



Chapter 6
WOUNDS OF JOINTS
Colonel AnthonyBallard, MC, USA (Ret.)
HISTORICALBACKGROUND
Joint injuries have traditionally presented a great challenge to physicians. During the American Civil War over 3,000 cases of knee joint injuries were recorded. The extremity was amputated in 70 percent, and 53 percent died. Open joint wounds during that conflict were treated with hot packs and immobilization of the joint (MSHWR 1883)
Early in the U.S. involvement in World War I, American surgeons treated joint wounds by debridement, irrigation with antiseptic solutions, and immobilization until the wounds healed. While this approach reduced mortality from chronic infections, it resulted in many complications. By the end of the conflict, surgeons had noted that this treatment caused fibrous ankylosis of many joints and that sterilizing the joints with antiseptics was not possible. In fact, many of the solutions used for sterilization, such as ether or a buffered aqueous solution of sodium hypochlorite containing 23 percent active chlorine (Dakin’s solution), were harmful to the synovial lining of the joints. The use of indwelling intra-articular catheters to drain joints was discontinued when it was observed that catheters were causing intra-articular damage.
World War I surgeons also closed joint wounds whenever possible, after which they immobilized the limb for eight to ten days before beginning a passive range of motion with massage. This step partially solved the problem of stiff joints secondary to prolonged immobilization. Although additional treatment measures significantly reduced the infection rate, it still remained a major concern (MD-WW 1927, 317-41).
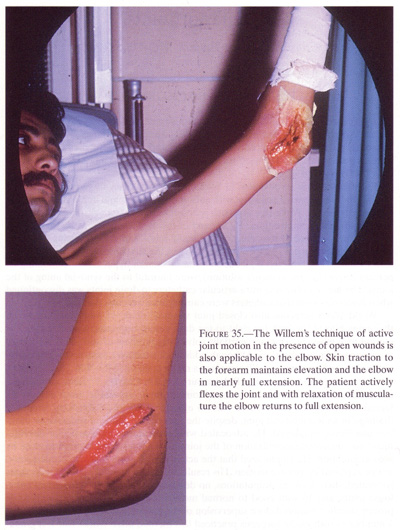
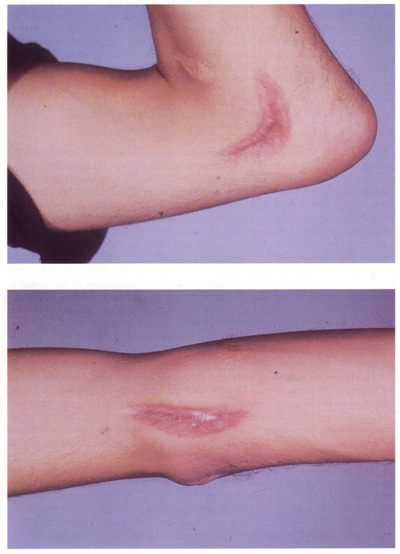
Immediately after the war, a Belgian surgeon, Dr. Charles Willems, proposed a completely different method of treating joint wounds, especially those already infected. He contended that there was no effective way of establishing adequate drainage in an immobilized joint, despite the numbers or kinds of incisions or intra-articular drains employed. He advocated wide arthrotomy, intra-articular debridement, and immediate mobilization of the joint, thus allowing the wounds to close by second intention. He emphasized that the active joint motion that was needed could not be replaced by passive motion. His results were exceptionally good. Of 20 cases so treated, there were no amputations, no deaths, 1 joint resection, 3 residual ankylosed joints, and 16 with good to normal motion. This method of treatment, while proven superior, required close supervision of the patient and was painful. Although a number of orthopedic surgeons practiced this method after World War I, it gradually disappeared as a treatment regimen in the United States (Willems 1919) (fig.35).
The surgeons of World War II were fortunate to have the sulfas as effective chemotherapeutics and, later in the conflict, some antibiotics. The standard treat-
108
{kind=link}
109
FIGURE 35 - Cont
{kind=link}
110
ment for uninfected joints was thorough debridement, closure of the wounds, instillation of penicillin into the joint, and immobilization with splints or casts. Aspiration of the joint and instillation of antibiotics were carried out through a window in the cast. This regimen was continued as long as significant effusion persisted. The wound was immobilized for ten to fourteen days after wound closure, and then an active program of joint mobilization was initiated. The overall results from this treatment method were good. In one series of 198 knee joint wounds so treated, the incidence of infection was 5.4 percent. Complete joint destruction from infection occurred in only 2 percent (MD-OSMTO 1957, 235).
OVERALL POLICY IN THE TREATMENT OF JOINT WOUNDS
Early in the Vietnam conflict, the method of joint wound care varied with the previous experience of the treating surgeon. Since few surgeons spent longer than one year in Vietnam and the receiving PACOM (Pacific Command) or CONUS (continental United States) hospitals provided little feedback, the ability of the surgeon treating the fresh joint wound to assess potential treatment results was poor. Judging from the fragmentary reports available, complications and morbidity increased for the first two months after the usual summer rotation “hump,” when experienced surgeons left to be replaced by new draftees from CONUS. The most consistently followed treatment guidelines available were probably those outlined in the NATO Handbook, “Emergency War Surgery” (1958). These called for early debridement through standard arthrotomy incisions or conversion of the wound to an appropriate approach to allow for wide exposure of the intra-articular structures. All blood clots, foreign debris, and loose bone or cartilage fragments were removed. The capsule or synovium was closed whenever possible, but the skin was left open and the wound closed later (DOD-EWS 1958, 238-40).
By the mid-1960s, the failings of the NATO Handbook’s approach were becoming apparent. Surgeons found that following the guidelines frequently resulted in a significant complication rate and, contrary to the handbook’s warning, exposed cartilage did not rapidly become necrotic. Thus, after 1966, many joint wounds were left open until delayed primary closure 5 to 7 days later. Closure was then done whenever possible, and the joint was immobilized in appropriate splints or plaster casts for transportation to another medical facility. Mobilization of the joint was generally begun 10 to 15 days after the wound was closed. Systemic antibiotics, usually 20 million units of intravenous penicillin a day, were continued for 10 to 14 days after wounding.
In May 1967 in an attempt to evaluate and standardize treatment of war wounds, representatives of all three services met in what subsequently became known as the CINCPAC Conferences on War Surgery. The first of these, held at the John Hay Air Base in the Philippines, included orthopedic surgery representatives from CONUS, Hawaii, the Philippines, Japan, and Vietnam. In general, this study group subscribed to the treatment principles of wounded joints as described in the NATO Handbook (1958).
A method employed by Maj. John Feagin at the 85th Evacuation Hospital in Vietnam aroused some interest (CINCPAC-1 1967, 38-39). His treatment consisted
111
of tight closure of the debrided joint overtwo catheters. Aqueous penicillin was instilled througha continuous drip at 5 million units a day and evacuated through thesecond catheter by gravitydrainage. Surgeons also examined another and similar method fortreating knee joints that hadsustained significant tissue damage, secondary to penetrating wounds.After thoroughdebridement of the wounded joint, the capsule and synovium were tightlyclosed, and aperforated polyethylene catheter was placed through separate stabwounds. The entrance of thiscatheter was superior, laterally, into the suprapatellar pouch, and theexit was anteromedial, justbelow the joint line. The skin was left open unless, because of loss ofsynovium or capsule, skinsuture was required to seal the joint. Through the catheter system, 5million units of penicillin in2,400 cc. of normal saline were run through the joint every 24 hours.The egress catheter wasclamped for one-half hour every 4 hours to ensure optimum lavage of thejoint. The cathetersystem was continued until the wound was closed at 5 to 7 days. (Feagin1966, CINCPAC-21968, 71).
Both of these methods were later found to have several drawbacks: patients could not be transported while the catheters were in place, catheters were frequently blocked, several known instances of complete synovial necrosis were thought to be caused by antibiotics, and gram-negative bacteria were cultured from the egress catheter (Feagin 1966, Whelan 1968). As a result, the second Conference on War Surgery recommended the deletion of the catheter method for the initial treatment of joint wounds. The study group also suggested loose closure of the synovium at five to seven days with split-thickness grafts or skin flaps, although primary closure was possible if the soft tissue had been avulsed. The group recognized that the joint function salvage rate would be low (less than 25 percent) using these methods (CINCPAC-2 1968, 71). The recommendations from the fifth and final CINCPAC surgical conference pertaining to joint injuries differed very little from those of the previous conferences (CINCPAC-5 1971, 44).
WOUNDS OF THE KNEE
The knee, a large, weightbearing, and poorly protected joint, is subject to injury in any highly active population. Such injuries account for a large portion of the surgery done by military orthopedic surgeons. The combat soldier is usually even more active than his brother in training; thus his knee is more subject to similar closed injuries. Patients with closed injuries, such as meniscal disruption, ligamentous sprains, patellar fractures, or dislocations were rapidly evacuated to PACOM and CONUS hospitals for appropriate treatment. Arthrotomy of knees with these types of injuries was discouraged in Vietnam, since return to duty as an effective combat soldier required weeks or months of rehabilitation. An accurate record of numbers and types of joint injuries and the final results of treatment is unavailable. Therefore, the information that follows in this section is anecdotal in nature.
Treatment of open wounds of the knee began on the battlefield when the unit aidman applied a compression dressing. Since helicopter evacuation was usually readily available, the patient was generally at a hospital within two hours. He seldom had to wait more than a total of four hours from the time of wounding until defini-
112
tive surgery. Rapid evacuation and earlydefinitive treatment, probably more than any otherfactor, favorably influenced the results obtained in treating kneewounds.
Upon arrival in the hospital receiving area, the patient underwent appropriate resuscitative measures and the start of intravenous fluids. He also usually received 20 million units of penicillin, and roentgenograms of his knee were obtained before he was taken to the operating room.
Operating room procedure included the initiation of anesthesia, usually spinal or general, and the application of pneumatic tourniquets. The extremity was shaved and washed with an antiseptic detergent solution circumferentially, from hip to ankle. The entire extremity was draped free. For small fragment or puncture wounds, anatomical arthrotomy approaches gained access to the interior of the joint. The wound area of skin, subcutaneous tissue, and capsule were debrided of a small amount of tissue, but the interior was examined through a formal arthrotomy approach. For large soft tissue wounds, the wound was extended sufficiently, both proximally and distally, to allow identification and protection of normal anatomical structures and visualization of damaged intra-articular tissues. During this process, later reconstruction of the joint was kept in mind. All loose intra-articular fragments of bone and cartilage were removed, and fragmented, torn, or detached menisci were excised.
The joint was irrigated with copious amounts (2,000 to 3,000 cc.) of sterile saline or antibiotic solution. An attempt was made to reduce major intra-articular fractures, but they were not internally fixed at the time of initial debridement. Large attached bone fragments were cleansed of all obvious debris and reduced, if possible. Generally, curettes and syringe irrigation were used in the debridement of large bone fragments. In some hospitals, however, a dental-type pulsating water jet system was used, an approach that gave rise to considerable controversy since some believed that the high pressure jet drove the contaminants further into the bone and soft tissue planes, while others concluded that it mechanically removed them from the area.
Before mid-1966, surgeons in Vietnam closed the joint synovium, the capsule, or both when there was sufficient tissue, but left the remainder of the wound open. In July 1966, however, information began to filter back to them that the knee wounds in which neither had been closed at the initial surgery were in better condition on arrival at the PACOM hospitals than those in which either the capsule or the synovium had been closed. These reports indicated that approximately 15 percent of those knees in which the synovium or the capsule had been closed initially had to be reexplored at the time of anticipated delayed primary closure because of joint effusion and suspected infection. In response, after initial debridement, Vietnam surgeons left an increasing number of knee joints open, and dressed the wounds, first with a layer of fine mesh gauze and then with a bulky occlusive dressing.
Fractures were dealt with by applying a cylinder cast which was immediately bivalved for later air evacuation. Where no major intra-articular damage was sustained, a bulky soft pressure dressing was applied, and medial and lateral plaster splints were placed over the dressing, secured in place with elastic bandages.
After immediate treatment in Vietnam, most patients with knee wounds were flown to offshore PACOM hospitals in the Philippines, Japan, Okinawa, or Hawaii within 7 days after injury. Frequently, the patients arrived dehydrated and exhausted from the prolonged trip through the evacuation system. The first 24 to 36 hours were spent, therefore, in general resuscitation of the patient, unless the clinical findings indi-
113
cated the presence of an active infection. Inthese instances, the patient was taken to theoperating room on the day of arrival for wound inspection andappropriate care.
The remainder of the patients were not taken to the operating room until 24 to 36 hours after arrival at the offshore hospital. With the patient under spinal or general anesthesia, the dressings were removed, the extremity was washed with an iodine-detergent solution, and the wound was examined. If the synovium and capsule had been previously closed and no significant joint effusion was encountered, the wound was closed by suture of the retinaculum and skin. If the synovium and capsule had been left open, the interior of the joint was inspected, irrigated with saline solution, and closed in layers. Penicillin (1 to 2 million units) was instilled into the joint before closing.
Postoperative care for the knee joint wounds without major intra-articular damage was similar to that of elective arthrotomies. After 10 days, the bulky pressure dressing or plaster cylinder cast and sutures were removed and range of motion and quadriceps strengthening exercises instituted. After remaining in the offshore hospital for 14 to 21 days, these patients were sent to a CONUS hospital for further rehabilitation.
In those cases where soft tissue loss made closure with local tissue unfeasible, split-thickness skin grafts were used to cover the area. In very few cases, skin flaps were employed to cover a wound. In knee joint injuries with major unstable intra-articular fractures, internal fixation with multiple Kirschner or Steinmann pins was attempted at the time of the delayed primary closure. Experience showed that if one waited until the wounds were healed, the bone fragments would have undergone marked osteoporotic changes, making secure internal fixation impossible. The fragment was likely to have partially healed in a poor position and, when motion was instituted, the dense periarticular adhesions that had formed might prove stronger than the osteoporotic bone of the joint. Therefore, after internal fixation, the joint was left open and a bulky occlusive dressing applied. The limb was kept elevated in a suspended Thomas splint with Pierson attachment for 5 to 7 days, then reinspected in the operating room with the patient anesthetized. The wound was closed if it was clinically free of infection and if sufficient soft tissue remained to allow suture of the wound. If these conditions did not permit closure, it was delayed another 10 to 14 days, at which time a split-thickness skin graft was applied. These patients were generally retained in the offshore hospitals for 30 to 60 days before evacuating them to CONUS.
When solid internal fixation was achieved, gentle active and passive flexion extension exercises were instituted within a few days, postoperatively. Usually this resulted in a functional early motion of the knee, although late realignment of the bony architecture rarely produced a functional joint.
To assess accurately the results of treating war injuries of the knee joint, one would need to follow the injuries from initial treatment to final disposition. However, in the Vietnam conflict, many men with minor wounds were treated in-country or at offshore hospitals and later returned to duty. Others succumbed to associated injuries. Since accurate data of this nature are not available, the results of treating a series of knee joint patients received at one general hospital are presented below. All of these patients were followed to a final disposition. However, one must keep in mind that this is a skewed series, representing primarily the more serious joint wounds.
From January 1968 through December 1970, 70 patients with knee wounds incurred in Vietnam were treated at Fitzsimons General Hospital (table 6). Twenty-eight injuries were caused by gunshot wounds, 38 wounds by fragments, and 4 puncture wounds by
114
punji sticks. Ten patients had infected kneesat the time of admission to Fitzsimons. Of the totalof 70 patients, 52 (74 percent) were returned to active duty and 18 (26percent) were dischargedbecause of residuals from the knee injury. At the time of finaldisposition, 56 (80 percent) of theknees had from 90 to 130 degrees of motion, 10 (14 percent) had from 60to 90 degrees, and 4 (6percent) had less than 60 degrees.
As would be expected, the knees that had sustained intra-articular fractures did not fare as well as those that did not (table 7). Twenty-eight (40 percent) knees had sustained major intra-articular damage varying from total disruption of the articular surfaces to a furrow plowed through one of the surfaces by the wounding device. Twenty of the fractures were caused by gunshot wounds and 8 by metal fragments. Fifteen (54 percent) of the patients returned to duty and 13 (46 percent) were discharged because of knee function impairment. Because of the greater velocity of the missile, the gunshot wounds generally caused greater disruption of the joint and, therefore, more serious impairment. Fifty percent of the patients with intra-articular fractures secondary to gunshot wounds and 37 percent of those with intra-articular fractures caused by metal fragments were disabled at discharge. The 28 cases with intra-articular fractures accounted for 13 of the 18 discharged related to knee residual impairment. In 3 of the remaining 5 cases, the disability was secondary to ligamentous instability, and 2 had marked limitation of motion from infection.
The actual number of knee joint wounds that eventually became infected is not available, but to most orthopedic surgeons who served in Vietnam, PACOM, and CONUS hospitals, it appeared that this was not a common complication. The knee wounds that were recognized as infected at the time of reexploration for delayed primary closure were further debrided, irrigated, and left open for reinspection 3 to 5 days later. If the wound appeared clean at that time, it was closed, systemic antibiotics were continued for 14 to 21 days, and, where applicable, an active range of motion was started in 10 to 14 days.
In the presence of continued infection, one of two courses was followed. One approach called for immobilizing the extremity in extension, leaving the wound open to drain, and administering appropriate systemic antibiotics until the infection appeared quiescent. After this had been achieved, wound closure was again attempted by whatever method necessary, most often by a split-thickness skin graft. When the joint appeared quiescent, motion was instituted. Where infection or the initial wounding agent had destroyed the joint, subsequent surgery was done to secure a solid bony ankylosis, which was commonly accomplished with a Charnley-type compression device (Charnley and Lowe 1958). This system allowed early ambulation during fusion. At one CONUS hospital, for 9 patients with destroyed knee joints, surgeons attempted to secure bony ankylosis with compression clamps and plaster immobilization without surgical excision of the remaining cartilage and subchondral bone. This goal was achieved in only1case. The other 8 had residual motion of the joint after removal of the clamps (Bailey and Burkhalter 1971).
The second approach involved a modified Willems’ regimen (Ballard et al. 1975). This method used wide arthrotomy, usually employing both medial and lateral parapatellar incisions because in several early cases where only the medial incision was used, lateral subluxation of the patella occurred. Through these incisions, the joint was thoroughly inspected and debrided of loose tissue fragments and other debris. Careful attention was paid to the synovium as it was incised. Purulent material exud-
115
ing from its cut edges indicated abscessformation within the structure, making synovectomynecessary. Synovectomy was also carried out if the synovium encroachedupon the articularsurfaces or in any way blocked joint motion. To complete thesynovectomy, the incisions wereextended proximally along the interior edges of the vastus medialis andlateralis muscles. Thisprovided access to all but the most posterior portion of the synovialtissue, which usually wasleft behind. The menisci were not excised unless severely damaged bythe initial trauma orsubsequent infection. The infrapatellar fat pad was not excised unlessobviously grossly infected.
TABLE 6.- Final disposition of patients with knee wounds
TABLE 7. - Influence of intra-articular fractures on final results
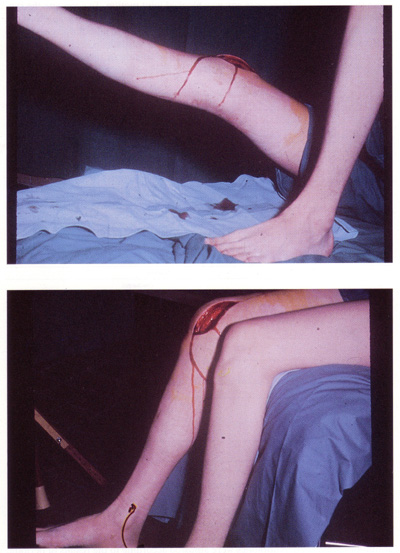
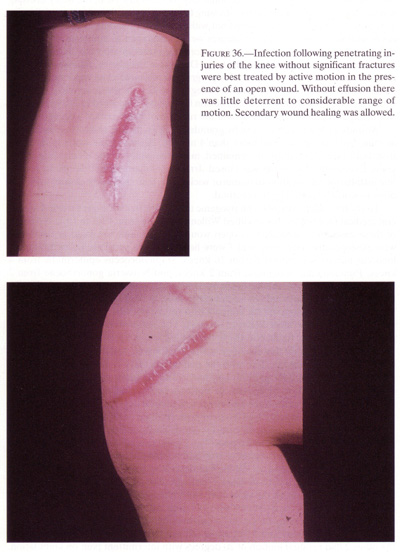
After the knee had been reexplored and a culture obtained both from the synovial fluid and a macerated fragment of synovium, a broad-spectrum antibiotic was given, intravenously, throughout the remainder of the surgery and thereafter for at least 48 hours. Oral antibiotics were then given until the erythrocyte sedimentation rate had returned to normal. Organisms identified in the cultures determined the antibiotics prescribed. Antibiotics were adjusted according to the results of periodic cultures of the effluent joint fluid throughout the remainder of the postoperative course. Usually the antibiotics were discontinued in 3 to 4 weeks (fig.36).
116
{kind=link}
117
{kind=link}
118
After surgical debridement, the wounds were left open on both sides. Fine mesh gauze was placed over the incisions, followed by a bulky pressure dressing, and the injured extremity was kept elevated continuously for 12 hours. Next, the bulky dressing was replaced by a smaller absorptive dressing to allow knee motion. Active-assistive exercises of the knee were then carried out with the patient standing at the bedside. Patients with stable intra-articular fractures were encouraged to ambulate on crutches with partial weightbearing. Unless this was done, the posterior aspect of the knee would act as a sump for the purulence in the knee. During his ambulation, the patient was required to use active knee motion. This program necessitated close supervision of the patient’s activity until he had obtained 70 degrees of flexion, which normally occurred within the first week. If this amount of flexion had not been achieved in 7 days, the knee was manipulated under anesthesia, and the regimen of knee motion was reinstituted.
Wounds were allowed to close by granulation. This usually took 4 to 6 weeks but in some instances it required more than 4 months. Normally the wounds closed in from both ends. A small fistula remained, most frequently on the medial side of the knee. Eventually this fistula was closed. Irrigation, chemical debridement, antibiotic installation, application of drains or wicks, or attempts at early closure were not done in wounds treated by this method.
Thirty-four adult patients with pyogenic arthritis of the knee were treated at several medical facilities by this modified Willems’ regimen from 1967 to 1972. Nineteen of these cases were secondary to open wounds of the joint sustained in combat, 8 were postoperative infections, and 7 were hematogenous pyogenic arthritis. Staphylococcus aureus was cultured from 26 knees, Staphylococcus epidermidis from 4 knees, Pseudomonas aeruginosa from 2 knees, and Neisseria gonorrhoeae from 2 knees. The infection was eradicated in all 34 patients, with no recurrences during the follow-up period. A subtotal synovectomy was done in 14 of the patients in this series. This procedure was reserved for patients with severe synovial involvement, not necessarily those with the most damaged cartilage. The results were graded good, fair, or poor, according to the findings at the first recorded follow-up examination.
A good result meant that the knee was asymptomatic, had more than 90 degrees of motion, and did not interfere with the patient’s activity. A fair result meant that the knee was only mildly painful, and had either 30 to 90 degrees of motion or caused some restriction of activity, or both. A poor result meant that there was more than mild pain in the knee and either less than 30 degrees of motion or the patient’s activity was markedly restricted, or both (Ballard et al. 1975).
In 19 patients with open infected wounds sustained in combat, the results achieved were 7 good, 6 fair, and 6 poor. The 7 good results were in patients who had not sustained fractures in the joint or who had no major damage to the articular cartilage from the wounding agent. Of the 6 patients with fair results in this group, 2 had fractures in the joint, 2 had moderate cartilage damage from the injury, 1 had a below knee amputation on the same side, and 1 had a below knee amputation on the contralateral side. Of the 6 patients who had poor results, 2 had surgical arthrodeses that resulted in solid bony fusion and a painless extremity, 2 had spontaneous ankylosis of the knee (1 bony and 1 fibrous--both resulting in a painless extremity), and the other 2 had residual motion of 20 degrees with intermittent pain on ambulation.
Three of the 8 patients with postoperative knee infections obtained good results. The results of the other 5 were fair. A good result was achieved in 6 or 7 patients with
119
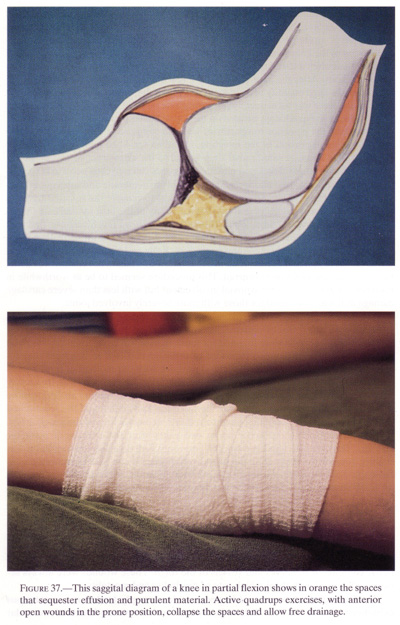
hematogenous pyogenic arthritis. Pyogenicarthritis in the adult knee was not a serious threat tolife or limb, but preservation of the joint remained a seriouschallenge to the treating physician(Jergesin and Jarvetz 1963). By using wide arthrotomies and earlyactive motion of the kneejoint, the joint could be more thoroughly evacuated of purulentmaterial than when allowed todrain in an immobilized position, regardless of the number ofincisions. After the joint was stillfor a few hours, the first active flexion of the knee caused a largequantity of exudate to spurtfrom the wound. More fluid was evacuated as the knee was subsequentlyput through its range ofmotion. As the knee was flexed actively, the quadriceps pressed on thesuprapatellar pouch. Inaddition, with active extension, the posterior compartment was alsocompressed. In some cases,active motion caused dispersion of the infection, but when the kneejoint was completely open,the fluid was evacuated rather than spread to the extra-articulartissues. In our patients, no sinustracts developed and no contiguous osteomyelitis occurred (fig.37).
Joint infections started and spread in the synovial membrane and subsequently invaded the joint cavity. Therefore, it seemed logical to remove the infected tissue, if the involvement was extensive and beyond the ability of the host to eradicate the infection, before it destroyed the joint. Although Albertin, a French surgeon, first suggested the use of synovectomy for the treatment of pyogenic arthritis in 1896, little was reported subsequently about this procedure. Kelly and associates from the Mayo Clinic (1970) reported one case of an infected elbow in which synovectomy was done, but only after ankylosis had occurred. This procedure seemed to be as worthwhile in fourteen patients with severe synovial involvement but with less than severe cartilage damage as it was when used for those with more severely involved joints.
The fate of the articular cartilage exposed to prolonged suppuration was not predictable in this series of patients. Twenty-one of the 26 patients with Staphylococcus aureus infection were infected for more than seven days. Eight of these had a good result. The prolonged exposure of articular cartilage in a wound that remained open up to six months concerned us, since with our method of treatment--open arthrotomy and early active motion--the articular cartilage was frequently visible for several weeks, in one instance for three months. We had an opportunity to look at the articular cartilage after the infection had healed and the wound had closed in two patients who happened to require reconstruction of the patellar tendon because of persistent laxity about two years after the episode of pyogenic arthritis. The cartilage appeared smooth and shiny with no gross erosion, but it was slightly thinned. A biopsy from the intercondylar area in one patient showed no microscopic abnormalities. Although the eventual outcome of this treatment regimen cannot be ascertained, the early results appeared promising.
WOUNDS OF THE HIP
Open wounds of the hip joint constituted another major problem. Hip joint wounds were frequently associated with damage to the adjacent abdominal and pelvic contents or to nerves and vessels of the thigh. These wounds were always serious and carried with them a high rate of morbidity and mortality.
The femoral head, because of its peculiar blood supply, leads a most precarious existence in the human body. When the femoral neck is severely fractured, avascular
120
{kind=link}
121
necrosis of the femoral head occurs in almostall cases. When a high-velocity missile insults thehead or neck and, at times, passes into the abdomen, contaminating thejoint both from withinand without the body, the chance of survival of that joint is nil.
Although most orthopedic surgeons treating casualties during the Vietnam conflict were familiar with multiple approaches to the hip joint, the precarious state of the patients who had sustained abdominal and vascular injuries frequently mitigated against an initial thorough debridement of the hip. Abdominal and vascular injuries always took priority in the treatment plan. After abdominal exploration or vascular repair, the patient’s condition was frequently too poor to withstand a major surgical procedure on the hip. Despite this, if the eventual morbidity was to be reduced, thorough debridement of the hip had to be carefully performed as soon as the patient was stabilized. Failure to do this was largely responsible for the high morbidity associated with hip joint wounds.
Since accurate data for hip joint wounds in the Vietnam conflict were not available, this section is confined to recommendations for treatment of these wounds (Thompson and Omer 1954) and results obtained from records in one of the CONUS hospitals.
Penetrating wounds involving the hip, pelvis, and lower abdomen were commonly treated by combined teams of general, urologic, and orthopedic surgeons. In general, small bowel wounds were treated by appropriate debridement and closure. Colonic and rectal injuries were usually treated with exteriorization and open loop colostomies. When deemed essential to healing, presacral drainage was done through the presacral space and exited posteriorly through an opening created by a coccygectomy. In those cases involving penetrating wounds through the lateral bony pelvis or hip joint plus lower bowel, the bones and joints invariably became infected if this type of drainage was not provided (Christy 1972).
All penetrating wounds of the hip joint required posterior arthrotomy and drainage, but exploration of the hip joint or ilium required the anterior approach for adequate exposure. The requirement of combined anteroposterior hip joint approaches, therefore, necessitated placing the patient in a lateral position on the operating table. A Kirschner wire or Steinmann pin was placed through the proximal tibia so that the lower extremity could be suspended from overhead in a moderately abducted position. The pin was used for subsequent traction as well. The entire thigh, hip, hemitrunk, and thorax were shaved and washed with antiseptic detergent, and the lower extremity was drape-free.
The anterior iliofemoral approach, extended proximally and posteriorly along the iliac crest as necessary, provided the best exposure to the hip joint, inner wall of the acetabulum, and both sides of the ilium. If possible, the existing wound of entrance or exit was incorporated into this approach. If not, debridement was accomplished separately, following the criteria of removing all possible contaminants and necrotic tissue. The hip joint capsule was opened with a “T” incision, the transverse portion of which paralleled the acetabular rim. All loose fragments of bone and cartilage were removed from the joint. If the femoral-fractured neck had been transected within the capsule and it was obvious that the blood supply to the femoral head had been destroyed, the free fragment of the femoral head and neck was excised. Failure to do this at the primary debridement only ensured further infection and prolonged morbidity. The joint was copiously irrigated with saline to flush out clot and contaminants. If the posterior capsule had been penetrated, the damaged
122
edges were excised. If the posterior capsulehad not been penetrated, a window was created inthis structure to allow for posterior drainage. When the wounding agenthad penetrated the iliumor acetabulum, both inner and outer walls were debrided, preferablythrough the anteriorapproach. The necrotic muscle clothing both sides of the ilium wasexcised, and bone edges wererongeured or curetted to free them from contaminants. If it had beenadvisable to leave thefemoral head in place, no internal fixation of the fracture was done atthe initial debridement.
If the incision had been extended to expose the anterior superior portion of the iliac crest, this portion of the wound was closed primarily, because retraction of the muscles made subsequent coverage of this portion of the ilium difficult or impossible. The remainder of the anterior incision, as well as wounds of entrance or exit, were left open. Posterior drainage was provided by a gluteal muscle-splitting incision. The sciatic nerve was identified and carefully protected during this approach. The gemellus and obturator muscles were transected at their insertion into the greater trochanter and allowed to retract. A large catheter was placed adjacent to the posterior capsular opening and brought out through the gluteal muscle and skin incisions. Fine mesh gauze was placed over the wounds and covered by an occlusive dressing. A one-and-one-half hip spica cast was applied, and the tibial pin used for skeletal traction was incorporated in the cast. The cast was bivalved, and appropriate windows were made in the anterior portion to accommodate evaluation and care of abdominal or lower pelvic problems. These patients were normally kept in a hospital in Vietnam until the intra-abdominal injuries and repairs were sufficiently healed to allow safe air evacuation to a PACOM or CONUS hospital. Usually, this period ranged from ten to fourteen days after injury.
Treatment at PACOM and CONUS hospitals consisted of removing the cast; inspecting the wounds under anesthesia in the operating room; redebridement when indicated by evidence of infection or residual necrotic tissue; and closing the anterior wounds if no infection was evident. Drains were removed from the posterior wounds. Usually, this site was allowed to heal by secondary intention. Granulating exit or entrance wounds that could not be closed with suture of local tissue were covered with split-thickness skin grafts. Use of rotating skin flaps was generally avoided.
Data are not available to allow accurate assessment of the treatment of hip joint wounds incurred in Vietnam, but the experience of one CONUS general hospital is probably representative of the overall results. Records are available for 19 patients with open wounds to the hip area admitted to Fitzsimons General Hospital from 1967 to 1971.
Open fracture of the acetabulum or ilium extending into the acetabulum was sustained by 7 of the19 patients in this series. In only 1 of these was major damage done to the acetabulum. Five of these patients developed an infection that required 2 or more subsequent surgical procedures. Four of the 5 with infections had associated intrapelvic or intra-abdominal injuries with bowel or bladder involvement. In 2 of these patients, the hip joint was eventually destroyed by the infection. The other 3 infections resolved without major damage to the hip joints. Two of this group of patients sustained a complete lesion of a major nerve, 1 femoral and 1 sciatic. In neither case was repair at subsequent exploration feasible. Three of this group of patients were returned to duty, while 4 were medically retired from the service as unfit for active duty.
Seven of the 19 patients had open extracapsular fractures of the proximal end of the femur. Six were comminuted intratrochanteric fractures, and 1 was at the base
123
of the neck of the femur. Two of thesepatients developed infections that required 3 or moresubsequent surgical procedures. Three developed malunion of thefracture, which compromisedgait and hip motion. One patient, with the basilar neck fracture,developed a nonunion requiringlate internal fixation, but eventually healed with a good result. Twoof this group had completesciatic nerve injuries without return of function after three years.One patient was a paraplegicsecondary to fragment wounds of the spinal cord, another had a smallbowel laceration, and athird later had a urethral transection. Of the group, 3 returned toduty with a limited duty profile,and 4 were medically retired. None of these patients suffered hip jointdestruction secondary toinfection.
Five of the 19 patients sustained open intracapsular fractures of the femur, but the femoral head was not excised at the initial debridement in any of these cases. All 5 developed avascular necrosis of the femoral head. Four of the 5 had prolonged infections that resolved only after removal of the dead infected head. Although the fifth patient did not develop an infection of the hip joint, the femoral head was removed because of avascular necrosis. Two of these patients sustained injuries to the sciatic nerve, 1 completed and 1 with peroneal involvement only. Neither of the nerve lesions resolved. The infection in 3 of the 4 cases cleared after removal of the femoral head and debridement of the joint. The other patient required 3 subsequent operative debridements before the infection finally resolved. In 4 of these cases, Ring metallic prostheses were used to reconstruct the joint three to twelve months after the infection had resolved clinically and radiographically. In the fifth case, a custom-built all-metallic femoral head neck and metallic acetabulum replaced essentially the entire top end of the femur as well as the destroyed acetabulum. In 3 cases, the Ring prosthesis loosened within two years of emplacement, resulting in pain and joint dysfunction. In each of these cases, the Ring prosthesis was removed and replaced with a metal-plastic prosthesis cemented to the femur and acetabulum. At the time of the second reconstructive procedure, cultures from the hip joint were negative for growth in all instances. These patients were followed from three to five years, and in no case was a subsequent infection of the joint found. All patients retained an excellent range of motion in a relatively painless joint. None required or used external support for ambulation. All 5 of these patients were medically retired from active duty. This method of reconstruction was not standard. Time will determine whether it should be considered a feasible alternative to joint resection or arthrodesis in the young active person with a destroyed hip joint secondary to an open combat injury.
WOUNDS OFTHE SHOULDER
Open injuries of the shoulder and upper arm were associated with a high incidence of neurovascular damage, which frequently proved to be the most disabling factor in the patient’s injury. In addition, head, neck, and chest wounds were commonly associated with combat wounds of the shoulder joint. The care of these associated life-threatening injuries always took priority over the treatment of the shoulder joint wounds. Tandem treatment teams cared for these multiple injuries, with the appropriate neurologic, vascular, thoracic, or general surgeon first taking care of the other injuries that did not involve the extremities. The orthopedic surgeon then debrided ex-
124
tremity wounds, including those of the joints. Perhaps peculiar to the military surgeon of the Vietnam War was the custom of making the orthopedist responsible for the initial, and frequently subsequent, treatment of the injured nerves in the extremities.
Whether rendered in the field by a corpsman or in a hospital, the initial treatment of the shoulder wound resembled that of any other injury. Once in the operating room, the surgeons addressed suspected injuries in order of priority. There, under general anesthesia, usually via endotracheal tube, the patient was positioned in a lateral or semilateral position; the shoulder girdle, neck, hemithorax, and upper limb were washed with an appropriate antiseptic solution; and a sterile drape was applied, with the upper extremity drape-free. An effort was made to pack the wound with a sterile sponge during the surgical preparation of the area to prevent further contamination as the remainder of the extremity and adjacent parts were cleansed. Anatomic anterior or posterior or both approaches incorporated the wound, where possible, into the incision. If neurological or major vascular structures had been damaged, the nerves and vessels were first identified in an area remote from the wound and then traced to the site of damage. This prevented inadvertent further damage during the surgical exploration. When the brachial plexus or subclavian vessels had been damaged by the traversing missile, resection of portions of the clavicle was sometimes necessary to gain access to these structures.
The principles of debridement emphasized in other sections of this book were followed in treating shoulder wounds. A minimal amount of damaged skin was removed. Fascia, because of its poor blood supply and potential source of infection, was liberally excised and incised to gain exposure to the deep structures. However, because muscle tissue was absolutely critical to future shoulder stability and motion, the real key to successful debridement was surgical judgment of viability of shoulder muscle tissue. If necrotic muscle was left behind, it served as a perfect culture medium for bacteria; yet overzealous excision of viable muscle reduced the potential for joint function, since the shoulder joint depends so extensively upon the rotator cuff for its stability and motion.
The criteria of muscle viability--color, contractility, consistency, and capillary bleeding--all served as useful guidelines in the course of debridement, with muscle consistency the most dependable. Nonviable muscle rapidly lost its firm rubbery consistency and became mushy, friable, and readily fragmented when grasped with tissue forceps.
Commonly the joint was exposed through the interval between the anterior deltoid and pectoralis major muscles. The conjoined tendons of the short head of the biceps, coracobrachialis, and pectoralis minor muscles were transected at the coracoid process and retracted medially and distally to allow greater exposure of the joint and better protection of the musculocutaneous nerve. The tendon of the subscapularis muscle was incised and this muscle retracted medially to expose the underlying capsule, which was trimmed carefully to preserve as much substance as possible to assist in the future stability of the shoulder. All small loose fragments of bone and cartilage were excised, while larger bone fragments with soft tissue attachments were carefully cleansed of visible contaminants and preserved. If the humeral head was completely devoid of soft tissue attachment and was lying as a loose free fragment in the joint, it was excised and discarded. Attempts to save this necrotic fragment of bone to aid in future reconstructive procedures were ill ad-
125
vised. Such attempts frequently led tochronic infection of the joint, additional loss of bonesubstance, and further compromise of future reconstructive procedures.
In perforating wounds, a separate posterior approach was required to complete the debridement. When possible, the incision incorporated the wound but, more importantly, anatomic approaches were followed so that undamaged tissue could be identified and protected. Access to the posterior shoulder was achieved by removing the posterior fibers of the deltoid from the spine of the scapula and incising the infraspinatus and teres minor tendons from the greater tuberosity of the humerus. Whenever possible, the supraspinatus tendon was left intact, since it is probably the most important member of the rotator cuff in providing shoulder stability during active motion of this joint. After surgical trimming of the contaminated and necrotic tissues, the joint was left open and dressed with fine mesh gauze placed loosely over the wounds. A bulky absorptive dressing was applied, and the limb was secured to the body with a Velpeau-type soft dressing, reinforced for transportation with a plaster cast. The cast was usually suspended from the opposite shoulder, which contributed to the comfort of the patient. Internal fixation of fractures was not done during this initial stage of wound care. Early in the conflict it was found that drains were not a good substitute for leaving the wound open, and their use was condemned by members of the CINCPAC surgical conference in 1967 (CINCPAC-1 1967). Rather than facilitating drainage, they actually blocked the egress of fluid from the depths of the wound, inviting further infection and tissue destruction.
Patients with shoulder wounds and without other serious injuries were evacuated to an offshore hospital two to three days after the initial debridement. Those with complicating head, neck, chest, or abdominal injuries were retained in the initial hospital for observation for an additional seven to ten days. Since shoulder wounds were associated with significant blood loss that rendered the patient quite incapable of withstanding a prolonged airplane ride sitting comfortably or safely, patients with significant shoulder wounds were usually transported through the evacuation system on a litter.
At five to seven days after initial wound debridement, the patient was returned to the operating room, the dressings were removed, and the wounds were inspected under general anesthesia. Further necessary debridement was then carried out. If the wounds appeared clean at this second-look procedure, the joint was closed, tendons were reattached where possible, and a delayed primary closure of the skin was done. When, because of tissue loss, skin closure was not possible, split-thickness skin grafts were used or the wound was left open to heal by secondary intention. Pedicle or local rotation flaps were rarely used, except for cases where coverage of nerves or major vessels was necessary. If the wounds were clean, appropriate internal fixation devices were used to stabilize major fracture fragments at this second-look procedure.
Early motion of the shoulder was encouraged in all instances where future joint function was considered to be feasible and the stability of the fracture fragments was such that this could be done. This motion was commonly initiated at seven to ten days after the second-look procedure. A collar and cuff sling provided part of the support for the upper extremity. With the sling in place, the patient bent forward from the waist, allowing the arm to hang perpendicular from the trunk, and with the assistance of a physical therapist, he put the arm through an increasing range of abduction, flexion, extension, and circumduction. Perhaps because of the
126
extensive scarring of the accompanying openwounds of the shoulder, surprisingly few of thesepatients developed subsequent problems with recurrent dislocations.
When sepsis of the joint was suspected, the patient was returned to the operating room as many times as necessary for further cleansing of the joint and to ensure adequate drainage. The infected wound was left open, and active motion was encouraged to assist in the evacuation of the collected fluid from the joint. Systemic antibiotics were continued until clinical evidence of sepsis was no longer present, and frequently until the erythrocyte sedimentation rate had returned to normal. From 1967 to 1969, surgeons also attempted to prevent or control wound infection of many areas, including the shoulder joint, by instilling local antibiotics through a suction irrigation system. A solution of 1,000 units per ml. bacitracin, 1 percent neomycin, and 0.1 percent polymixin B was instilled by constant drip into the joint and evacuated either continuously or periodically, with a suction machine. Although this regimen was sometimes efficacious in controlling local infection, it carried with it considerable risk of systemic toxicity, especially in wounds such as the shoulder joint, where large areas of muscle tissue were bathed by the solution and absorbed it into the bloodstream. A number of cases of partial nephro- and ototoxicity were attributed to this treatment method. Therefore, in January 1968, Col. Thomas Whelan, surgical consultant to CINCPAC, distributed a communique to all hospitals in PACOM advising discontinuance of this method of treatment.
In the patients with total destruction of the humeral head or glenoid or both, the limited available ways to handle the problem were resection arthroplasty, shoulder fusion, and prosthetic replacement of the upper portion of the humerus. The prosthetic replacements were rarely applicable to the treatment of combat wounds of the shoulder. They depended upon the reconstruction of the rotator cuff for their stability, and this structure had usually become so scarred and contracted by the time the shoulder was ready for reconstruction that prosthetic replacements could not be used.
Partial resection arthroplasty of the shoulder was the most common treatment method during the patient’s initial hospitalization. This procedure provided for some motion but was frequently associated with residual pain and weakness that precluded heavy lifting or other vigorous use of the upper extremity. However, because of the heavy workload at the military hospitals and the desire of many patients to leave the hospital at the earliest possible date, many with severely damaged shoulders were discharged after their partial resection arthroplasty. A better functional result could probably have been achieved by a shoulder arthrodesis.
Shoulder arthrodesis was considered the most effective way of treating patients with severely damaged shoulder joints. Multiple methods of achieving this goal were used. Most incorporated three steps. First, all remaining cartilage was excised from both sides of the joint. Second, the humerus was securely fixed to the remaining scapula with metallic devices. Finally, an extra-articular bone graft was frequently added by placing the outer end of the osteotomized acromion into the remaining top end of the humerus or by a method preferred by a number of surgeons, the modified Brittain posterior scapulohumeral arthrodesis, in which a bone graft was inserted between the humerus and the scapula. Brittain (1952, 168-76) used an arrow-shaped tibial graft inserted into the humerus and notched to straddle the axillary border of the scapula. He recommended arthrodesis of the shoulder in 80 degrees of abduction, 30 degrees of internal rotation, and 40 degrees of forward flexion. This standard salute position was also recommended by the research committee of the American Orthopedic Association in
127
1942. It was used extensively in thetreatment of flail shoulders secondary to birth injuries andpoliomyelitis in children and was usually quite satisfactory for theseconditions (Barr et al. 942). This position, however, was not withoutdifficulty in the adult,as has been pointed out byRowe (1974) and Davis and Cottrell (1962). The excessive abduction andforward flexionresulted in winging of the scapula, a prominent medial border of thescapula, chronic stain of thescapulothoracic muscles, and neck pain.
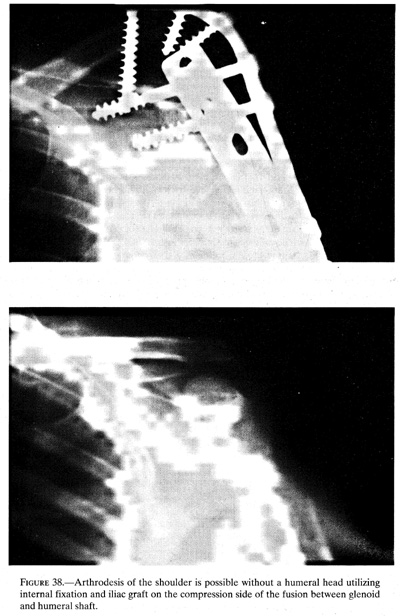
The shoulder arthrodesis method preferred by the surgeons at Fitzsimons General Hospital used a tricortical iliac graft fashioned to fit in the arc formed by the humeral metaphysis, lower edge of the glenoid, and the adjacent area of the scapula. This procedure was done through the posterior approach described by Kocher (1911, 1:322-23). The shorter iliac graft was made possible by the different position in which the shoulder was fused. The most satisfactory shoulder arthrodesis position in the adult was to abduct the arm to 20 to 30 degrees from the side of the body, forward flexed 30 degrees, and internally rotated 40 degrees. From this position the patient was able to reach his hand to his face by scapulothoracic motion and elbow flexion. He could also reach his hip area without difficulty. From this position, the patient was also able to do heavy work that could not be done from the abducted position, which depends upon the scapulothoracic muscles for its maintenance (fig. 38).
Despite the known advantages of shoulder arthrodesis over shoulder resection, which allowed only limited motion frequently associated with pain, few shoulder arthrodeses were done on Vietnam patients during their hospitalization for initial wound care. Probably, the surgeons did not urge for this procedure because of their already high workload and the patient’s usual desire to leave the hospital as soon as possible. Whether subsequent arthrodeses were done in these patients at other facilities cannot be ascertained.
From records available at Fitzsimons General Hospital, it is possible to glean some information on the history of shoulder wounds. Undoubtedly these cases represent a skewed series, including those patients with severe wounds of the shoulder as well as the complicating associated injuries. For 40 of these patients, sufficient records were available to assess the results of their shoulder wounds and subsequent treatment. All of these were young men between nineteen and twenty-five years old. Twenty-three had sustained gunshot wounds in the shoulder region. The remaining 17 shoulder wounds were secondary to metallic fragments from explosive devices. Nine patients had no injury other than that of the shoulder joint; the other 31 had associated injuries. Some patients had wounds in multiple other areas:
Ipsilateral upper extremity nerves........................................................................ 12
Contralaterial upper extremity nerves.................................................................. 1
Chest................................................................................................................. 12
Neck................................................................................................................... 5
Upper extremity (ipsilateral).................................................................................. 7
Upper extremity (contralateral).............................................................................. 2
Brachial artery....................................................................................................... 4
Head..................................................................................................................... 3
Thigh.................................................................................................................... 6
Leg....................................................................................................................... 5
Foot...................................................................................................................... 1
128
{kind=link}
129
Of the 40 patients with shoulder wounds, 20 (50 percent) were returned to an active duty status with a functional shoulder. The other 20 patients were discharged unfit for duty. Nine patients were unfit because of shoulder dysfunction secondary to bony or soft tissue injury about the shoulder, 8 were unfit due to residual compromise of hand and forearm function caused by associated nerve injury, 1 patient had an above elbow amputation resulting from vascular injury, and the remaining 2 had normal shoulders but residual osteomyelitis from their open tibial fractures.
Two patients developed a shoulder wound infection that necessitated further surgical debridement. In both cases the wounds healed after the second surgery without residual osteomyelitis or further compromise of shoulder function. Both of these patients were returned to duty. Of the 9 patients with residual shoulder dysfunction, 6 had sustained comminuted intra-articular fractures with loss of substance of the joint, and the remaining 3 had lost the support of the soft tissue about the shoulder, resulting in a flail joint. Four of these patients had shoulder arthrodeses, 2 during their initial hospitalization and the others within 2 years of discharge. Whether other patients discharged with residual shoulder dysfunction had subsequent surgical procedures elsewhere is not known.
Since the shoulder is a loose-fitting enarthrodial joint with a hemispherical humeral head rotating on a much smaller shallow glenoid fossa, it can absorb considerable damage and still retain its motion if its supporting muscle and capsular structures remain functional. The careful surgery done at all levels in the evacuation chain resulted in the surprisingly good results that were achieved during the Vietnam conflict. The infection rate was low, and the return to duty of even those who had sustained significant injury was quite high. The treatment of the severely damaged shoulder was by resection of loose unattached fragments, usually followed by institution of early motion. Residual painful or flail shoulders were treated subsequently by shoulder arthrodesis, frequently using a modification of the extra-articular arthrodesis described by Brittain (1952).
REFERENCES
Albertin, -----. 1896. De la synovectomie et de l’arthrectomie dans les arthrites infectieuses aigues du genou consecutives aux plaies penetrantes de cette articulation. LaProvinceMedicale, 1896: 195-97, 206-09.
Bailey, J., and Burkhalter, W. E. 1971.“Failure to obtain knee fusion after severe injury to theknee joint. Unpublished manuscript.
Ballard, A.; Burkhalter, W. E.; Mayfield, G.W.; Dehne, E.; and Brown, P. W. 1975. Thefunctional treatment of pyogenic arthritis of the adult knee. J. BoneJoint Surg. (Am) 57,119-23.
Barr, J. S.; Freiberg, J. A.; Colonna, P. C.; and Pemberton, P. A. 1942. A survey of end results on stabilization of the paralytic shoulder. Report on the Research Committee of the American Orthopedic Association. J. Bone Joint Surg. (Am) 24:699-707.
Brittain, H. A. 1952. Architecturalprinciples in arthrodesis. 2d ed. Edinburgh: E. & S.Livingstone.
Charnley, J., and Lowe, H. G. 1958. A studyof the end-results of compression arthrodesis of theknee. J. Bone Joint Surg.(Br) 40: 633-35.
Christy, J. P. 1972. Complications of combatcasualties with combined injuries of bone andbowel--personal experience with nineteen patients. Surgery 71:270-74.
130
CINCPAC -1. 1967. Commander in Chief,Pacific.First CINCPAC Conference on Surgery. Tri-service conference on warsurgery conducted at John Hay Air Base,Philippines, 20-25 May 1967.
CINCPAC -2. 1968. Commander in Chief,Pacific. SecondCINCPAC Conference on War Surgery. Tri-service conference on warsurgery conductedat John Hay Air Base, Philippines, 25-28 March 1968.
CINCPAC -4. 1970. Commander in Chief,Pacific.Fourth CINCPAC Conference on WarSurgery. Tri-service conference conducted on war surgery in Tokyo,Japan, 16-19February 1970.
CINCPAC -5. 1971. Commander in Chief,Pacific.Fifth CINCPAC Conference on WarSurgery in Tokyo, Japan, 29 March-2 April 1971.
Davis, G. L. 1970. Management of open woundsof joints during the Vietnam War. Clin.Orthop. 68:3-9.
Davis, J. B., and Cottrell, G. W. 1962. Atechnique for shoulder arthrodesis. J. Bone Joint Surg.(Am) 44:657-61.
DOD-EWS-Dept. of Defense, 1958.
Feagin, J. 1966. The treatment of penetratinginjuries of the knee joint with significant tissuedestruction. Unpublished report, Headquarters, 85th EvacuationHospital, 4 Nov 1966.
Hampton, O. P., Jr. 1957. Orthopedic surgeryin the Mediterranean Theater of Operations. Officeof The Surgeon General, Department of the Army. Washington: GPO.
Jergesin, F, and Javetz, E. 1963. Pyogenicinfections in orthopedic surgery. Am.J. Surg.106:152-62.
Kelly, P. J.; Martin, W. J.; and Coventry, M.B. 1970. Bacterial (suppurative) arthritis in theadult. J. Bone Joint Surg.(Am) 52-4:1595-1602.
Kocher, T. 1911. Textbook of operativesurgery, vol. 1. New York: Macmillan Co.
MD-WW-MedicalDepartment, U.S. Army. TheMedical Department of the UnitedStates Army in the world war, vol. 11, pt.1. Washington: GPO.
MSHWR-U.S. Surgeon General’s Office. 1876.The medical and surgical history ofthe War ofthe Rebellion. Washington:GPO.
NATO Emergencywar surgery handbook. 1958.Department of Defense. Washington: GPO.
Rowe, C. R. 1974. Re-evaluation of theposition of the arm in arthrodesis of the shoulderin the adult. J. Bone Joint Surg.(Am) 56:913-22.
Thompson, M. S., and Omer, G. E., Jr. 1954.Gunshot wounds of the hip joint. Surg.Gynecol.Obstet. 98:237-40.
Walton, S. 1970. Report of OrthopedicConsultant visit to Republic of Vietnam on 3-15 April1970 and to 5th Field Hospital, U.S. Army, Bangkok, Thailand, 16-17April 1970.
Whelan, T. J., Jr. 1968. Ltr, Col. T. J.Whelan, Jr., to Lt. Col. Clyde N. Herrick, 31 Jan 1968, sub: A Warningin the Use of Irrigation Aspiration Technique for TopicalNeomycin,Bacitracin and Polymixin B Administration.
Willems, C. 1919. Treatment of purulentarthritis by wide arthrotomy followed by immediateactive mobilization. Surg. Gynecol. Obstet.28:546-54.