.; and Wirts, C. W. 1966. Acute hemolytic anemia complicating viral hepatitis in patients with glucose-6-phosphatedehydrogenase deficiency. Ann. Int. Med. 65: 1210-20 .
Schreiner, G. E. 1963. The nephrotic syndrome. In Diseases of the kidney, ed. M. B. Strauss and L. G. Welt, pp. 335-45. Boston: Little, Brown & Co.
Sitprija, V.; Indraprasit, S.; Pochanugool, C.; Benyajati, C.; and Piyaratn, P. 1967. Renal failure in malaria. Lancet 1: 185-88.
Spitz, S. 1946. The pathology of acute falciparum malaria. Mil. Surg. 99: 555-72.
Stone, W. J.; Hanchett, J. E.; and Knepshield, J. H. 1972. Acute renal insufficiency due to falciparum malaria. Arch. Int. Med. 129: 620-28.
Stone, W. J.; Paletta, T. L.; Heiman,E. M.; Bruce, J. I.; and Knepshield, J. H. 1969. Toxic effects following ingestion of C-4 plastic explosive. Arch. Int. Med 124: 726-30.
Treatment of malaria, USARV Regulation. See USARV Reg.
USARV Reg-Headquarters, USARV. 1968.Treatment of malaria. USARV Regulation Number40-33, 15 Mar. 68.
Ward, P. A., and Conran, P. B. 1966.Immunopathologic studies of simian malaria. Mil. Med 131(supp.): 1225-32.
Whelton, A.; Donadio, J. V., Jr.; and Elisberg, B. L. 1968. Acute renal failure complicating rickettsial infections in glucose-6-phosphate dehydrogenase-deficientindividuals. Ann. Int. Med69: 323-28.
![]()