



Chapter 2
PENETRATING INJURIES OF THE THIGH WITH ASSOCIATED FEMORAL FRACTURE
Colonel William E. Burkhalter, MC, USA(Ret.)
In both World Wars, a battle-incurred compound fracture of the femur was regarded as one of the most serious skeletal injuries a soldier could sustain (Hampton 1957, 137). In World War I, 971 or (25 percent) of the 3,850 soldiers with femoral fractures and penetrating wounds of the thigh died. Fractures of the femur constituted approximately 24 percent of the 16,339 recorded World War I battlefield fractures. The mortality figures in World War II were much lower. One study indicated only 7.9 percent of all deaths were attributed to compound fractures of the lower extremity (Hampton 1957). During the Vietnam conflict fractures of the femur continued to be one of the most costly injuries sustained by the combat soldier, in terms of the length of hospitalization and residual functional impairment. Direct comparisons of the three conflicts are impossible because of changes in categories and classification systems.
The concepts and practices for treatment of combat casualties with penetrating wounds of the thigh and a fractured femur changed markedly from war to war. During World War I, splinting rather than plaster was generally emphasized, in order to maximize the desired freedom of joint movement. Infection was treated by local applications of such agents as bismuth subnitrate, iodoform, and paraffin (BIP) or by the elaborate irrigation ritual of the Carrel-Dakin method. Evaluation of the results indicated a high incidence of malunion, nonunion, and infection, as well as excessively high rates of amputation and fatality. After the war, the Carrel Dakin method fell into disuse and was replaced by the closed plaster technique, usually credited to H.Winett Orr, whereby the wound was left open to allow drainage and the limb was placed in a plaster cast with skeletal fixation of the fracture. The objective of this method was to prevent the trauma and reinfection that was so prevalent with frequent changes of dressings. It was a one-stage program for management of the combat-incurred compound fracture of the femur with associated soft tissue injuries. The first wartime test of the closed plaster technique came during the Spanish Civil War. Trueta, as cited by Hampton (Hampton 1957, 53) reported excellent results, but United States surgeons during the North African campaign found the program unworkable (Hampton 1957, 55). The theoretical benefits of the technique were negated by complications caused by moving patients from forward to rear hospitals. Patients became febrile, plaster disintegrated or proved ineffective, circulatory problems arose, transfixion pins broke, and infection set in, to name a few. By early 1944, the practice had been largely discontinued.
With the failure of the closed plaster technique, Army surgeons in the Mediterranean theater turned to the delayed primary closure of “clinically clean” wounds. The bacteriological culture reports that had been relied for twenty-five years were
22
abandoned because they required extensive laboratory assets and multiple changes of dressings. The first step in compound fracture management was now limited, for the most part, to wound exploration and debridement. At that time, care of the fractured femur was limited to correction of gross malposition and splinting for transportation. When the patient was in a fixed hospital, during the “golden period” for fracture management, usually four to seven days after wounding, he underwent a second surgical procedure. Performed under anesthesia, it involved further debridement of necrotic tissue, irrigation, fracture reduction, delayed primary closure, drainage conduits, antibiotic therapy, traction, splinting, and casting. The patient was prepared for return to the Zone of the Interior.
World War II military surgeons who treated patients with penetrating injuries to the thigh accompanied by fractured femurs expected prolonged recumbency with resultant inanition, muscle atrophy, and fibrous ankylosis of joints. Their reports (Bray and Fitts 1946; DeLorme et al.1950) indicated that the natural history of the fracture healing required twenty-four weeks before the patients could begin ambulation. Only 30 percent of these patients were expected to have ninety degrees or more of knee flexion. Soto-Hall and Horwitz (1946) reported a series of 122 fractures in which 86 percent of the fractures united, 27 percent remained infected with definite evidence of osteomyelitis, and 33 percent had limited knee extension. Five percent of these patients refractured the femurs.
PRACTICESDURING THE VIETNAM CONFLICT
The basic principles of debridement, delayed primary closure, and fracture management did not change dramatically from World War II to Vietnam. Technological advances and the availability of broad-spectrum as well as gram-negative and gram-positive specific antibiotics did little to alter the criteria and priorities for management of fractures associated with penetrating wounds of the thigh.
Femoral shaft fractures secondary to penetrating injury posed massive problems for combat surgeons. The wound took precedence over the fracture at the initial surgery. Following initial surgery, the limb was splinted to prevent further trauma to surrounding soft tissue. Only after absolute wound control did physicians become concerned about reduction of the fracture. Fracture of the femur associated with severe penetrating wounds required more than one surgical exploration and wound debridement.
Initial treatment at the hospital began with resuscitative measures and general examination carried out in the triage area. Although examination of the wound was not done in the triage area, a search was made for an exit wound (because of the possibility of an intra-abdominal course of the bullet with associated injuries in this area) and for associated vascular or nerve injuries.
With the limb splinted and resuscitation proceeding, roentgenograms were obtained in two planes. Constant monitoring of the efficacy of resuscitation and observations for signs of deterioration continued. If the patient was in severe difficulty, he was sent immediately to the operating room. If he was not, after he had received adequate blood replacement and his vital signs had been stabilized, he was sent in order of triage-determined priority. Once the patient was in the operating room, the surgeon and his team removed the splint and placed a Steinmann pin through the
23
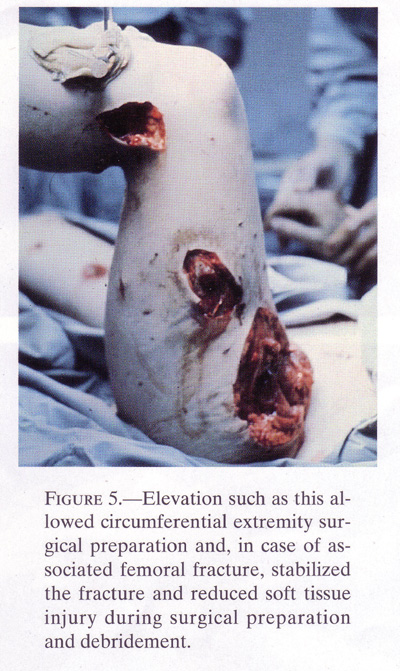
tibial tubercle. If suspensionequipment was available or could be improvised, the limb wassuspended by the pin so that both hip and knee were in 90 degrees offlexion. This allowedtraction to the femoral shaft fracture during preparation of the limb,draping of the limb, andactual surgery of exploration and debridement. The traction reducedfurther soft tissue injuryduring the usual manipulative portion of the prepping, draping, anddebridement of the thighwound (fig.5).
{kind=link}
Since excessive bleeding often occurred in patients with partially lacerated vessels when clots were disturbed, ready access to the common femoral artery could prevent considerable blood loss. Therefore, circumferential prepping and prepping of the groin were necessary for care of the wound as well as for immediate access to the common femoral artery in the event that excessive bleeding occurred during wound exploration.
Longitudinal wound extension allowed exploration of the depths of the wound and required considerable knowledge of cross-sectional anatomy. Since wound debridement was time consuming and resulted in considerable blood loss, blood for transfusions had to be available if surgeons were to perform optimal surgical exploration. At the conclusion of exploration and debridement, fine mesh gauze was applied directly to the wound, which was left open.
24
{kind=link}
25
{kind=link}
26
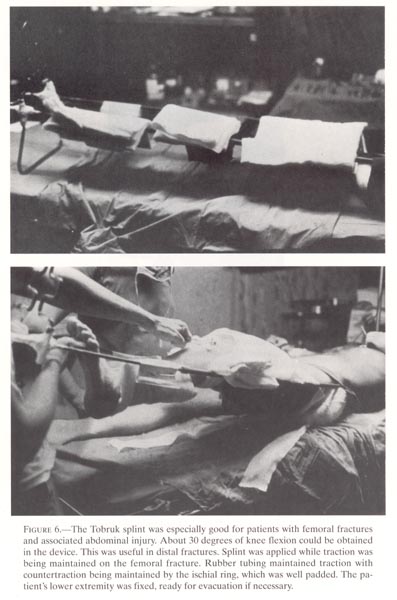
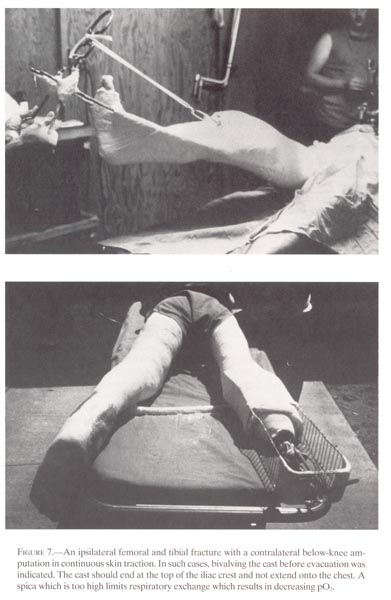
The decision about which of the two types of immobilization should be used depended on the surgeon’s assessment of the adequacy of the debridement and presence of associated injuries, the flow of patients, and the number of casualties. If the patient was not scheduled for immediate evacuation, the modified Tobruk splint with a half-ring splint, foot extension, and slings supported the extremity (fig.6). The previously placed Steinmann pin and bow were attached distally with surgical tubing to the foot extension on the half-ring splint. Dressing or plaster of Paris bandages were applied directly over the limb and leg splint for greater immobility. For early evacuation to an offshore hospital or to CONUS, the second type of immobilization, a one and one-half spica, was applied without extension onto the chest and without excessive abduction of the legs in order to limit mobility of the fracture during air evacuation. The two portions were held together with plaster bandages (fig.7).
If signs of sepsis, excessive drainage, or excessive pain at the fracture site occurred following the initial wound surgery, the patient was returned to the operating room for reexamination under anesthesia. In the highly compartmentalized thigh, more than a single operative procedure was frequently necessary to achieve a surgically clean wound, particularly after a combat injury with its associated penetrating foreign bodies.
No attempt was made to perform delayed primary closure of these wounds in hospitals in Vietnam because of the relatively high breakdown rate of wounds of the thigh treated by delayed primary closure. No closure was preferable to wound breakdown following premature closure. These wounds healed better by secondary intention or later wound excision and closure. This was true even for those patients who could not be evacuated because of associated vascular injuries or wounds to the chest or abdomen.
Vascular injuries which caused interruption in distal blood flow were the most serious trauma an extremity could receive because failure to restore distal blood flow quickly would lead to the loss of the limb (Bagg 1967). Treatment began with immediate action to control bleeding, followed by adequate wound debridement. Vascular repair to restore blood flow distally had to be accomplished as soon as possible if the extremity was to survive. Repair of vascular injuries received priority in the treatment of the injured extremity. In Vietnam, both the equipment and surgical skills were available to repair injuries to the femoral artery. The most critical factor in the success or failure to reinstitute distal blood flow was the interval of time between the injury and the reestablishment of the blood flow. The major cause of failure of the vascular repair was low-grade sepsis secondary to poor or no debridement.
When an arterial injury was associated with a fractured femur, although the orthopedic surgeon assisted the vascular surgeon, the primary concern wasthe rapid restoration of distal flow.Whileadequate wound debridement was absolutely necessary, fracturemanagement could be delayed.Internal fixation was rarely needed and indeed was consideredcontraindicated because of thetime required (CINCPAC-4.1970). Soft tissue coverage over bone orfracture site at the time ofinitial surgery was not necessary in most injuries of the thigh but,when arterial injury wasinvolved, it was necessary to obtain good soft tissue coverage over thevascular repair.
Patients who sustained a vascular injury and repair were kept in Vietnam for three weeks to allow time for the vascular repair to stabilize before the trauma of evacuation unless the military situation precluded this course of action. When the
27
patient was evacuated,he was encased in a spica cast that was usually bivalved so that thesite ofvascular repair and a point of proximal control of arterial bleedingwere both readily accessible.
The military orthopedic surgeon had to keep his priorities in order, especially in the combat zone. Reduction and fixation of the fracture, accomplished as expeditiously as possible, were performed only on those occasions when stabilization was necessary to avoid further injury to soft tissues or to prevent placing the vascular repair in jeopardy. In these situations, transfixation with Steinmann pins was usually satisfactory; intramedullary fixation was rarely the procedure of choice. The reduction of bone length could be an advantage for the vascular surgeon, but reduction and fixation of the femur before vascular repair were usually contraindicated The procedure increased the time between injury and restoration of blood flow, the time required for the first surgical exposure, and the time the surgeon was required to devote to the individual patient when numerous casualties were awaiting treatment, and, in addition, added to the risk of sepsis.
After initial surgical treatment, the patients were considered for evacuation. Adequately hydrated patients with stable vital signs and acceptable hematocrits were ready for evacuation. Most patients evacuated to offshore hospitals arrived five to eight days after injury. If possible, moving the patient in difficulty was delayed until his condition was as close to optimal as possible.
TREATMENT INJAPAN
During 1968, 1,658 patients with fractures of the femur passed through the hospitals of the United States Army Medical Command in Japan. From this group, an in-depth review of 300 cases provides a picture of the patient from wounding to ultimate disposition.
All of the patients were healthy, young, physically fit men on active duty in Vietnam during wartime. The cause of the injury to the thigh ranged from hostile action to falls (table 1). Seventy-three percent of the soldiers in the series were in the pay grades E-1 to E-4, 15 percent were noncommissioned officers, grades E-5 to E-9, and 12 percent were commissioned or warrant officers.
Thirty-one medical facilities in Vietnam sent patients to hospitals in Japan where, after several weeks of treatment (average length 18.1 days), they were sent to forty-six different CONUS medical centers. The average period of hospitalization before return to duty or separation from active duty was 300 days. Seventy percent of soldiers with combat sustained fractures of the femur were not able to return to duty and required medical separation. They averaged 418 days of hospitalization from time of injury to separation and required nearly one-half million patient days of care (1,658 X 300 = 497,400). Thus, in spite of technical improvements, the combat-incurred femoral shaft fracture remained a fracture with significant morbidity, as evidenced by the data in this chapter.
The distribution of the fractures along the shaft of the femur shows a spread of 39 percent midshaft; 37 percent distal third; 25 percent proximal third, including the intertrochanteric area and femoral neck; and 3 percent undetermined (table 2).
28
TABLE 1.- Mechanism of injury of 300patients with fractured femurs
TABLE 2.- Location and type of femoral fracture
The 34 percent of patients who incurred fractured femurs secondary to fragment wounds had the highest incidence of associated organ injuries. Ten patients (3 percent of the survey group) eventually required amputation of the extremity. Six of these were done within five days of wounding secondary to failure to restore vascularity of the extremity after a concomitant vascular injury. Three amputations, performed while the patients were hospitalized in Japan, were necessitated by non-viability of the extremity resulting from vascular injury and massive distal infection. One was performed in a CONUS hospital because of residual causalgia, chronic infection, and marginal blood flow. This case was also accompanied by a sciatic nerve injury. Twenty-seven cases (9 percent) sustained ipsilateral fractures of the tibia.
Patients received in Japan from Vietnam with penetrating injuries of the thigh had received fairly standard treatment. Surgeons had already debrided the wound, removing all nonviable tissue and fascia without debriding the bone. The wound had been thoroughly irrigated and appropriate open drainage established. Exposed bone was allowed to remain exposed. Surgeons in Vietnam did not do swinging muscle or muscle cutaneous flaps over the bone, nor did they repair nerves.
29
Some patients were evacuated to Japan in Tobruk splints, some with modified Tobruk splints and the bivalved spica. Transportation in the spica had the potential of lowering the patient’s pO2 because this cast limited the patient’s ability to breathe. Upward displacement of the diaphragm further compromised the respiratory capacity because expansion of intraviscal gas (resulting from the increase in the plane’s altitude) distended the abdomen. The adverse effects on the patient, however, proved transient. Patients usually arrived in Japan no later than five days after injury.
During the early war years, variations in treatment occurred from hospital to hospital and physician to physician in the Pacific Command. Gradually, a standard method of treating fractured femurs emerged. If the patient was fairly comfortable and medically stable, he rested for the day following his arrival while baseline values were established and he was sufficiently rehydrated Then, with the patient under sedation or anesthesia in the operating room, the spica case was removed and further debridement, if appropriate, was performed
Wound breakdown following delayed primary closure was higher in wounds of the thigh than in most other parts of the body. The high incidence of failure for delayed primary closure of these penetrating wounds of the thigh associated with fractured femurs can be explained by several factors. The wounding agent created a relatively large cavity, in which necrosis of the tissue occurred When debridement of this and of other devitalized tissue was performed, the debridement created a rather large permanent cavity that was often inadequately drained. As a result, the policy on the management of these wounds gradually changed until secondary or delayed primary closure became the exception rather than the rule. Wounds were allowed to heal by secondary intention or by wound excision and closure at a later date. In most instances, the patient treated with “no closure” had the extremity placed in balanced suspension, preferably with the tibial pin for traction, until the wound was healed. Anterior wounds required different procedures because treatment in balanced suspension required leaving the patient in a supine position. Drainage by counter incision posteriorly proved ineffective. Debridement created dead space and longitudinal traction tended to maintain it. In this case, when the dead space could not be obliterated, no closure gave better results than delayed primary or secondary closure.
Once the fractured femur was in satisfactory position and “sticky,” a spica cast was applied and the patient considered for air evacuation to a CONUS hospital. Since the four to six days the patient might be in transit and the up to two stopovers enroute, each requiring transfer from the airplane to a medical facility, were exhausting, many factors had to be considered in making the decision to evacuate. In particular, medical personnel had to consider the capability of the patient to sustain so many days in transit before arrival at his final destination, when only emergency medical care could be undertaken en route.
In the majority of patients reevaluated in CONUS, removal of the travel spica cast revealed no loss in bony alignment. Once reinstituted, balanced suspension successfully held the alignment of the femur until union occurred. Soft tissues usually healed promptly. In those cases where delayed primary closure had broken down, the wounds were allowed to heal by secondary closure after a simple redebridement.
30
TREATMENT INCONUS--AMBULATION IN THE CAST BRACE
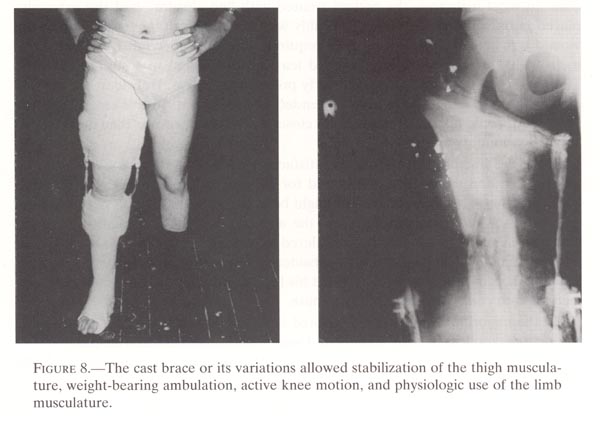
In the early years of the Vietnam War, the ambulation treatment regimen for femoral fractures sustained in combat was similar to methods of treatment during the latter part of World War II and the Korean conflict. Use of these techniques, such as traction or the ambulatory spica, did not permit physiologic compression of the fracture and ambulation did not occur until internal fixation was present. In the 1960s, a new modality, the cast brace, proved to be an effective adjunct when the patient reached the ambulatory stage. The cast brace demonstrated that awaiting internal fixation before ambulation was not necessary. This was an important development because early ambulatory status improved the patient’s well being, his appetite, and the status of his wound. It was not at all unusual to see a febrile patient with a large open wound become afebrile and his drainage become thin after a few days of ambulation. The cast brace, which allowed upright posture since the wearer was not encumbered by a bulky cast, provided a support which invited active muscle activity and easier wound drainage (Connally et al.1973; Moll 1973). The cast brace was the most significant innovation in treatment of combat-wounded patients with fractures of the femur that military medicine developed during the Vietnam era (fig.8).
Success with ambulatory management of tibial shaft fractures turned attention to the ambulatory management of patients with open comminuted femoral fractures. At the urging of Dr. Vert Mooney, Col. Charles Metz at Walter Reed embarked on early ambulation of femoral shaft fractures. The concept of early weightbearing ambulation in open comminuted femoral shaft fracture cases (Mooney et al.1970) appealed to all military surgeons. Those experienced in managing open tibial fractures were
{kind=link}
31
certain the method would be successful. Thedistal one-third of the femur could be handled easilybecause support of the bone could be achieved by controlling the softtissue at and above thefracture site. However, in the proximal injuries, the proximal fragmentwas relativelyuncontrolled and the inability to control hip abductor functionultimately resulted in a varusangulation. Brown (1971) concluded that, although application of thecast brace was critical andtime consuming, it offered many advantages. The patient’s moraleimproved, he gained weight,developed better musculature, and took an interest earlier inrehabilitation. Unfortunately,angulation up to 20 degrees could be expected in approximately 20percent of the high femoralfractures ambulated in a cast brace before there was bony stability(Brown 1971).
Of the first fifty comminuted femoral shaft fractures secondary to penetrating injuries treated with the cast brace at Fitzsimons General Hospital in Denver, Colorado, over 50 percent of the patients regained more than 90 degrees of motion (Burkhalter 1973). In a similar series at Valley Forge General Hospital, all forty-five patients in the group had over 90 degrees of motion before discharge from the hospital. The patients in both series had nonunion of the fractures only where there was extensive bone loss (Deffer et al.1971).
Bailey et al. (1976) reported a series of 156 patients with open femoral fractures treated at Fitzsimons. The patients usually arrived from the combat zone or an offshore hospital in a bivalved hip spica with a Steinmann pin in the tibial tubercle. The cast was removed and the limb was placed in balanced skeletal traction. After necessary evaluation and interim care, the patient began exercises for the quadriceps. As soon as he gained control of the leg, a cast brace was applied. The device consisted of a total contact long-leg cast with the knee in full extension. The plaster was shaped into a quadrilateral configuration at the base of the leg. Elastic plaster was used to improve the fit around the root of the leg. Roentgenograms were obtained and, if needed, wedging was placed in the cast to correct the angulation. Single axis drop-lock knee hinges were incorporated the next day. Twenty-four hours later, the patient began weightbearing ambulation with crutches. The patient performed the prescribed knee exercises from a sitting position. When enough control was achieved, the knee joint in the cast was unlocked. Position and condition of the femur were reevaluated radiographically each week for four weeks and monthly thereafter. One-third of the fractures at union had angulated. Eight had anteroposterior angulation 5 valgus and 38 varus angulation. Of the varus angulation, 24 had less than10 degrees and 14 greater than 10 degrees of angulation. In terms of motion, one month after removal of the cast brace, 93 of the 156 patients had greater than 90 degrees of motion of the knee, and 18 had between 70 and 90 degrees. Average time to union of the femur was 22.4 weeks. Two “nonunions” required bone grafts and then united with cast brace ambulation. There were three cases of established osteomyelitis.
Throughout the military, Moll (1973) probably has the earliest and most extensive experience with cast bracing in these open femoral fractures. Of 184 fractures in 178 patients at Brooke Army Medical Center, San Antonio, Texas, only 3 failed to unite. Malunion--(union with more than two centimeters of shortening and more than 10 degrees of varus or valgus angulation)--occurred in 15 cases.
Because of angulatory problems, Deffer et al. (1971) designed a mini-spica cast brace applied after the patient gained muscular control of the injured limb, and with the hip abducted and flexed to 30 degrees. Radiographs confirmed the position of the
32
fracture. If the position was notsatisfactory, it was altered, as necessary, by wedging. Knee jointswere incorporated and ambulation was instituted. The ankle was notincluded in the cast. In theinitial series of thirty-nine fractures, Deffer et al. (1971) reportedthat only one ultimately resultedin nonunion, All regained at least 90 degrees of motion at the kneejoint and none had chronicosteomyelitis. Average time to unsupported weightbearing wasapproximately twenty-threeweeks (5.7 months).
LESSONSLEARNED
Without question, the Vietnam experience showed that the loss of significant bone complicated the initial treatment and affected the end results significantly. In one study from Brooke Army Medical Center, a report on 60 patients with segmental bone loss (Moll and Willhoite 1970), only 4 demonstrated a complete segmental loss on the initial roentgenograms following injury. The remaining 56 showed the bone loss occurred at the time of initial or subsequent debridement. In all reviewed series of Vietnam casualties involving fractures of the femur, the greatest cause for nonunion was a significant loss of bone at the fracture site. This finding suggests that debridement of bone should be avoided and that every effort should be made to preclude the development of large segmental bone losses during surgical debridement.
In the presence of extensive soft tissue injury, skeletal traction, which for most patients lasted three to four weeks, caused early fibrosis of the fracture site. Furthermore, compression of the fragments did not occur with ambulation. When bone loss caused a shortening of less than two inches, controlled shortening and attempt at primary bone union were the most effective course of treatment.
During World War II, Hampton and Cleveland (Hampton 1957) advocated judicial use of internal fixation. During the Korean conflict, Brav and Jeffress (1953) and Carr and Turnipseed (1953) observed that in selective cases internal fixation may be not only beneficial towards fracture wound healing but may actually be lifesaving. In Vietnam, fixation of closed fractures was usually an elective procedure. However, it was used for open fractures, particularly as a late reconstructive measure. The advantages of the method were many. By restoring bone and joint architecture, it minimized the use of incumbering external stabilizing devices. It obliterated dead space, thereby accelerating soft tissue healing. And by minimizing the chances for displacement of bone that could injure nerves and vessels critical to the restoration of the extremity, it facilitated patient handling during transit.
With the use of the cast brace for functional treatment of femoral shaft fractures, however, union usually occurred without internal fixation, although all series of patients included a few that failed to unite with or without persistent drainage. Since Brav and Jeffress (1953), Brav (1957) and Carr and Turnipseed (1953) reported excellent results with intramedullary nailing of the delayed or nonunion without wound closure, the procedure seemed promising. In a series of 225 open femur fractures at the106th General Hospital in Japan, intramedullary nailing was performed in 5 cases through the open-wound without adverse effects.
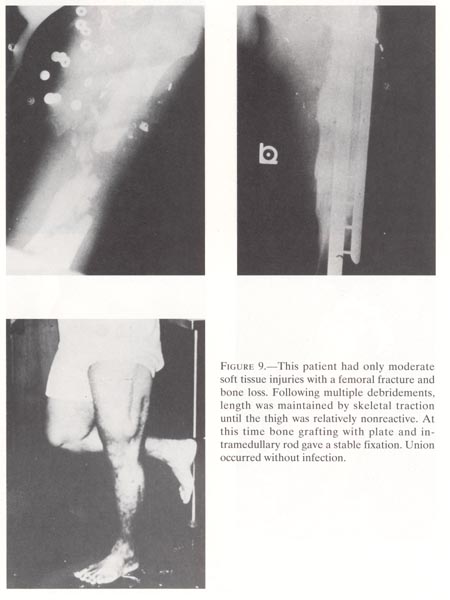
In cases of bone loss with a healed wound, internal fixation with bone grafting of cortiocancellous grafts was possible if length had been maintained in traction (fig. 9). The decision to maintain length or allow controlled shortening had to be
33
{kind=link}
34
{kind=link}
{kind=link}
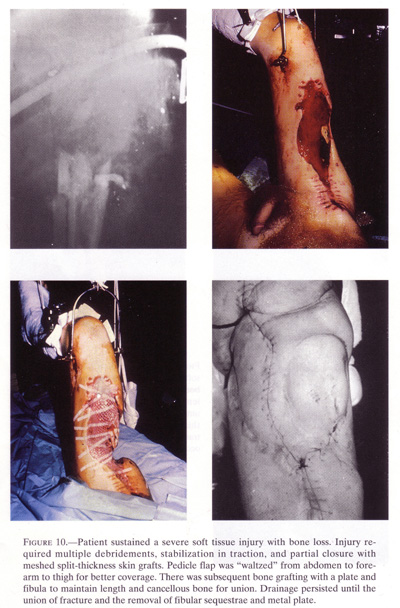
made within three to four weeks after theinjury. If delayed longer, shortening was difficult toavoid, even with ambulation. Although shortening of 2 cm. was easilyaccepted by both patientand physician, even shortening of 4 to 6 cm. was recognized andaccepted. The latter was usualin the case of some soft tissue injury or loss and in complex woundswhere there was difficultygetting wound control. In this situation, maintaining length by bonegrafting was not usuallyconsidered feasible (Moll and Willhoite 1970) (fig.10).
Althoughthe cast brace was ideally suited for the open comminuted femoral shaftfracture, angulating malunion occurred in the more proximal fractures.In this group of patients,osteotomy with internal fixation was carried out following union andrehabilitation of theextremity.
Woundswith persistent drainage or potential chronic osteomyelitis alsoconcern themilitary physician because they preclude healing. Although antibioticscertainly proved aninvaluable adjunct, they did not preclude the surgeon’s responsibilityfor distinguishing betweenlocal wound contamination, local wound infection, systemic infection,or a combination of theseconditions. Wound contamination was usually contained at the time ofdebridement withirrigation and excision of tissue, and systemic infections subsidedwith use of appropriateantibiotics. Localized wound infection usually subsided when union wasobtained.
Exceptin desperate situations, there appeared to be little need to useinternal fixation. Ifdebridement, drainage, and antibiotics did not stabilize the wound areaand the patient,intramedullary nailing of the infected femur was carried out, asadvocated by Brav and Jeffress(1953) following the Korean conflict (Brav 1957). The value of theearly ambulation following I-M nailing or use of the cast brace cannotbe overstated in hastening the healing process andreducing the number of cases of persistent drainage or osteomyelitis
36
Theorthopedic surgeon had to be constantly aware of the problems thatcould follow avascular repair. Massive swelling of the calf with the requirement forfasciotomy had to beconsidered. Thrombosis was possible any time during the first twoweeks. Disruption at the siteof anastomosis was also possible and was usually secondary to infectionbecause of inadequatedebridement. The nursing staff needed standard operating procedures foraction if disruption ofarterial repair occurred. All treatment relating to the fractured femurhad to be supported by theprogram which gave the best assurance of a successful and lastingvascular repair. At all times,the medical personnel needed easy access both to the site of vascularrepair and to an area ofproximal digital control.
Duringthe course of initial treatment of the fractured femur, previouslyundetectedvascular lesions sometimes surfaced. Palpation of extremities wastherefore part of the routineexamination in the management of combat injuries. Metallic fragmentsnear the course of majorvessels (identified on roentgenograms) heightened the index ofsuspicion of an unrecognizedvascular injury. One patient with a fractured femur who should havebeen in an anabolic coursecontinued in a catabolic course with a persistent tachycardia and wassuspected of having anunrecognized arteriovenous fistula. These lesions made themselves knownby spontaneoushemorrhage from wound sites, an area of rapidly increasing swelling, orby palpation of a thrillover a course of a vessel. Such unrecognized vascular lesions werefairly common. During thecourse of treating patients with extremity injuries, personnel werecautioned to watch diligentlyfor any evidence of such lesions.
Insome cases, vascular repair was unsuccessful. The inability to restoresuccessful distalcirculation usually resulted in ablation of the nonviable portion ofthe extremity. When thisoccurred, primary rules of surgery continued in effect: the extremitywith the fractured femur wasablated at the most distal site possible. Presence of a fractured femurdid not alter the decision fora below-knee amputation if the vascular supply to the extremitysupported an amputation at thatlevel. Consideration was not given to amputation at the fracture siteunless there was no distaltissue viability. In the majority of cases where below-knee amputationdid occur, experience hasshown that the fracture of the femur healed satisfactorily, and thepatient could be fitted with abelow-knee prosthesis.
Thebest concepts and practices from military surgeons of World Wars I andII and theKorean conflict were practiced by orthopedic surgeons during theVietnam War. No substitutefor adequate debridement was considered. Broad spectrum antibiotics andspecific antibiotics forgram-negative and gram-positive organisms were only adjuncts topreventing systemic and localinfections. Adequate drainage and “no closure” were practiced in thecare of open woundsinvolving fractured femurs with disruption of surrounding tissues.Reestablishment of distalvascular flow took precedence over fracture management.
Well-doneinitial wound surgery and early reexploration in signs of sepsis werethe keysto wound and fracture management. Skeletal traction and exercises toall musculature until thepatient gained control of the leg followed. The next step wasweightbearing ambulation with theextremity in a well-fitted cast brace. Early functional rehabilitationgave us superior results.Indeed, the early ambulation of patients in cast braces appears to bethe most outstanding medicalinnovation of the Vietnam conflict for treating thigh wounds.
37
REFERENCES
Bailey, J. D.; Hackthorn, J. C.; Donley, J.;and Burkhalter W. 1976. Cast brace treatmentof femoral fractures. Contemp.Surg.8:32-6.
Bagg, R. J. 1967. Presentation before FarEast Chapter of Association of Military Surgeons.
Brav, E. 1957. Further evaluation of the useof intramedullary nailing in the treatmentof gunshot fractures of the extremities. Journal ofBone and Joint Surgery(Am)39:513-20
Brav, E. A., and Fitts, W T., Jr. 1946.Gunshot fractures of the femoral shaft. Surg.Gynecol. Obstet.82:91-100.
Brav, E. S., and Jeffress, V. H. 1953.Modified intramedullary nailing in recent gun shotfractures of the femoral shaft. Journalof Bone and Joint Surgery35:141-52.
Brown, P 1971. Cast bracing of fracturessponsored by the National Academy of Sciences,Washington, D.C.
Burkhalter, W. E. 1973. Open injuries of thelower extremity: symposium on trauma.Surg.Clin. North Am. 53:1439-57
Carr, C. R., and Turnipseed, D. 1953.Experiences with intramedullary fixation of compoundfemoral fractures of war wounds. Journalof Bone and Joint Surgery 35:153-71.
CINCPAC-4. 1970. Commander in Chief, Pacific.Fourth CINCPAC Conference onWar Surgery. Tri-service conference on war surgery conducted in Tokyo,Japan,16-19 February 1970. Incl with Cover ltr, Frank B. Voris, M.D., RADMUSN,CINCPAC Surgeon, 2 Mar 70.
Connolly, J. F; Dehne, E.; and LaFollette, B.1973. Closed reduction and early castbrace ambulation in the treatmentof femoral fractures. Journalof Bone and Joint Surgery 55:1581-95
Deffer, P.A.; Roschelle, I. A.; and Goodman, F. G. 1971. The managementof fractures of the femur by early ambulation utilizing a mini spicacast brace. Presentation at workshop on cast bracing offractures, sponsored by the National Academy of Sciences, Washington.
DeLorme T. L.; West, F. E.; and Schriber, W. J. 1950. Influence ofprogressive resistance excercises of knee function following femoralfractures. Journal of Bone and JointSurgery (Am) 32:910-24
Hampton, O. P., Jr. 1957. Orthopedicsurgery in the Mediterranean Theater of Operations. MatherCleveland, ed. Washington: GPO.
Moll, J. 1973. The cast-brace walking treatment of open and closed femoral fractures. South. Med. J. 66:345-52
Moll, J. J., and Willhoite, D. R. 1970. Abstract: long-bone defects due to missile injury. Journal of Bone and Joint Surgery (Am) 52:835-37.
Mooney, V.; Nickel, V. L.; Harvey, J. P., Jr.; and Snelson, R. 1970. Cast-brace treatment for fractures of the distal part of the femur. Journal of Bone and Joint Surgery (Am) 52:1563
Soto-Hall R. and Horwitz, T. 1946. Treatment of compound fractures of the femur. J.A.M.A. 130:128-34.