



Chapter 7
VIETNAM WAR AMPUTEES
Colonel Gerald W. Mayfield, MC, USA (Ret.)
WOUNDS AND WOUNDING AGENTS
Wounding agents during the Vietnam War differed from those in previous conflicts. In World Wars I and II, and in Korea, artillery had been the greatest threat to the soldier. In World War II, land mines and shell fragments caused a majority of the wounds that resulted in amputation and were responsible for an increase to 5.3 percent of troops suffering major amputations from the 2 percent from World War I (Cleveland and Shands 1970). Vietnam saw a significant shift in both the characteristics and the management of those wounds which caused the loss of a limb. The enemy had few heavy weapons, and, as a result, most casualties were caused by rifle and machine gun fires, mines, and booby traps. Such weapons had inherently greater destructive potential than shell fragments and made the proportion of limb-threatening wounds greater. Of these, mines and booby traps, weapons that exploded at very close range, caused the greatest trauma and accounted for approximately 55 percent of all amputations in one series. On the other hand, gunshot wounds caused only 8 percent of the amputations in the same series.
Although the proportion of limb-threatening wounds was greater in the Vietnam War than in previous conflicts, rapid helicopter evacuation from the wounding site to a surgical facility that could resuscitate and treat all wounds expeditiously saved many apparently fatally wounded soldiers. Ironically, this success also dramatically increased the proportion of survivors with multiple amputations. Soldiers with more than one extremity amputated had accounted for 2 percent of the wounded in World War I and 5 percent in World War II. But during the Vietnam War multiple extremity amputations rose to 19 percent in one series of 415 amputee patients and to 18 percent in a longitudinal survey of 169 amputees. Many of these ablations were the result of inadequate vascular flow to the distal portion of the extremity.
Even in cases of multiple system injuries, surgeons made every effort to save an extremity. Many facets of the patient’s condition were considered before making the decision to amputate. Decisions were easy if the soldier arrived from the battlefield with a completely nonviable limb attached to the proximal segment by a few strands of tissue, or if there was complete absence of the distal portion. In contrast, decisions were difficult if the patient had a proximal wound with varying degrees of structural instability, tissue viability, infection, and altered states of nerve and vascular supply to the distal part. American surgeons usually practiced a conservative approach to amputation, believing that the World War II experience demonstrated that reconstruction of severely injured extremities could be accomplished if surgeons provided proper initial debridement, meticulous wound care, and appropriate fracture management.
132
In general, management paralleled guidelines listed in the NATO Handbook, Emergency WarSurgery(1958).However, deviations inevitably evolved. These deviations and theirimplicationswill be discussed in the following sections on management of amputeesin different regionalzones of treatment.
MANAGEMENT OF PATIENTS WITH AMPUTATIONS
Treatment in Vietnam
Complete information concerning the management of Vietnam War amputees in the United States Armed Forces, from the time of injury to some subsequent stable point, is not available. The following narrative concerning amputee management is a composite of information gathered from published materials written by other orthopedic surgeons, a review of hospital records, and personal observations by surgeons from a number of medical facilities, including the 106th General Hospital in Yokohama, Japan; Valley Forge General Hospital in Pennsylvania; and Fitzsimons General Hospital, Denver, Colorado.
Geographic factors, combined with fluctuating patient loads from changing tactical situations in Vietnam, had a direct effect on the continuity of optimum management of the amputee. Most commonly a helicopter evacuated the patient from the battlefield to a hospital for evaluation of the extremity and wound assessment. If any distal portion of the extremity remained, the decision to amputate was made by or under the guidance of an orthopedic surgeon.
Subsequent to the amputation, the amputee was evacuated from Vietnam to a PACOM hospital within a few (three to ten) days. The time span depended on his general condition and the efficiency of the evacuation system. After an intermediate stage of evaluation and treatment in a PACOM hospital, where the average stay was fourteen days, the patient was evacuated to CONUS.
One of the most difficult decisions in the field of trauma surgery was whether to amputate an intact extremity with massive loss of bone, muscle, tendon, and nerve and with a compromised circulation. However, amputating at a preconceived “ideal” level was also discouraged. The ultimate course of treatment in the difficult-decision cases concerning amputation usually reflected, at least in the later stages of the evacuation chain, a joint patient-physician agreement. Amputation for life-threatening infections was performed occasionally. However, their incidence was lower in Vietnam than in previous conflicts. Amputation for established gas gangrene was rarely required. Col. Raymond Bagg reported in 1977 that hyperbaric oxygen was used successfully to avoid amputation in two cases of clostridial myofascitis at the 106th General Hospital in Japan.
Replantation of a sharply severed extremity was popular in civilian practice during the late 1960s and early 1970s, but replantation was apparently never attempted in the Vietnam War. Replantation may not be feasible even in future wars because of the devastating effects of wounding agents, nonavailability of an appropriate team and facilities, and the potential necessity for rapid evacuation.
In the Vietnam combat zone, open amputation was usually recommended. It was performed at the most distal point feasible, without regard to the “site of election.” Surgeons emphasized debridement of all nonviable tissue and tried, if possi-
133
ble, to leave viableflaps. Frequently these flaps were irregular in contour and unsupportedbyunderlying skeletal tissue. Appropriate support of these flaps withdressings and well-appliedskin traction was necessary to preserve the viability of the flap. Anotable exception was thefailure of many primary Syme’s-type amputations, because of necrosis ofthe heel pad portion ofthe stump.
Some stumps were closed in Vietnam during the delayed primary closure period, extending from three to ten days after injury. Frequently, however, patients were evacuated from the combat zone before the operating surgeon knew whether the delayed primary closure was satisfactory and whether the wound had healed without subsequent infection or flap necrosis. The operating surgeon had no official channel for follow up on the patient’s condition after he was evacuated from the combat zone.
Blasting-type injuries from mines, booby traps, mortars, and grenades frequently caused deep penetrating wounds proximal to the level of amputation. Blasts beneath the person caused foreign material to penetrate vertically deep into thigh and buttock muscle and frequently to reach the knee and hip joints. Areas of deep contamination required additional longitudinal incisions on the extremity for adequate debridement.
Control of arterial bleeding occasionally required other incisions proximal to the site of amputation. In above-knee amputations, open fractures of the ipsilateral femur required debridement stabilization by a plaster spica with skin traction to the stump. In the below-knee amputations with an associated femur fracture, skeletal traction with a tibial pin was accomplished. Before evacuation, a spica cast was applied, incorporating the pin in the plaster.
Immediate application and continuous use of skin traction on the open stump by methods described during World War II (MD-OSMTO 1957) were used, but not as extensively as they should have been. Wilber (1970) reported that, in Vietnam, only 44 percent of 300 patients with open amputations were treated initially with skin traction. Only 50 percent of a group of orthopedic surgeons who cared for amputees at two or more echelons of evacuation indicated that adequate skin traction was applied or maintained during evacuation. Each of these surgeons, however, stated that he personally used skin traction in the initial treatment of the amputee, if it could be applied.
The technique of applying skin traction is critical to its effective use. The NATO Handbookon Emergency War Surgery (1958) describes gluingstockinette to the distal 8 inches of the skin as ameans of applying traction to the stump. Application of the adhesivematerial and subsequenttraction to the skin proximal to a point only 2 inches from the end ofthe stump proved moresuccessful, because it increased the efficiency of the traction on themost critical distal 2 inchesof the stump and thus provided more rapid closure and tapering of thestump.
To maintain effective skin traction through the healing phase, the weight and direction of traction had to be kept constant and adjusted only by the physician. At the U.S. Army Hospital, Camp Zama, Japan, approximately 80 percent of the amputees arrived in 1969 with the skin traction ineffective. The weight bag was invariably resting on the evacuation litter. On questioning personnel involved in the transfer of the patients in the evacuation route, they replied that the patients had complained of pain, which was eased by relieving the tension of the swinging weight bag dangling over the litter pulley.
In an effort to overcome the swinging weight problem, surgeons incorporated a wire ladder splint into a plaster spica for the above-knee amputee. For the below-knee am-
134
putee, they provided an above-knee cast with traction applied by meansof rubber tubingextending between the stockinette and a wire ladder splint. The majordisadvantages of thismethod were difficulty in obtaining the materials necessary to applythe device and, in somecases, having to alter the device to meet air evacuation requirements.
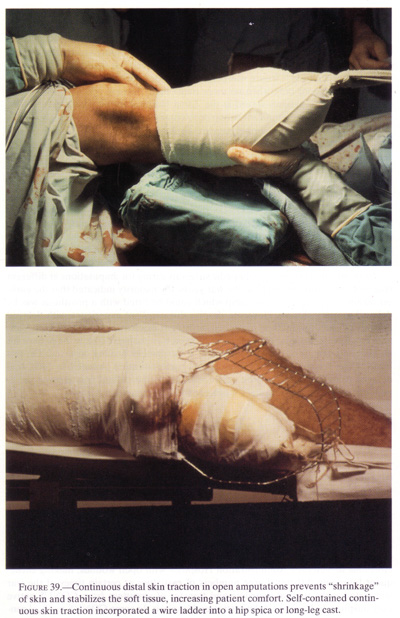
A self-contained centrifugal pulley device, providing constant traction, was introduced to circumvent the problems of unknown tensions and balkiness on the wire-ladder-splint-rubber-band method. These devices never became widely used because they were seldom returned to the initial treatment area. Moreover, they were often found detached and not providing traction when the amputee arrived in the PACOM hospitals (fig.39).
Immediate Treatment in Offshore Hospitals
Although a patient was occasionally kept in Vietnam for a longer period because of other associated injuries so severe that he could not be evacuated, the patient with a major amputation usually arrived in an offshore hospital within three to ten days after being wounded. The long flight to the offshore hospitals required multiple transfers that exhausted amputees, who also suffered varying degrees of dehydration and anemia as their bodies adjusted to the wound insult and subsequent surgery.
Shortly after the patient’s arrival at the offshore hospital, efforts were made to correct any general medical and fluid problems. When his condition was stabilized adequately (usually within forty-eight hours), the amputation site was inspected under general anesthesia in the operating room. Frequently, redebridement was necessary to remove tissue that had declared itself nonviable since the original debridement. Proximal longitudinal incisions were sometimes necessary in both the below-knee and above-knee amputations for debridement of nonviable muscle from selective compartments in the extremity. The anterior compartment muscles of the short or intermediate length below-knee stump and the adductor muscle area in the above-knee amputee were most frequently found to be necrotic.
After redebridement, skin traction was applied. If other injuries or medical conditions mitigated against early evacuation, skin traction was maintained by weights suspended over a pulley from the end of the bed. When the patient was likely to be evacuated in the immediate future because of abdominal, chest, other extremity, or other injuries, a self-contained traction apparatus was applied.
A notable change in the management of the amputation wound at the offshore hospital evolved during the course of the war. In 1966, Dr. Oscar Hampton (1966) reinforced the concept of delayed primary closure of wounds, including amputation stumps. At the second CINCPAC Conference on War Surgery (CINCPAC-2 1968), the recommendation was made that an open amputation wound be regarded as “a major open war wound and that at the end of three to seven days, it [would] be partially closed with skin graft and the modified skin flaps. . . sutured in the most desirable position without pinching.” This advice, combined with other recommendations throughout the conference (such as delayed primary closure at four to seven days), was interpreted by some in the offshore hospitals as an indicator that delayed primary closure should be performed on all amputation stumps, if possible. The fol-
135
{kind=link}
136
lowing paragraphs reveal some observations about the practices and results in care of the amputee in the offshore hospitals.
In 1966 and 1967, at the hospital in Camp Zama, a number of delayed primary closures of selected amputation stumps were performed: Only stumps that had a “clean appearance, without gross necrosis, and were seen less than 10 days after amputation” were closed. Closure was performed by or under the direct supervision of orthopedic surgeons only when no more than “light” tension was necessary at the suture line. These patients stayed at the Zama Hospital for an additional 10 to 14 days to assure that no significant stump problems developed before evacuation.
Although no specific recorded data are available concerning the outcome of this particular group of patients, it is our impression that the majority of these stumps remained closed, without debilitating wound breakdown. We expected and observed only minor suture reactions and localized areas of minor wound breakdown that did not require major operative intervention.
Subsequent studies of longitudinal groups of patients treated at the 106th General Hospital (Japan) and in CONUS revealed that both below-knee and above-knee stumps treated by delayed primary closure required significantly shorter time for fitting a final prosthesis than those treated by the open-wound method. This observation may reflect a preselection of cases that were left open because of associated injuries and, therefore, would be expected to take a longer period for healing.
In an informal survey of orthopedic surgeons caring for amputations at different stages of evacuation throughout the war years, the majority indicated that the earliest means of getting a closed stump which could be fitted with a prosthesis was by delayed primary closure. However, despite this excellent experience with delayed primary closure, this method presented difficulties in a forward zone, either in Vietnam or offshore, because the operating surgeon was unable to follow the patient for an adequate length of time to determine if satisfactory healing occurred. On this basis, it was recommended, through verbal communication channels in 1968, that delayed primary closure not be performed unless the patient was assured of remaining in the treating hospital for at least 14 days after closure.
Conditions in CONUS
Most amputees arriving in CONUS hospitals about 2 to 8 weeks following injury were in better physical condition and less fatigued than those patients arriving 3 to 5 days after injury. Nevertheless, depending on the status of wounds, further examination under anesthesia with redebridement was necessary in some patients. The extent of treatment leading to the point of definitive stump healing and prosthetic fitting varied considerably at different times at different institutions, based on many factors.
Multiple amputees and thigh amputees derived a financial benefit by becoming medically retired as soon as their general condition was stabilized. Therefore, many of these amputees were not fitted with prostheses, but were discharged from Army Hospitals to Veterans Administration Hospitals with open wounds, making subsequent follow up difficult. Large numbers of casualties at certain times of the war stimulated early medical boarding and transfer of amputees from CONUS active duty hospitals to Veterans Administration Hospitals. In some CONUS medical cen-
137
ters, it was feasible to award the patient amedical discharge from the service and, yet, tocontinue treating him as an inpatient under a medically retired status.Thus, continuity of carewas not interrupted, and the patient continued the rehabilitationprogram and prosthetic fitting atone institution.
In the course of the Vietnam War, no medical centers in CONUS were designated as “Amputee Centers,” with the possible exception of Valley Forge General Hospital, which was given the authority on 1 February 1969 to establish an amputee service “to direct and supervise the care of all amputees in the hospital” (LaNoue 1971).
In the majority of the hospitals, the amputees were not segregated onto a separate ward or into a specific “amputee service.” They were mixed with other orthopedic and trauma patients with a variety of orthopedic surgical diagnoses. In such a milieu, rehabilitation efforts were directed to the patient with multiple injuries, whether he was an amputee or whether he was otherwise injured. In treatment centers other than Valley Forge, less formal arrangements were made in which one or more staff members concentrated their efforts on the overall management of the amputees. Due to the high volume of patients with amputations, who comprised 10 percent of the orthopedic census at any one time, there appeared to be no difficulty in one amputee relating to another, although they were on a general trauma ward. The amputees usually benefited from this interaction with each other.
MANAGEMENT OF AMPUTATIONS CLASSIFIED BY ANATOMICAL SITE
FootAmputations
In managing foot amputations, surgeons strove to preserve all available skeletal and viable soft tissue length. Omer and Pomerantz (1972) stressed the preservation of as many segments of the foot as possible. [In a separate chapter of this volume Ballard also discusses amputations as related to other injuries of the foot.] Toe amputations, with the exception of the large toe, generally needed no special considerations. Amputation of the large toe at the metatarsophalangeal joint interfered with running and fine balance adjustments, but did not present a major problem in ordinary ambulation. Transmetatarsal amputations were relatively infrequent in the Vietnam War and usually were maintained at the level of initial loss if sufficient skin flaps were present.
The eventual functional results of amputation of the lateral two rays of a foot were usually good, allowing ambulation with a filler in the shoe. However, feet sustaining amputation of the entire first ray, particularly if any involvement of the second ray was present, usually had to be revised to a Syme’s amputation later because the remaining lateral rays generally proved insufficient for painless efficient weightbearing.
When traumatic amputations through the midtarsal area (Lisfranc) and through the midtarsal-tarsal joint (Chopart) occurred, usually insufficient skin remained to cover the terminal ends of these wounds. Small antipersonnel mines (“toe-poppers”) caused only partial injury to the bone and vascular structures, but destroyed the skin on the plantar aspect of the foot. These injuries were best treated by early Syme’s amputation, as the functional results of a skin-grafted plantar surface of the foot were usually poor. Such management was an exception and counter to the concept of retaining as much skeletal support as possible until secondary revisions could be accomplished.
138
Experience at Fitzsimons General and in other CONUS hospitals indicates that the majority of patients who had Lisfranc or Chopart level amputations required later revision and amputation proximal to those sites. Muscle imbalances resulting from Lisfranc and Chopart amputations caused the remaining mid-foot and hind foot to go into progressive equinus and varus. If some of the ankle dorsiflexors and foot evertors remained or were reattached surgically or spontaneously the deformity could be avoided. Transfer of the posterior tibial tendon through the interosseous membrane to the dorsum of the remaining mid-foot was accomplished successfully in one patient at Fitzsimons General Hospital. This patient had a severe injury to the contralateral extremity, and it was desirable to maintain as much proprioceptive function in the foot amputation as possible. Weakening of the gastrocnemius-soleus muscle group by early lengthening should be considered when equinovarus overpull is present.
Prosthetic fitting of the transmetatarsal amputee usually required only a filler in the shoe. The coincidental development of a polypropylene foot-ankle orthosis in the civilian community during the Vietnam War allowed patients with Lisfranc and Chopart-level amputations to obtain more functional and less bulky fitting forefoot prostheses.
The underlying causes of an extremely high failure rate of primary Syme’s amputations performed at the initial treatment hospitals may never be known. However, some of the following facts should be considered. The surgical technique of Syme’s amputations is exacting, particularly in the need to preserve an adequate blood supply to the plantar flap. A careful, unhurried dissection, based on exact knowledge of the anatomy, is necessary. It is possible that at least some of these amputations were performed by surgeons inexperienced in Syme’s amputations, or that mass casualty situations prevented some surgeons from spending the time necessary for a proper dissection.
Another and probably more crucial factor in the survival of the flap was the method of stump stabilization after the operation. The Syme’s amputation flap could not be placed in a conventional circumferential skin traction apparatus. At the U.S. Army Hospital, Camp Zama, Japan, a number of patients with primary Syme’s amputation stumps arrived with necrotic flaps. These were apparently due to a dropping, posteriorly, of the unsupported plantar flap, causing an acute folding or torsion (or both) at the base of the flap that caused vascular compromise. The majority of the patients with Syme’s amputation stumps arrived in Japan without adequate stabilization by either external or internal means. A limited number arrived with either Kirschner wires or Steinmann pins traversing the flap into the distal tibia. Although this method seemed to support the flap in proper anatomical relationships, in some cases, there was still some folding of the base of the flap and necrosis in the distal portion of the flap.
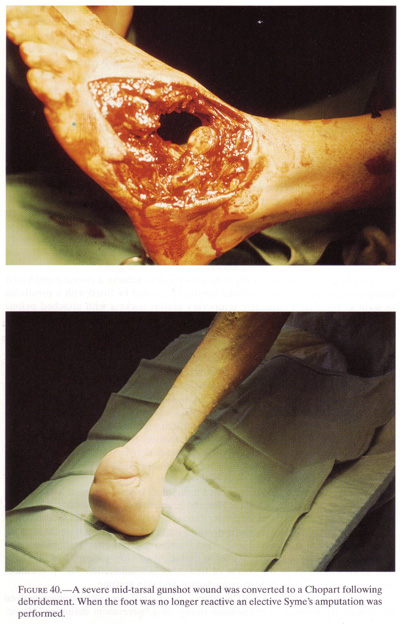
The Vietnam experience suggests that a primary Syme’s amputation should not be performed as the initial debridement procedure, which should consist of removing all obviously nonviable soft tissue and any skeletal elements of the foot that do not provide longitudinal length for the support of the remaining viable soft tissue. Later, when wound healing was stabilized, a secondary revision to a Syme’s amputation could be accomplished with much less risk of loss of the plantar flap. Experience at the 106th General Hospital confirmed that a large number of partial flap necroses occurred secondary to battlefield first-stage Syme’s. However, the majority of the patients in that series were still able to retain a Syme’s-length amputation
139
stump and were fitted with a Syme’s prosthesis. This suggests that even though a partial flap necrosis occurred, a below-knee amputation was not necessary (fig.40).
During the Vietnam War, some important techniques evolved regarding secondary revision to a Syme’s amputation. To provide a good, stable end-bearing Syme’s stump and to avoid an unstable condition of the end pad, the extrinsic tendons were cut as high as possible and allowed to retract. The soft tissue pad was then stabilized by means of adhesive strapping and plaster external immobilization for six to eight weeks. To streamline the shape in some cases, the malleoli were shaved. This procedure allowed a better cosmetic prosthetic fit and, for best results, was done only after the Syme’s stump was well vascularized and well healed, not at the initial amputation.
Below-Knee Amputations
In the majority of below-knee amputations performed during the Vietnam War, particularly toward the latter stages, an effort was made to preserve as much length as possible. Usually, the occasional primary closure and the more frequent delayed primary closure stump wounds healed completely or partially with some skin-edge necrosis and drainage, but some were total failures. The stumps that were surgically closed and then had to be opened for redebridement were usually treated with traction and gradual closure with the aid of Steri-strip or skin grafts.
The primary aim in the CONUS hospitals was to achieve a closed noninfected stump (without sacrificing functional length) that could be fitted with a prosthesis as soon as possible. Frequently, temporary plaster sockets with attached pylons were applied to both open and closed immature stumps. Fitting a prosthesis on a patient promoted his functional psychological rehabilitation. Emphasis was placed on ambulation, as soon as possible. Generally, prolonged bedrest and use of wheelchairs were discouraged. Early ambulation and mobilization appeared to enhance the healing of associated lower extremity fractures.
Varying methods and techniques were used at different times and in different centers to facilitate closure of the open below-knee amputation. Some of the methods used at one time or another in treatment of below-knee amputees included: skin traction of either continuous or intermittent type until closure of wound; delayed primary closure; secondary closure by revision; Steri-strip closure; a temporary plaster socket to the open stump with attached pylon, and early ambulation until closure; either split-thickness or mesh-type skin grafts to the end or sides of the stump; and pedicle flap coverage of the stump.
Medical records of amputees from Fitzsimons General Hospital and patients passing through the 106th General Hospital in Japan were evaluated to determine the efficacy of each of these methods. Retrospectively, it is difficult to determine the exact extent of skin traction effectiveness during the first several weeks after injury. This is because, in many cases, skin traction was not effectively maintained during the initial stage when it was most useful. Also, many patients had skin traction at varying times in the course of treatment in combination with procedures such as secondary revision, Steri-strip closure, and skin grafting.
In definitive-treatment CONUS centers, several different philosophies evolved concerning the revision of below-knee stumps to a “permanent definitive” stump.
140
{kind=link}
141
At some of the centers, the majority of amputations were treated with one of the methods until skin was essentially healed. Then, after a medical board, the patient was discharged from the hospital and transferred to a Veterans Administration Prosthetic Facility. Others used different management methods. At Fitzsimons General Hospital, the majority of below-knee amputees were fitted with “permanent” prostheses without revision to a “more permanent-type” stump. Most of these patients were able to tolerate a patella-tendon-bearing socket with soft end pad without revision of scars on the end of the stump.
At Valley Forge General Hospital, emphasis was placed on performing more definitive type revisions to eliminate redundant soft tissue and adherent scar and to provide a more stable amputation stump. An Ertl-type revision, creating an osteosynthesis between the distal tibia and fibula, was performed successfully in a number of cases (Deffer 1970; Moss 1970). Special prosthetic fitting was necessary to fit the shape of altered stump and to allow for the end weightbearing characteristics of this type of amputation.
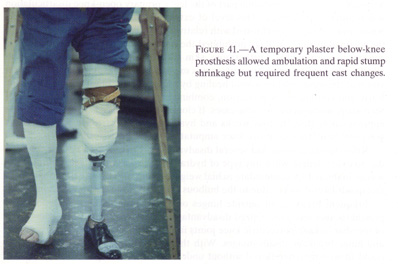
Several hospitals emphasized the use of temporary plaster sockets with attached pylon and foot to treat those amputees with immature stumps (fig.41). This early weightbearing method, which also was used in World War II (Wilson 1969), rapidly decreased stump swelling in both open and closed stumps. At Fitzsimons General Hospital, a number of open amputation stumps were treated in this manner. The plaster sockets had to be changed every 3 to 5 days to accommodate the rapid shrinking of the stump, especially in the early phases of treatment. It was important to follow the detail of temporary plaster socket application as described by Burgess et al. (1969) to avoid breakdowns in normal skin areas due to poor fitting plaster.
Occasionally, closed revision of a below-knee amputation stump with immediate fit of a temporary plaster socket effectively controlled stump edema. However,
{kind=link}
142
it was found detrimental to the closedincision site if the patient began full weight-bearing earlierthan seven to ten days after the closed revision.
Short below-knee amputation stumps (arbitrarily listed as less than four inches of tibial length) frequently were skin-grafted or allowed to close secondarily. Another approach to the short below-knee amputation was the use of pedicle flaps to provide more durable skin surface for prosthetic fitting. To aid in future ambulation, preservation of the knee joint, even with a short stump sometimes measuring only 2.5 to 5.0 cm. (1 to 2 inches) it was desirable to provide proprioceptive feedback and overall stump length. Anesthetic skin flaps did not present a problem in fitting the prosthesis or in its acceptance by the below-knee amputees (Keblish et al. 1970). Sometimes lack of skin about the knee joint meant revision of the short below-knee stump to an above-knee amputation rather than knee disarticulation.
An ipsilateral fracture of the femur was a common complication. Twenty-one ipsilateral femur fractures associated with below-knee amputations were treated at Fitzsimons General Hospital and fourteen were recorded in a series at Valley Forge General Hospital (Herndon et al. 1973). Initially, the femur fracture reduction was maintained by means of a pin through the proximal tibia with balanced skeletal traction. After the patient reached one of the CONUS treatment facilities, a modified cast brace was applied which incorporated the Steinmann pin in the cast brace. A pylon and solid ankle cushion heel (SACH) foot was attached. In some cases, the knee could be mobilized by appropriately placed knee hinges.
Knee Disarticulation
When it was apparent that a below-knee level amputation would not remove all nonviable tissue in the proximal part of the leg, a primary open-knee disarticulation was frequently performed. This level of extremity removal for debridement purposes could be rapidly performed with relatively little blood loss. It was alleged that the retained hyaline cartilage prohibited the proximal spread of infection, but this concept is questionable. Furthermore, skin grafts over this area took poorly, if at all, after the hyaline articular cartilage was exposed. Secondary closure by either revision at the same level or wound healing by secondary intention was unsuccessful. Early and continuous skin traction, combined with delayed closure by suture or Steri-strip, was effective in some cases. If closure had not been accomplished within approximately three to four weeks and hyaline articular cartilage decomposition was prominent, then an above-knee amputation had to be performed.
Knee disarticulations had several disadvantages. First, there was poor cosmesis due to excess length when any type of hydraulic knee was fitted, and second, there was an inability to accommodate ischial weightbearing with the use of the total contact quadrilateral socket, due to the bulbous condyles at the end of the stump.
Frequent breakage of outside hinges on a conventional knee disarticulation prosthesis also was a recognized disadvantage. The introduction of two new types of four-bar linkage polycentric knee joints in the late 1960s alleviated the cosmetic and hinge breakage disadvantages. With this new type of knee joint, the patient could sit with the knee flexed without undesirable excess length of the prosthesis.
143
At Oakland Naval Hospital, thirty-three patients with knee disarticulations underwent osteoplastic revision of the distal end of the stump, excising the prominent femoral condyles as described by Mazet and Hennesy (1966). This surgical modification of the stump allowed fitting of total contact quadrilateral suction sockets (Utterback and Rhobrer 1973).
Above-Knee Amputations
As much thigh length as possible was kept at the time of initial amputation in order to provide a biomechanically functional remnant and to obtain a closed stump. All methods described for the treatment of the below-knee amputee were applicable, in some form, to above-knee amputations. Frequently, the injuring agent also caused trunk, upper extremity, and contralateral extremity wounds, as well as the above-knee deficit. The number of bilateral above-knee and triple amputee patients was significant.
Early application and maintenance of skin traction was useful in closure of the open-circular type and equal-flap type amputations. Many of the above-knee stumps, however, had irregular flaps with large areas of skin loss and proximal wounds, all of which tended to negate the effects of conventionally applied skin traction. Split-thickness skin grafts, particularly the mesh type, were helpful in covering these large irregular wounds, especially in the short above-knee stump. Steristrip closure also played a part in decreasing wound size.
In a number of instances the above-knee amputations were performed because a vascular repair failed at the site of a thigh wound that also included a fracture of the femoral shaft. In some cases, amputation was performed through the fracture site, thus removing a potentially useful distal segment of femur which could have been used ultimately to provide a longer stump and thereby improve the patient’s ambulation. Another reason that amputation should not have been performed through the fracture site was that there was frequently a chance that the surrounding soft tissues would support union of the femur fracture, which would result in a longer and more functional stump.
At the time of secondary stump revision, a few surgeons performed myodesis or myoplasties to provide increased muscle control and proprioceptive feedback as advocated by Weisse, perhaps because identifying the muscles and reestablishing muscle length in these traumatic amputees were difficult. An important consideration in ultimate fitting of the above-knee amputee’s prosthesis was excess bulk, particularly on the end of the amputation stump. This bulk caused relative instability of the femur within the above-knee prosthetic socket. Some amputees developed a painful bursa beneath the excess muscles as they rubbed across the bone end.
Special problems occurred in the management of amputation wounds of the high thigh, hip disarticulation and hemiplevectory type. Contamination of the wounds by fecal material was prevalent, particularly in those amputees with high bilateral losses. A diverting colostomy was performed in many of these patients. This procedure significantly decreased wound contamination by fecal material. Skin traction could not be effectively applied to these areas by the usual methods. One method, utilizing wire sutures placed through the skin edges and attached to traction, was im
144
provised, but this technique could be usedonly for a short time, a few days at the most, beforethe wires would necrose the skin edges and pull out.
Hand Amputations
The upper extremity amputee presented a different challenge to the trauma surgeon. While the lower extremity amputee needed a stable skeletal support, surrounded by mature, nonpainful soft tissues and durable skin which could tolerate both high friction and pressure loading, the upper extremity amputee needed to retain as much sensitivity as possible in the remaining part of the extremity. The untrained, unilateral upper extremity amputee transferred many functions to the remaining intact hand and seldom used the extremity with the amputation. Therefore, one of the major aims in management of the upper extremity amputee was to reduce the natural tendency for complete substitution of all functions to the intact hand.
Initial treatment of the wound causing loss of the distal portion of the upper extremity involved thorough debridement of any nonviable soft tissues. Every effort was made to maintain as much of the skeletal support as possible as well as to preserve skin for use in later reconstruction. After initial debridement and during subsequent stages of care, skin traction was applied. In many cases, this hastened closure of the wound. Delayed primary closure and secondary closure by suture or skin graft were also used, as required, without shortening of the amputation stump.
In general, utilizing these methods of care, the wounds of the upper extremity amputee healed more favorably than those wounds treated by the same methods in the lower extremity amputee (LaNone 1971).
Wrist Disarticulation
A wrist disarticulation was performed whenever there was an intact distal radius and ulna as well as sufficient skin flaps to cover the bone ends. This level of amputation was considered more functional then a medium or long below-elbow amputation. The expanded shape of the radius and ulna allowed for a more “rectangular” configuration, providing a large stable contact area for the socket.
There were, however, major disadvantages with this level of amputation. This long stump, when fitted with a prosthesis, had a total length as long or longer than the normal extremity. This added length had poor cosmetic qualities because it accentuated the presence of the prosthesis and amputation condition. It also precluded the use of a self-contained electronic terminal device. This “electric arm” needed space between the stump and terminal device to house the batteries and integrated electronic components. In one survey of amputee clinic chiefs, 56 percent preferred the long below-elbow amputation to a wrist disarticulation (Newsletter 1970).
Below-Elbow Amputations
The short below-elbow stump was preferable to an elbow disarticulation or an above-elbow amputation. Full thickness skin graft coverings were accomplished in a few cases to preserve this lower level of amputation, thereby preserving motion at
145
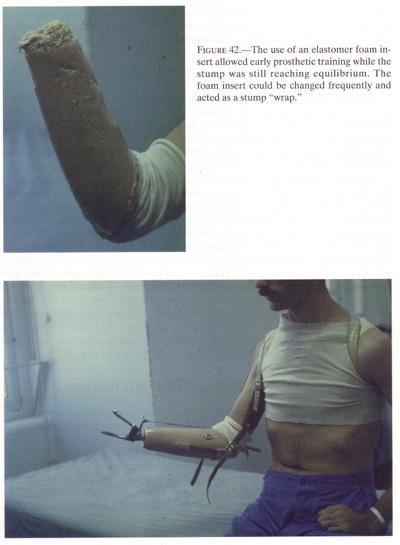
the elbow joint. Salvage of the shortbelow-elbow amputation with pedicle flap skin coveragewas achieved in some cases. Fitting by means of a Munster-typebelow-elbow socket made useof the preserved proprioception and elbow motion in these shortbelow-elbow stumps (fig.42).
{kind=link}
146
Rehabilitation for below-elbow amputees began with learning to use a temporary training prosthesis. At Fitzsimons General Hospital, thirty-eight below-elbow amputees were treated with application of temporary upper extremity prosthetic training devices. Plaster sockets with attached terminal devices and appropriate harnessing allowed early functional rehabilitation and training to negate some of the tendency for the patient to become entirely “one-handed.” At the same hospital, an oversized laminated socket filled with Elastomer foam to make a custom fit for the stump was used as a temporary training arm while awaiting stump maturity and permanent prosthetic fitting (Burkhalter et al. 1976).
Elbow Disarticulations and Above-Elbow Amputations
Retraining the humerus in extremely short above-elbow amputees was advantageous because this benefited the shoulder joint contour cosmetically and provided some base for suspension of a prosthesis. As the upper extremity level became progressively shortened, the patient acceptance rate became lower; however, six of nine shoulder disarticulation patients at Fitzsimons General Hospital were considered prosthetic wearers one to two years after amputation (Burkhalter et al. 1976).
A few patients with elbow disarticulations were fitted with prostheses that utilized the condyles of the humerus to aid in suspension. An additional advantage of disarticulation was better rotational control of the socket on the stump, provided by the prominent condyles of the humerus. Prosthetic fitting of external elbow joint hinges was necessary to avoid excess length. This was a minor disadvantage and, due to the relatively low stresses applied, breakage of the hinges was not a common problem. As much length as possible of the above-elbow stump was preserved and, frequently, to preserve the skeletal length, skin grafts were applied over open areas. These skin grafts were particularly useful in covering short above-elbow amputations. At Fitzsimons General Hospital, twenty-nine above-elbow amputees were fitted with temporary training arms, and early functional use of the extremity was emphasized. This training arm was similar to the one described for the below-elbow amputee--an oversized laminated plastic socket with an interposed Elastomer foam between the stump socket and the attached elbow-terminal device unit (Burkhalter et al. 1976).
SPECIAL PROSTHETIC CONSIDERATIONS
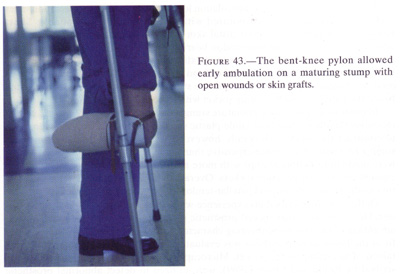
Responding to the need to place the lower extremity amputee in the upright walking position to enable him to return to useful society as soon as possible, a number of special prosthetic devices were originated in the CONUS treatment centers. Temporary plaster sockets with attached pylons and feet were used. In lieu of the temporary plaster socket and pylon, seventy-five below-knee amputees were fitted with bent knee pylons at Fitzsimons General Hospital. These lightweight devices, constructed from aluminum crutches, featured a supporting platform and a pelvic band which allowed the amputee freedom from crutches. Thus, he could use his upper extremities for other activities (fig. 43). When below-knee amputees with flexion contractures used this device, their contractures decreased (Pinnell and Mayfield 1972). A similar
147
{kind=link}
stump-containing device with attached pylons, both articulated and nonarticulated, was attempted for the above-knee amputees but did not prove successful.
The bilateral above-knee amputee presented a challenge throughout the rehabilitation phase. To lower the center of gravity and to aid the balance of the amputee, he was fitted with a “stubby” training prosthesis. The device allowed the patient to get out of the wheelchair early and, frequently, to walk without crutches or canes on the first attempt (Brown 1970).
Although stubby prosthesis permitted the bilateral above-knee amputee early ambulation and balance training, personal communications with some of these patients indicated a negative psychological impact. The rather marked foreshortening was considered demeaning, though they realized this pair of “stubbies” was only a temporary mode in their rehabilitation cycle. Later at Fitzsimons General Hospital (February 1970 to October 1972), this problem was circumvented by fitting 17 bilateral above-knee amputees with early temporary plaster quadrilateral sockets and four-bar linkage polycentric nonhydraulic knee joints. These Polycadence knee units were extremely stable in stance phase and allowed the amputee to stand with normal length prosthetic devices. Frequently, he was able to ambulate with minimal assistance after several days (Mayfield and Burkhalter 1973; Mayfield 1971).
The fitting of permanent prostheses at the centers that retained amputees until they could be fitted was influenced in part by the simultaneous development of prosthetic innovations in the civilian community. Cooperation with the Veterans Administration Prosthetics Research Unit allowed introduction of some of the newest developments in prosthetic research to the men who incurred amputations from wounds during the Vietnam War.
148
For the Syme’s and knee disarticulation level amputees, sleeve-type slip-in inner sockets with suspension incorporated within the socket were available. Short below-knee amputees with poor distal skin surface were often fitted successfully with a variance of the patellar-tendon-bearing prosthesis. The total contact hard patellar-tendon-bearing socket was used extensively to fit the more mature below-knee stumps. A soft Silastic material endpad was used with a hard socket to accommodate changes of the relatively immature stump. Some amputee clinics continued to use the patellar-tendon-bearing socket with a soft Kimbrough liner.
In order to accommodate immature stumps that could be expected to change dimensions rapidly, certain heat labile plastic substances, such as Polysar, were used to construct the sockets. Generally, however, these sockets were more time-consuming to construct and more expensive than a temporary plaster socket. Attempts were made to fit mature stumps with more advanced socket designs, including air-cushion sockets and gel-lined sockets. Overall, these attempts were not as satisfactory as the more conventional patellar-tendon-bearing hard or soft sockets.
Deffer (1970) described his experience with nearly one hundred Ertl osteoplasties. He emphasized that specialprosthetic considerations were necessary to take advantage of the end weightbearing characteristics of this revised stump. Accurate fit of the below-knee prosthesis was evaluated by use of weightbearing x-rays obtained of the stump in the socket. Microcapsule pressure-sensitive sockets, as described by Brand and Ebner (1969), were utilized to detect abnormal prosthetic socket pressures on the skin of the stump.
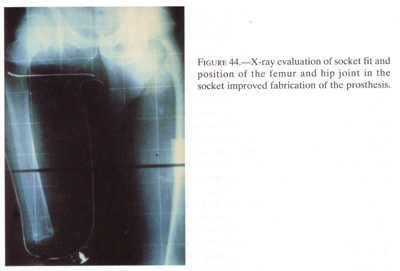
A radiographic technique was developed at Fitzsimons General Hospital to assess the socket fit and the relative adducted/abducted position of the hip joint on the amputation side. The x-rays were taken with the patient standing and with the heels two inches apart. It was found that the majority of prostheses were fitted with the amputee’s hip in abduction and with poor stump support by the lateral wall of the socket. This alignment placed the hip abductor muscles at a disadvantage and gluteus melius type of gait was present. This x-ray technique was utilized during the prosthetic fitting process to assure proper adduction position of the hip (fig 44).
The majority of above-knee amputees were fitted with prostheses containing either constant-friction single-axis knee joints or assorted swing-phase-control hydraulic or pneumatic units. The Henche, Mauke S&S knee joint unit, which incorporated a more stable stance phase mode, was fitted to both unilateral and bilateral above-knee amputees at Fitzsimons General Hospital and Walter Reed Army Medical Center (Baker 1970). An amputee fitted with a prosthesis of this type of knee joint required special training before he could utilize all of the features properly. After 1969, at Fitzsimons General Hospital, the majority of bilateral above-knee amputees were fitted with four-bar linkage Polycadence knee joints, which provided stance phase stability and allowed the amputee to walk with only one cane. Four amputees were fitted with a Polycadence knee on one side and a Henche, Mauke S&S knee in the opposite prosthesis. This was a favorable combination because the patient could use the S&S knee to aid in sitting and descending stairs while the Polycadence knee provided stance phase stability. A four-bar linkage, polycentric knee with a swing phase hydraulic cylinder was used in some prostheses in the latter stages of the Vietnam War. This combination was used to the best advantage when fitted in those amputees with knee disarticulations or long above-knee level amputations.
149
{kind=link}
LESSONS LEARNED
Preservation of the major bony skeletal structures of the extremity at the most distal level possible is recommended to serve as a supporting strut for any viable soft tissue. This tissue is useful in later reconstructive stump revision even though the bone itself may not be preserved for the eventual amputation level. Conversion of the traumatic Lisfranc or Chopart level of foot amputation to a Syme’s amputation at a later time is an example of this concept.
Irregular stump configurations maintaining viable skin flaps and other soft tissue that can be used to cover critical skeletal elements proximally should be salvaged. Initial circular amputation through a “site of election” should be avoided, particularly if variable skin flaps can be retained for use in reconstruction of a stump that saves a functioned joint. For example, with soft tissue flaps to cover a short skeletal segment of a below-knee stump, we could salvage the critical function of the knee joint.
Exploding weapons, such as mines at ground level, frequently propelled foreign inorganic and organic material, as well as the amputee’s own bone fragments, deep into the proximal tissues. The only evident open wound was the traumatic amputation, the more proximal skin remaining intact. If proximal trauma was not suspected and proximal debridement neglected these foreign elements and surrounding tissue, necrosis secondary to their high velocity passage was as source of deep infection and potential loss of limb at a level proximal to the traumatic amputation site. A high index of suspicion of this condition in all blast-type amputations was necessary, and adequate proximal longitudinal incisions, frequently the length of the proximal limb segment, were required to perform adequate debridement of the wound. Proximal
150
swelling associated with contaminated traumatically dissected tissue planes at the amputation level, the “dirty envelope syndrome,” was a clue to pursue proximal dissection along these planes. An x-ray of the proximal limb segment was a necessity and could reveal proximally driven stones, metal, or bone, or air in the soft tissue. The most common example of this occurrence was the blast injury incurred below-the-knee amputation with contamination and necrosis of the adductor area of the thigh. Exploration of the knee or hip joints should be considered in all blast injury--incurred amputee patients if there is any suggestion of proximal contamination.
Retention of the knee joint with intact muscles and nerves to provide motion and proprioceptive feedback in below-knee amputees promoted more stable gait patterns than were possible for above-knee or knee disarticulation amputees. An open circular amputation stump with only two inches of tibia should be retained with split-thickness skin grafts, secondary thickness pedicle flap coverage, or eventual closure by secondary intention wound healing to complete the skin coverage.
Statistics show that delayed primary closure of selected “clean” amputation stumps allowed the least time before prosthetic fit as compared with all other courses of wound management. Many factors contribute to the decision to perform a delayed primary closure of a traumatic amputation stump in a war zone environment. The surgeon must have considerable experience in wound evaluation, particularly in assessing tissue for contamination and viability. Adequate skin must be available to close the wound without tension at the suture line, and the operating surgeon must be able to evaluate the wound and patient’s response to delayed primary closure for at least seven days postoperatively. If deep infection or tissue necrosis occurs, endangering either the patient’s life or eventual stump length, the surgeon must not hesitate to perform a “delayed primary opening” procedure and to remove all sutures in the stump. Then he must perform meticulous redebridement of the stump. A switch to an open method of skin traction and plaster dressings will then be necessary.
Temporary plaster sockets with attached pylons and prosthetic feet were used successfully in CONUS hospitals. These allowed ambulation of the lower extremity amputee within a few weeks after amputation (Mayfield and Burkhalter 1972). The increased mobility of the amputee in an upright walking posture contributed significantly to positive mental attitudes as compared to those amputees treated by the nonambulatory methods of continuous skin traction in bed. Ambulation also contributed to rapid stump shrinkage and maintenance of proximal muscle group tone and coordination. Maximum advantage of this ambulatory treatment was obtained by applying the temporary socket and pylon approximately ten to fourteen days after stump closure by delayed primary closure or secondary revision. In the interval between closure and pylon fitting a temporary nonweightbearing plaster dressing was used to immobilize soft tissue, to decrease pain and edema, and to protect against direct external forces (Mayfield and Burkhalter 1972).
Open stumps that could not be closed safely or those that broke down after closure were treated by immediate application of weightbearing socket and pylon after another thorough debridement. These stumps closed eventually by secondary intention. Meanwhile the patient was ambulatory and maintained the functional length of the salvaged longer stump. Relatively little pain was experienced by the amputee with an open stump ambulating in a socket-pylon.
151
After surgery on the upper extremity amputation stump, the patient was immediately fitted with a temporary plaster socket or an oversized laminated socket filled with Silastic foam and an appropriate terminal device with harness attached. This permitted early prosthetic training and return to functional activities. When early functional use of the extremity was obtained by this method, phantom pain syndrome was reduced.
Observations were repeatedly made at the PACOM and CONUS hospitals that, despite the impressions of evacuating surgeons that skin traction was “always” applied before evacuation, skin traction was not maintained in the evacuation route. This was unfortunate because skin traction only to the distal two inches of skin was essential in the initial phases of treatment and evacuation, if early closure of the open amputation was to be achieved. This was true irrespective of the subsequent closure method, be it delayed primary closure, continued skin traction, skin grafting, or plaster socket and early ambulation.
Therefore, should future wars require evacuation of amputees, a uniform inter-service education program should be designed that includes established guidelines and specific directives concerning maintenance of continued skin traction to the stump by self-contained methods. A well-applied plaster cast immobilizing the joint most proximal to the amputation level with attached outrigger continues to be the most satisfactory method of achieving this goal.
Abrupt massive bleeding from failure of the proximal vein graft anastomosis was observed in some amputees who had amputations through the thigh at the level of the grafting procedure. To prevent this dramatic complication, the vein graft should be removed and ligation of the most distal part of normal artery done at the time of amputation.
Diverting colostomies should be done in patients with hip disarticulations, hemipelvectomy, and high above-knee amputations early in the course of treatment to decrease local fecal contamination of the wound.
Myodeses and myoplasties have been described as beneficial in producing stronger and more functional stumps through reestablishment of myoneural reflex patterns. However, most of the traumatic-type amputations sustained in the war zone were not amenable to this procedure. Ertl osteoplasty revisions of the longer below-knee stumps were performed frequently in some centers. This procedure created a stump allowing more stability and a closer contact prosthetic fit with end weightbearing than the ordinary below-knee stump. It is recommended for selected, well healed below-knee stumps.
Several innovations in prosthetic design and manufacture which occurred during the rehabilitation period of our Vietnam War amputee population proved beneficial. The Henche, Mauke S&S hydraulic knee was popular for the active young unilateral above-knee amputee. Stable four-bar linkage knee systems, sometimes in combination with the S&S knee unit, were utilized to ambulate the bilateral aboveknee amputee in some centers (Mayfield 1971).
Myoelectric devices to drive powered upper extremity protheses were introduced to selected upper extremity amputees through the Veterans Administration and Northwestern University combined research program. Acceptance rate was variable, however, and the more conventional “hook” was the most widely accepted terminal device for upper extremity amputees.
152
In summary, many different types of amputee management were performed during our years in Vietnam. As the war progressed, the concept of maintaining a viable skeletal strut and retaining all possible viable skin flaps evolved as a basic guideline in most amputations. Meticulous debridement had no substitute, and included a search proximally for possible fragments or vascular injuries. Early evacuation had its advantages, but some patients suffered from lack of traction being maintained to the open stump. In CONUS, rehabilitative efforts were focused on early weightbearing for the lower extremity amputee and early functional use of the prosthesis (or orthesis) for the upper extremity amputee.
REFERENCES
Baker, G. I. 1970. Communications from the clinics. Newsletter. Amputee Clinics. 2, #1.
Brand, P. W., and Ebner, J. A. 1969. Pressure-sensitive devices for denervated hands and feet. J. Bone and Joint Surg. (Am) 51:109-16.
Brown, P. W. 1970.Rehabilitation of bilateral lower extremity amputees. J. Bone andJoint Surg.(Am) 52:687-700.
Burgess, E. M.; Romano,R. L.; and Zetti, J. H. 1969. Themanagementof lower extremity amputations.Washington:Prosthetics and SensoryAids Service, Veterans Administration.
Burkhalter, W. E.;Mayfield, G. W.; and Carmona, L. 5. 1976. The upper extremity amputee.Early and immediate post surgical fitting. J. Bone and Joint Surg.(Am)58:46-51.
CINCPAC-2. 1968.Commander in Chief, Pacific. Second CINCPAC Conference onWar Surgery. Tri-service surgical conference conducted at John Hay AirBase,the Philippines, 25-28 March 1968.
Deffer, P. R. 1970. More on the Erti Osteoplasty. Newsletter. Amputee Clinics. 2, #1.
Hampton, O. P., Jr.1957. Orthopedicsurgery in the Mediterranean Theater of Operations. Office of The Surgeon General, Department of the Army. Washington: GPO.
Hampton, O. P., Jr.1966. Report of consultant tour, 15 February-25 March 1966.
Herndon, J. J.; Tolo, V. T.; LaNoue, A. M.; and Deffer, P. A. 1973. Management of fractured femurs in acute amputees. J. Bone andJoint Surg. (Am) 55-1600-1613.
Keblish, P A.; LaNoue,A. M.; and Deffer, P. A. 1970. Preservation of the short BK amputationstump withpedicle flaps. Presentation at Eastern Orthopaedic AssociationMeeting.
LaNoue, A. M. 1971. Care and disposition of amputee war casualties. Student Paper, U.S. Army Command and General Staff College.
Mayfield, G. W. 1971.Experience with polycadence knee joint. Newsletter. Amputee Clincs.3, #2.
Mayfield, G. W., andBagg, R. 1978. Longitudinal survey of 169 RVN amputees created.(Unpublished data) 106th General Hospital (Japan).
Mayfield, G. W., andBurkhalter, W. E. 1972. Treatment of open ambulation stumps bytemporary prostheses and early ambulation. ScientificExhibit, AmericanAcademy ofOrthopaedic Surgeons Annual Meeting.
Mazet, R., Jr., andHennesy, C. A. 1966. Knee disarticulation and a new knee jointmechanism. J.Bone and Joint Surg. (Am) 28:126-39.
Moss, J. H. 1970. Moreon the Ertl Osteoplasty. Newsletter.Amputee Clinics. 2, #2.
NATO Emergency war surgery handbook. 1958. Department of Defense. Washington: GPO.
153
Omer, G. E., Jr., and Pomerantz, G. M. 1972. Initial management of severe open injuries and traumatic amputations of the foot. Arch. Surg.105:696-98.
Pennell, C. R., and Mayfield, G. W. 1972. Bent knee pylon for the below knee amputee. Physical Therapy 52:1051-55.
Utterback, T. D., andRhobrer, D. W. 1973. Knee disarticulation level as an amputation level.J. Trauma. 2:116-20.
Wilber, M. C. 1970.Combat amputees. Clin. Orthop.68:10-13.
Wilson, P D. 1969. Earlyweightbeaning in treatment of amputations of lower limbs. J. Bone andJoint Surg. 4:224-47.