



CHAPTER XIII
Medical Assistance to Vietnamese Civilians
U.S. civilian medical aid programs began in the early years of support inVietnam. As the U.S. military commitment grew throughout the 1960's, new andexpanded programs were developed. Through such efforts as PHAP (ProvincialHealth Assistance Program), MILPHAP (Military Provincial Health AssistanceProgram), MEDCAP (Medical Civic Action Program), and CWCP (Civilian War CasualtyProgram), medical aid in increasing amounts and effectiveness was given to thepeople of Vietnam.
Provincial Health Assistance Program
The Agency for International Development initiated a program in the early1960's to supplement the health services of the Vietnamese. A major objective ofPHAP was to improve the training of Vietnamese physicians, nurses, and medicaltechnicians. Others were to expand and improve Vietnamese hospitals anddispensaries and to eradicate malaria.
Under the auspices of AID, surgical teams of U.S. civilian physicians,nurses, and technicians were sent to Vietnamese provincial hospitals. The firstof these teams arrived at the provincial hospital in Can Tho in the summer of1962; shortly thereafter, teams were assigned to the hospitals at Nha Trang andDa Nang. Surgical units, consisting of two operating rooms, a central supplyarea, and a four-bed recovery ward, were constructed adjacent to the provincialhospital where the team was assigned.
Despite the valiant efforts of the U.S. teams, augmented by those from NewZealand, South Korea, the Philippines, and other nations of the Free World, thebroad and ambitious aims of PHAP could not be realized. The task ofsubstantially improving health care in an underdeveloped nation was difficultenough. Compounded by civil strife and guerrilla warfare, it became impossible.
Military Provincial Health Assistance Program
The increase in military medical resources which accompanied the buildup ofU.S. combat troops in 1965 permitted an expansion of the effort to improve thehealth of Vietnamese civilians. In conjunction
163
{kind=link}
with the buildup, the Secretary of Defense directed the services to prepare aprogram to aid the civilian health effort in Vietnam. The new program, whichinitially employed Army military medical teams in direct aid to civilians, wasMILPHAP. It was developed jointly by AID and USMACV.
The first MILPHAP teams went into operation in Vietnam in November 1965. Eachteam was composed of three physicians, one medical administrative officer, and12 enlisted technicians. A MILPHAP team was assigned to a Vietnamese provincialhospital where its work was under the supervision of the provincial chief ofmedicine. By early 1966, six teams were functioning in provincial centers andthe decision was made to add 15 teams to the program. The number increased toeight Army, seven Navy, and seven Air Force MILPHAP teams by May 1968. At theend of 1970, teams were assigned to 25 of the 44 provinces.
Sent to both provincial hospitals and district dispensaries, the unitsprovided continuity in medical care at permanent civilian medical facilities. Byaugmenting or, in some cases, replacing the Vietnamese medical staff, MILPHAPteams assisted in clinical, medical, and surgical care. They provided apermanent source of support for local public health programs. With theco-operation of the chiefs of medicine in the provinces, the teams established aprogram of evacuation for patients to those Vietnamese and American medicalinstallations which had a greater capacity for extended treatment.
The MILPHAP teams were reorganized in 1969 to make them more responsive tothe requirements of the varying sizes of the medical installations to which theyare assigned. The reorganization provided more surgeons and nurses with levelsof skill appropriate to the medical facility
164
in which they served. By the end of 1970, the program supported a total of 30Vietnamese Ministry of Health hospitals, in addition to its work in district andsmaller Vietnamese medical installations.
A major objective of MILPHAP was to improve the medical skills of theVietnamese. In 1970 alone, for example, more than 700 Vietnamese nurses receivedtraining in hospitals supported by MILPHAP teams. Through this type of training,the program advanced toward its primary goal, the development of an independent,self-sustaining health service program in Vietnam.
A medical policy co-ordinating committee was established in 1965 to plan andco-ordinate the growing number of medical programs involving aid to Vietnamesecivilians. Headed jointly by the Assistant Director for Public Health, AID, andby the Surgeon, USMACV, the committee also included the surgeons of the USMACVcomponent commands. Efforts to eliminate duplication in the administration ofcivilian health programs between AID and USMACV resulted in the establishment ofjoint USMACV-AID working committees in 1968. The committees formulated jointplans for hospital construction, medical supply, medical education and training,preventive medicine, and public health. By including military and civilianVietnamese medical officials as members of the committees, policy makers laid abasis for the future assumption of responsibility for these programs by theVietnamese themselves.
Medical Civic Action Program
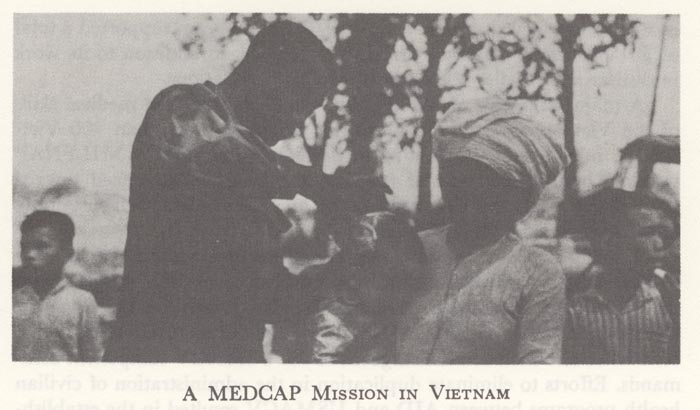
The best known of the various programs in Vietnam for medical civilassistance was MEDCAP. Developed from a joint proposal by the American Embassy,Saigon, and USMACV made in 1962, MEDCAP began operation under the auspices ofthe Department of the Army in January 1963.
The primary objective of MEDCAP was to provide increased outpatient care forVietnamese civilians living in rural areas. American and Vietnamese militarymedical personnel were used in the program, a major goal of which was toincrease mutual respect and co-operation between the military forces and thecivilian population.
Originally, medical assistance was provided by U.S. military advisory teamsand Special Forces personnel; as the program grew, regular American militaryunits participated. Initial MEDCAP organization comprised some 127 U.S. Armymedical personnel, working in three teams. Later, medical personnel came fromall the U.S. military services in Vietnam, although the Army continued toadminister the program and support it logistically.
Although some improvisation was necessary due to local needs and conditions,the MEDCAP teams normally traveled to hamlets and vil-
165
lages with their ARVN counterparts and established temporary health stations,of dispensary size, to provide medical care for the inhabitants. Through theoperation of these teams, Vietnamese medical personnel were also trained inmedical techniques.
In contrast to MILPHAP, the MEDCAP team was a mobile unit which visited avillage for a short period of time, treating civilians only on an outpatientbasis. Although each team was supervised by a medical officer, the enlistedmedical personnel provided most of the direct effort. MEDCAP can properly beregarded as complementing the more permanent operation of the MILPHAP team.While the latter might operate a surgical facility in a provincial hospital, orassist in the renovation of local medical facilities, the former team worked ona "one-day visit" basis in areas where more permanent medical aid wasimpractical.
The buildup of U.S. forces in Vietnam beginning in 1965 afforded theopportunity both to expand and to extend MEDCAP. Direct participation in theprogram by American and Free World military units of battalion size and largerbecame known as MEDCAP II; the original program which continued was then calledMEDCAP I. Even in the expanded effort, however, U.S. personnel were directed,unless it was impractical, to conduct their medical civic action effort througha member of the RVNAF medical service or the Vietnamese civilian governmentmedical authorities. MEDCAP retained the objective of eventually enabling theVietnamese to assume the complete burden of medical care for their own people.
To support the expanded effort, a new supply system was developed for MEDCAPin July 1967. Previously, medical supplies had been furnished through the RVNAFmedical depot system, but difficulties of distance and co-ordination made thismeans of supply increasingly unwieldy. Under new procedures, MEDCAP units wereauthorized to requisition material directly through the regular U.S. Army supplychannels. Supply levels were also increased in recognition of the larger numberof MEDCAP projects.
The extent of the MEDCAP program in Vietnam was remarkable. Both American andFree World forces participated in it, often on a volunteer basis. On manyoccasions, U.S. medical personnel devoted their free time to MEDCAP activities.In the later years of the program, when time and circumstances allowed, moreextensive treatment than outpatient care was given. From 1 December 1967 to 31March 1968, a monthly average of 188,441 civilians received outpatient treatmentfrom personnel of the program. A monthly average of 17,686 Vietnamese wereimmunized in the same period. By 1970, the MEDCAP II program alone treated anaverage of 150,000 to 225,000 outpatients per month.
Both U.S. dental and veterinary military personnel participated in the MEDCAPprogram with equally gratifying results. The dental con-
166
tribution to the program is often termed "DENTCAP." An attempt toalleviate the dental defects of the Vietnamese people was made by dentalofficers and enlisted technicians. During the 1967-68 period previouslymentioned, dental treatments under the program averaged approximately 15,000 permonth.
In a country as predominantly rural and agricultural as Vietnam, veterinaryactivities were of great importance in any medical civic action program. U.S.Army veterinary personnel provided much aid in swine husbandry and animaldisease control as early as 1966. Sometimes called VETCAP, veterinaryparticipation in MEDCAP increased in the following years. Treatment of sick andwounded animals, cattle vaccination, and guidance in the care and feeding ofswine and cattle were all part of VETCAP activities. A rabies control projectwas also undertaken. During 1967 alone, a total of 21,391 animals in civiliancommunities were immunized against rabies, and 2,254 farm animals were treatedfor various diseases.
Civilian War Casualty Program
The success of MILPHAP and MEDCAP only partially met the medical needs of theVietnamese people. As the tempo of the war increased in 1967, the growingproblem of civilian war casualties called for new efforts. Estimates of 50,000such casualties a year indicated that existing Vietnamese medical resourceswould be overwhelmed in providing care for these victims.
After some discussion U.S. Government officials assigned to the Department ofDefense the mission of providing additional care for Vietnamese civiliancasualties. The U.S. Army was directed to begin a program to this end, and inApril 1967, a detailed plan drawn up by USMACV was approved by the Secretary ofDefense. The CWCP was provided with the resources necessary to constructadditional hospitals in Vietnam to care for civilian casualties.
A temporary allocation of 300 beds in U.S. Army hospitals in Vietnam wasmade, with this number increased to 400 in December 1967. Three Army hospitals,the 27th Surgical at Chu Lai, the 95th Evacuation at Da Nang, and the 29thEvacuation at Can Tho, with a total bed capacity of 1,100, were then designatedas CWCP hospitals. American military medical personnel were assigned to theprogram, and plans were made for additional hospital construction.
The original intent of CWCP was that medical installations assigned to theprogram would remain separate from the U.S. military hospital system in Vietnam.Because of the reluctance of Vietnamese civilians to leave their home areas fortreatment in distant hospitals, and because of the increase in civiliancasualties during the Tet Offensive in early 1968, the program was modified.Treatment of Vietnamese civilians in U.S.
167
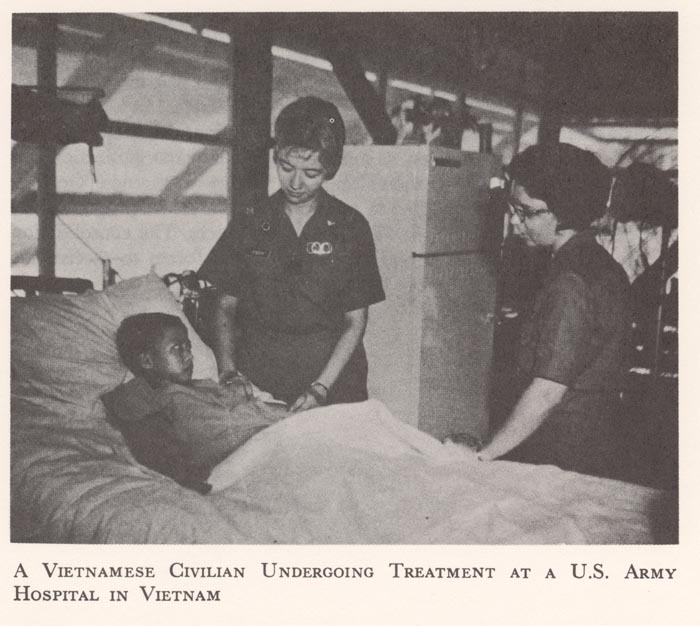
A Vietnamese Civilian Undergoing Treatment at aU.S. Army Hospital in Vietnam
{kind=link}
military hospitals had been authorized on a limited basis since the buildupof American forces and installations in the country. During the period of theTet hostilities, a civilian patient load higher than normal was assumed by allU.S. military hospitals. This system of "joint occupancy" by Americanmilitary and Vietnamese civilian patients was found to be the more practicalalternative to a separate CWCP hospital system.
Under this system, Vietnamese civilians more readily accepted extendedtreatment at a location near their home areas. Additionally, administrative andevacuation procedures were simplified under the system and constructionrequirements were lessened. Acting on the direction of the Secretary of Defense,USMACV incorporated the previously designated CWCP hospitals into the U.S.military hospital system in April 1968. Vietnamese civilian patients wereauthorized treatment at all military hospitals on a space available basis. Asthe number of American forces was reduced during 1970, a requirement to maintain600 beds in U.S. Army hospitals for CWCP was established. Provision for periodicre-evaluation of the facilities needed for the program were included in thisrequirement.
168
In late 1968, USMACV and AID jointly proposed that Vietnamese military andcivilian hospitals be merged. The proposal called for the merger of RVNAF sectorhospitals with the civilian provincial hospitals in areas where the move wouldimprove medical service. In a three-stage implementation of the plan followingits adoption, 13 hospitals were chosen for immediate merger, 12 more needingminor reorganization and rehabilitation were added thereafter, and certainVietnamese Government buildings were converted to hospital use. The entireprogram integrated the hospital systems in 26 of the 44 provinces. Theconsolidation enabled the Vietnamese people and their armed forces to receivethe maximum care available from their medical resources.