



Chapter 5
WOUNDS OF THE FOOT
Colonel Anthony Ballard, MC, USA (Ret.)
While foot disease and injuries were rarely life threatening during the Vietnam conflict, they did result in prolonged morbidity and great loss of manpower. A considerable amount of this morbidity can be attributed to inadequate treatment of what appeared to be minor wounds. Many minor foot wounds were ignored by the soldier until a deep infection had become well established and the function of the foot seriously compromised. Medical facilities tended to compound the problem by giving foot wounds the lowest priority and providing treatment that frequently included inadequate debridement.
The majority of orthopedic surgeons serving in the Republic of Vietnam during the early years of the conflict were not trained to carry out the extensive exploration and debridement of the foot necessitated by many of the wounds. Because of a general unfamiliarity with the plantar compartments of the foot and fear of plantar incisions, attempts at wound debridement were frequently carried out through medial, lateral, or dorsal, rather than plantar approaches. However, these techniques were inadequate for complete debridement. Moreover they placed the tendons and neurovascular structures of the plantar aspects of the foot in jeopardy.*
TREATMENT PRINCIPLES
Preoperative clinical and radiographic assessment of the foot to determine the extent of damage to the nerves, vessels, and bony architecture was the first step in treatment. Anteroposterior, lateral, and oblique roentgenograms of the foot and ankle were taken to evaluate the extent of damage to the bones and joints. If the injury was secondary to a fall from a height or to explosive forces directly beneath the foot, fractures of the femoral neck of lumbar vertebrae were suspected and roentgenograms also were made to evaluate these areas.
The extent of damage to the nerves of the foot was determined by checking the pinprick sensation of the areas supplied by the major nerves. Anesthesia over the medial plantar surface of the foot indicated damage to the medial plantar nerve, while altered sensation over the lateral one-fourth of the sole and fourth and fifth toes indicated lateral plantar nerve damage. Anesthesia of the heel pad was secondary to injury to the calcaneal branch of the posterior tibial nerve.
Assessment of vascular injury was critical. Surgeons in Vietnam recognized that the foot was supplied with blood through extensive anastomosis of the dorsalis pedis, posterior tibial, and peroneal arteries. Although interruption of any of these
* Unless otherwise indicated,anatomicaldiscussions in this chapter are based on Anatomy of the human body(Gray 1959).
84
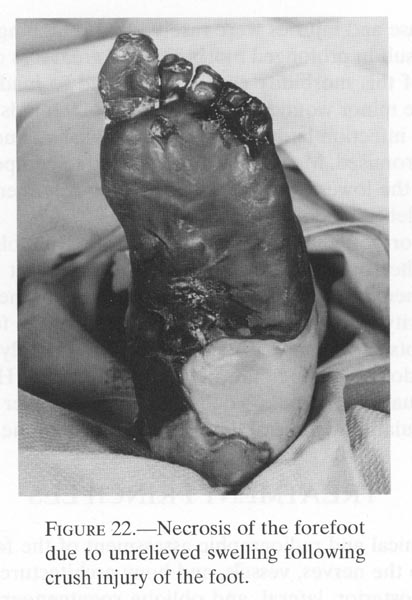
vessels usually would not jeopardize the survival of the foot, injuries that caused extensive swelling within the deep compartments of the foot could compromise the blood supply through all three vessels, resulting in reduced vascularity and either loss of the foot or deep extensive fibrosis (Omer and Pomerantz 1972). In particular, hindfoot dislocations, crush injuries, and injuries resulting from explosions directly beneath the foot were more likely to cause extensive vascular damage and compromise more than were gunshot wounds (fig.22).
FIGURE 22.- Necrosis of the forefoot due to unrelieved swelling following crush injury of the foot.
{kind=link}
Analysis of vascular injury was made primarily by clinical evaluation of skin color, temperature, and palpable pulses. In some centers, ultrasonic flow detectors, angiography, and plethysmography supplemented clinical evaluation of circulation (Lavenson, Rich and Strandness 1971; Strandness and Bell 1965; Rusher et al. 1967). The ultrasonic flow detector could determine arterial flow through the digital arteries of the toes even in a grossly swollen foot.
The procedure for foot debridement was designed to remove contaminants and necrotic tissue as well as to open the deep compartments to release pressure and thus preserve viability of the tissues. Viability of muscle was determined by its color, contractility, capillary bleeding, and consistency (CINCPAC-3 1969, 15-19). Of these four viability determinants, muscle consistency was the most reliable. A necrotic muscle rapidly lost its firm rubbery consistency and had a mushy feeling when grasped with forceps. This finding was usually present at the time of initial debridement.
Neither muscle contractility nor muscle color were reliable signs of viability. If the debridement was carried out under tourniquet hemostasis, after several pinches
85
with the forceps, the muscles would no longercontract and could be mistaken for tissue nolonger viable. At the time of initial debridement, muscle color wasalso not a reliable indicator ofviability because muscle tissue damaged either directly or indirectlyby the passage of a missilewas altered by diffuse blood about the fibers. Although this gave themuscle an unhealthy hue, inmany instances the majority of the muscle fibers retained theirviability.
Wherever possible, lacerated common and proper digital nerves were debrided of contaminants and the free proximal ends were left buried deep in the foot surrounded by soft tissue. Repair of the nerves was not attempted during the initial debridement. Loss of function of the medial plantar nerve rendered three-fourths of the plantar surface of the foot anesthetic and, in some instances, badly compromised foot use. If skin closure over the medial plantar nerve was feasible, it was repaired proximal to its branching. After debridement of contaminants and necrotic tendon tissue, lacerated tendons were left unrepaired.
Since the foot could survive evacuation if either the dorsalis pedis or posterior tibial artery remained patent, except in a few instances, vascular repair distal to the midcalf was not attempted in the war zone. However, if both vessels were disrupted, they were ligated and viability of the foot was determined at a later date. (Lavenson, Rich and Strandness 1971). Amputation subsequently became necessary in some cases because of a vascularity of the remaining part. In some of the CONUS medical centers, microvascular repair of vessels was done, but even when operating microscopes, fine nonabsorbable sutures, and a well-trained surgical team were all available, patency of the vessel was difficult to maintain.
Surgeons treated the damaged skeleton of the foot by removing all small, contaminated, and isolated bone fragments, leaving those larger fragments still attached to soft tissue in place to serve as subsequent bone grafts. This procedure was especially important in the first metatarsal region. Internal fixation of bones to maintain alignment was not performed during the initial debridement. In appropriate cases, it could be performed at subsequent operative procedures when the wound was determined to be clean (CINCPAC-3 1969, 68).
Following the surgical removal of contaminated and necrotic tissue, wounds were thoroughly flushed with saline or an antibiotic solution. This was done by placing the tip of the irrigating device into the depth of the wound and, with gentle pressure of the fluid, floating loose debris to the surface. In some treatment facilities in Vietnam, attempts were made to cleanse the wound with a dental instrument that produced pulsating jets of water under pressure. This method was controversial. Its advocates contended that this was an effective method of removing superficial contaminants from tissue while others believed that this resulted in further imbedding or spreading of the contaminants throughout the wound area. Although the pulsating water method was not widely used in the treatment of foot wounds in Vietnam, further experience has demonstrated the efficacy of pulsating lavage.
After debridement, wounds were left open and dressed with fine mesh gauze over the raw surfaces. The lower leg and foot were encased in bulky dressings. Drains proved to be ineffective and were discouraged (CINCPAC-3 1969, 15-19). Splints were applied from the knee to beyond the tips of the toes to stabilize the underlying fractures and injured soft tissues. All wounds were inspected five to seven days after debridement. If depths of the foot had been entered by either the wound-
86
ing device or the surgeon, this second look was done in the operating room with appropriate anesthesia, tourniquet hemostasis, adequate lighting, and surgical instruments. The entire wound was reexplored and any remaining necrotic tissue excised. Only if the wound was clinically clean did surgeons perform necessary internal fixation of fracture, nerve repair, and closure.
The foot was immobilized and elevated for ten to fourteen days after injury. Crutch ambulation was started when the edema had begun to subside. Weightbearing (utilizing patellar tendon bearing casts to reduce the amount of weight borne by the plantar surface of the foot) was dictated by the extent and type of fractures. After skeletal stability had been achieved, weightbearing was helpful in reducing the morbidity resulting from the extensive disuse osteoporosis.
Primary closure of war wounds of the foot should rarely be considered (Omer and Pomerantz 1972). Delayed primary closure at five to seven days allowed reassessment of debridement and its adequacy without a significant delay in healing and was generally safer than primary closure. Even then, delayed primary closure was done only if the sound edges of the wound could be brought together and sutured without tension. Relaxing incisions or undermining edges of the skin to close the wound was not recommended because they resulted in a high rate of wound breakdown and increased skin loss. Delayed primary closure was usually applicable only to wounds of the dorsum of the foot and was not recommended for plantar wounds, since wounds on the plantar surface or sides of the foot without large areas of skin loss closed readily by secondary intention (Omer and Pomerantz 1972).
The skin over the ball of the foot was frequently associated with damage to the adjacent toes. When this occurred, the toes were filleted and the skin was used to cover the weightbearing area of the distal forefoot. This skin retained its sensibility and held up well with continued use. Incidence of deep infection of these wounds was lower with this approach than it was with delayed closure.
When feasible, wounds with large areas of skin loss were closed at ten to fourteen days with split-thickness skin grafts. The mesh graft proved to be one of the most effective methods of secondary wound closure in treating Vietnam casualties with skin loss of the feet.
Pedicle grafts were rarely indicated in the treatment of foot wounds, since the failure rate of resurfacing the foot with this method was high. Even though they could provide a pad over the weightbearing areas of the forefoot and heel, pedicle grafts were anesthetic and did not wear well with weightbearing and use. At Fitzsimons General Hospital in Denver, Colorado, between 1966 and 1970, a pedicle graft was used in 4 of the104 patients treated for open wounds of the foot (Ballard 1966-70). In three, the graft was designed to replace the loss of the heel pad; in the fourth, it was designed to replace the skin over the ball of the foot. Three of the pedicle grafts failed, and the procedure was aborted after the first stage in the fourth case because the wound had already closed by granulation tissue, before the pedicle was ready to be transferred.
Case 1: A twenty- three-year old soldier sustained an injury to the right foot when he stepped on a land mine in Vietnam. This resulted in a comminuted fracture of the calcaneus and loss of the major portion of the heel pad. At initial debridement on 2 March 1967, the calcaneus was removed and the wound was left open. On 16 March 1967, a pedicle flap was raised on the left calf and was implaced on the left heel on 6
87
April 1967. The wound became grossly infectedand the entire pedicle flap was lost. The patientunderwent a below-the-knee amputation on 2 June 1967 and was ambulatorywithout externalsupport or discomfort three months later.
Case 2: A twenty-year-old soldier sustained a bullet wound in the left heel in Vietnam on 29 December 1965. This resulted in a comminuted fracture of the calcaneus and loss of the posterior aspect of the heel pad. After initial debridement, which included removal of portions of the calcaneus, the wound was left open. A split-thickness skin graft was used to close the wound on 25 January 1966. A cross-leg pedicle graft was applied to the left heel on 25 February 1966. The graft had a 75 percent take, and the remaining area granulated in. Sixteen months later, the patient returned to the hospital because of repeated breakdown of the pedicle flap and continuous pain with ambulation. During that period, the patient required the use of crutches or a cane. Three months after a below-the-knee amputation, the patient was ambulatory in a patellar tendon bearing prosthesis, without external support and without pain.
Case 3: A twenty-year-old soldier sustained a gunshot wound to the right heel on 6 January 1968. In addition to loss of most of the heel pad, the patient had a comminuted fracture of the calcaneus. Most of the calcaneus was removed at the initial debridement. On 8 January 1968, a pedicle graft from the left calf to the right heel was done. Five days later there was purulent drainage from beneath the pedicle graft and most of the pedicle graft was nonviable. The entire graft was removed. On 20 January 1968, a mesh split-thickness skin graft was applied to the heel defect, with a 90 percent take. The remaining portion of the open wound closed by granulation. By 19 August 1968, the wound was completely closed and the patient was ambulatory, wearing a special shoe with a soft heel insert and using a cane. The patient returned to the hospital in March 1969, because of constant pain in the foot and repeated breakdown of the heel area. A below-the-knee amputation was done on 4 April 1969. By 16 June 1969, the patient was ambulatory without external support in a patellar tendon bearing prosthesis. He had no pain in the extremity at that time and continued to be a good prosthesis wearer.
Case 4: A twenty-four-year-old soldier sustained an injury to his left foot on 30 November 1966, when he accidentally discharged a 12 gauge shotgun into the dorsomedial aspect of his forefoot. In addition to destruction of the distal end of the first metatarsal bone and first metatarsophalangeal, the patient had a 3 x 3 cm. skin defect over the plantar weightbearing surface of the foot. Following initial debridement, the wounds were left open and subsequently remained clean. On 5 January 1967, when the flap was ready for insertion into the foot, the plantar wound had completely healed, and the patient was ambulating without discomfort. The pedicle flap procedure was aborted.
SPECIFICINJURIES
PunctureWounds
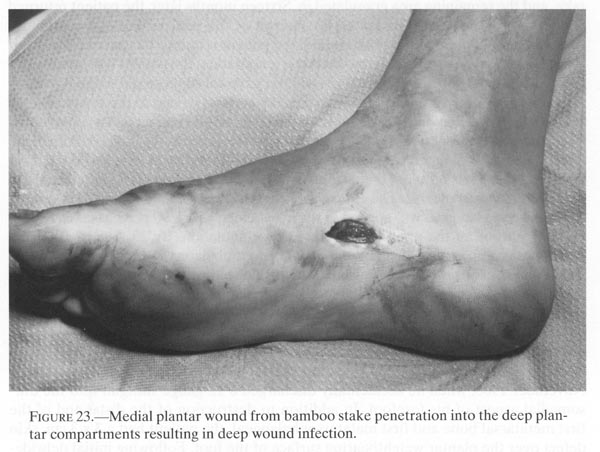
The enemy found an inexpensive and effective means of temporarily inactivating a large number of American troops through the use of sharpened, sometimes fire tempered, bamboo stakes. These sticks, pushed into the ground at an angle, were hidden by the high grasses and underbrush especially prevalent in the highlands area of Vietnam. These devices could puncture the fabric sides and rubber
88
soles of the jungle boots worn by theAmerican soldier and enter the foot to various depths. Theresulting wound was usually a small (1 cm.) innocuous appearinglaceration on the side orplantar surface of the foot (fig.23). Early in the Vietnam conflict,since the potentially seriousnature of these wounds was not fully appreciated, the treatment oftenwas not effective. Thedevastating effectiveness of this simple weapon was recognized onlyafter many patientsreturned to the medical facilities with deep infections of the foot.These patients required weeks,and sometimes months, of hospitalization; some acquired prolonged orpermanent disability.
{kind=link}
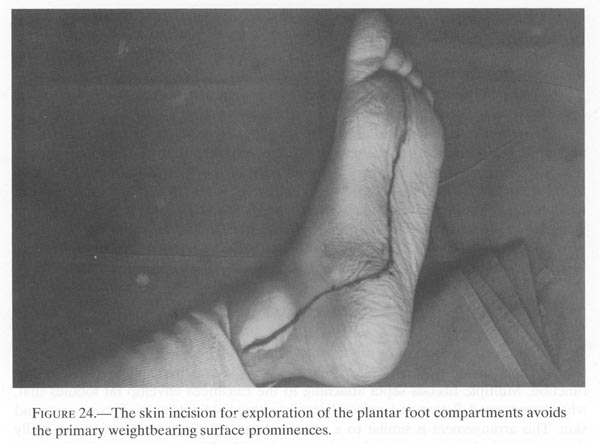
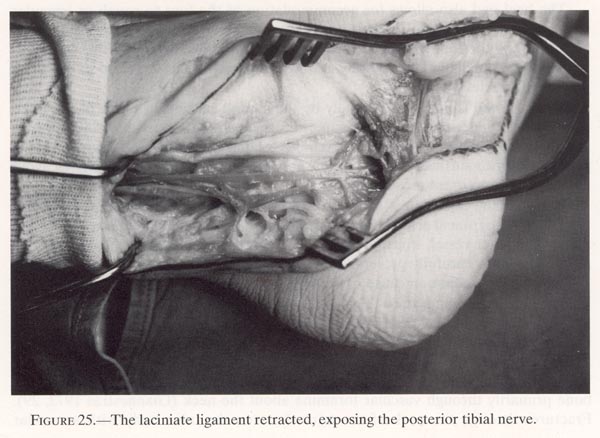
A thorough investigation was conducted concerning the characteristics of these puncture wounds, the most efficacious methods of preventing potential morbidity, and their effective management. Microscopic examination of the tissue taken from along the wound tracks revealed multiple small retained slivers of bamboo surrounded by microabscess formation. Once this type of damage was recognized, a more vigorous treatment program was instituted (figs.24 and 25). It consisted of:
(1) longitudinal incisions extending the wound or separate anatomic incisions on the nonweightbearing plantar surface, thus allowing for exploration in the deep compartments of the foot(2) complete excision of contaminated tissue adjacent to the wound track throughout its length (3) thorough irrigation of the wound with saline solution, flushing out clot and retained foreign bodies
89
{kind=link}
FIGURE 25.- The laciniate ligament retracted, exposing the posterior tibial nerve.
{kind=link}
90
(4) with the wound left entirely open after the initial debridement, application of a bulky pressure dressing, and elevation of the foot for ten to fourteen days postoperatively (5) intravenous antibiotics, usually 10 to 20 million units of penicillin, preoperatively and for the first five days postoperatively (6) tetanus toxoid boosters preoperatively, and reexamination of the foot in the operating room five to seven days after initial debridement.
If there was no clinical evidence of infection, many of these wounds were closed at the second look operation. Despite these efforts, many of the plantar wounds that had penetrated into the deep compartment of the foot subsequently became infected and broke down. As more experience was gained with this injury, most of these wounds were left open to heal by secondary intention. This provided an open track for ready egress of blood and purulent material. The incision on nonweightbearing areas of the plantar surface of the foot healed well by secondary intention, leaving a thin-line scar that was both cosmetically and functionally acceptable.
Hindfoot Wounds
The hindfoot, consisting of the talus, calcaneus, and heel pad, absorbs the initial shock of impact in the stance phase of gait. The heel pad is remarkably designed for this function. Multiple fibrous septa attaching to the calcaneus envelop fat lobules that, when compressed, flatten and expand laterally within the limits of the fibrous septa and skin. This arrangement is similar to a pneumatic tire. If injury or infection has badly damaged the fat lobules and they have been replaced by fibrous scar tissue, the heel pad loses its shock absorbing qualities and functions like a deflated pneumatic tire.
The heel pad also allows for accommodation of the foot to rough or irregular surfaces and is effective in limiting friction between the skin and the shoe or ground, when the foot changes direction of travel. It does this by shifting for a limited distance, medially and laterally, a function sometimes referred to as the third joint of the ankle.
The heel pad is innervated largely by the medial calcaneal branch of the tibial nerve, which pierces the posterior superior aspect of the laciniate ligament to run subcutaneously alongside the distal Achilles tendon and enters the heel pad on its medial posterior surface. Incision in this area should be planned carefully to avoid injury to this important sensory nerve.
Blood to the heel pad is supplied from anastomoses of the lateral calcaneal branch of the peroneal artery and the medial calcaneal branch of the posterior tibial artery. The latter vessel, which provides the major portion of the flow to this anastomosis, should be carefully preserved when incisions in this area are made. Damage to this vessel is a common cause of necrosis of the heel pad in Syme’s amputations.
The talus is also important to gait for it not only transmits all of the body weight to the foot but also serves as a center of motion around which most of the dorsiflexion plantarflexjon and inversion-eversion occur. The talus has no muscular attachments, so its only connection to adjacent structures is by synovial membrane, articular capsules, and ligaments. The talus has a precarious blood supply that enters the bone primarily through vascular foramina about the neck (Giannestras 1973, 29). Fractures through the neck of the talus threaten the talus body with avascular
91
necrosis (Hawkins 1970). The talusarticulates with four bones: tibia, fibula, calcaneus, andnavicular. Damage to any one of these articulations can result inalteration of gait and inability ofthe foot to accommodate to irregular surfaces.
In Vietnam casualties, badly comminuted open fractures of the talus were treated by initial talectomy. Any large fragments left behind after debridement, except possibly the talar head and neck, were found to sequester and became a source of chronic infection (Hawkins 1970). The most useful approach for debridement of the talus or talectomy was an anterior lateral ankle incision. This allowed dissection completely around the talus. The skin incision began 2 to 3 inches (5 to 7 ½ cm.) above the ankle joint medial to the fibula and was carried distally over the superior aspect of the calcaneal cuboid joint to the base of the third or fourth metatarsal. If possible, the skin incision was altered to incorporate the wound. If this was not feasible, the entry and exit skin wounds were debrided separately, with the internal debridement through the elective incision.
Then, the transverse and cruciate crural ligaments were divided in the direction of the skin incision. The ankle joint capsule was excised anteromedially and laterally. The fragmented talus was excised, leaving the head and neck, if possible. Care was taken to preserve the dorsalis pedis artery, since a penetrating gunshot wound of the hindfoot frequently damaged the posterior tibial and peroneal vessels. After debridement, the wounds were left open and were dressed, and the foot was splinted for stability.
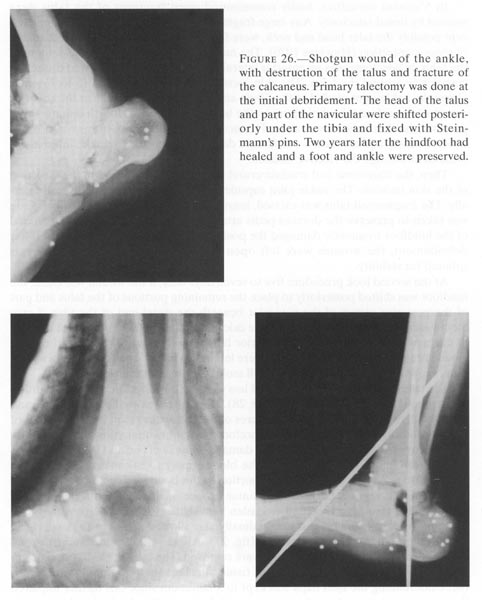
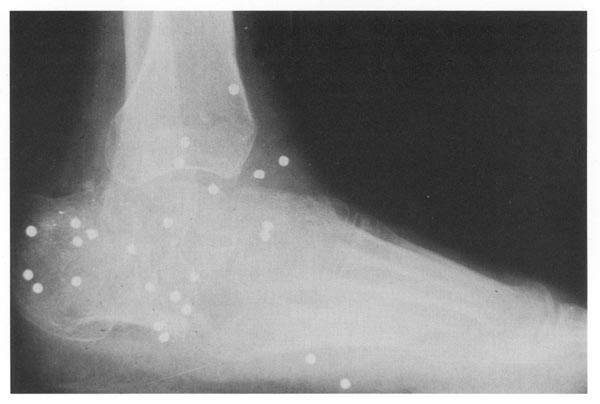
At the second look procedure five to seven days later, if the wound was clean, the hindfoot was shifted posteriorly to place the remaining portions of the talus and part of the posterior aspect of the navicular beneath the distal end of the tibia. Large Steinmann pins were driven through the calcaneus into the tibia to stabilize the foot in this new position (fig.26). The anterior lateral incision was closed but the other wound areas were left open. The pins were left in situ for six weeks and following pin removal, ambulation was begun in a well molded patellar tendon bearing cast.
The calcaneus forms the shorter and less yielding posterior limb of the longitudinal arches of the foot (Giannestras 1973, 28). It articulates with the talus, above, and the cuboid, distally. Intraarticular fractures of the calcaneus result in compromise of the hindfoot inversion-eversion and forefoot pronation-supination. Extraarticular fractures are frequently associated with damage to the heel pad and the problems resulting from injury to this structure. The blood supply to calcaneus is multisource and extensive. Aseptic necrosis of any portion of this bone is uncommon.
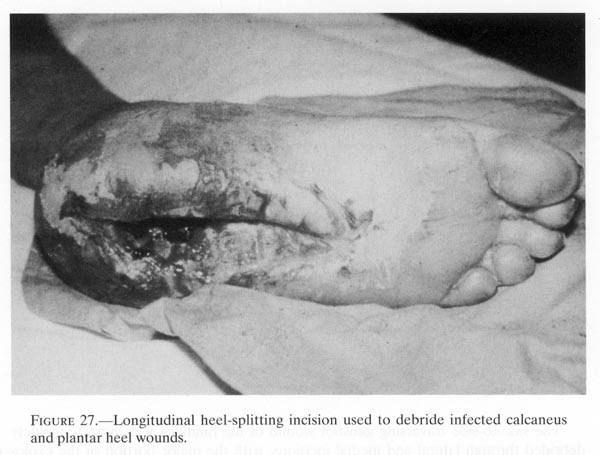
Penetrating wounds through the plantar surface of the heel pad were explored and debrided through a modified Gaenslen heel-splitting incision (Gaenslen 1931). This approach split the fat pad longitudinally and allowed access to the underlying comminuted contaminated calcaneus (fig.27). All identifiable contaminants and small fragments of bone and cartilage were removed. The lateral, medial, and posterior shells of the calcaneus with its soft tissue attachments were preserved, if possible. Undermining the heel flaps was kept to a minimum since this further impaired the neurovascular supply to the structure and destroyed the shock-absorbing capacity of the heel pad. Internal fixation of fracture fragments of the calcaneus was considered contraindicated because of the high incidence of osteomyelitis. Following surgical debridement, the wound was flushed with normal saline or an antibiotic solution and left open. No attempt at secondary closure was made in these wounds.
92
{kind=link}
93
{kind=link}
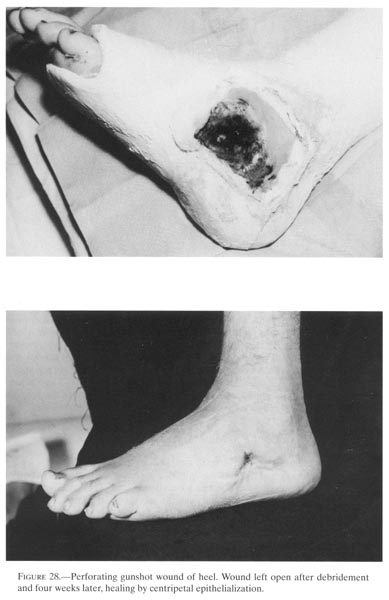
The side-to-side traversing gunshot wound of the hindfoot was most adequately debrided through lateral and medial incisions, with the major portion of the exploration through the lateral incision. This procedure avoided further damage to the medial calcaneal branches of the posterior tibial nerve and to the tibial artery that supplied the heel pad. A medial incision through the fat pad was prone to transect the calcaneal branches of the posterior tibial nerve, rendering the majority of the heel pad anesthetic. These wounds were left open, appropriately dressed and splinted. Healing of wounds of several centimeters in size occurred quite readily by ingrowth of surrounding epithelium over the framework of the underlying granulation tissue (fig.28). Well molded circular casts were applied, and ambulation was allowed as the wound condition permitted. A patellar tendon-bearing cast applied over a one inch (2.5 cm.) thick sponge rubber pad placed over the plantar surface of the foot helped to decrease the forces transmitted through the hindfoot and allowed for early ambulation.
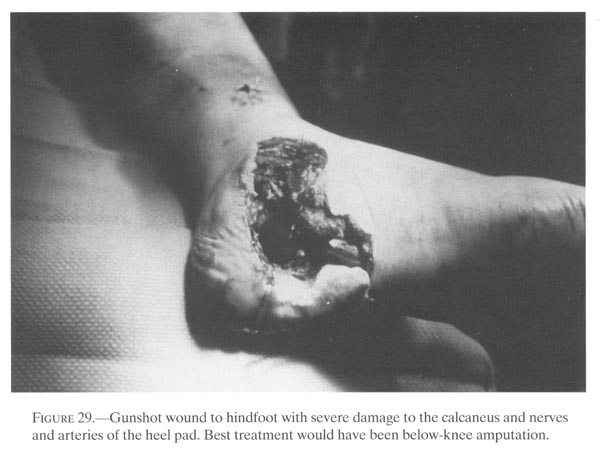
The final hindfoot wound discussed in this section is the injury in which the heel pad and the underlying bones were irreparably damaged. The sentiments of Hampton after World War II are still applicable:
Compound fractures of the tarsus, especially when the os calcis was involved, were a source of prolonged disability. Functional results were seldom optimal and were often actually poor. Although conservatism was ordinarily practiced, many orthopedic surgeons, when they reviewed their experience, wondered whether this had been the wisest course. They could recall many cases of extensive bony disorganization and persistent infection, with continuing destruction of bone or loss of weightbearing skin on the plantar surface of the heel, in which conservative measures had been employed but in which amputation might have been the wiser course. In some of these cases, amputation was eventually performed in the Zone of Interior but only after the soldiers had been hospitalized for months and even years.
{kind=link}
If Hampton’s advice had been followed by the surgeons treating patients with this injury sustained in Vietnam, rehabilitation of the patient would have been more rapid and successful. Amputation should be done before the surgeon and the patient become so emotionally attached to the foot that their goals become unrealistic. The amputation, therefore, should be done at the initial debridement or at the second look operation (fig.29).
Statistics on foot injuries during the Vietnam War are not available for analysis; therefore, the results of treatment of hindfoot injuries from a major hospital are reported as representative of this type of wound. Twenty-four patients with twenty-six significant hindfoot injuries were treated at Fitzsimons General Hospital during 1966-70 with results as follows:
Returned to:
Duty w/o symptoms.................................................................................. 2
Limited duty w/symptoms........................................................................ 5
Total returned to duty: .......................................................................... 7
Discharged as unfit for duty:
Ambulatory without assistance or pain...................................................... 1
Ambulatory with pain and assistance......................................................... 8
Early amputation (first hospitalization)........................................................ 3
Depayed amputation (subsequent hospitalization)....................................... 5
Total Discharged...................................................................................17
Total Patients................................................................................. 24
95
{kind=link}
96
{kind=link}
In general, these patients with hindfoot injuries were treated until final disposition so that the end results reported here probably represent their eventual condition. The hospital stay for this group of patients ranged from 28 to 625 days, averaging 246 days. Of the 17 patients medically unfit for further military service and discharged, 8 had significant pain and required external support for ambulation; 1 had a spontaneous ankle fusion, denied pain, but had an altered gait; 3 had below-knee amputations early in their stay at the hospital; and 5 returned to the hospital within three years and requested below-knee amputations, which were done.
Midfoot and Metatarsal Area Wounds
The midfoot, composed of five small tarsal bones, roughly resembles a wedge with the apex laterally and the base medially. Through and about these five bones, part of the movements of pronation and supination occurs. They augment the inversion and eversion that take place through the subtalar joints. These bones form the apex of the longitudinal arch of the foot (Grant 1952, 444-48). Surgically, the dorsum of the midtarsal and metatarsal areas was approached through appropriate longitudinal incisions.
The deep plantar artery joins the lateral plantar artery from the posterior tibial artery to form the plantar arterial arch. At the base of the second and third metatarsals the artery branches into the first dorsal metatarsal artery and the deep plantar artery. Care was taken to identify and preserve the dorsalis pedis artery as it
97
crossed the dorsum of the midfoot lying inturn on the talus, lateral side of the navicular, andsecond cuneiform.
At the second-look operation or at a later date when the wound was determined to be clean, internal fixation with small Kirschner wires was used to align displaced skeletal parts. The Kirschner wires were cut off below the skin so that they could be readily retrieved later. Stability in the position of function gave the best chance of useful future foot function. When the injured tissue stabilized and edema decreased, the initial cast or splints were replaced with a well-molded plaster cast. Weightbearing ambulation was begun when some bone stability had been achieved, usually six to eight weeks after injury. Fractures of the distal metatarsals allowed much earlier weightbearing, usually within a few days of injury. The surgical approach to the plantar surface of this area is described later in this chapter.
At Fitzsimons General Hospital during 1966-70, 60 patients with open injuries of the midfoot or metatarsal areas or both were treated, with the following results:
Return to duty:
Without symptoms............................................................... 4
Limited duty with symptoms............................................... 22
Total returned to duty...................................................... 26
Discharged as unfit for duty:
Ambulatory without significant symptoms............................. 5
Significant symptoms requiring crutch or cane...................... 29
Total discharged............................................................... 34
All patients.................................................................... 60
Most of these patients were treated until a final disposition could be determined. Except for those who returned later for amputation, the results reported here are probably representative of the final results from these types of injuries. The initial hospitalization of this group of 60 patients was from 6 to 839 days, with an average of 193 days. Of 26 patients returned to duty, 22 were asymptomatic and walking with no external support. Four were returned to a permanent limited duty status, and all 4 had symptoms of limited foot motion.
Thirty-four patients were unfit for active duty at the end of their hospitalization. Twenty-nine of this group were symptomatic and required either a cane or crutch for ambulation. Ten of the 29 patients returned to the hospital within 4 years for an amputation of the foot. Whether others of this group went elsewhere for subsequent ablative procedures is not known. Five patients had minimal discomfort and required no external support to ambulate but were unfit for duty because of marked limitation of motion, anesthetic portions of the feet, or significant plantar skin loss.
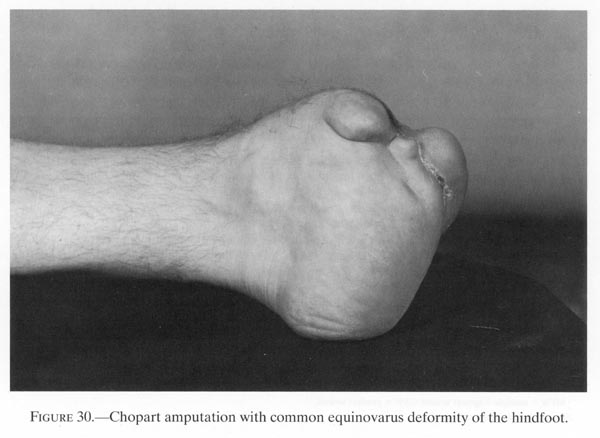
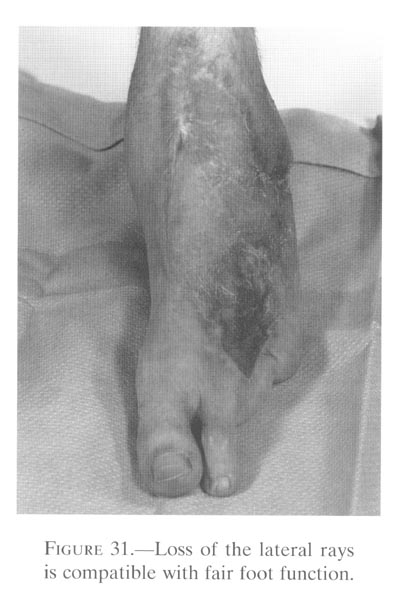
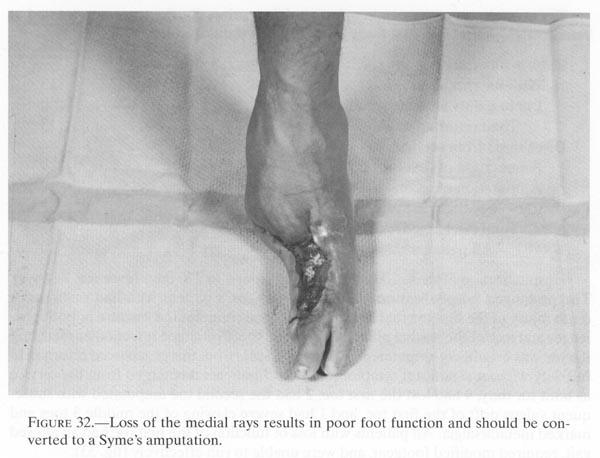
Sixteen of the sixty patients had an amputation of a portion or all of the foot during their first hospitalization (table 3). Two patients who were discharged with Chopart amputations returned to the hospital later because of persistent equinovarus deformity of the stump, poor ambulatory ability, and pain with ambulation (fig.30). Five patients had resections of the outside rays of the foot during their first hospitalization; three had the medial second or third rays resected and two had resection of the lateral two rays (fig.31). Two of the patients with medial ray resections returned to the hospital later for a revision to a Syme’s amputation because of
98
pain and poor ambulatory capacity (fig.32).The final status of the third patient with medical rayresection is not known.
Ten of the patients previously treated at Fitzsimons General Hospital and discharged as unfit for further duty returned to the hospital later for revision of a previous amputation or for a primary amputation (table 4). A Syme’s amputation was done on four of the patients who had previously undergone partial medial foot resections and whose Chopart amputation was unsatisfactory.
Omer and Pomerantz (1972) reported the results of the management of severe open injuries and traumatic amputations of the foot. Of the 410 patients treated from 1966 to 1969 at Brooke General Hospital, San Antonio, Texas, 307 had sustained major foot injuries. Of the 307 patients, 171 (55 percent) had assisted painful ambulation or had elected an amputation by the end of their first hospitalizations (table 5).
Toe Wounds
???In the foot, unlike the hand, stability takes precedence over motion, and bone balance is of greater importance than muscle balance. The foot supports and propels the body forward in an upright posture. The foot functions principally while it is on the ground. The toes press against the sole of the shoe or the ground and establish a point from which forward propulsion occurs. The toes also provide protection for the metatarsal heads. Both in function and structure, the great toe differs from the lesser
99
FIGURE 30. - Chopart amputation with commonequinovarus deformity of the hindfoot.
{kind=link}
FIGURE 31. - Loss of the lateral rays is compatible with fair foot function.
{kind=link}
100
toes. While the lesser toes contribute to the stability of the walking base, the great toe is the base from which the body is propelled forward (Kelikian 1965, 27-30).
???A large proportion of toe wounds were self-inflicted by a few soldiers seeking relief from duty. Most frequently, the left foot was involved and, fortunately, the lesser toes were most commonly injured. Despite the high velocity of the rifles used in Vietnam, damage was usually confined to a limited area, probably because the toes offer little impedance to the passage of a bullet and thus little energy was ex-
101
{kind=link}
pended within the part. Throughout theVietnam War, periodic attempts were made to keep thesoldiers with a self-inflicted wound in the zone until they could bereturned to duty.Unfortunately, these wounds took several weeks to heal sufficiently toallow full combat dutyand, if retained in Vietnam, the hospitalized patient could not bereplaced with a more effectivesoldier.
Since the great toe is important in normal gait, every effort was made to preserve its function. After debridement, when the wound was determined to be clean and ready for closure, small Kirschner wires were used to align and stabilize the fractures. The interphalangeal joints of the first toe were fused without great loss of function, but mobility of the metatarsophalangeal joint was preserved, if possible, either by resectional arthroplasty in Vietnam, or, at some CONUS centers, by use of artificial partial or complete first metatarsophalangeal joints. The artificial joint was more stable than the resection arthroplasty and thus provided a better axis around which the muscles of propulsion could work. Implants had no place in the initial surgery of combat casualties and were reserved for reconstruction at a later time in the clean closed wound.
Loss of the first toe was frequently associated with damage to the intrinsic muscles of the foot, leading to a claw toe deformity of the lesser toes. These digits then not only became functionless, but further impaired the wearing of footgear and ambulation. Such patients were much better off with amputation of all toes rather than with the preservation of stiff, deformed claw toes.
102
Twenty patients with open injuries involving, primarily, the toes were treated at Fitzsimons General Hospital from 1966-70 with results as follows:
Returned to duty:
Without symptoms.......................................................................... 13
Limited duty without symptoms...................................................... 0
Total returned to duty................................................................ 13
Discharged from service:
Amputation of first toe.................................................................... 4
Amputation of second toe with hallux valgus.................................... 2
Claw toe......................................................................................... 1
Total discharged.......................................................................... 7
All patients.............................................................................. 20
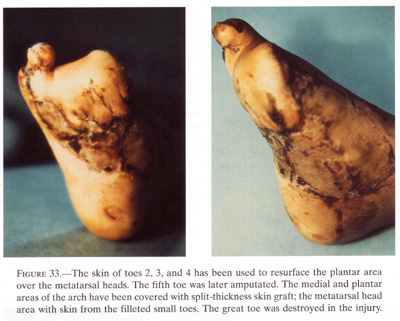
Hospitalization of these 20 patients varied from 4 to 270 days (average, 71 days). The prolonged hospitalization--270 days--was for a patient who had sustained a crush injury of the first toe that resulted in an open comminuted fracture of both phalanges and loss of the medial plantar skin of the toe. Prolonged infection ensued, and the toe was eventually amputated. Thirteen patients from this group were returned to full duty without significant symptoms. Of the 7 patients discharged from the service as unfit for duty, 4 had lost the first toe, 2 had the second toe amputated with subsequent valgus drift of the first toe, and 1 had severe clawing of the middle 3 toes and marked metatarsalgia. All patients with loss of function of the first toe had an altered gait, required modified footgear, and were unable to run effectively (fig.33).
RECOMMENDED OPERATIVE APPROACH TO DEEP COMPARTMENTS OF THE WOUNDED FOOT
A high percentage of patients with open injuries of the foot suffer from prolonged disability. Part of the morbidity resulting from foot wounds sustained in Vietnam was attributable to inadequate initial debridement and subsequent deep foot infections. As experience accumulated, greater use was made of plantar incisions, which facilitated better exposure of the damaged area and afforded greater protection of the undamaged tissues. One particularly useful approach, all or any portion of which may be used to explore the plantar aspect of the foot, is described below.
Initially, an incision is made in the skin1.5 inches (3.8 cm.) proximal and 1 inch (2.5 cm.) posterior to the tip of the medial malleolus. It is extended distally and plantarward to run just in front of the heel pad and then along the longitudinal plantar arch to a point between the second and third metatarsal heads. This incision roughly parallels the course of the medial plantar nerve. The neurovascular bundle lies below the laciniate ligament and posterior to the flexor digitorum longus tendon and can be readily identified behind the medial malleolus. At the superior edge of the laciniate ligament, the tibial nerve divides into two terminal branches, the medial plantar nerve and lateral plantar nerve. The laciniate ligament should be divided over the flexor digitorum longus tendon to avoid damage to the medial calcaneal branch of the tibial nerve, which passes through the superior posterior aspect of the ligament, near its attachment to the calcaneus. The medial and the lateral plantar
103
{kind=link}
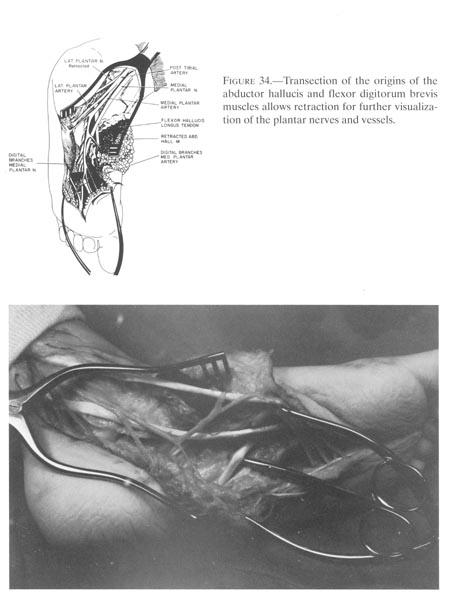
nerves, accompanied by the posterior tibial artery, pass deep to the abductor hallucis muscle and enter the plantar surface of the foot between this muscle and the flexor digitorum brevis. They are best exposed and protected by excising the origin of the abductor hallucis from the calcaneus. A suture ligature placed through the free end of the muscle is used to retreat it distally and medially.
The medial plantar nerve supplies sensation to the medial three-fourths of the sole of the foot. In its course through the foot, the medial plantar nerve lies deep to the flexor digitorum brevis muscle and superficial to all other muscles and tendons of the foot. Beneath the abductor hallucis, the medial plantar gives off two or three muscular branches to the deep surface of this muscle at its middle and distal thirds. Distal to the muscular branches, it divides into three common digital nerves, each of which splits into two proper digital nerves to supply the first, second, third, and one-half of the fourth toes. This terminal division occurs just proximal to the transverse metatarsal ligaments.
The lateral plantar nerve supplies sensation to the lateral one-fourth of the sole of the foot and provides motor branches to most of the deep intrinsic muscles of the foot. Upon exiting from beneath the abductor hallucis muscle, it runs obliquely laterally and distally in the interval between the flexor digitorum brevis muscle and the quadratus plantae muscle. The large lateral plantar artery accompanies this nerve. By transecting the origin of the plantar aponeurosis and flexor digitorum brevis from the calcaneal tuberosity and retracting these structures, laterally, and the abductor hallucis muscle medially, the midfoot course of the medial and lateral plantar nerves and arteries can be exposed and protected. The relationship of these structures is shown in figure 34.
104
{kind=link}
105
A suture ligature placed in the cut end of the flexor digitorum brevis is helpful in retraction and exposure. The medial plantar nerve and artery are retracted medially and the lateral nerve and artery are retracted laterally along with the flexor digitorum brevis. The quadrants Plantae muscle inserting into the flexor digitorum longus tendon now lies in the floor of the wound. Access to the third layer of muscles, to the deep plantar ligaments, and to the bones and joints is gained by transecting the insertion of the quadrants Plantae along with a narrow strip of the flexor digitorum longus tendon and retracting this structure, laterally. By retracting the flexor digitorum longus tendons medially the plantar aspect of the foot, from the calcaneal tuberosity to the mid-metatarsal areas, can be exposed. Running a course from proximal lateral to distal medial in the floor of the wound are the peroneus longus tendon and the deep branch of the lateral plantar artery. The lateral plantar artery unites with the deep plantar branch of the dorsalis pedis artery in the interval between the bases of the first and second metatarsal to complete the plantar arterial arch. Interruption of this vascular arch at any site is compatible with survival of the distal foot, but unrelieved pressure from midfoot swelling will result in necrosis and loss of the forefoot. By extending the incision distally, through the second and third web spaces, the second, third, and fourth metatarsal areas can be explored readily. If exposure of the first or fifth metatarsal is indicated, separate incisions are required.
SUMMARY
The prolonged morbidity and ultimate high incidence of permanent disability of foot wounds were not fully appreciated by many surgeons during the Vietnam War. Inadequate debridement of wounds through inappropriate surgical exposures contributed to the poor results. Some of the lessons learned by experience in treating foot wounds were:
(1) Contamination of the deep plantar compartments of the foot necessitated thorough debridement, which was best done through plantar incisions. These incisions allowed protection and preservation of the important neurovascular structures and removal of contaminants and devitalized tissue.
(2) Wounds causing loss of the heel pad were best treated by early below-knee amputations.
(3) Some medical centers achieved satisfactory results from Chopart-type midfoot amputations by carefully balancing muscle forces about the ankle and with appropriate partial foot prosthesis. However, in most treatment facilities, the majority of patients with severe forefoot wounds were better served by a Syme’s amputation that reduced the length of morbidity, the number of surgical procedures, and prosthetic revisions.
REFERENCES
CINCPAC-3. 1969. Commander in Chief, Pacific. Third CINCPACConference on War Surgery. Tri-service conference conducted at CampH.M. Smith, Hawaii, 20-23 Jan. 1969.
Gaenslen, F. J. 1931. Split-heel approach inosteomyelitis of os calcis. J. BoneJoint Surg.13:759-72.
106
Giannestras, N. J. 1973. Footdisorders: medical and surgical management. 2d ed. Philadelphia: Lea & Febiger.
Grant, J. C. B. 1952. A method ofanatomy: descriptive and deductive. 5th ed. Baltimore:Williams & Wilkins.
Gray, H. 1959. Anatomy of the human body. 27th ed.Philadelphia: Lea & Febiger.
Hampton, O.P. Jr. 1957. Orthopedic surgery in the MediterraneanTheater of Operations. Office of the Surgeon General, Department of the Army. Washington: GPO.
Hawkins, L. G. 1970. Fractures of the neck ofthe talus. J. Bone Joint Surg.52-A:991-1002.
Kelikian, H. 1965. Hallux valgus, allied deformities of theforefoot and metatarsalgia. Philadelphia: W. B. Saunders.
Lavenson, G. S., Jr.; Rich, N. M.; andStrandness, D. E., Jr. Ultrasonic flow detector value incombat vascular injuries. Ann.Surg.102:644-47.
MD-OSMTO--Medical Department, U.S. Army.1957. Orthopedic surgery in theMediterraneanTheater of Operations. Surgery in World War II. Washington: GPO.
Omer, G. E., Jr., and Pomerantz, G. M. 1972.Initial management of severe open injuries andtraumatic amputations of the foot. Arch.Surg.105:698.
Rusher, R. G.; Baker, D. W.; Johnson, W. L.;and Strandness, D. E., Jr. 1967. Clinicalapplications of a transcutaneous ultrasonic flow detector. J.A.M.A. 199: 104-06.
Strandness, D. E., Jr., and Bell, J. W. 1965.Peripheral vascular disease: diagnosis and objectiveevaluation using a mercury strain gauge. Ann. Surg. (Suppl.) 161:3-35.