



CHAPTER XII
Corps Services
Nursing Service
The men and women of the ANC (Army Nurse Corps) have provided nursing care ofthe highest quality to U.S. troops in Vietnam since mid-1962. Thirteen nurseswere included on the staff of the 8th Field Hospital which arrived at Nha Trangin March 1962. Thereafter the number of nurses sent to Vietnam increasedgradually as the troop buildup continued. The number reached a peak strength of900 in January 1969, after which it fell rapidly to about 650 by July 1970 asthe withdrawal of U.S. troops gained momentum.
Administration
From 1962 through 1964, when the 8th Field Hospital was the only Armyhospital operating in Vietnam, the nursing service did not require theassignment of a chief nurse as a special staff adviser to the surgeon at Armycomponent headquarters in order to function efficiently. In anticipation of theimminent buildup of Army combat and support forces, a decision was made to placea chief nurse on the staff of the USASCV surgeon early in 1965. On 3 February,Lieutenant Colonel Margaret G. Clarke, ANC, senior nurse at the 8th FieldHospital, was assigned that position as an additional duty.
Just as was true for all other Medical Department officers who wore two hatsduring that period, the physical separation of the 8th Field Hospital fromHeadquarters, USASCV, in Saigon, hindered Colonel Clarke in the accomplishmentof her staff responsibilities. Consequently, when USASCV was redesignatedHeadquarters, USARV, on 20 July 1965, a primary duty space was authorized in thesurgeon's office for a staff nurse. However, not until 15 September, whenColonel Clarke was transferred from the 8th Field Hospital to Headquarters,USARV, to assume the duties of chief nurse, was that position filled.
As chief nurse on the staff of the USARV surgeon, Colonel Clarke and hersuccessors acted as advisers on all nursing activities, and as nursingconsultants for the medical service structure in Vietnam. The scope of herresponsibilities included initial assignments for incoming ANC officers andrecommendations on personnel actions. That Colonel
143
Clarke, as the first full-time chief nurse in Vietnam, did her job well isreflected in her winning the award of "U.S. Army Nurse of the Year" in1965.
The arrival of the 44th Medical Brigade in 1966 had no appreciable effect onthe staff structure for nursing service in Vietnam. The USARV chief nurse simplyassumed a second staff position as staff nurse at Headquarters, 44th MedicalBrigade. By 9 March 1967, however, increases in ANC personnel and expandednursing activities in the theater of operations warranted the assignment of afull-time nursing adviser to the staff of the commanding officer of the brigade.Consequently, Lieutenant Colonel (later Colonel) Rose V. Straley, ANC, wasappointed chief nurse with responsibility for assigning and managing all ANCpersonnel within the brigade.
On 10 August 1967, the 44th Medical Brigade became a major subordinatecommand of USARV headquarters. As a result of that reorganization of the medicalservice structure, a position for a staff nurse in the brigade headquarters wasdeleted. Colonel Straley was reassigned to the 24th Evacuation Hospital withduty assignment as assistant chief nurse in the USARV surgeon's office. Onceagain, the USARV chief nurse donned a second hat as chief nurse of the 44thMedical Brigade.
The final reorganization of the U.S. Army medical service structure inVietnam occurred on 1 March 1970, when Headquarters, 44th Medical Brigade, wasconsolidated with the USARV surgeon's office. The unified USAMEDCOMV retained achief nurse as a staff adviser to the USARV surgeon and the USAMEDCOMVcommanding general, and as nursing consultant for all U.S. Army medicalfacilities in Vietnam.
Assignments. The tour of duty was 1 year and this caused a problem ofstaff rotation in hospitals. Most hospitals arrived with a full complement ofnurses whose tours ended simultaneously, necessitating complete restaffing atthe end of the year. While waiting for the hospital to become operational, theoriginal nurses were permanently assigned to units already in operation. As thehospital began to receive patients, nurses were assigned to the staff so thattheir eligibility for return to the United States would be staggered, thussolving the problem of mass rotation to some extent.
Assignments were often based on unit needs rather than on TOE (table oforganization and equipment) authorization. Owing to rapidly changing needs, newassignments were made to a specific unit after the nurse's arrival in-country.Some factors used to meet hospital staffing requirements were the type andrapidity of admissions and dispositions, the status of enlisted staffing, andthe strength or weakness of the individual officer assigned. Most nurses wereassigned to hospitals and to the 6th Convalescent Center at Cam Ranh Bay. Nurseswere authorized
144
by TOE for thoracic, orthopedic, neurosurgical, maxillofacial,neuropsychiatric, renal, and other specialized teams.
The difficulty of assigning nurses was further complicated by the fact that60 percent of the nurses assigned had less than 6 months' active duty and lackedexperience in combat nursing. Vietnam became a training ground for a largenumber of inexperienced officers. This problem was solved by the institution ofintensive training programs in each unit and continuous counseling and guidanceby more experienced nurses. Army nurses also participated in professionalconferences sponsored by the Allied Nations medical personnel in-country.
There was a crucial need for nurses trained in certain specialized skills.The critical need for operating-room nurses was lessened by cross training andby lending trained nurses to other hospitals in emergencies such as increases incasualties. To meet Vietnam needs, the length of the operating-room course (inthe United States) was decreased from 22 to 16 weeks and offered at eight Armyhospitals. The rise in the number of medical units caused by the troop buildupand high casualty rates increased the need for nurse anesthetists. Becausereplacements sent to Vietnam were often inexperienced, the policy of utilizingsenior nurse anesthetists as instructors and traveling consultants was initiatedin 1970. Ward patient care was adversely affected by the lack of field grademedical-surgical nurse supervisors; however, this shortage was alleviated byusing experienced captains in supervisory positions.
Utilization of male nurses. Since 1955 men have received commissionsin the Amy Nurse Corps. Male nurses were assigned to organic medical units ofmajor combat elements as well as to hospitals in Vietnam. Male nurseanesthetists were assigned to the 173d Airborne Brigade, the 101st AirborneDivision, and the 1st Cavalry Division (Airmobile). They gave direct patientcare, supervised nursing activities, and administered anesthesia to patientsduring emergency surgical procedures. One-half of all male nurses were in theclinical nursing specialties of anesthesia, operating room, and neuropsychiatry.Male nurses were used in special situations as in November 1967 when the nursingservice of the 18th Surgical Hospital (MUST) was reorganized as an all-male unitin anticipation of increased enemy activity.
Combat Nursing
The highest quality of nursing care was given despite the constant threat ofattack. All hospitals from the northern highlands at Pleiku to the Delta townof Vung Tau were vulnerable to enemy mortar, rocket, and small arms fire.Several, such as the 45th Surgical Hospital at Tay Ninh, the 3d Field Hospitalat Saigon, and the 12th Evacuation Hospital at Cu Chi, for example, were hit oneor more times. First Lieutenant
145
U.S. Army Nurses Hold Sick Call at a VietnameseOrphanage
{kind=link}
Sharon Anne Lane, ANC, was killed by hostile fire on 8 June 1969, while onduty at the 312th Evacuation Hospital at Chu Lai. On 11 November 1969, anintensive care ward at Fitzsimons General Hospital, Denver, Colo., was formallydedicated as the Lane Recovery Suite in memory of her service at that hospital.
The principles of good nursing remained unchanged in Vietnam but ingenuitywas required to maintain high standards of nursing care. The nurses used theirresourcefulness to overcome a lack of certain equipment. Stones in a Red Crossditty bag made weights for traction, a piece of Levin's tube could be used as adrinking straw, plastic dressing wrappers served as colostomy bags, soap andintravenous bottles were used as chest drainage bottles, and items of equipmentnot authorized by hospital TOE were designed and constructed from scrap lumberand other materials. Improvements were constantly needed, and some were made inmethods of sewage disposal and in bathing and laundry facilities. Duringseasonal offensives, heavier-than-normal workloads were placed on medical units,and all nurses went on 12-hour work schedules in order to maintain highstandards of nursing.
Army nurses voluntarily gave medical assistance to the Vietnamese duringtheir off-duty hours. Clinics were established and staffed by nurs-
146
ing personnel who gave basic care, including immunizations, to the civilians.Sick calls were conducted at various orphanages and courses in child care weregiven to the natives. Vietnamese nationals were hired as nurses' aides and weregiven intensive on-the-job training in English and basic nursing procedures.Nurses taught in Vietnamese Armed Forces hospitals, and USMACV nurses helped theVietnamese Army train its own nurses.
Dental Service
Background
The Vietnam conflict generated new approaches for conducting warfare whichextended to all phases of combat, combat support, and combat service supportactivities. In the latter area, changes in US, Army military dentistry rangedfrom those caused by the Vietnamese environment to others adaptable to anycombat environment.
Treatment problems of the Dental Corps differ from those faced by otherspecialty services of the Army Medical Department, whose programs and policiesare designed to cope with acute, episodic diseases and injuries. Generally,persons entering active duty are healthy young people. However, from theperspective of the Dental Corps, many of these individuals are already afflictedwith chronic oral diseases. Since early in World War II, when dental standardsfor entry on active duty were all but eliminated, the Army has inherited fromcivilian life vast accumulated needs for dental care. The result was that theArmy had too few dentists to remedy the results of years of neglect.
From a military perspective, the major effect of oral disease occurs when anacute, painful lesion develops. A soldier with a toothache is not a casualty inthe same sense as one with a combat wound. However, if he must be absent forseveral days for emergency dental treatment, this absence is just as much adrain on the fighting force as is any other disability. To improve the oralhealth status of the military population during times of hostilities, the dentalservice designed programs not only to treat but also to prevent such dentalemergencies.
The goal of the program during World War II and the Korean War was to treatall dental problems before the soldiers left CONUS for overseas assignments.Much of the needed treatment was accomplished, but over-all results wereunsatisfactory because there were not enough dentists to perform all thenecessary work, because training schedules interfered with treatment, andbecause new and more effective controls were needed.
In the early period of American involvement in Vietnam, dental preparation ofmen for duty was similar to that used in previous years. As long as the numberof men involved was small, complete corrective care for all on a one-time basiswas possible. But when troop strength started escalating in 1965, dentalproblems in preparing soldiers for
147
combat duty also escalated. In response, new approaches were developed tosupport the combat missions.
Mission Concept
The major development in the concept of mission support of combat arms wasthe Dental Effectiveness Program. This development began after Major GeneralRobert B. Shira, chief of the Dental Corps, visited Vietnam in the spring of1968. He was disturbed by reports from field commanders that combateffectiveness was being disrupted by dental emergencies which incapacitated keymen for as long as 7 days. General Shira's onsite evaluation resulted in theauthorization of a 20-percent increase in dental officer strength to 278officers in-country by June 1968, in the promotion of programs of massapplication of preventive agents, and in the appointment of a task force tocollect data on types and treatments of dental emergencies.
Preventive services, an added step in dental service activities since theKorean War, were limited because professional personnel had to perform theservices. In the fall of 1968, a stannous fluoride phosphate paste, which thepatient could apply himself, was developed. Semiannual applications of thispaste reduced the incidence of new caries from as much as 60 percent.
The task force recommended that a dental combat effectiveness program beestablished at all CONUS posts conducting advanced individual training. Theobjectives of the program were to select individuals with critical militaryoccupational specialties, identifying their dental needs and treating them withthe least possible interference to combat training, and to develop anintermediate restorative material for fast effective scaling of deep caries.
The survey of dental emergencies disclosed an annual rate exceeding 142 per1,000 men, which corroborated the field commanders' impressions. Since aboutthree-fourths of the emergencies were caused by advanced caries, treatment wascentered on caries likely to need attention within 12 to 18 months.
Two additional phases of dental care were started in Vietnam: in replacementcenters of combat units, dental screening became part of the in-processing; andany previously overlooked dental conditions were treated immediately. In thefield, dental forward area support teams provided both screening and neededdental care.
Within 9 months after the program began, the annual dental emergency rate hadbeen reduced to 73 per 1,000 men, or by about 50 percent.
148
Dental clinic of the 85th Evacuation Hospitalin Vietnam
{kind=link}
Distribution of Personnel
A new concept in the Vietnam conflict was the provision of most dentalservices through cellular dental units, not organic to the combat division butserving in an area support role. Team KJ, Dental Service Detachment, the firstsuch unit, was made up of 15 dental officers, an administrative officer (MedicalService Corps), and 21 enlisted men; this team provided routine dental care. Thefour dental officers still assigned to the medical battalion of each division(compared to the previous 15) treated emergency conditions. Medical units, suchas hospitals and dispensaries, also had organic dental officers: officersassigned to hospitals treated the hospital staff; those assigned to dispensariestreated individuals located in their immediate area.
Command and Control
At the beginning of 1965, the seven dental officers in Vietnam were assignedto the 36th Medical Detachment (KJ). Lieutenant Colonel George F. Mayer, DC, wascommanding officer of the 36th; he was also dental surgeon to the 1st LogisticalCommand. In July 1965, the 36th was assigned officially to the 1st LogisticalCommand, as were other KJ
149
teams when they arrived in-country. In December 1965, the 932d MedicalDetachment (AI) assumed command over KJ teams and dental personnel organic toother medical units.
Concurrently with the arrival of the 932d in Vietnam, the position of dentalsurgeon was created in the Office of the Surgeon, USARV. Colonel Ralph B.Snead, DC, was assigned to this position and was also to supervise dentalpersonnel assigned to combat divisions.
No further changes in command and control setup occurred until October 1967,when Colonel Jack P. Pollock, DC, was assigned additional duty as 44th MedicalBrigade dental surgeon and technical supervisor over dental personnel in medicalunits as well as divisions.
Early in 1970, the USARV surgeon's office and the 44th Medical Brigade werecombined to form the Medical Command, USARV. At this time, the positionspreviously listed as USARV dental surgeon, 44th Medical Brigade dental surgeon,and commanding officer of the 932d Medical Detachment were combined tointegrate more effectively the efforts of dental personnel in KJ teams withthose in nondental units.
Equipment
Among the improvements in field dental equipment were the lightweightautomatic dental film processor, portable ultrasonic prophylaxis, field dentalequipment set for the hygienist, more powerful air compressor, water-jetdevices, and lighter and more compact field dental sets. The superior Encoreportable speed dental engine was issued to more units; the power difficultiescreated by this engine were finally solved with the availability of additionalelectric power.
Dental treatment clinics were widely dispersed and ranged in size from onechair to 14 chairs; almost half of the clinics were air conditioned. They werelocated in tents, tropical shelters, wooden frame or concrete buildings,warehouses, quonset huts, bunkers, and mobile vans. The initial airmobile dentalclinic, used by the 39th Medical Detachment (KJ) in the Pleiku area andtransported by a Flying Crane helicopter, was an immediate success.
Automated records reduced the work required to maintain and gather data.
Oral Surgery
For the first time in U.S. military history, the Army Dental Corps hadavailable both a large cadre of trained oral surgeons to provide skilledspecialized surgical support, and helicopter ambulances to provide evacuationfor early definitive treatment of maxillofacial injuries. New and importantresearch contributions of the Army Institute of Dental Research to oral surgeryincluded an improved type of surgical
150
dressing, pulsating water-jet devices for lavage, a cold curing resinmaterial for rapid splinting of jaw fractures, preformed silicone mandibles, andan intermediate restorative material and the ultrasonic Cavitron for peridontaldisease.
Veterinary Service
The U.S. Army Veterinary Corps shares in the responsibility of safeguardingthe health of the Army. In South Vietnam, during 1965-70, the Veterinary Corpsperformed its traditional activities under conditions which were often unlikeany previously encountered by American troops. It also participated in civicaction programs, and furnished advisory support to the ARVN veterinary servicein an effort to improve its animal care and veterinary personnel training.Above all, however, the Veterinary Corps, in its food inspection activities andanimal medicine care, met a variety of challenges and resolved difficult andcomplex problems posed by conditions peculiar to the Vietnamese conflict.
Food Inspection
Veterinary food inspection in Vietnam encompassed a variety of activities.The objective of these activities was to protect the health of the soldier. Toachieve that objective, veterinary food inspectors carried on surveillanceinspection of depot food stocks, receipt inspection of foods delivered to portfacilities, and procurement inspection of indigenous ice, bread, and freshfruits and vegetables.
Initially, all veterinary activities were carried out by the 4th MedicalDetachment in Saigon. With the increase in U.S. troop strength in 1965,additional depots and ports were established throughout Vietnam, from Da Nang inthe north to Vinh Long in the Delta. Only one or two food inspectors from the4th Medical Detachment were permanently assigned to the larger of the newdepots, such as that at Cam Ranh Bay, with mobile teams organized for dispatchto the smaller ones to resolve special problems. Thus, veterinary foodinspection was concentrated on those major food depots which received fooddirectly from refrigerated ships or by secondary LST shipment. Finally, in 1968,a sufficient number of veterinary food inspectors were authorized to permittotal coverage for each food distribution activity.
Depot stocks. Although veterinary inspectors were primarily concernedwith protecting the health of troops by preventing the consumption of unsafefoods, they were also interested in food conservation.
As more refrigerated storage facilities became available, it was possible toreplace the field ration diet with one which included more dairy products aswell as fresh and frozen foods. The refrigerated storage
151
facilities available for such foods ranged from a few cold-storage warehousesremaining from French colonial days, to the self-contained, portable, walk-inboxes which became a part of each food distribution point, and to refrigeratedNavy barges anchored offshore. Despite this variety, refrigerated storage wasseldom of adequate capacity or temperature, and never caught up with demand.Lack of refrigerated storage frequently caused significant losses. To keep suchlosses to a minimum, produce on the verge of spoiling was inspected daily todetermine which items to salvage and which to condemn, including items thatwould spoil if shipped.
Losses also occurred because depots and supply points bulged with stocks farin excess of amounts that could be consumed before deterioration. Nonperishableswere stored in the open, canned goods corroded, and flour soured. With thesestockpiles far greater than requirements, depot personnel were indifferent towaste. The saving factor in this subsistence supply chaos was simply theoverabundance of foods which continued to flow into the country.
To bring some order out of this chaos, the 1st Logistical Command, in 1967,directed the Veterinary Corps to inspect nonperishable food stocks every 60days. Although the Veterinary Corps favored regular, routine checks, such aworkload was too great for the food inspection forces available. Surveillanceinspection continued to be limited to "spot check" at irregularintervals.
Indigenous food. The purchase of indigenous foods soared after theactivation of the U.S. Army Procurement Agency in May 1965. By the fall of 1966,more than $900,000 worth of produce was being purchased monthly. The amount oflocally produced foods examined by veterinary inspectors rose from 50 millionpounds in 1965 to 430 million in 1966. (Table 10) By 1967, 39 Vietnamesestores and plants had been approved as a source for the purchase of commodities,ranging from baked goods to ice.
Representatives of the Veterinary Corps and the Army Procurement Agencyworked together to develop standards to govern the production of locally grownfruits and vegetables and the preparation of bread and ice. Though not as highin Vietnam as in the United States, the sanitary standards were as realistic aspossible. The yardstick was: Does it endanger the health of the soldier? Themanner in which the sanitary standards of the two cultures were reconciled isperhaps best illustrated in regulations governing the production of ice.
Ice was in enormous demand because of the hot, muggy climate. If ice from anapproved source was not available, the soldier purchased it from the nearestVietnamese vendor, even when it was yellow with sediment and made from waterpumped from a drainage ditch. There
152
TABLE 10.-INSPECTION OF FOOD BY THE U.S. ARMY VETERINARYSERVICE IN VIETNAM, BY YEAR, 1965-70
Year | Grand total | Procurement inspections | Surveillance inspection | ||
Passed | Rejected | Passed | Rejected1 | ||
(Pounds) | (Pounds) | (Pounds) | (Pounds) | (Pounds) | |
| 1965 | 1,180,257,008 | 50,371,193 | 185,413 | 1,128,915,986 | 784,416 |
| 1966 | 8,977,251,632 | 451,415,274 | 647,125 | 8,515,523,924 | 9,665,309 |
| 1967 | 13,506,313,375 | 1,009,590,408 | 11,892,306 | 12,449,488,510 | 35,342,151 |
| 1968 | 10,162,947,762 | 1,480,914,582 | 8,226,612 | 8,621,357,986 | 52,448,582 |
| 1969 | 7,171,058,733 | 898,613,272 | 7,829,909 | 6,238,029,734 | 26,585,818 |
| 19702 | 3,667,790,436 | 549,214,720 | 1,111,051 | 3,112,474,068 | 4,990,597 |
1Quantities shown represent condemnation ofGovernment-owned foods.
2January-June only.
Source: Veterinary Activities Reports, 1965-70.
153
was evidence that contaminated ice contributed to an outbreak of viralhepatitis and that it posed a significant health hazard. To solve this problem,the Army approved purchase from Vietnamese icemaking plants which chlorinatedthe water to have at least 5.0 parts per million free available chlorine. Also,because attempts to sell nonpotable ice continued, all iceblocks were testedupon delivery.
Inspection of Vietnamese bakeries posed another problem. Since baking wasdone at night, observation during production was unsafe, even in Saigon.(Vietnamese managers claimed that Vietcong "tax collectors" chose thehours of darkness to make their rounds.) The alternative was to section samplesof bread and rolls upon receipt, and examine them for insects, other extraneousmatter, and "ropey dough" caused by bacterial contamination duringprocessing of the dough. The organism involved, although nonpathogenic, causedbread to sour within 36 hours, which was often less than the time needed todistribute the bread to units. Contaminated bakeries were suspended untilcleanup procedures had eliminated the problem and the bread kept for 96 hoursat ambient temperatures.
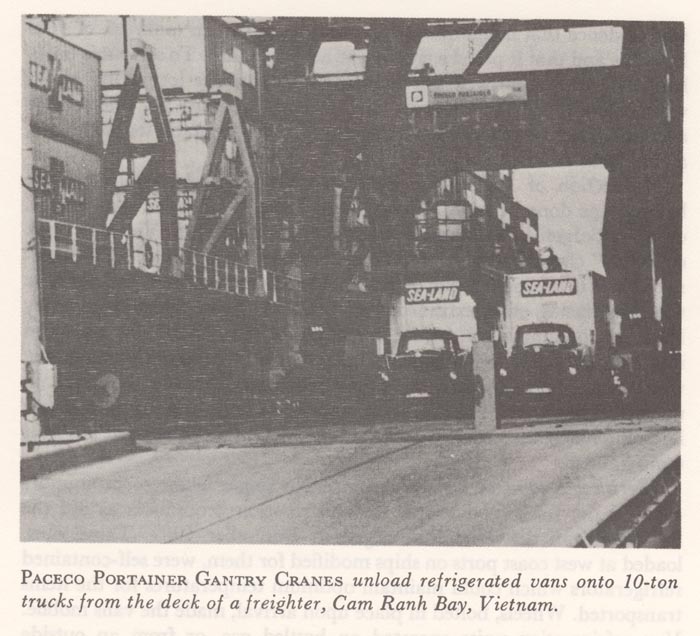
Perishable food at resupply points. No single factor so profoundlyaffected the fresh food supply and distribution procedures as did the Sea-Landvan deliveries that began in December 1967. These vans, loaded at west coastports on ships modified for them, were self-contained refrigerators which couldmaintain optimum temperatures for the items transported. Wheels, bolted in placeupon arrival, made the vans mobile. Van refrigeration units operated on bottledgas, or from an outside source of electric power. The advantages of the vans wereobvious: better temperature control, less handling of product, and fasterloading and off-loading, with issue made directly from vans to ration trucks.This revolutionary procedure made possible volume delivery of such highlyperishable items as lettuce, pears, tomatoes, and melons.
Food inspectors made daily checks of the vans parked in Sea-Land yards,recording temperatures and noting product condition. This information, suppliedto the 1st Logistical Command, permitted immediate response and centralizedcontrol of perishable items. In addition, veterinary out-turn reports forwardeddirectly to CONUS provided procuring activities with feedback data. As roadsecurity improved, vans made direct delivery to the supply points of all but themore remote combat units.
With increased utilization of Sea-Land vans and the advent of palletizedshipping containers, the veterinary food inspection specialists authorized forTransportation Terminal Commands in Vietnam could not be fully utilized at theports, for to dismantle palletized and weatherproofed packaged items at docksidewould compromise the protection
154
{kind=link}
provided against the elements and against pilferage. Furthermore, becauseport operations were either "feast or famine," food inspectionresources could be better utilized in nearby depots. Accordingly, an informalagreement was made with Transportation Terminal commanders, making foodinspection personnel organic to these commands available to the major veterinaryfood inspection unit in that area. This move materially aided the over-allinspection effort.
Animal Medicine
Routine care. Initially, in 1965, routine professional veterinary carefor military dogs in Vietnam was provided by three small veterinary foodinspection detachments then in-country. Each of these units was authorized oneveterinary animal specialist, in addition to its food inspection specialists. Atthat time, approximately 350 Army and Marine Corps sentry dogs were assigned tosome 10 locations throughout the country.
With the buildup of U.S. forces and the accompanying increased use of dogs infield operations, the dog population rose from the 350 in 1965, to more than1,200 in 1968, dispersed widely throughout Vietnam.
155
With more veterinary support required in the forward areas, additionalveterinary detachments arrived in Vietnam, but without a comparable increase inthe numbers of animal specialists. Veterinary food inspectors from the forwarddetachments were used to augment the small number of these specialists.Utilizing the services of these additional veterinary enlisted men was, atfirst, hampered by their inexperience in animal medicine and by the lack ofveterinary medical equipment sets in the food inspection units. This situationwas remedied by training food inspectors locally in certain animal specialistskills, and by obtaining equipment from the veterinary hospital and dispensarydetachments.
The need for fewer food inspectors and for more animal specialists and animalmedical equipment sets in Vietnam constituted a significant change in theoperation of veterinary service detachments. To reflect this need, appropriatechanges were subsequently made in the veterinary service tables of organizationand equipment.
Hospitalization and evacuation. The 4th Medical Detachment maintaineda small-animal clinic in Saigon for the emergency care and treatment of militarydogs and for mascots and animals privately owned by U.S. Army troops and otherauthorized personnel. All animals requiring extensive treatment were evacuatedto Saigon, except Marine Corps dogs which were evacuated to Da Nang.
In January 1966, the 936th Veterinary Detachment (ID), a veterinarysmall-animal hospital, arrived at the Tan Son Nhut Airbase to provide definitivemedical care and hospitalization for all military dogs in the II, III, and IVCTZ. Additionally, it provided a consultation service to the field, monitoringall dog medical records, requisitioning and issuing all veterinary drugs to areaveterinarians, and collecting and evaluating veterinary military dog statistics.On 19 October 1966, a small-animal dispensary detachment, the 504th MedicalDetachment (IE), arrived in Da Nang. Although organized as a dispensary, thisunit provided complete veterinary service for scout and sentry dogs in theentire I CTZ. In 1966, also, the veterinary department of the 9th MedicalLaboratory became operational, making available comprehensive veterinarylaboratory diagnostic services and investigations of animal diseases of militaryand economic interest.
In 1968, with the arrival of additional small-animal dispensary detachments,the three echelons of veterinary care and treatment of military dogs-unit,dispensary, and hospital-became clearly established. Particular emphasis wasplaced on improving administrative procedures to provide more definitive data onthe health of military dogs. An expanded monthly morbidity and mortalityreporting system was developed, and
156
completion of detailed admission reports for hospitalized dogs was stressed.
Deployment of scout dogs in 1966 resulted in casualties suffered in action.To insure prompt treatment, dogs were evacuated by air to the 936th VeterinaryDetachment (ID). Handlers were evacuated with their dogs, and remained with themuntil treatment was completed.
During 1969, difficulties were encountered in evacuating military dogs fromdog units and veterinary dispensaries to veterinary hospital facilities.Accordingly, a firm evacuation policy was established. All dogs requiringtreatment for more than 7 days were evacuated. In addition, a veterinarymedical regulator was designated to direct the flow of dogs to the hospitalfacilities. Evacuation of military dogs was co-ordinated with the Air Force andwith medical units utilizing ground and air ambulances.
In 1969, also, the high incidence and prolonged course of Tropical CaninePancytopenia left some military dog units unable to perform adequately. Theremedy was establishment of dog-holding detachments at the two veterinaryhospitals. Dogs to be hospitalized for 15 days or longer were transferred to the dog-holding detachment, thereby enabling the dog unit to requisitionreplacement dogs.
Medical problems. Canine disabilities most frequently seen, inaddition to wounds from hostile action, were heat exhaustion, ectoparasites andendoparasites, myiasis, nasal leeches, and dermatoses of varying etiology.Heartworms posed a potentially severe canine disease problem. Cases ofmicrofilaria were as high as 40 percent in some scout dog platoons, although fewanimals exhibited clinical signs of disease. The incidence of hookworms wascomparable to that of heartworms, and was frequently manifested by clinicalsigns. Outbreaks of disease resembling leptospirosis occurred; one incidentinvolved 55 dogs, but laboratory examinations did not confirm the clinicaldiagnosis. Ticks, a persistent problem throughout Vietnam, required equallypersistent control measures.
Tropical Canine Pancytopenia, an unusual disease characterized byhemorrhage, severe emaciation, pancytopenia, and high mortality, broke out in1968, in U.S. military dogs in Vietnam. Know first as IHS (IdiopathicHemorrhagic Syndrome) and ultimately as TCP (Tropical Canine Pancytopenia), thedisease seriously jeopardized the operational efficiency of combat unitsdependent on military dogs. Between July 1968 and December 1970, about 220 U.S.military dogs, primarily German Shepherds, died of the disease, and it was thecontributing reason for the euthanasia of many others. Near the end of 1969, aprogram of tetra-
157
cycline and supportive therapy for 14 days, based on recommendations from theWRAIR laboratories in Saigon, was initiated for all TCP cases. This therapyreturned to duty approximately 50 percent of the dogs treated for the disease.
Beginning in May 1969, "red tongue," a nonfatal, nonsuppurativeglossitis, occurred in a significant number of military dogs. The glossitis wasoften accompanied by excessive salivation, gingivitis and edema of the gums,and, at times, a serious conjunctivitis. The condition is extremely painful, andaffected dogs could eat and drink only with difficulty. In most instances, thesigns regressed and the dogs returned to normal in 3 to 7 days. The etiology ofthe condition has not been established.
Acute glossitis in scout dogs spread throughout Vietnam during 1970.Morbidity rates as high as 100 percent in some platoons made these unitsnoneffective for periods up to 2 weeks.
Up to 1966, the Army veterinary rabies control program was primarilyrestricted to vaccination of military dogs, pets, and mascots. In August of thatyear a co-ordinated rabies program was put in operation. Vaccination clinicswere held, often as far forward as medical clearing stations. Three majordifficulties were recognized: the enormous number of pets acquired by Americans,the large number of small units throughout the country, and the absence ofmeaningful civilian rabies control programs.
In September 1967, standard procedures were established for the control ofpets and the program was widely publicized by radio and television, stressingthe dangers of rabies. More than 7,000 animal vaccinations were reported for1967, the majority being rabies immunizations. Nevertheless, in that year onlyhalf of the animals owned by U.S. soldiers were vaccinated. The significantproblem here was that many men were located in small detachments scattered amongthe Vietnamese communities, where pet control was essentially nonexistent. Onecountermeasure was to vaccinate Vietnamese dogs around U.S. militaryinstallations, thereby lessening the chance of dogs on these bases coming intocontact with rabid animals. Where possible, dogs were vaccinated on Vietnamesemilitary installations. Also, with the requirement that soldiers pay for havingtheir pets vaccinated, many were reluctant to immunize or identify theiranimals.
The Vietnam experience showed the need for free rabies vaccinations foranimals privately owned by U.S. personnel, to assure an unhampered,comprehensive disease control program. Toward this end, with the existing activecombat conditions in Vietnam, the Army waived the provisions of the regulationwhich required payment to the Government for immunization and quarantine of suchprivately owned animals.
158
Army Medical Specialist Corps Services
Three AMSC (Army Medical Specialist Corps) officers (two dietitians and onephysical therapist) were assigned to Vietnam in the spring of 1966. There was noauthorization for these officers in existing TOE's (tables of organization andequipment) for field and evacuation hospitals, but because hospitals in Vietnamoperated as fixed installations, providing essentially the same services asstation and general hospitals in the continental United States, the need fordietitians and physical therapists was recognized. The relatively short periodsfor which patients were hospitalized in Vietnam precluded the long-rangerehabilitation programs provided by occupational therapists; however,occupational therapy was used extensively in caring for patients evacuated toJapan. During the buildup of medical support in Vietnam in fiscal year 1966, 30AMSC officers-13 dietitians, 10 physical therapists, and seven occupationaltherapists-were assigned to hospitals in Japan.
The two dietitians assigned to Vietnam in 1966 acted as consultants tohospitals in establishing food service programs. Major (later LieutenantColonel) Patricia Accountius, dietitian, was originally assigned to the 3d FieldHospital in Saigon, but was soon given the additional post of dietary consultantfor the 44th Medical Brigade, 1st Logistical Command. Captain James Stuhmullerwas assigned at the medical group level. Major (later Lieutenant Colonel)Barbara Gray, physical therapist, was assigned to the 17th Field Hospital,Saigon, but also acted as consultant to hospitals throughout the command.Because of the contributions made by these officers to the improvement ofhospital food service and to the in-country rehabilitation of patients, requests were received for the assignment of additional AMSC personnel.
In the spring of 1967, four dietitians and 10 physical therapists wereassigned. The senior dietitian continued to act as dietary consultant to the44th Medical Brigade and dietitians were assigned to headquarters staff ofmedical groups. Physical therapists were utilized in evacuation and fieldhospitals, with the senior therapist having the additional duty as consultant atthe brigade level.
The utilization of physical therapists remained essentially unchanged. InAugust 1967, the dietary staff adviser of the 44th Medical Brigade was given theadditional duty as consultant to the USARV surgeon. With the formation ofUSAMEDCOMV (Provisional) in March 1970, the dietary staff adviser was assignedto the office of the USARV surgeon. Another major organizational changeaffecting dietitians occurred in July 1968, when food service sections were madeseparate elements within each medical group headquarters. Staff dietitians,designated as primary staff officers, food service warrant officers (foodadvisers) and hospital food service noncommissioned officers (food servicesupervisors) con-
159
stituted the section staffs. Concurrent transfer of all food servicefunctions and personnel from the S-4 Section to the newly created food servicesection increased the effectiveness of dietitians as consultants at the grouplevel. The maximum authorization for AMSC officers in Vietnam was 17, whichincluded 12 physical therapists and five dietitians. The largest number of AMSCofficers serving in Vietnam at any given time was 21.
Dietitians
Because a shortage of dietitians precluded their assignment at the hospitallevel, the concept of the group or "shared" dietitian provided thebest utilization of these specialists. Dietetic supervision of several hospitalswas easily accomplished because of the proximity of hospitals within each groupand the availability of air travel. The use of the Army Master Cycle Menu (FieldRation Menu) in all medical facilities, coupled with the necessity forcentralizing food requirements for modified diet food items to assure logisticalsupport, lent itself to the concept of centralized planning and control.
A major accomplishment of dietitians in Vietnam was in menu planning and theprocurement of adequate subsistence supplies for hospitals. At the request ofthe 1st Logistical Command and in co-operation with the Defense Supply Agency,the 44th Medical Brigade dietitian, in 1966 developed a 28-day cycle master menuwhich was used by both field and hospital messes in Vietnam. A hospital mastermenu was also developed which provided meal plans for the approximately 14 typesof modified diets commonly served in hospitals. These menus were updated as awider variety of food and equipment became available. With the excellent supportof the subsistence section of the 1st Logistical Command, early problems inavailability of subsistence items were largely resolved, and hospitals weregiven first priority for food issues when shortages did occur.
Staff dietitians reviewed, analyzed, and evaluated space design and layoutsto upgrade medical food service facilities. By personal visits to varioussupply depots, they were able to locate and arrange for delivery ofgarrison-type mess equipment to hospital messes. By the end of 1968, TOE foodservice equipment in all hospitals within the 44th Medical Brigade, with theexception of the I Corps Tactical Zone, had been replaced by garrison-typeequipment.
Improvements in assigning, utilizing, and training enlisted men and civiliansresulted in high-quality food service to hospitalized patients. Originally,hospital tables of organization and equipment did not authorize hospital foodservice enlisted personnel (MOS 94F40 and 94B30), and as a result, many militarycooks and mess stewards assigned to hospitals were without previous experiencein this specialized type of feeding. Many food service warrant officers (MOS941A), who were
160
directly in charge of food service at individual medical facilities, alsolacked experience in this type of food service. Conversely, hospital-trainedfood service personnel were often assigned to troop-feeding facilities. Throughpersonal screening of food service personnel arriving in-country, this situationwas partially alleviated, and in 1967, modified tables of organization andequipment reflected the need for hospital-trained enlisted men in food servicesections. The accomplishments of many of these men in upgrading the quality offood service to patients deserve special recognition.
Food service to bed patients remained a problem. Electric carts used todeliver bulk food to the wards were not suitable for use in hospitals which didnot have covered ramps and cement walkways. Many hospitals continued to useinsulated containers to hand-carry food to ward areas. There was no provision intables of organization and equipment for ward tray service attendants, andovertaxed nursing staffs often had the responsibility for assembling trays onwards and delivering food to patients. In 1969, authorization was received toemploy Vietnamese for this purpose.
Dietitians provided assistance to Allied personnel serving in Vietnam. TheUSARV dietary consultant, working with the 1st Logistical Command II Field Forcefood service consultant and the G-4 of the Royal Thai Army Volunteer Forces,developed a more acceptable ration for the Thai Army and assisted in trainingprograms for Thai food service personnel. At the request of the U.S. ArmyEngineer Command, Vietnam, dietitians assisted Free World forces from Korea andAustralia with their cantonment mess programs in procuring equipment and intraining personnel in the use of the equipment in food preparation.
Physical Therapists
The work performed by the first physical therapist assigned to Vietnam in1966 demonstrated the value of this type of treatment for certain injuries,particularly soft-tissue injuries to extremities. The need for additionalphysical therapists was evident from the many requests for their services fromphysicians throughout the country. After evaluation of the numbers and types ofpatients who could benefit from physical therapy in USARV medical facilities,the decision was made in 1967 to assign physical therapists to field andevacuation hospitals and to the 6th Convalescent Center. The senior therapist,in her capacity as Brigade consultant, had the responsibility for constantlyassessing facilities and workloads and for assigning incoming officers andenlisted men to hospitals most in need of their services.
Malassignments often occurred with physical therapy specialists (MOS 91J20).Since no authorizations existed, trained specialists arriv-
161
ing in-country were often assigned in their secondary military occupationalspecialty. Until this deficiency was corrected, records of incoming personnelwere carefully screened and qualified individuals were diverted to medicalfacilities where their specialized training and experience could be betterutilized.
The primary treatment goal of physical therapy was the rehabilitation ofpatients who were capable of being returned to duty. For patients requiringevacuation, treatment was aimed toward starting basic rehabilitation procedureswhich could be continued throughout the evacuation process. Because of therelatively short periods of hospitalization of patients in Vietnam, physicaltherapy during the initial years was largely limited to ward-treatmentprograms, although a number of outpatients were treated in some hospitals.Because commanding officers were so pleased to have the services of physicaltherapists, they were most co-operative in providing space for clinics andhelping to procure equipment. As facilities and equipment were improved, thetypes of treatment available in physical therapy clinics were also expanded.More long-term treatment programs, particularly for Vietnamese patients, wereinitiated, and a great deal of emphasis was placed on training Vietnamesetechnicians in physical therapy techniques and procedures. Physical therapistsvolunteered their services to civilian hospitals and rehabilitation centers toassist in treatment of civilian casualties. In May 1970, at the request of theU.S. Military Assistance Command, Vietnam, a physical therapist was assigned tothat command to participate in rehabilitation programs being established in ARVNhospitals. Her primary responsibility was training Vietnamese to conduct theseprograms.