



Chapter 3
PENETRATING WOUNDS OF THE LEG WITH ASSOCIATED FRACTURES OF THE TIBIA
Colonel William E. Burkhalter, MC, USA (Ret.)
HISTORICALBACKGROUND
During World War I, 4,485 American servicemen incurred fractures of the tibia and fibula. Indeed, about 20 percent of all fractures were unstable fractures of the lower leg secondary to battle-incurred injury. The morbidity and mortality from this injury were significant. In the U.S. Army, for battle-incurred fractures of the tibia alone the mortality was 10 percent, and slightly higher if both bones of the leg were fractured. The amputation rate in combined injury to tibia and fibula was 906 of the 4,485 cases or over 20 percent (MD-WW 1927, 493, 499, 507).
At first, prefabricated splints were used in the management of the injury but this method as well as skin or skeletal traction proved unsatisfactory, and both methods resulted in an excessively high rate of nonunion. Tibial fractures made up a substantial proportion of battle-incurred fractures, and tibial fracture nonunion was the most common nonunion. Surgeons at the time concluded that the nonunions had occurred because such fractures required prolonged protection from weightbearing. Thus the plaster of Paris cast became the preferred method of treatment (MD-WW 1927, 507-08, 639-41).
In World War II, military surgeons emphasized the technique of delayed primary closure in debrided open fractures (Cleveland, ETO 1956; Hampton 1957). In the European theater, however, delayed primary closure proved unsatisfactory for battle-incurred injuries below the knee and was possible in only 60 percent of the cases. In a series of 2,393 delayed primary closures with accompanying fractures, primary healing occurred in only 1,592 or about 66 percent. Partial success was achieved by the surgeons in 27 percent, but in 6.7 percent of the cases they suffered complete failure. In a similar group of wounds allowed to heal by secondary intention, 87 percent closed in ten to twelve weeks with 5.4 percent incidence of osteomyelitis (Cleveland, ETO 1956, 91-99, 151). In the Mediterranean theater, Dr. Oscar P. Hampton, Jr., attempted delayed primary internal fixation at the time of delayed wound closure in fractures below the knee; but in 41 of 168 cases, massive skin and bone loss occurred (Hampton 1957, 199).
For battle-incurred fractures of the tibia, treatment continued to emphasize prolonged traction and immobilization followed by prolonged nonweightbearing. Weightbearing was not permitted until beginning union was demonstrated radiographically. No traction or splints were used to maintain stability (Cleveland and Shands 1970, 702). The typical treatment program consisted of a long-leg cast with
40
the knee in various degrees of extension andnonweightbearing. The use of nonweightbearingambulation with plaster of Paris immobilization to manage tibialfractures continued through theKorean War.
Delayed primary closure as a technique achieved support from its use in penetrating injuries of the thigh and upper extremity. However, delayed primary closure with or without internal fixation of the fractures of the lower leg seemed to yield relatively poor results. Statistically, this proved to be another fracture in which delayed primary closure was not an acceptable technique in early management.
TREATMENT INVIETNAM
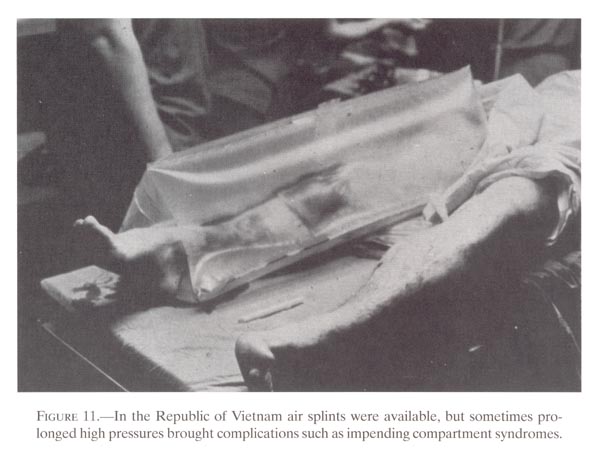
In most instances in Vietnam, open injuries below the knee with associated fractures of the tibia were secondary to high-velocity wounding agents, such as mine explosions and direct bullet wounds, rather than shell fragments. Such wounds were compounded from without and contained considerable debris. The company aid-man provided initial management of the wound and the fracture. He applied sterile occlusive dressing to prevent further contamination from without and to decrease bleeding. Tourniquets were not used. Following application of sterile dressings, some type of external splintage was needed before evacuation from the field. Although pneumatic splints were sometimes available, the leg was usually placed in an Army half-ring splint and held in position with additional slings or triangular bandages (fig.11). Occasionally, bamboo splints and pieces of wood were used. Depending upon the area of operation and sophistication of the equipment, intravenous fluids and, occasionally, blood were given in the field before helicopter evacuation to a fixed facility--a surgical, field, or evacuation hospital.
Upon arrival at the hospital, the patient went to the triage area where his general condition was evaluated and a search was made for additional injuries before surgery. Also in triage the patient received intravenous fluids, tetanus prophylaxis, and large doses of antibiotics. Although the wound itself was not evaluated at this time, the neurocirculatory status of the limb was determined and roentgenograms were obtained in two planes while the limb was supported in the splint. The radiographic examination, in addition to delineating fracture geography, gave additional information about the extent to which the wounding agent had blown gas into the tissues and in the tissue planes proximal to the site of injury. The presence of air proximally along tissue planes alerted the surgeon that he must explore the area extensively for radiolucent foreign bodies. The occlusive dressing and splints remained in place until the patient was in the operating room. Blood transfusions were given as required.
After initial evaluation, the patient was placed in a preoperative holding area and monitored while awaiting surgery. The limb remained splinted with dressings in place, and the patient received intravenous fluids or blood and antibiotics. At this time, most patients did not require analgesic medication. Splinting the limb seemed to decrease post injury pain.
In the operating room at least one person assisted the surgeon during the operative procedure. Treatment began with application of a pneumatic tourniquet and prepping the entire extremity. Next, the wound was explored through longitudinal incisions with little or no skin debridement. Wide incisions and excisions of fascia
41
{kind=link}
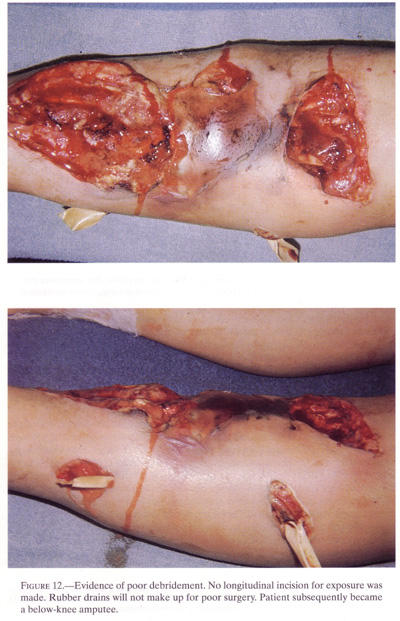
were performed to allow decompression ofindividual muscle compartments and excellentexposure of neurovascular structures and muscle tendon units. Exposureof the arteries and thenerves in the leg during wound debridement allowed protection of thesestructures and avoidedaccidental injury during wound excision. The surgeon removed tissuewith poor blood supply andpoor resistance to infection. In addition, with fascial decompression,he exposed individual musclecompartments. Release of the fascial envelope from each musclecompartment in the leg permittedthe muscles to expand freely (fig.12).
Before Vietnam, medical opinion held that an open fracture decompressed the muscle compartment of the leg and that necrosis of muscle in an intact compartment was rare. This belief was not borne out clinically in Vietnam where compartment syndromes were seen in open fractures. However, this condition differed from those reported by Ellis (1958) and by Owen and Tsimboukis (1965) in closed fractures with accompanying compartment syndromes* because the combination of an open wound with disseminated muscle necrosis throughout the limb resulted in amputation (Schmitt and Armstrong 1970). Therefore, fascial decompression was essential because, without it, muscle swelling in a closed compartment reduced perfusion to the muscle and sometimes resulted in ischemic necrosis of an entire compartment. Ideally, fascial release involved all four muscular compartments in the leg to allow maxi
* Raymond Bagg, M. D. (Col., MC,USA, Ret.),unpublished records of a longitudinal study of cases from 106th GeneralHospital (1966-1970).William E. Burkhalter, M.D., (Col., MC, USA, Ret.) and D. Reich, M.D.Deep posterior compartment syndrome in the lower extremity.
42
{kind=link}
43
mum decompression (Kelly and Whitesides1967). Some vascular injuries in the leg resulted inamputation, but usually widespread fascial excision and compartmentdecompression allowedperfusion to improve and the limb to survive.
The initial treatment was directed primarily to the wound. Exploration and debridement were extremely important at this time; fracture management was secondary. Closure was not carried out, in any instance, at the time of initial wound surgery.
At the conclusion of wound debridement, the tourniquet was deflated, a search made for major bleeding vessels, and the quality of circulation distal to the site of injury evaluated. If no major bleeding points were noted, the tourniquet was reinflated, the wound dressed with fine mesh gauze, and a long-leg plaster cast applied in two sections. The first section applied was the distal portion with the knee flexed at 90 degrees over the edge of the operating table so that gravity would reduce the fracture. The second or proximal portion of the cast was applied above the knee, after the first part had set and generally with the knee in nearly full extension.
After the whole cast had hardened, it was bivalved and wrapped with a bandage to maintain stability for the fracture and soft tissue injury. Some surgeons in Vietnam attempted to use long-leg posterior splints made of plaster of Paris as a substitute for a bivalved long-leg cast, but these repeatedly proved ineffective. The splint broke at the knee and at the ankle and did not protect the fracture and soft tissue injuries. Also, patients so fitted experienced considerable discomfort during evacuation. Frequently, ill-fitting splints produced pressure sores about the heel and, on occasion, a common peroneal nerve paralysis resulted from pressure in the area of the fibular head. The stability of the bivalved and wrapped long-leg plaster cast was far superior to any type of plaster of Paris splint.
If signs of sepsis or excessive pain at the fracture site developed during the immediate postoperative period, the patient was returned to the operating room for redebridement and more extensive exploration. In mine injuries or shell fragment wounds, particularly, the blast effect frequently carried debris proximally, subcutaneously or along fascial planes in the leg. Opening of apparently undamaged muscle compartments both proximal and distal to the wound was required. In certain instances, the wounding agent even blew foreign material into the proximal synovial tissues, such as the tenosynovium around tendons, or even the joints. If the extent of wounding was not appreciated at the time of the initial wound surgery, signs of sepsis developed rapidly and the patient became toxic within the first twenty-four hours. Reoperation with more extensive proximal longitudinal incisions was then necessary to save the extremity. Adequate radiographic films and their perusal at the time of the initial injury sometimes helped the surgeon delineate the extent of the problems, including gas along tissue planes proximal to the actual wounding site.
Because of the interest in delayed primary closure in the management of soft tissue wounds as well as wounds associated with fracture, some attempts were made in evacuation hospitals in Vietnam to apply this technique. In the early years of the Vietnam War, if patients could not be evacuated out of country because of associated injuries, surgeons attempted delayed primary wound closure after the patient was hospitalized in Vietnam for five or six days. Experience showed that this technique was not effective for penetrating injuries of the leg with associated tibial and fibular fractures. This mirrored the World War II experience reported by Hampton (1957, 53-57, 160-80). Soft tissues were markedly swollen, frequently skin was lost,
44
and usually the wound was anterior or anteromedial in the leg. If tension is applied to the skin of this particular area, known for its poor tolerance of tension, necrosis promptly results. Attempts to make relaxing incisions in the posterior calf and to shift skin anteriorly were unsuccessful. Associated complications included massive loss of skin, subcutaneous infection beneath the transferred skin, and further loss of tissue at the fracture site. As a result of this experience early in the Vietnam conflict, participants at the first Pacific Conference on War Surgery in 1967 recommended against tension closures or skin shifts to cover exposed bone (CINCPAC-1 1967, 40) and discouraged relaxing incisions and local rotation flaps. Our experience indicated that, even if a patient could not be evacuated because of associated injuries, no attempt should be made to use the technique of delayed primary closure in penetrating injuries of the leg with associated tibial fractures. Therefore, after the wound had been rendered surgically clean in the operating room, the wound was left open and an occlusive dressing and plaster cast were applied. If nothing suggested sepsis at the fracture site, there was no reason to examine the wound again in Vietnam, even if evacuation had to be delayed because of associated injuries.
Following bivalving of the cast, if the patient was nontoxic, well hydrated, and had an adequate hematocrit, and if other injuries permitted, he was evacuated. A brief operative note concerning the status of damaged tissues in the limb was supposed to accompany the patient, but this was sometimes lost. In order to assure communication in the event that records did not accompany the patient, a conscientious surgeon made notes on the plaster cast regarding whether there were vascular or nerve injuries. If there was a nerve injury, the note regarding loss of substance, simple contusion, or loss of an entire muscle tendon unit was extremely important to the surgeon receiving the patient. Even if operative notes accompanied the patient, they were usually grossly inadequate; the vital positive and important information was not provided on a consistent basis.
TREATMENT AFTER VIETNAM
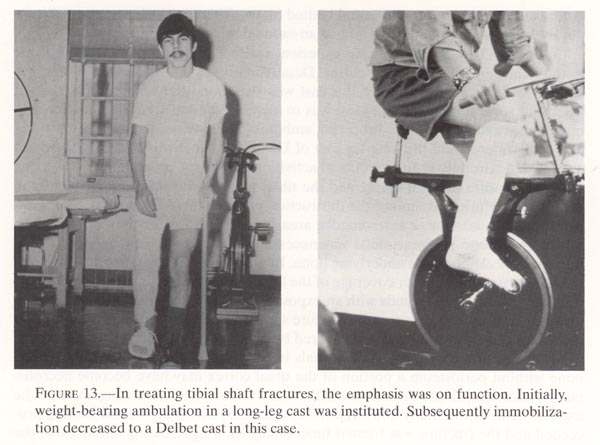
Once the patient left Vietnam, weightbearing ambulation became the goal. In 1961, Ernst Dehne et al. reported on the management of the tibial shaft fracture by weightbearing ambulation in a long-leg plaster cast. This functional method of treatment ignored the wound after the initial surgery and concentrated on early restoration of function using the long-leg cast. Wound closure occurred by secondary intention healing under the cast during weightbearing activity. Until 1965, this method of management was widely practiced in U.S. Army station and general hospitals. Although there was some concern among members of the general orthopedic community about shortening during weightbearing ambulation, the high incidence of union in a relatively short time without associated joint stiffness of the foot, knee, or ankle impressed them. The combat-incurred tibial shaft fracture met the criteria for this functional method of treatment. The highly comminuted fracture was allowed to shorten in a controlled fashion to improve contact stability. Maintenance of full length by traction invited delayed union or nonunion (Dehne et al. 1961a; Dehne et al. 1961b) (fig.13).
{kind=link}
Secondary intention wound healing obviated the need for relaxing incision, tension closure, covering bone by split-thickness skin grafts, cross-leg flap with its associated requirement for internal fixation, and above all the prolonged recumbency of the patient. Because of these advantages, the majority of patients with combat incurred tibial shaft fractures were treated by weightbearing ambulation in a long-leg plaster cast (Brown 1973; Brown 1974; Dehne 1969; Dehne 1974).
In certain instances, surgeons covered large wounds of the calf or lateral leg with split thickness skin grafts before the beginning of weightbearing ambulation. Closure of these wounds decreased fluid loss from the wound and permitted the long-leg cast to be kept in position for a longer time without severe odors developing and cast changes becoming necessary.
Generally, when a patient with an isolated tibial shaft fracture arrived at a fixed facility, he was evaluated in an orthopedic holding area. If there were no signs of sepsis and nothing to suggest problems with the wound, a surgeon in mask and gloves inspected the wounds. He applied a new sterile dressing and a well contoured, total contact long-leg cast that included a walker. Then the patient was ready for weightbearing ambulation. On the other hand, if there were signs of sepsis or considerable foul odor and pain in the extremity, the patient was not evaluated in the holding area. He was removed instead to the operating theater for further operative exposure, debridement, and exploration. Even in an offshore hospital, such as Tripler Army Medical Center in Hawaii and the hospitals in Japan, most of the tibial shaft fractures were treated for a few days with weightbearing ambulation using crutches
46
before evacuation to the continental United States. This approach was generally applicable only to those patients who had an isolated injury below the knee.
Sarmiento (1967) described his experience with the total-contact short leg cast in the management of tibia! fractures. Depending upon the fracture level and the severity of the soft tissue injury, this cast was also used after several days, several weeks, or several months. The ideal was to increase the range of knee motion and muscular activity during weightbearing ambulation. However, in both the short-leg cast of Sarmiento and the long-leg cast of Dehne, the goal was to return the damaged lower extremity to full functional activity as rapidly as possible.
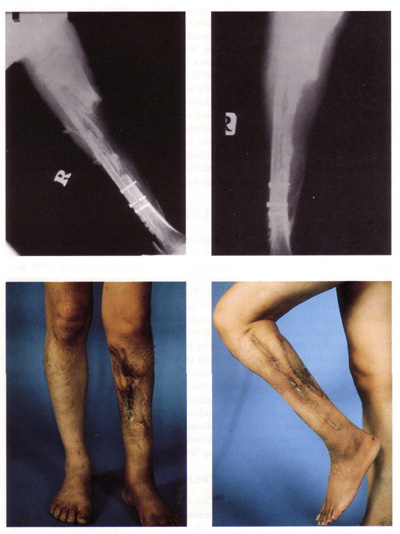
The exposure of tibial cortex and the tibial fracture site was seen frequently in penetrating injuries because of the destruction of overlying skin and soft tissues, especially in the anterior or anteromedial area. Initially, surgeons believed that covering exposed bone by tissue shifts was necessary to preserve bony integrity and to prevent desiccation of the underlying bone. In some large wounds, tissue loss was so great that cross-leg flaps for coverage of the bone were thought to be required. However, in well debrided wounds with an exposed tibial fracture site, union of the fracture occurred without covering the fracture site by tissue shifts, either locally or from a distance. The exposed bone was covered by granulation tissue from viable muscle peripherally and from Volkmann’s canals in the tibial shaft itself. In the exposed bone without periosteum a portion of the tibial cortex may have become necrotic, but the actual depth of necrosis was difficult to evaluate, and the management of the exposed bone was initially nonsurgical. As secondary intention wound healing proceeded and the fracture was treated functionally by weightbearing ambulation, the obviously necrotic bone tended to separate from viable bone beneath and made the decision on depth of bone debridement quite easy. Union of these fractures occurred in a similar time frame to that for open fractures and with no greater infection rate. Union occurred through the well vascularized posterior and lateral tibial cortex and periosteum (Burkhalter and Protzman 1975) (fig.14).
In Brown and Urban’s (1969) discussion of early weightbearing ambulation of tibial shaft fractures, the authors stated that in a series of 60 adult patients with 63 open fractures of the tibia, all fractures united. Forty-two of these 60 patients had combat incurred injuries. In this series, the wounds of 4 patients continued to drain intermittently until the patients were discharged from military service. In these 4 cases, however, drainage was minimal and did not interfere with normal function of the limb or activities of daily living. The final outcome of the drainage was not known. Witschi and Omer (1970) discussed their results with 84 patients with tibial shaft fractures incurred in Vietnam combat. They reported that after their initial attempts to obtain wound closure by split-thickness skin grafts through windows in a plaster cast, their concern with soft tissue wound healing gradually abated. They preferred long-leg or short-leg casts and ambulatory treatment of the fracture, avoiding excessive concern with soft tissue healing. In their series of 84 patients, 7 had established osteomyelitis.
Burkhalter and Protzman (1975) evaluated 228 combat-incurred open tibial shaft fractures treated by debridement, weightbearing ambulation in a long leg-cast, and wound healing by secondary intention. They believed that a well debrided wound allowed to heal by secondary intention responded similarly to a civilian-incurred injury. An open fracture allowed to heal with exposed bone at the fracture site required an average of only two weeks additional time before removal of the
47
external immobilization than did anuncomplicated open fracture. The infection rate in these 228plus 61 civilian cases was 3.8 percent. All of the these infectionsoccurred in military open-penetrating injuries.
In a series of 200 tibial fractures that were treated at the 106th General Hospital in Japan and were followed by record in two hospitals in the United States (Bagg 1966-70), thirteen extremities required some type of amputation, either before or after arrival at the 106th or in a follow-up hospital. The most common cause for these amputations was failure to control sepsis. This was previously reported by Schmitt and Armstrong (1970) from the U.S. Air Force Hospital, Clark Air Base, in the Philippines, for the period 1965 through 1967. Ten of the amputations in the106th General Hospital series were below the knee and three were above the knee or disarticulations of the knee. Five of the patients were lost to follow-up before a definitive decision was made regarding function of the leg and union of the bone.
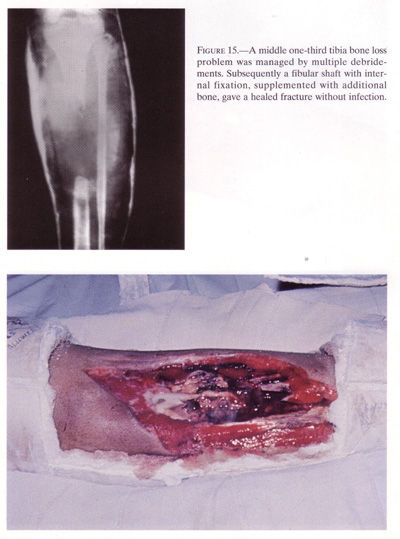
In bone loss injuries the intent was either to obtain union of the tibia by posterior graft or to create a posterior tibial fibular synostosis by the position of the graft in the interosseous space between the tibia and the fibula.
Gaines and Reid (1976) from Brooke Army Medical Center in Texas reported on 44 infected nonunions of the tibia treated by posterolateral bone grafting. Twenty-three of these patients had established osteomyelitis at the time of operation but were free of drainage. Twelve wounds were actively draining anteriorly at the time of the surgery. Following insertion of the graft, the operative wounds were allowed to heal by secondary intention, and weightbearing ambulation was started within a few days of surgery. Union occurred in all cases and drainage ceased in 9 of 12 that were actively draining at the time of surgery.
From Letterman Army Medical Center in San Francisco, Freeland and Mutz (1976) described a similar series of 23 infected nonunions treated by posterolateral bone grafting. At the time of their operations 12 patients had actively draining wounds. Of these 23 cases, all patients achieved bony union. Wounds that were actively draining in 10 other patients at the time of surgery ceased drainage following the operation and union. As in earlier series (Hanson and Eppright 1966; Harmon 1945; Jones and Barnett 1955), these surgical wounds, created when the posterolateral bone graft was applied, were allowed to heal by secondary intention, and weightbearing ambulation in a long-leg cast was started within a few days postoperatively.
In certain cases of open injury of the leg, large gaps were left in the tibial shaft, with or without an intact fibula. Nevertheless, although high degrees of comminution frequently accompany high-energy missile injuries, loss of bone substance was usually minimal. Moll and Willhoite (1970) commented that, while the wounding agent might cause actual bone loss, the usual cause for bone loss was overdebridement of the bone at the time of the initial surgery. To avoid these large gaps, surgeons should place continuing emphasis on saving all bone, even without attached soft tissue. Even though necrotic, these fragments add some immediate support and act as a scaffolding for future bone formation. If sepsis becomes a problem, these loose pieces of bone can be sequestered, as dictated by the host.
When large bone gaps were encountered, management of the wound varied with the state of soft tissue injury. Wound management of the patient with normal nerve and vessel function in the foot, a good functional calf, and good posterior skin differed considerably from that of a patient with a stiff anesthetic foot and poor muscu-
48
{kind=link}
49
{kind=link}
50
{kind=link}
{kind=link}
52
lature in the leg. If the patient’s foot and soft tissue in the leg were in reasonably good condition so that amputation was initially ruled out, the problem could be approached in two ways. The most obvious approach was controlled shortening. If shortening of two inches allowed bone contact, this was certainly preferable to maintaining full length and creating a bone loss nonunion. Certainly with only marginal soft tissues in the leg, this was proper procedure. Since most surgeons would not accept more than two inches of shortening, for a loss greater than this, some type of bone grafting was necessary. Huntington’s fibular shift (Huntington 1905; Wilson 1941), although adding additional instability by fibular section, was used, in some cases, to manage the problem of the tibial shaft loss with the intact fibula (fig.15). This fibular shift was augmented by additional cortical cancellous iliac graft and served as one approach to the management of the loss of tibial shaft. The creation of a proximal and distal tibial fibular synostosis by using cortical cancellous graft was also effective. Both of these procedures avoided poor skin and scar anteriorly, placed the bone graft in the best vascular bed (that is, the well vascularized posterior calf muscles), and allowed continuing functional activity. The persistence of anterior drainage was no deterrent to these posterolateral procedures.
RECOMMENDATIONS
The penetrating injury to the leg with associated tibial fracture should be managed by wound exploration and debridement, as indicated. Wound closure by tissue shifts or transfer from a distance is generally not required even though there may be actual soft tissue loss at the fracture site. Secondary intention wound healing will occur beneath a functional plaster cast. The single most important factor in the management of the open tibial fracture is early, adequate wound debridement, followed by the return of leg function through weightbearing ambulation in a plaster cast. Exposure of bone or fracture site is no indication to alter the treatment plan. Nonunion with or without infection can be managed successfully in almost all cases by posterolateral bone grafting. Union in these cases frequently may bring about cessation of drainage from the fracture site. The most widely used method of management of the open tibial fracture in the Vietnam War consisted of meticulous wound debridement and wound exploration, the application of a functional plaster cast as soon as possible, and the institution of weightbearing ambulation, also as soon as possible. These wounds were allowed to heal by secondary intention. The precepts of closed plaster treatment followed in the Vietnam War were those advocated by Trueta (1976) before and during World War II.
REFERENCES
Brown, P. W. 1973. The open fracture. Clin.Orthop.96:254-65.
_______. 1974. The early weightbearing treatment of tibial shaft fractures. 105:167-78.
Brown, P.W., and Urban, J. G. 1969. Earlyweightbearing treatment of open fracturesof the tibia. Journal of Bone andJoint Surgery (Am) 51:59-75.
Burkhalter, W. E., and Protzman, R. 1975. The tibial shaft fracture. J. Trauma 15:785-94.
53
CINCPAC–1. 1967. Commander in Chief, Pacific.First CINCPAC Conference onWarSurgery. Tri-service conference conducted at John Hay Air Base, Baguio,thePhilippines, 20-25 May 1967.
Cleveland, M., ed. 1956. Orthopedic surgery in the European Theaterof Operations. Office of the SurgeonGeneral, Department of the Army. Washington: GPO.
Cleveland and Shands, A.R., eds. 1986.Orthopedicsurgery in the Zone ofInterior. Officeof the Surgeon General, Department of the Army. Washington: GPO.
Dehne, E. 1969.Treatment of fractures of the tibial shaft. Clin.Orthop. 66:159-73.
_______. 1974.Ambulatory treatment of the fractured tibia. Clin.Orthop. 105:192-201.
Dehne, E.; Deffer, P.A.; Hall, R. M.; Brown, P. W.; and Johnson, E. V. 1961a.Thenatural history of the fractured tibia. Surg.Clin. (N Am)41:1495-513.
Dehne, E.; Metz, C. W.; Deffer, PA.; and Hall, R. M. 1961b. Non operative treatment of the fractured tibia by immediate weightbearing. J.Trauma 1:514-35.
Ellis, H. 1958. Disabilities after tibial shaft fractures. Journalof Bone and Joint Surgery (Br) 40:190-97.
Freeland, A. E., and Mutz, S. B. 1976. Posterior bone grafting for infected ununited fracture of the tibia. Journal of Bone and Joint Surgery (Am) 58:653-57.
Gaines, J. H., and Reid, R. L. 1976. Salvage of the infected tibial non-union. Journal of Bone and Joint Surgery (Am) 58:723.
Hanson, L. W., and Eppright, R. H. 1966. Posterior bone-grafting of the tibia for non-union. Journal ofBone and Joint Surgery (Am) 48:27-43.
Hampton, 0. P., Jr.1957. Orthopedicsurgery in the MediterraneanTheater of Operations. Mather Cleveland, ed. Office of The Surgeon General, Department of theArmy. Washington: GPO.
Harmon, P. H. 1945. A simplified surgical approach to the posterior tibia for bone-grafting and fibular transference. Journal of Boneand Joint Surgery (Am) 27:496-98.
Huntington, T. W 1905.Case of bone transference: use of a segment of fibula to supplya defect in the tibia. Ann. Surg. 41:249-51.
Jones, K. G., andBarnett, H. C. 1955. Cancellous-bone grafting for non-union of thetibia through the posterolateral approach. Journalof Bone and Joint Surgery(Am) 37:1250-60.
Kelly, R. P., and Whitesides, T. E., Jr. 1967. Transfibular route for fasciotomy of the leg. Journal of Bone and Joint Surgery (Am) 49: 1022-23.
MD-WW. 1927. The Medical Department of theUnitedStates Army in the world war. vol. 11, pt.1. Washington: GPO.
Moll, J. H., and Willhoite, D. R. 1970. Long bone defects due to missile injury. Journalof Bone and Joint Surgery (Am) 52:835-36.
Owen, R., and Tsimboukis, B. 1965. Incidence of ischaemic contracture following closed injuries to the calf. Journal ofBone and Joint Surgery (Br) 47:184.
Sarmiento, A. 1967. Afunctional below-the-knee cast for tibial fractures. Journal ofBoneand Joint Surgery (Am) 49:855-75.
Schmitt, H. J., Jr., andArmstrong, R. G. 1970. Wounds causing loss of limb. Surg.Gynecol. Obstet. 130:682-84.
Trueta, J. 1976.Reflections on the past and present treatment of war wounds andfracturesMilitary Medicine 141:255-58.
Wilson, P. D. 1941. A simple method of two-stage transplantation of the fibula for use in cases of complicated and congenital pseudarthrosis of the tibia. Journalof Bone and Joint Surgery (Am) 23:639-75.
Witschi, T. H., and Omer, G. F., Jr. 1970. The treatment of open tibial shaft fractures from Vietnam war. J. Trauma 10:105-11.