



Chapter 4
WOUNDS OF THE HAND
ColonelWilliam E. Burkhalter, MC, USA (Ret.)
The hand wound is unique in military surgery. The wound is not mortally dangerous, but without meticulous care, it can be the source of considerable disability for years. Because hand wounds are not life threatening, the priority for evacuation and early surgery is low. In the patient with multiple injuries, a hand wound is treated after lifesaving surgery has been performed, the normal procedure in both military and civilian hospitals. About 15 percent of combat incurred injuries have a hand injury alone or associated with injuries to other limbs, the abdomen, or the chest (Bunnell 1955, 20). Despite the relative benignity of the wound, injury to the hand, wrist, or distal forearm is of considerable interest to military surgeons because a soldier is militarily useless without use of his hands. Thus, these lightly wounded personnel may be the source of great loss of manpower and utilize many military medical resources.
DEVELOPMENT OF ARMY HAND SURGERY*
Wounds of the hand have been a common problem for the military surgeon for some time. Maj. Gen. George E. Armstrong, former Surgeon General of the Army, pointed out that in the Civil War (1861-65) hand wounds numbered approximately one-ninth of wounds recorded in the Union Army (Bunnell 1955, v). Approximately 15,200 flesh wounds of the hand and 12,865 fractures of the hand and wrist bones caused by shot injury were recorded. Despite this high incidence, hand wounds received little special attention. In the official Medical and Surgical History of the War of the Rebellion (MSHWR 1876), only six pages are devoted to hand wounds and operations and an additional twenty-four pages to wrist wounds and operations, a pattern that continued in World War I. In the volume published in 1927 that describes the Medical Department of the U.S. Army in World War I, fewer than 500 lines cover the subject of hand injuries (MD-WW 1927).
By World War II, however, with the increasing specialization of American medicine, some surgeons began to concentrate on wounds of the hand, which comprised a substantial portion of all wounds. One estimate indicates that of the 592,170 persons wounded and injured in action during World War II, 148,042 (25 percent) incurred upper extremity wounds and 88,825 (15 percent) had wounds or injuries which affected the hand. Some 22,000 injured hands were treated in hospitals in the Zone of Interior (Bunnell 1955, 17-75).
One surgeon particularly interested in hand wounds was Dr. Sterling Bunnell. In November 1944, Bunnell began the first of a series of eight tours of the nine
* Raymond M. Curtis, M.D., contributed to this section.
56
hand centers in the Zone of Interior. In thefall of 1945, despite the fact that the centers were atthe peak of their activity and surgeons assigned to them were operatingon 933 patients a month,he found the centers had few hand surgeons (Bunnell 1945). Nonetheless,out of these handcenters came the impetus for the development of this importantspecialty of surgery.
Dr. Bunnell’s visits allowed him to put surgeons interested in hand surgery in contact with each other. In the fall of 1945, Drs. S. Benjamin Fowler, Robert Payne, Darrel T. Shaw, and George Van O. Webster met in the quarters of Dr. Joseph H. Boyes at the Newton D. Baker General Hospital to discuss the formation of a hand group. On 20 January 1946, the American Society for Surgery of the Hand was organized in Chicago, with thirty-five founding members present (Curtis 1971; Reid 1979).
After World War II, when residency training programs in orthopedics and plastic surgery were established, the need to include training in hand surgery was apparent. The outbreak of the Korean War once again demonstrated the need for hand surgeons, but the Army found hand specialists in short supply. Only a few Regular Army officers had been assigned to the hand centers during World War II, and the last of the centers, Letterman Army General Hospital in San Francisco, had discharged its last hand patient in 1948. The solution was to appoint civilians, many of whom had served during World War II in the hand centers, as consultants to the general hospitals. One particular center of hand work was Valley Forge General Hospital, Pennsylvania, where Dr. J. William Littler, who had been a surgeon in a hand center during World War II, acted as civilian consultant, assisting Capt. Eric E. Peacock, Jr., MC. Despite the obvious need for hand specialists, a hand service was not organized at Walter Reed General Hospital until 1960, when Col. John D. Blair, MC, then chief of orthopedics at Walter Reed, assigned Lt. Col. Charles W. Metz, Jr., assistant chief of orthopedics, the duty of establishing a hand service and a one-year fellowship in hand surgery. To assist in the organization of this program, The Surgeon General, Lt. Gen. Leonard D. Heaton, appointed Dr. Raymond M. Curtis Consultant in Hand Surgery to The Surgeon General on 31 May 1960.
Although the hand service at Walter Reed was a part of the orthopedic service, this special year of training was open to any Army medical officer. The orthopedic service was staffed so that one officer, after completing his fellowship, remained as the assistant chief of orthopedics and the chief of the hand service, thus providing continuity within the hand service and the supervision and teaching needed for each new fellow.
The program was organized to make it possible to train enough officers with special interest and expertise in hand surgery to assign one to each general hospital. By 1963 this was possible, and when the casualties from Vietnam began to arrive, specialists in hand surgery were available at each general hospital to manage these difficult problems. By 1979, thirty-six Army Medical Corps officers had completed the fellowship in hand surgery at Walter Reed (Reid 1979).
GeneralManagement of Hand Wounds
As a rule, hand wounds in the Republic of Vietnam were initially managed by a fully or partially trained orthopedic surgeon with an interest in hand surgery, who, if he had no formal training in hand surgery, was supervised or assisted by a surgeon with special interest or training. Initial wound management began in the triage area with
57
{kind=link}
58
{kind=link}
{kind=link}
60
examination of the hand and forearm for nerve, vascular, or tendon injury and the application of a simple wound dressing. At this time, because the low priority for hand surgery led to delays in operating on these wounds, the hand was elevated and splinted to minimize swelling. Usually penicillin and tetanus prophylaxis were administered. A radiographic examination of the hand at this time was extremely important so that fractures, foreign bodies, and dislocations could be diagnosed prior to surgery. Most injuries of the distal portion of the upper extremity had tendon, bone, and joint involvement, as well as associated dislocations. Basilar joint of the thumb and intercarpal or carpometacarpal dislocations occurred from the penetrating injury or from the fall following the wounding. In the triage area, roentgenograms done in two planes to determine the extent of bone and joint injury frequently disclosed large metallic fragments, such as pieces of shell casing and spent bullets, lodged in the tissues.
In the operating room, the wound was examined with a pneumatic tourniquet in place for temporary hemostasis, adequate light, and either general or axillary block anesthesia. Initially, the surgeon focused on the meticulous cleaning of the skin and fingernails to reduce foreign body and bacteria contamination. After satisfactory preparation, the wound was explored. The majority of hand wounds required extension into physiological incisions for exposure of damaged structures and for the protection of undamaged structures during wound debridement. Additional incisions for exposure included opening the carpal tunnel to protect the median nerve and its branches during debridement of proximal palmar injuries. In crushing wounds, intrinsic muscle decompression was performed through small dorsal longitudinal incisions. These incisions extended into the intermetacarpal spaces and decompressed these closed spaces between the metacarpal shafts. The status of injured structures was noted in the operative records, and surgical extensions were described.
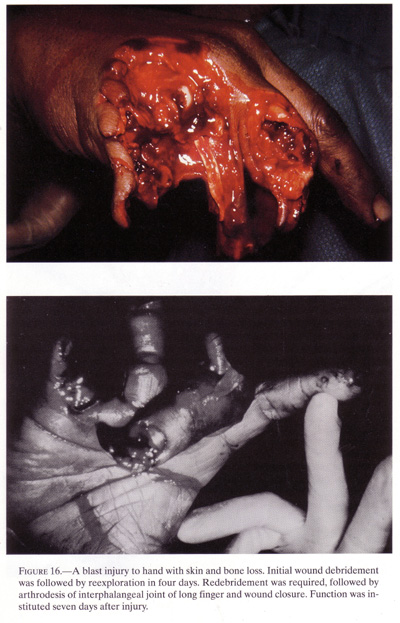
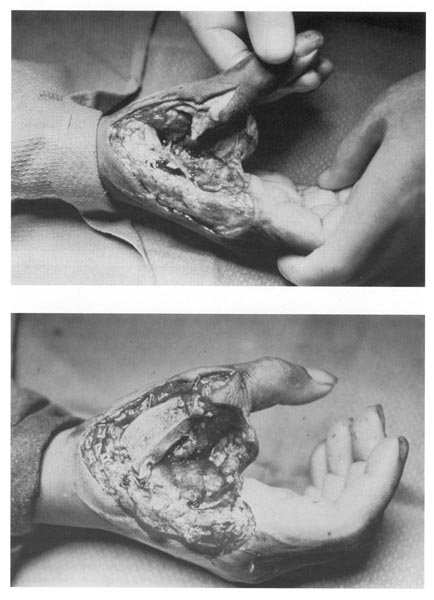
Leaving the wound open after the initial debridement allowed the surgeon to reexamine the tissues in three to seven days (fig.16). At that time, viable and nonviable muscle could be distinguished more easily, and decisions about future management could be made. Debridement of intrinsic muscle resulted in considerable loss of function and was avoided, if possible, during staged wound management. However, this did not imply that the initial exploration and debridement were unimportant. If the initial surgery failed to clean the wound thoroughly, the second procedure would inevitably involve debridement of a wound that would probably become infected. Therefore, initial surgery guidelines called for minimal skin debridement and generous fascial excision. Bone, tendons, nerves, and blood vessels were preserved, and only nonviable muscle was excised. Questionable tissue was left to await a second look procedure. Although Bunnell, in World War II, had maintained that hand wounds should be closed immediately after wound debridement, in Vietnam, highly contaminated hand wounds were not closed at the time of the initial wound surgery but were managed like other wounds. This procedure proved best in literally hundreds of cases (Burkhalter et al.1968; Butler 1969; Jabaley and Peterson 1973; Churchill 1944; Cutler 1945).
After complete wound exploration and debridement, as indicated, the hand was rendered surgically clean in the operating room. The wound was then dressed with fine mesh gauze and an occlusive dressing that offered gentle compression by fluffs placed between individual fingers, helped avoid swelling, supported the wounded parts, and positioned the thumb in opposition to avoid stiffness in a nonfunctional position. A plaster splint stabilized the wrist. A piece of stockinette, triangular ban
61
{kind=link}
62
{kind=link}
63
{kind=link}
dage, or muslin was fashioned into a sling tomaintain elevation with the elbow supported andwithout constriction. Elevation was unremitting either in the slingwhile asleep or by the use ofthe patient’s own musculature.
After initial surgery, the patient with a hand injury was ready for evacuation either to an evacuation hospital in the Republic of Vietnam or to an offshore hospital. His evacuation priority was based on medical preference, the tactical situation, and his associated injuries. Ideally, no matter where he was sent, the occlusive dressing was maintained in place for three to seven days. The patient was then placed under anesthesia in an operating room for a second wound exploration. In this procedure, the surgeon at an evacuation or offshore hospital, rather than the original surgeon, searched for nonviable muscle, loose bone, necrotic fascia, and foreign bodies. When the wound was free of necrotic tissue and foreign debris through debridement and inspection, the surgeon planned the reconstruction. The first consideration was skeletal stability. With minimal degrees of comminution, internal fixation of fractures with a small Kirschner wire gave the stability necessary for early action motion. Dislocation, in addition to fracture, sometimes gave instability to the hand. The two most commonly noted and frequently missed dislocations were at the basilar thumb joint and the carpometacarpal joint, either of the two ulnar most digits or all the carpometacarpal joints of the hand. The severe soft tissue wound plus the dynamics of the dislocation made internal fixation with Kirschner wires almost mandatory after reduction of the dislocation. Loss of reduction during subsequent operative procedures or during evacuation was sometimes associated with considerable morbidity and functional loss.
If bone loss was present or comminution was extensive, spacer wires applied to the metacarpals could be used to maintain metacarpal length and give stability.
64
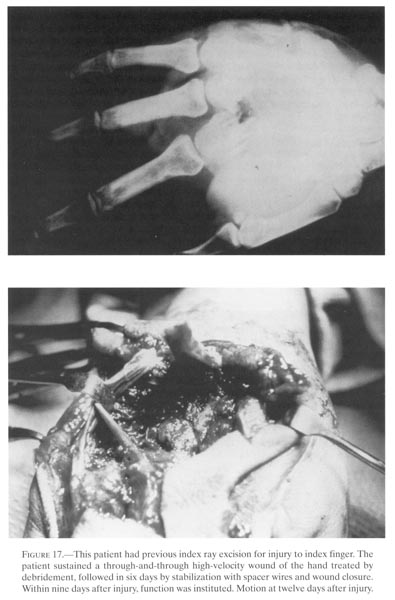
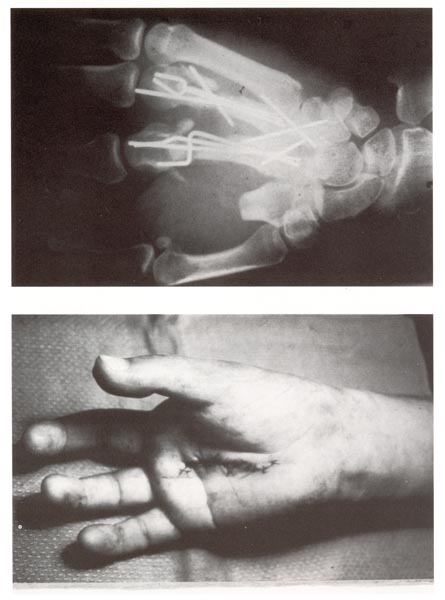
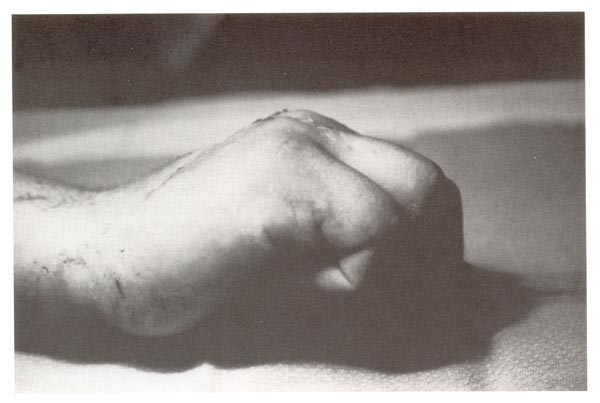
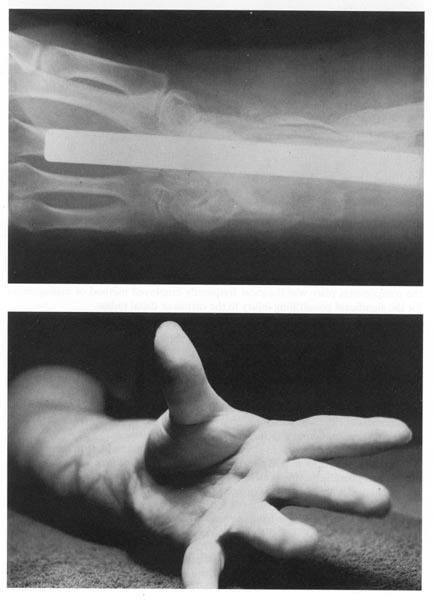
These spacer wires were created by the operating surgeon at the operating table. Proximally the wire was placed in the medullary canal of the proximal portion of the metacarpal fracture and bent at 90 degrees at the fracture or bone loss site so that the wire then abutted on the cortex. Another 90 degree bend was made back to the original plane of the wire. These two 90 degree bends allowed cortical abutment. The bone loss length system dictated the next 90 degree bend in the wire distally at the area of cortical bone and then another 90 degrees so that it went in the medullary canal of the bone distally. If this was in the cancellous head, longitudinal traction on the finger could bring about increase in length and then the wire could be snapped into position. Generally, two or more of these 0.045 inch Kirschner wires crossed obliquely could be used to maintain length, and additional wires increased necessary stability. Although the term “spacer wire” has been used, the major usefulness of these devices lay in achieving skeletal stability so that even in a bone loss situation active motion could be instituted (fig.17).
Although there was a temptation to perform tendon and nerve repairs in a wound that was clean and ready for closure, the explosive injury with widespread multitissue damage throughout the hand did not lend itself to this type of surgery. Further trauma and immobilization were not needed in the hand with such widespread damage. Thus, at the secondary operative procedure, tendon and nerve repair was not generally carried out. The emphasis was placed on achieving a surgically clean wound that would accept closure without the development of infection but with stable skeletal structures.
Finger and thumb amputations or partial hand loss generally occurred at the time of wounding. The initial wound surgeon, therefore, performed only initial wound exploration and debridement of a traumatic amputation rather than amputation surgery. Unfortunately, at the initial surgery, there was a tendency to remove nonfunctional but viable tissue. Obviously, in the hand with multiple injuries, all viable tissue should be preserved. Fingers that are useless but have skeletal structures supporting usable tissues should be maintained at the initial wound surgery. Removal of skeletal stability at the time of the initial wound surgery results in loss of skin support and, if for any reason wound closure could not be carried out on schedule, the skin would shrink and lose its usefulness as a covering agent. At the time of the second look, finger filleting could be done and wound closure achieved with skin that had been under normal tension just a few minutes before.
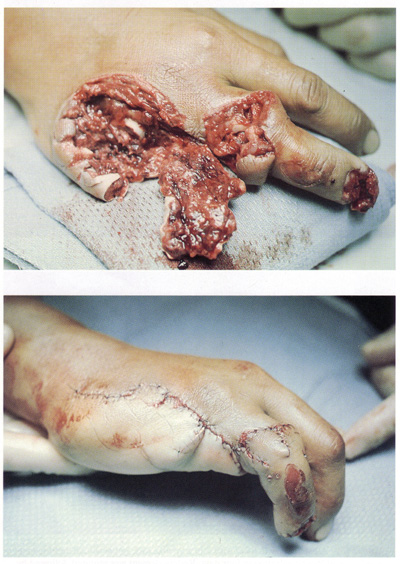
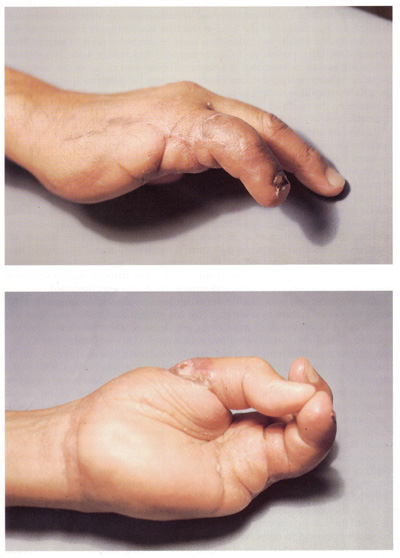
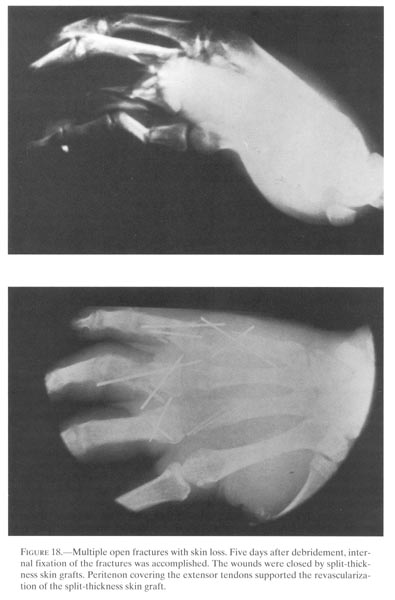
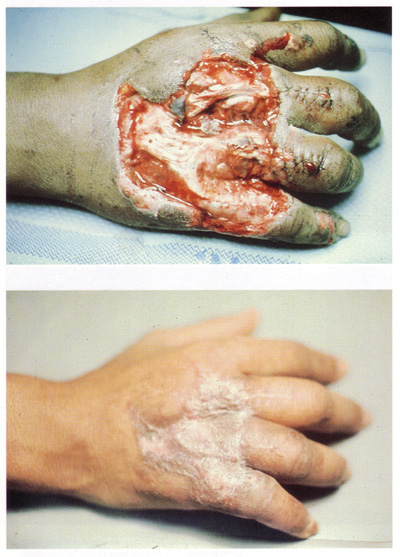
Wound closure is an elective operative procedure that should be carried out when the wound is free of necrotic tissue and foreign bodies and has a low bacterial count. Clinically, in most situations, the surgeon carrying out wound closures at the second look determined the absence of necrotic tissue and foreign bodies by inspection because lack of resources generally prohibited bacterial counts. Methods of closure usually used were direct suture, split-thickness skin graft, or finger fillet. If skin loss was a problem, split-thickness skin graft, with or without meshing, was carried out. Surgeons avoided local tissue shifts within the hand, volarly or dorsally, because infection and poor blood supply might result in loss of transposed tissue. Wound closure failures occurred in the hand, as in other parts of the body, because of dead space, lack of drainage, or closure under tension. Delayed primary closure of hand wounds was successful in 95 to 98 percent of the cases (fig.18).
Certain explosive wounds required pedicle tissue from a distance for wound closure. If so, following the initial wound surgery, the patient should have been evacuated
65
{kind=link}
66
{kind=link}
67
{kind=link}
immediately to a fixed facility withconsiderable holding capability where the procedure couldbe carried out under ideal circumstances. In those cases where this wasnot done and abdominalpedicle flaps were applied in Vietnam at the time of the initialsurgery or at the time of thesecond look, difficult problems occurred postoperatively for thepatient, the physician, and thehospital staff. Because of time lost during evacuation and lack of goodmanagement during theevacuation process, patients leaving Vietnam with abdominal pedicleflaps in place usuallyarrived at their destinations with low grade wound infections,edematous stiff hands,considerable discomfort in the shoulder and elbow, displaced dressings,and flaps frequently lostbecause of displaced dressings or tension (Butler 1969). If the patientrequired pedicle flapcoverage, the procedure should have been carried out in a delayedprimary fashion that wouldhave allowed evacuation of the patient to an offshore or a morepermanent facility and permitteda second look before wound closure. Then, after surgeons removednecrotic tissue and foreignbodies, the flap could be applied. Ideally, the flap was applied to anoptimally debrided wound.Because of the requirement for secondary surgery, flap coverage as themethod of closure atdelayed primary time usually was indicated for dorsal skin and tendonloss, with or withoutfracture. Thumb web space and palmar skin loss areas accepted splitthickness skin graft closuresreadily.
Reconstructive Surgery
Reconstructive surgery of the combat-incurred hand injury was done at an offshore hospital or in the United States. The decision to evacuate a patient who still had his hand in the initial wound dressing was based on patient flow, volume of cases, and lack of associated injuries that precluded early evacuation. Some patients arrived in
68
continental United States (CONUS), often within two weeks of injury, with their open hand wounds in the dressings applied at the time of initial wound surgery. Within CONUS, these patients then underwent all reparative surgery, such as reduction and stabilization of fractures or fracture dislocations and closing of wounds.
The timing of reconstruction in the patient with a penetrating hand injury was important. Achieving a closed wound with minimal tissue reaction and with a stable skeleton meant that rehabilitation could be instituted. Active motion, splintage to improve overall range of motion, and the use of the hand in activities of daily living and light work were all used in the rehabilitation effort. Between wound closure and reconstructive surgery, the aims included achievement of a full range of active motion, passive motion, or both; absence of swelling; and giving the patient the ability to use whatever hand function he had in some useful endeavor. Full range of motion meant no contractures, but in this group of combat-injured hand patients, achievement of a full range of even passive motion was unlikely. Some residual deformity would likely remain, but the absence of swelling and the hand’s usefulness and relative freedom from pain generally indicated readiness for reconstructive procedures. Even today, regardless of the type of reconstruction contemplated, the criteria indicated above should be met before undertaking a reconstruction operative procedure. Results of premature operative procedures, performed too close to the time of the initial wounding and when the hand is still reactive, often failed, discouraging both patient and physician. Waiting too long was preferable to operating prematurely.
Reconstructive surgery for the patient with a complex hand injury with skin loss usually took place at an offshore hospital where wound exploration or skin closure was done. The most obvious methods of wound closure for explosive injuries, were finger fillet or split-thickness skin graft. Postoperative management of the split-thickness skin graft of the hand usually consisted of applying an occlusive dressing for four to six days with subsequent dressing changes. However, the irregular wound surfaces, perhaps with postoperative bleeding or oozing, frequently compromised the overall “take” rate. Because of the limited success of the split-thickness graft, the hand was frequently immobilized for many days. The open technique, which had been so successful in the grafting of lower extremity wounds (the graft could be observed frequently and rolled back to keep fluid from collecting beneath it), did not lend itself readily to hand wounds because of the gross irregularity of the surfaces and the need for early joint motion.
To cover burns, Tanner, Vandeput, and Olleg (1964) described the technique of creating mesh out of split-thickness skin grafts by placing parallel cuts to increase the graft size. The Tanner-Vandeput method of meshing autogenous skin graft proved well suited in dealing with extensive skin loss on the lower extremity. Meshing increased the graft size. The high “take” rates characteristic of this technique seemed to be related to its inherent drainage characteristics, its tendency to conform well to the irregular surface, and its rapid adherence to the recipient site. For the same reasons, this approach promised to be just as satisfactory for coverage of open hand wounds as for similar injuries in the lower extremity. Experience proved that the ability of the graft to conform to the irregular and cavitary type of hand wound plus the drainage characteristic made this an excellent method of obtaining wound closure in a complex explosive injury. Moreover, the rapid adherence of the graft to the recipient shortened immobility time following grafting.
69
Shaffer’s experience (1971) with mesh skin graft in the hand demonstrated an average “take” rate of 93 percent. He believed that at least 50 percent of these patients did not require a further operative procedure, either for cosmetic or functional requirements. That is, the graft was satisfactory and did not have to be replaced by pedicle tissue. Mesh grafts adhered more quickly than sheet grafts. The decreased period of immobility to achieve wound closure prevented loss of motion in severely damaged hands that had complex disseminated injuries. Once its advantages became clear, the meshed split-thickness skin graft was widely used to achieve rapid wound closure in offshore and CONUS hospitals.
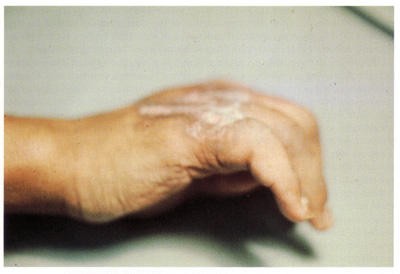
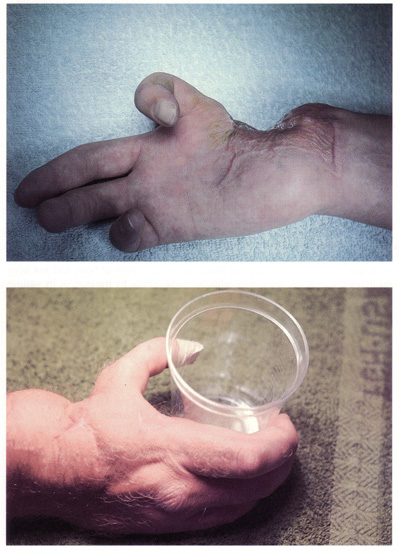
Secondary intention wound healing as a method of skin closure proved effective, contrary to the belief of many authorities that allowing hand wounds to heal by secondary intention brought about stiffness and loss of motion. If skin loss was considerable and if the hand was immobile or splinted in a poor position, this was indeed true. If the patient, however, was capable of actively moving the joints and tendons, stiffness did not result, regardless of the status of the skin cover. Certainly this was seen in the patient with dorsal burns who achieved full mobility before autogenous skin grafting. Active motion within a few days of injury was the key to prevention of motion loss and joint stiffness, and it was much easier to prevent this condition than to overcome it, once established, surgically or by splintage. In certain instances in which tendon or bone work was necessary to overcome fixed deformities, pedicle flap coverage from a distance became necessary. For years, the classic abdominal pedicle flap or thoracoabdominal flap to give fat and full thickness skin had been the standard of reconstruction for these damaged hands. In 1917, Aymard described a deltopectoral flap based on the perforating vessels of the internal mammary artery. This flap was used for nasal reconstruction. At about the time of the outbreak of the Vietnam War, Bakamjian (1965) promoted a similar flap for pharyngeal and esophageal reconstruction. McGregor and Jackson (1970) mentioned the use of this deltopectoral flap in hand surgery. They pointed out that the flap could be elevated without delay, tubed to produce a closed system, and rotated almost 180 degrees upon itself. The flap could be made long enough to allow skin coverage on either the palmar or the dorsal surface of the hand or wrist. In addition, the location of the flap in the deltopectoral area permitted elevation of the hand during transfer of the flap (fig.19). The tube pedicle provided enough freedom for active use of the fingers and wrist during transfer of the skin. The large donor defect in the chest and arm was the only real deterrent to its routine use. Stein and Morgan (1972) presented their experience at Valley Forge General Hospital with the deltopectoral flap for the release of contractures, for resurfacing areas of skin loss both volarly and dorsally, and as an effective aid in osteoplastic reconstruction of the thumb. The general belief of many hand surgeons in CONUS was that the deltopectoral flap was extremely usable in the hand. They were in agreement with McGregor and Jackson (1970), who believed that the deltopectoral flap was a marked functional improvement over the abdominal pedicle because of the quality of skin, the creation of the tube system without delay, and the persistent elevation of the hand during skin transfer.
Reconstructive surgery could also involve bone grafting, which was frequently necessary after penetrating hand trauma. Extreme degrees of comminution and bone loss secondary to injury, debridement, or both usually required the addition of bone to achieve
70
{kind=link}
71
{kind=link}
72
union. These bone grafts were most frequentlyused in the metacarpals and were only rarelynecessary in the phalanges. Spacer wires in the metacarpals of thefingers gave sufficientstability to the digits so that active motion and external splintage,if necessary, could beinstituted. Once these wires were in place, there was no immediaterequirement to bone graft themetacarpal to prevent shortening. In single metacarpal injuries of thelong or ring finger, boneloss did not usually require spacers because of splintage by themetacarpals on adjacent sides.The deep intermetacarpal ligaments gave stability and preventedshortening to a significantdegree. In this situation, the severity of the soft tissue injury andthe ability to maintain orachieve motion in the digit determined whether bone grafting or rayamputation was theappropriate reconstructive surgery. The iliac crest was the most widelyused donor site for bonegrafts in the hand.
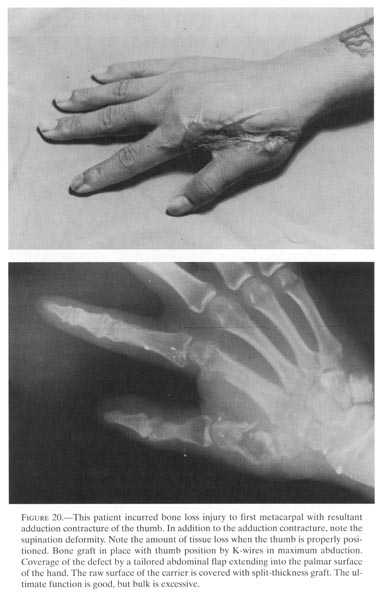
Multiple operative procedures in the severe open injury that required insertion of a bone graft and internal fixation of the graft certainly set the stage for development of infection because cortical bone tolerates sepsis poorly and rarely is revascularized in the presence of infection. The osseous tissue obtained from the iliac crest for bone grafts in the hand could be both cortical and cancellous for rapid union and revascularization. The graft could then be either tri-or bicortical, depending on whether both inner and outer table and the crest were removed. The graft could be fashioned easily to fit any deformity. Internal fixation with Kirschner wires generally gave adequate stability so that early motion could be instituted. This graft would be incorporated even in the presence of sepsis. Generally, cortical cancellous iliac grafts needed only short periods of protection before instituting full use of the extremity (fig.20). Pathologic fractures of the graft, as might be encountered in cortical bone, were not seen.
When bone grafting to replace bone loss, if the length of bone had not been maintained during the interim by adjacent metacarpals, by traction, or by various types of spacer wires, no attempt was made to regain length during the reconstructive operative procedure. Attempted lengthening following weeks or months of shortening resulted in marked tightening of the intrinsic muscle tendon unit with subsequent difficulty in finger flexion and subluxation or dislocation of the metacarpophalangeal joint.
Tendon Injury
One has only to read the hand surgery volume of the Medical Department, United States Army, Surgery in World War II series (Bunnell 1955) to realize the serious problem posed by the flexor tendon injury from 1942 to 1946. The combination of multiple tissue injuries, generally one or more fractures, sometimes low grade sepsis, and often delay between injury and surgery compromised the overall result in this group of patients. The wide dissemination of injury delayed tissue equilibrium, frequently for many months. The association of tendon injury, scar tissue with or without fracture, and nerve injury militated against achieving a good functional result from free graft or transfer.
During the Vietnam conflict, two approaches were used to restore tendon function. One, basically, was the complete debridement of all scar tissue, including pulley tendon remnants, along the course of the bed to be grafted. Skin with the fat was then applied to the underlying bones and joints. At this time, joint releases or nerve grafts could be achieved. Frequently this excision of tendons and their remnants resulted in
73
{kind=link}
{kind=link}
75
{kind=link}
76
{kind=link}
a rather marked increase in the passive range of motion of the digit. When the finger was believed to be unreactive and ready for a further-operative procedure, a tendon graft operation was carried out without pulleys. Rather than open all portions of the previous incision, the tendon in these areas was actually burrowed into the subcutaneous space without creating formal pulleys. Three to four weeks after the tendon graft, motion was instituted. The aim was to use either removable rings or the patient’s finger on the opposite hand to act as temporary pulleys until motion within the digit was achieved. After finger motion through the graft was achieved, pulley reconstruction or wearing of a ring for a prolonged period of time could be prescribed. The results were variable, and the process took many months. Usually three operative procedures were required to achieve a functional digit (Butler et al.1968).
Another approach, as reported by Hunter (1965), required Silastic implants and the creation of artificial tendon sheaths. These implants were used in complex injuries that had both a poor tendon bed and poor tendon substance. Considerable difficulty was initially encountered with the implant because of foreign body reaction, infection, and the development of synovitis. However, surgeons were eventually able to use the artificial tendon extensively to create a better bed for tendon grafting in severely damaged hands. The artificial tendon was placed in the poor tendon bed, joint releases were carried out as indicated, and nerve repairs or grafts done at the same time, if indicated. Three to six months after the insertion of the artificial tendon and achievement of a functional range of passive motion, a tendon graft was pulled into the artificial sheath and anchored proximally and distally. This gave more predictable results than the scar excision technique and was used by many surgeons in Army hospitals throughout the United States.
77
The Wrist
The wrist is the key to hand function because a mobile painless wrist is required for normal hand function. Penetrating injuries of the carpus and the distal radius created highly localized problems that compromised hand function even in the absence of significant tendon or nerve injury. The penetrating injury in this area of eight carpal bones damaged considerable articular surface and this, coupled with ligament injury and bone loss, often brought about intercarpal subluxations and dislocations. In addition, because of the proximity of bone and tendon and of bone and nerve in this area, foreign bodies and bone fragments were sometimes displaced into the carpal tunnel, where they caused secondary compression of the median nerve or interference with flexor tendon gliding.
In Vietnam, the initial management of the penetrating injury of the wrist was similar to that of other hand injuries. However, in the wrist area, anatomic exposure was extremely important. Considerable carpal injury could be created by even a small fragment with small entrance and exit wounds. Exploration of this limited area through the wounds of entrance and exit was difficult. Consequently, with carpal injuries, a physiological volar exposure generally was carried out. This exposure brought about release of the carpal tunnel, protection of the median nerve during debridement, and also permitted wound exploration as indicated. After debridement, some type of external immobilization was usually imposed to prevent the volar flexed position of the wrist. The wound itself was managed as were other hand wounds, preferably with delayed primary closure.
Prolonged splintage of these fractures with the wrist in slight dorsiflexion or at least avoiding volar flexion was usually the method of management. This method allowed the osseous injury in the wrist to consolidate and permitted emphasis to be placed on movement of flexor and extensor tendons with full mobility of fingers and thumb. If required, elastic traction was applied to aid in both flexion and extension of the fingers. In the early years of the Vietnam War, immobilization for these injuries was believed to be only a matter of a few weeks. Later it became obvious that the longer the immobilization, the more stable the wrist would be, and the increased stability would permit the patient heavy use of the wrist and fingers with little discomfort. In certain cases of extreme articular damage with bone loss, surgeons attempted to use Silastic implants in the wrist joint. However, the irregular bone loss gave poor Silastic support and made the maintenance of a mobile and painfree wrist difficult, even with good motor control. The generally excessive instability in the wrist then resulted in poor distal finger function.
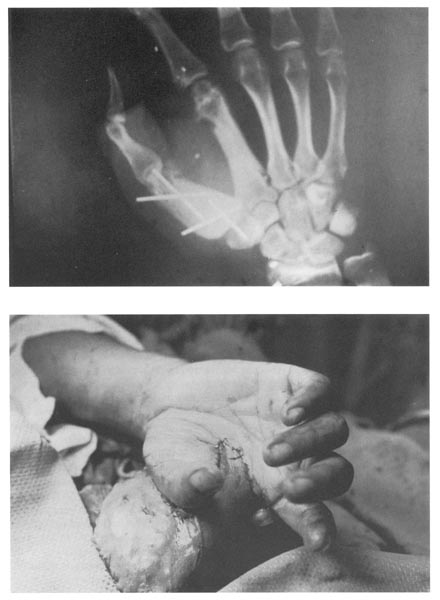
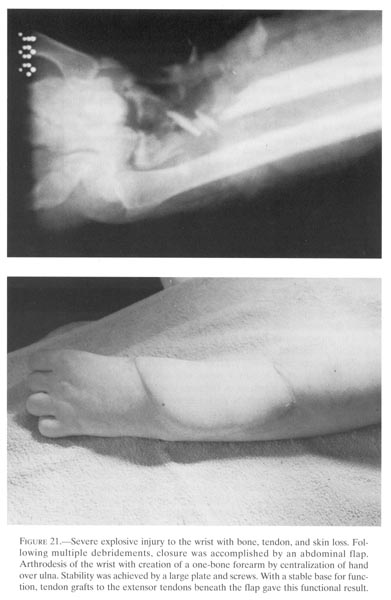
It soon became clear that arthrodesis of the wrist was a far superior method of management for the severe open distal radius and carpal injury. But the bone loss problem made arthrodesis of the wrist difficult in certain instances. The use of late internal fixation in the form of a compression plate, with or without additional bone graft, allowed minimal external immobilization. With this internal stability, additional procedures could be carried out at the time of wrist arthrodesis (fig.21). Tenolysis of the extensor tendons with metacarpophalangeal joint release could be carried out easily at the same time, without concern for loss of stability of the arthrodesis. Postoperatively, traction loops to bring about metacarpophalangeal flexion could be added without particular difficulty. The arthrodesis with or without
78
{kind=link}
79
{kind=link}
80
{kind=link}
the compression plate was the most frequentlyemployed method of management for thesignificant penetrating injury to the carpus or distal radius.
CONCLUSIONS
Inasmuch as orthopedic residency training requires at least some exposure to hand surgery, a surgeon with an interest and training in surgery of the hand was usually available in Vietnam to treat the patient with a hand injury. Guidelines from other surgeons emphasized the initial management of the wounded hand, the importance of debridement without primary closure of the wound, and early (three to seven days) evacuation to a facility for definitive management.
In offshore hospitals, where physicians with interest and training in hand surgery also managed the hand injured-patients, the second operative procedure was carried out. At this point, achieving skeletal stability was most important. With skeletal stability achieved with Kirschner wires or spacer wires, motion of joints and tendons could be instituted. After the patient’s second procedure, an occupational therapist helped him to improve active hand motion with exercise and splintage.
Upon arrival in CONUS, the patient was usually sent to a specialized treatment center for reconstructive hand surgery. These centers, established in designated general hospitals to improve the overall management of those patients, were staffed by orthotists, occupational therapists, and usually graduates of the hand fellowship program at Walter Reed General Hospital. All in all, wounded soldiers with hand injuries received excellent care throughout the treatment chain, from the point of initial wounding to the large military medical center.
81
REFERENCES
Aymard, J. L. 1917. Nasal reconstruction.Lancet2:888-91.
Bakamjian, V. Y. 1965. A two-stage method forpharyngoesophageal reconstruction witha primary pectoral skin flap. Plast.Reconstruct.Surg. 36:173-84.
Bunnell, S. 1945. Suggestions to improve the early treatment of hand injuries. Bull. U.S.Army Med. Dept. 88:78-82.
Burkhalter, W.E.; Butler, B; Metz, W.; and Omer, G. 1968. Experiences with delayed primary closure of war wounds of the hand in Vietnam. J. Bone Joint Surg. (Am) 50:945-54.
Butler, B., Jr. 1969. Initial management of hand wounds. Milit. Med.134:1-7.
Butler, B., Jr.; Burkhalter, W. E.; andCranston, J. P. III. 1968. Flexor tendon grafts inthe severely scarred digit. J. BoneJoint Surg. (Am) 50:452-57.
Churchill, F. D. 1944. The surgicalmanagement of the wounded in the Mediterraneantheater at the time of the fall of Rome. Ann. Surg.120:268-83.
Curtis, R. M. 1971. Surgery of the hand, itspast, present, and future. J. BoneJoint Surg.(Am) 53:810-12.
Cutler, C. W., Jr. 1945. Early management ofwounds of the hand. Bull. U.S. Army Med.Dept. 85:92-98.
Hand surgery. Surgery inWorld War II. SeeMD-HS.
Hunter, J. M. 1965. Artificial tendons--theirearly development and applications. J. BoneJoint. Surg. (Am) 47:631-32.
Jabaley, M., and Peterson, H. Early treatmentof war wounds of the hand and forearmin Vietnam. Ann. Surg. 177:163,1973.
McGregor, I. A., and Jackson, I. T. 1970. Theextended role of the delto pectoral flap.Br. J. Plast. Surg. 23:173-85.
MD--HS--Medical Department, U.S. Army. 1955. Handsurgery. Surgery in World War II. Washington: GPO.
MD--WW--Medical Department, U.S. Army, 1927. The Medical Department of the UnitedStates Army in the world war, vol. II. pt.1 Washington: GPO.
The medical and surgical history of the War of the Rebellion. See MSHWR.
The Medical Department of the United States in the world war. See MD-WW.
MSHWR--U.S. Surgeon General’s Office. 1876. The medical and surgical history of the War of the Rebellion, vol.2, pt.2. Washington: GPO.
Reid, R. L. 1979. Hand surgery and themilitary: A historical review. Milit. Med.144:385-8.
Tanner, J. C., Jr.; Vandeput, J.; and Olley,J. F. 1964. The mesh skin graft. Plast.Reconstruct.Surg. 34:287-92.