



Chapter 8
PERIPHERAL NERVE PROBLEMS
Colonel George E. Omer, Jr., MC, USA (Ret.),and
Colonel William W Eversmann, Jr., MC, USA(Ret.)
Final disposition data from Army hospitals in Vietnam indicate an incidence of peripheral nerve injuries of approximately 7.3 percent of the nonmortal wounds from 1964 through 1973 (Bzik and Bellamy 1984; Rothberg et at. 1983). The same data indicated that 61 percent of 7,138 peripheral nerve injuries involved the upper extremity. Multiple nerve injuries were more common in the upper extremity. In a series of 653 patients with upper extremity injuries, 188 extremities had multiple nerve involvement (Omer 1974). Combined neurovascular injuries are frequent in battlefield trauma. The Vietnam Vascular Registry (Rich and Spencer 1978) recorded concomitant nerve injury in 42.4 percent and fractures in 28.5 percent of 1,000 acute major arterial injuries.
INITIALSURGERY
The presence or absence of a peripheral nerve injury was of very little consequence in the resuscitation and initial management of the wounded soldier. The nerve injury was the secondary result of the same hostile action that caused the extremity wound, which was handled in routine fashion. Associated fracture splintage and resuscitation was followed by wound exploration. At the 85th Evacuation Hospital, at Qui Nhon, Vietnam, there was a concerted attempt made to identify the nerve injury preoperatively and to explore the damaged nerve during the debridement procedure. This effort had a dual purpose--to protect damaged nerves during the wound exploration, and to identify the nerve injury and try to address its implications for subsequent management. The information that a median nerve that was nonfunctioning preoperatively had proved on exploration to be normal, contused, divided, or segmentally lost would be of enormous value to the doctors receiving the patient in the United States. Frequently, such information never reached the surgeons managing the patient definitively (Omer 1975). In most other hospitals in Vietnam, no definite search was made for the damaged nerve, but if one was found, a note was made regarding its continuity or the degree of injury that could be determined grossly.
Often, especially in the upper, extremity, a vascular injury would accompany the nerve injury. Although in such a situation some note should be made regarding the status of the nerve which was in close proximity to the damaged vessel, this was often not done. If a note was made, it would not necessarily be accurate, and incorrect information in such a circumstance could be more damaging than no information. Such mistakes were common, in part because only a few of the surgeons actually debriding extremity wounds had extensive experience in peripheral nerve surgery or were well enough versed in the cross-sectional anatomy to be able to identify dam-
156
aged nerves in the swollen, distortedextremity. In addition, since the main problem was wounddebridement and vascular repair, surgeons were reluctant to search fordamaged nerves beforevascular repair because it would prolong the ischemic period to thelimb. Searching aftervascular repair, however, might compromise the repair.
The diagnosis of peripheral nerve injury was more likely to be made in the communication zone, although it might be made on physical examination rather than by surgery. But an isolated peripheral nerve injury without fracture was not likely to be specifically addressed in a communication zone. Patient stabilization, wound control, and subsequent wound closure were the major concerns, and nonoperative and occasional operative stabilization of fractures before evacuation to the zone of interior were also carried out at this time. More frequently than not, wound closure would be obtained, rehabilitation of the extremity would be instituted, and splintage as required by occupational or physical therapy modalities or perhaps even a plaster cast would be added before the patient's evacuation. A patient with a long bone fracture might be held in the communication zone for a long period of time to gain some degree of skeletal stability before the application of the plaster cast for evacuation.
Because causalgia would easily develop within one to two weeks of injury, it was usually first seen in the communication zone. It has always been felt, perhaps incorrectly so, that causalgia is a problem that develops a number of weeks or months after the major mixed nerve injury, but our experience in Vietnam led us to conclude that it was essential to institute treatment early in order to bring about a successful conclusion of the causalgic problem. In general the more proximal the nerve injury and the less destructive in character the wound, the more likely the patient was to develop a causalgic pattern. The management of causalgia is not controversial, but certainly the results of the treatment options are far better with the institution of early treatment. The surgeons in the communication zone who initially recognized this phenomenon and began early sympathetic blocks and/or surgical sympathectomies are to be congratulated.
Depending upon the patient flow, the amount of hostile action, and the presence of associated injuries, patients with peripheral nerve damage could arrive in the zone of the interior within a few days of the initial injury with open wounds, or they could arrive several weeks following the initial injury in a plaster cast with a surgically closed and clean wound. Nevertheless, our initial plan was to obtain wound control, then to close the wound, and finally to achieve skeletal stability and rehabilitate the patient's injured limb. The time from nerve injury to definitive nerve repair or graft could be as long as a few weeks to several months. In most situations in the zone of the interior, the patient with a nerve injury had far more than an isolated nerve wound. He probably had a diffuse extremity injury that required skin grafting or closure with flaps. Perhaps bone grafts for skeletal stability were needed before the nerve injury could be addressed surgically. The surgeons responsible for these patients in the United States disagreed on their management. One group believed that as soon as the diagnosis of a peripheral nerve injury was made and as soon as the internal environment of the limb permitted an operative procedure, the nerve should be explored, grafted, or repaired as necessary (Brown 1970). A second group felt that spontaneous recovery was likely to occur in the majority of the patients and therefore, whether the injury was low or high velocity, watchful waiting and further rehabilitation of the limb was preferable to a secondary exploratory procedure (Omer 1982). In the majority of these cases, entering the limb to deal with a nerve injury early or as soon as a closed wound had been
157
obtained was probably not going to be useful. Surgical explorationmight well be needed in asmall number of patients treated by watchful waiting, limbrehabilitation, and other proceduresthat were required rather than by concentrating so much on nerveexploration and repair. Omerwas a proponent of watchful waiting, as much of the publishedinformation from Brooke ArmyMedical Center in Texas confirms. Although Brown from FitzsimonsGeneral Hospital inColorado was a proponent of early nerve exploration and repair, asrequired, and/or neurolysis,Omer felt that, since most of the nerve injuries were concussive innature and recovery waslikely to occur, surgical exploration was meddlesome.
Experience has demonstrated that the initial exploration and debridement and the delineation of the status of the nerve at the time of wounding (initial surgery) was extremely important. An additional exploration of the extremity could be avoided when a nerve palsy existed in a nerve that had already been explored and found to be in continuity although contused.
SPONTANEOUSRECOVERY
Sunderland studied, retrospectively, a series of patients during World War II and found spontaneous recovery in 68 percent (1972). Rakolta and Omer (1969) observed that spontaneous regeneration could be delayed up to eleven months without excluding the possibility of clinical recovery (table 8). Omer (1982) developed a prospective study of 595 gunshot wounds from Vietnam to determine the percentage of spontaneous recovery. Spontaneous recovery occurred in 227 of 331 low-velocity gunshot wounds (69 percent) and 183 of 264 high-velocity gunshot wounds (69 percent) (table 9).
TABLE 8 -Interval between injury and spontaneous recovery in gunshotwounds 1, 2
Prognosis is more accurate if the time required for return of clinical function is known. Omer (1974) selected two parameters for a time frame: (a) the interval after injury at which one-half of the nerves had recovered function, and (b) the interval after injury after which only 10 percent of the nerves recovered function. This established a time frame from three to nine months in 90 percent of the nerve lesions that demonstrated spontaneous recovery. Proximal (high) extremity injuries took a longer time to show clinical function than distal (low) injuries. Extensive injuries producing multiple nerve lesions needed a longer time period to show clinical function than isolated nerve injuries (table10).
158
TABLE 9. -Time scale in months for spontaneous recovery in gunshot wounds
TABLE 10. - Summary of upper extremity nerveinjuries at Brooke Army Medical Center
MANAGEMENT OF PAINFUL NEUROMA IN CONTINUITY AND CAUSALGIA
Many clinical syndromes involving burning pain, abnormal vasomotor response, and dystrophy have been described in medical literature since the American Civil War, the first major conflict in which high-velocity missile injuries were common. The dreadful pain associated with penetrating injuries of nerves was best described by S. Weir Mitchell, George R. Morehouse, and William W. Keen in their monograph in 1864, although the condition of causalgia had been described as early as 1813 by A. Denmark, another military surgeon whose patient was wounded in the arm at the storming of Badajoz (Sunderland 1972). Classic causalgia may have variants that are termed Leriche's posttraumatic pain syndrome (minor causalgia), Sudek's atrophy, or shoulder-arm-hand syndrome (Lankford 1980).
The incidence of causalgia has generally varied with the criteria used for diagnosis. Data from World War I and World War II indicate that causalgia occurs in 2 to 4 percent of wounds involving major nerves (Rothberg et al. 1983). Omer and Thomas (1972) indicated that in a 54-month Vietnam series, 74 percent of the cases of causalgia involved the median or sciatic-tibial nerves. These cases included a high incidence of multiple nerve injuries; only 21 percent were due to wounds distal
159
to the elbow or knee. The lower extremity wasinvolved more often than the upper extremity(table 11). In 49 percent of the cases in this Vietnam series, theonset of pain was within the firsttwenty-four hours after injury, and in 70 percent, it occurred withinthe first week (table 12).
TABLE 11 . - Causalgia: Nerves involved (1966-70), during Vietnam War 1
TABLE 12. - Causalgia: Time of onset of symptoms (1969-70), during Vietnam War1
Chemical Blocks
Treatment should be instituted as soon as the syndrome causalgia is suspected (tables 13 and 14). A central chemical sympathetic block should be performed promptly as a diagnostic test as well as a therapeutic procedure. The anterior approach is preferred for a stellate block, with a paravertebral injection of the lumbar sympathetic chain. While the patient is free from pain, an accurate physical examination of the extremity can be performed. Subsequent central blocks may utilize an anesthetic agent with a longer duration, such as bupivacaine. A series of four or five blocks should be given on consecutive days; one placebo of normal saline solution should be given during the series to confirm the diagnosis. The potential for the series of blocks to give permanent relief of pain is uncertain, but some generalizations were made. One block may give total relief or reduce residual pain to a tolerable level. The
160
effective duration of the first block mayexceed that expected of the agent, and subsequentblocks may give progressively shorter pain-free periods. Lastly, theblock gives relief only forthe duration expected from the anesthetic agent used (Omer and Seymour1969). If the blockseries produces total relief or reduction of pain to a tolerable levelfor progressively longer pain-free periods, the prognosis for permanentimprovement is excellent. If the block series givesshorter pain-free periods or less relief than expected, permanentimprovement should not beexpected (Bzik 1984).
TABLE 13.- Causalgia:Causative agent(1966-78), during Vietnam War 1
TABLE l4. - Causalgia: Results of treatment (1966-70), during Vietnam War 1
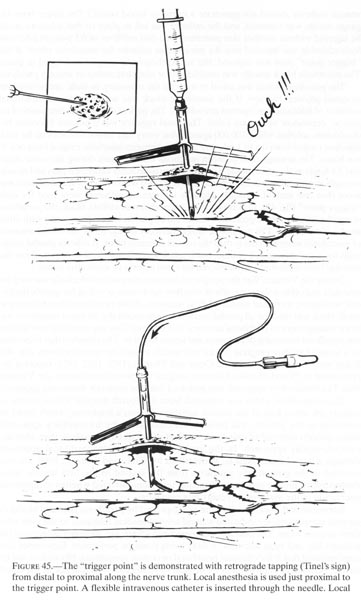
The technique for a peripheral chemical sympathectomy in an extremity was developed at Brooke General Hospital during the Vietnam War (Omer and Thomas 1971, 1972, 1974). When the patient with causalgia was examined, the involved extremity was tapped very gently from distal to proximal to demonstrate any 'trigger points' of extreme irritation. If a 'trigger point' was found, the area was surgically prepared and marked with a sterile pen. After local cutaneous anesthesia, a l6-gauge needle was inserted into the area of irritation. The needle was aspirated to avoid blood vessel penetration, and a flexible 18-gauge polyethylene intravenous catheter was inserted through the l6-gauge needle. (If performed in this manner, the intra-
161
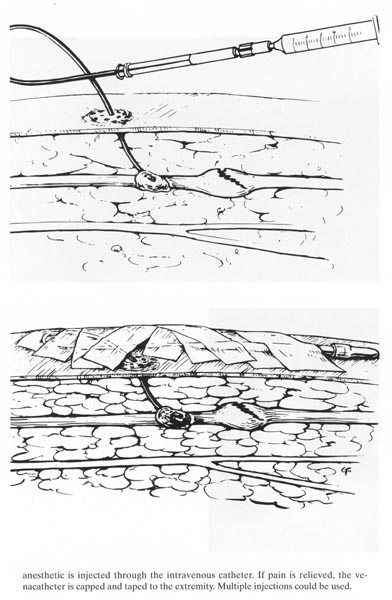
venous catheter should not penetrate a nerveor blood vessel.) The larger bore 16-gauge needlewas removed, and the catheter was left in place so that infusions couldbe injected withoutanother skin puncture. One-half milliliter of 0.5 percent lidocainehydrochloride was injectedinto the intravenous catheter for anesthetic effect. If the 'triggerpoint' pain was relieved, thevenacatheter was capped and taped in place. The anesthetic blockusually was insufficient forcomplete motor or sensory paralysis.
The pain-free patient was asked to exercise the extremity, to walk, and to perform assigned physical therapy. If the anesthetic block was not effective, an additional milliliter of lidocaine was injected periodically. The patient decided the frequency of injection, dependent upon pain relief. The usual regimen was 2 percent lidocaine hydrochloride solution with 1/100,000 epinephrine every four hours. The volume for each injection ranged from 0.5 to 1 ml., and the time between injections ranged from one to ten hours. The average time between injections was 2.2 hours during the acute stage, and 3.4 hours as the effect of the peripheral sympathectomy decreased pain and muscle strength improved. Infusions were continued for two weeks in a few cases. If there was more than one area of irritation, separate intravenous catheters were used for each 'trigger point' (fig. 45). In contrast to a central chemical stellate block, the peripheral sympathectomy is a ward procedure that could be performed simultaneously with other modes of treatment. The peripheral sympathectomy should block the local formation of neurokinin more effectively than the central chemical block. It relieves painful symptoms for a variable period of time, but is much less effective in those cases where the pain has been untreated and unrelieved for three months or more after injury.
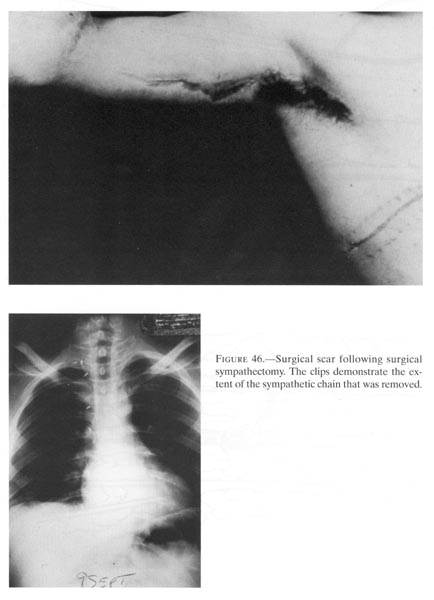
During the Vietnam War, the peripheral chemical sympathetic blockade was used for causalgia and other reflex sympathetic overflow syndromes as well as for specific peripheral nociceptive increased stimuli, such as neuroma. While peripheral chemical sympathetic block was used for all painful conditions in an extremity, its major usefulness was in the management of peripheral neuroma in continuity. This was especially true if there was significant remaining distal motor and sensor function. The causalgia that responded to a series of stellate ganglion blocks was usually treated by sympathectomy (fig.46). Baker and Winegarner (1969) and Omer and Thomas (1971, 1972, 1974) reported improvement in 59 and 65 cases following surgical sympathectomy during the Vietnam War. The transaxillary approach was preferred over the posterior transcostal approach.
The sympathetic chain was removed from the fourth thoracic level superior to include the lower half of the stellate ganglion. Horner's syndrome, which could be annoying to the patient, was present less often after the transaxillary approach, which permits removal of only the lower half of the stellate ganglion, than after the supraclavicular approach. In the lower extremity, a retroperitoneal approach through a lateral flank incision, as described by White and Sweet in 1969, allowed removal of the sympathetic ganglions from the second to the fifth lumbar level. Postoperative precise sudomotor function tests demonstrated whether sympathetic enervation of the involved extremity was complete.
Interviews with patients who were not improved by peripheral chemical blocks or surgical sympathectomy indicated a trend toward gradual tolerance to the pain after three years or more. The pain still was considered severe, but no longer dominated the patient's life, and most activities of daily living could be performed. Experience also demonstrated that if the chemical peripheral or central sympathetic blockade is not effective, permanent improvement by surgical sympathectomy should not be expected.
162
{kind=link}
163
{kind=link}
anesthetic is injected through theintravenous catheter. If pain is relieved, the venacatheter iscapped and taped to the extremity. Multiple injections could be used.
{kind=link}
165
Phantom Pain
A significant problem in the military population is phantom pain. Following an amputation, an adult feels as if the nonexistent limb were still present. It may feel exactly like the original limb as to shape, size, position, and ability to move. These sensory phenomena are termed phantom and may persist for varied periods of time. The phantom has been reported to continue from six months to twenty years (Frazier and Kalb 1970). Phantom pain is an entirely different dimension than is phantom sensation. The patient with phantom pain resulting from physical causes can usually be distinguished from one with psychogenic pain (Frazier and Kalb 1970). When the cause is physical, the patient has a period of no pain following amputation, and the onset of pain follows nerve distribution. The patient with psychogenic problems has pain immediately following amputation, the pain does not follow nerve distribution, and it is evoked especially by reference to disturbing events. A review of more than 7,000 amputees from World War II and Korea treated at the Navy amputation center in Oakland found that phantom pain exists in approximately 2 percent of amputees (Canty and Bleck 1958). Omer (1976, 1981) had an experience similar to that of Ewalt, who reported that only 8 of 2,284 military amputees suffered phantom pain (Ewalt et al. 1947). Amputee patients have a common psychological disturbance and, with the advantage of group therapy, should have similar goals. Fitzsimons Army Medical Center developed a comprehensive program to encourage the new amputee to abandon bedridden activities and enter the world of other amputees (Brown 1970b). Therapeutic procedures included organized athletics and social activities. Functional activity was supported by peers with similar problems, and their assurance was of greater value to the patient than the prescriptions of therapists and surgeons. The utilization of group therapy was recognized as the major factor in rehabilitation. Peripheral nerve irritation, abnormal sympathetic function, and psychological factors all contribute to phantom pain (Omer 1981). The treatment program for every amputee afflicted with this difficult syndrome must be approached on an individual basis.
Functional Activity
The second principle in all treatment programs for pain is functional activity for the involved extremity. Physical modalities may be divided into passive and active assistors. The passive activities will improve circulation, decrease edema, prevent contracture, and prepare the patient for voluntary participation in the active exercise program. Passive modalities include elevation, traction, plaster casts, static splints (orthoplast), vibrators, faradic muscle stimulation, microwaves, ultrasound, ice packs, hot paraffin packs, combined contrast baths, massage, and inflatable splints with positive-negative pressure. Delicate desensitization techniques used to help the apprehensive patient include stroking the skin lightly with a feather, followed by gentle massage, and progressing to hot paraffin baths. Other desensitization techniques include contact with foam rubber chips, jelly beans, navy beans, and rice to provide progressively greater contact pressure (Omer 1984). Some passive modalities may be contraindicated in some cases--the whirlpool bath, for example, involves dependent heat and may increase edema and inflammatory reaction.
166
The more important phase in use of the extremity is active exercise, which can be assisted with dynamic splints, supportive exercising slings, and special handles for tools. Special care must be directed to key circulation areas, such as the rotator cuff muscles in a shoulder-arm-hand syndrome. General body condition is important, and the patient should be ambulatory, if at all possible, to meet his environment. Function can be developed with diversional games, assigned work, and activities of daily living.
Physicians, physical therapists, occupational therapists, and other attendants must be compassionate and yet stimulate maximal effort in the patient. The best functional activity is a patient who has returned to active military duty. Ultimately, the patient 'cures' his own case.
When pain has subsided, elective surgery such as tenolysis and joint releases may be undertaken in order to regain motion after an extensive physical medicine program has been faithfully performed by the patient. Elective surgery performed without these safeguards is ill-advised.
SURGICAL TECHNIQUES
Five annual conferences on war surgery were held in the Pacific from 1967 through 1971. All proceedings emphasized the value of a complete description of the nerve injury as observed at debridement. An appropriate debridement includes incisions into the area of injury, with evaluations of the damage to adjacent tissue, of the state of the musculature, and of the exact site of the neurovascular lesion. An estimate of the percentage of laceration or disruption should be reported. Delayed primary closure was recommended for the extremity wound. Primary nerve suture was discouraged because neurorrhaphy should be performed in the hospital providing definitive care (CINCPAC-2, 1968) (tables 15 and 16).
TABLE 15. - Vietnam neurorrhaphy related to etiology and level of injury.1
167
TABLE 16. - Vietnamneurorrhaphy secondarysuture--specific nerves. 1,2
NERVE INJURY AND REPAIR
Sharp lacerations that do not involve loss of nerve tissue and are allowed to persist for a number of weeks or months create nerve gaps. In complex extremity injuries with fractures and tissue loss, the nerve gap may result from scarring and loss of nerve substance. Overcoming nerve gaps was a significant problem for surgeons in the zone of interior.
World War II studies (Woodhall and Beebe 1956) indicated an average loss of 6 percent from the optimal motor recovery for every centimeter of nerve gap. A nerve gap of 7.5 centimeters was the maximum amount that could be approximated without requiring rigid immobilization of the extremity in flexion (Omer 1976). During the Vietnam War, the techniques used to close a nerve gap included:
Mobilization of nerve trunk. This longitudinal release forces the nerve to survive on its internal longitudinal circulation.
Shortening the skeleton. Potentially dangerous because all soft tissue structures, such as muscle-tendon unit, are relatively lengthened and weakened.
Bulb suture. An unacceptable technique because it produces acute stretch of the nerve. There should be minimal longitudinal tension, and functional failure has been reported when stretching as little as 5 percent of the length (Lui et al. 1948).
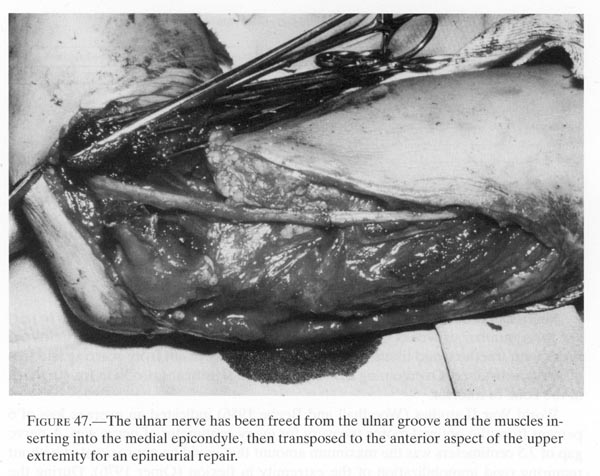
Transposition and rerouting. An example is transferring the ulnar nerve from the extensor to the flexor surface at the elbow (fig.47). At Letterman General Hospital, Mutz recorded that 3 to 5 centimeters of radial nerve could become available to close a gap by anterior transposition of the nerve following dissection of the proximal segment to the level of the posterior cord of the brachial plexus. If a choice is available, the distal portion of a nerve should be rerouted, since the proximal portion contains the regenerating axons.
Flexion of joints. The elbow or knee should not flex beyond 90 degrees, nor the wrist beyond 30 degrees. After the initial healing period of three to six weeks, joints should be extended only 10 degrees per week to prevent intrinsic ischemia (Highet and Sanders 1943).
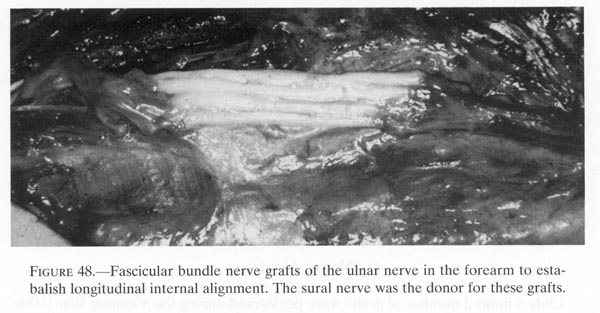
Nerve grafts. Autogenous material is preferred for graft; the sural nerve and the medial or lateral antebrachial cutaneous nerve are the best sources.
168
{kind=link}
During the Vietnam War, the use of magnification, delicate instruments, and finer, less reactive suture material improved the techniques of nerve suture. In addition, battle area evacuation was more expeditious. An effort was made to perform suture as early as possible. Seventy percent of the successful anastomoses were performed within six weeks of injury (Omer 1974). The majority of sutures were performed within the first 3 months after injury. Omer (1974) reported the results of 143 epineural sutures of upper extremity nerves followed for at least twelve months and Brown (1970) recorded the results of 135 epineural sutures followed 6 to 24 months (table 16). Neither study had adequate follow-up, and the results are not fully graded. Brown (1970b) states 'some return.' Omer (1974) has two criteria for 'clinical return': for above-elbow lesion--progressive motor return with independent movement and point localization of 3.84 von Frey filament without over-response (M3-S2); for below-elbow--progressive motor return with independent movement and two-point discrimination, less than 20 millimeters (M3-S3) was needed. In addition, Omer (1974) noted that none of his patients with above-elbow neurorrhaphy had recovery of the intrinsic muscle of the hand during the period of study. The results of the two Vietnam series were similar and indicated that only 40 to 45 percent of sutured nerves result in progressive functional return. Final recovery was not complete and therefore not evaluated. We now know there is significant recovery up to five years (Omer 1990, 1991).
169
Neurolysis
Neurolysis has often been recommended when an intact nerve was found on exploration of a nonfunctioning nerve. During World War II, according to Woodhall and Beebe (1956) neurolysis was external in 70 percent of cases, with saline injection in 25 percent and fascicular dissection in 5 percent. These authors found no evidence that internal and external neurolyses differed in their effect on recovery. During the Vietnam War neurolysis was primarily an external technique. Brown (1970) utilized magnification at Fitzsimons General Hospital to perform intraneural fascicular dissection.
Omer (1974) performed external and internal neurolysis in 59 cases in which the injured nerve was found in continuity, but bound in scar. When 50 of the cases were followed more than three months, neurolysis was found to have been successful in 60 percent of the nerves. The return of function was more successful in above-elbow lesions (18 of 29 nerves compared with 12 of 21 nerves in below-elbow lesions).
There is doubt concerning the success of a neurolysis if function of the extremity returns during the time scale for spontaneous recovery after injury. The intact nerve may have recovered without the surgery. In those patients (table 17) who had neurolysis, 12 recovered function during the time frame for spontaneous recovery. Therefore, Omer (1974) considered the net result of neurolysis as successful in only 18 (36 percent) of 50 nerve lesions. Kline's subsequent studies would indicate an invivo nerve action potential study during the neurolysis procedure (Kline and DeJong 1968; Kline 1980, 450-61).
TABLE 17. - Vietnam cases1 with external neurolysis
Nerve Grafts
Only a limited number of grafts were performed during the Vietnam War (table 18). Most of these were free cable or pedicle grafts done without consideration for precise longitudinal alignment of the fasciculi groups. No information is retrievable concerning the nerve gap that was closed or the longitudinal tension on the nerve graft. All were delayed procedures, more than three months after injury. Only four of thirty-four grafts (12 percent) demonstrated functional activity.
The number of nerve grafts performed was small, the follow-up was variable, and the results were disappointing. Usually the battle-injured peripheral nerve had a scarred bed and a long gap secondary to nerve loss. Often, a long time had passed
170
from injury to graft. Frequently the injurywas proximal so the distance that regenerating axonshad to travel was long. All of these factors would portend a poorresult.
A cable graft is preferable to a full-thickness main nerve trunk graft because the full-thickness graft is in jeopardy of inadequate revascularization with central necrosis. The technique involves a microsurgical anastomosis with several cables of fascicular groups matched to the pattern of fascicular groups in the proximal and distal trunks of the injured nerve. Nerve grafts should be done by an experienced surgeon and as soon as clinically possible after the nerve injury (fig.48).
TABLE l8. - Autogenous grafts of major nerves-Vietnam War 1
{kind=link}
EXTREMITYRECONSTRUCTION
MotorFunction
Several surgical techniques were developed during the Vietnam War for selected early tendon transfers to serve as internal splints and to enhance function while awaiting nerve regeneration in the upper extremity (Brown 1969; Burkhalter
171
1974; Omer 1968). The objectives of earlytendon transfers are to stimulate sensibilityreeducation and to improve the coordination of residual muscle-tendonunits. The muscle-tendonunits used for early internal support should be synergistic with themuscle-tendon unit to bereplaced, such as a wrist flexor in substitute for a finger extensor. Asynergistic tendon will beable to utilize spinal reflex arcs and other automatic feedbackmechanisms to enhancereeducation. Two principles are followed: use as few muscle-tendontransfers as possible, sinceany active muscle-tendon unit used to restore a useful extremityposition will weaken thestrength of the residual active function; and avoid performing amuscle-tendon transfer that willcause deformity when the nerve function recovers.
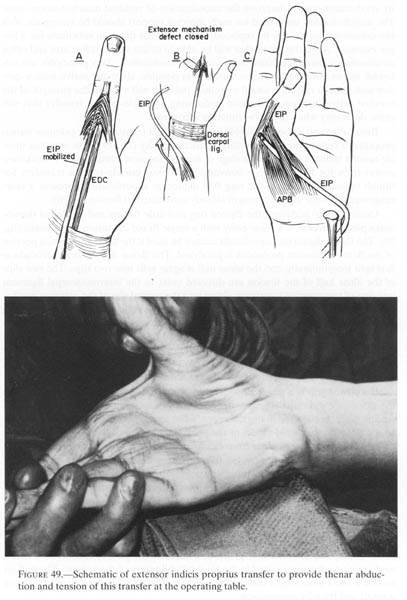
Burkhalter and associates (1968) utilized a direct transfer of the extensor indicis proprius to restore thumb opposition in median palsy (fig.49). This extensor muscle-tendon transfer has the advantage of introducing new strength into a weakened power-train for flexion, while conventional flexor muscle-tendon transfers for thumb opposition, such as the ring flex digitorum superficialis, represent a rearrangement of volar muscle strength already committed to flexion activity.???
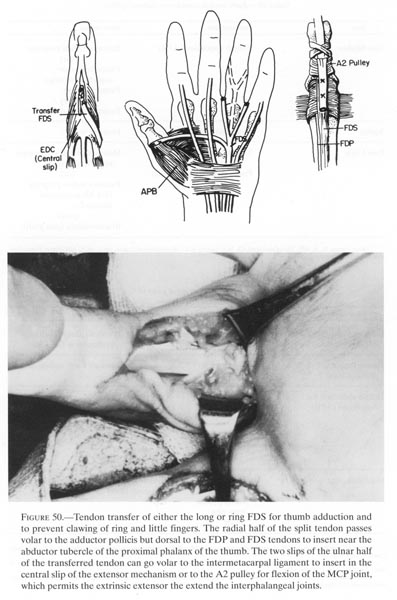
Omer (1974b) stabilized the clawed ring and little fingers and improved thumb-index pinch power in low ulnar palsy with a single flexor digitorum superficialis (fig.50). The flexor digitorum superficialis cannot be used if the ulnar innervated portion of the flexor digitorum profundus is paralyzed. The flexor digitorum superficialis is first split longitudinally, and the ulnar half is again split into two slips. The two slips of the ulnar half of the tendon are directed volar to the intermetacarpal ligament into one of two possible insertions: either into the central slip of the extensor mechanism insertion on the middle phalanx or into the A-2 pulley of the flexor sheaths in the ring and little fingers. The transfer should correct metacarpophalangeal hyperextension and improve interphalangeal coordinated flexion. The radial half of the superficialis tendon is directed across the adductor pollices, distal to the volar palmar ligament and dorsal to the flexor tendons, into the insertion of the abductor pollices brevis for improved pinch strength and to reinforce thumb pronation.???
If a power grip is a major consideration, Burkhalter and Strait (1973) lengthen the extensor carpi radialis longus or the brachioradialis with a multiple tailed free tendon graft through the lumbrical space, volar to the intermetacarpal ligament, to an insertion on the radial aspect of the proximal phalanx of the clawed digits. This transfer introduces new power from extensor muscles into the flexion action.
These innovative muscle-tendon transfers were designed for early active use of the upper extremity as soon as possible after injury and neurorrhaphy (table 19). In a great many other patients, traditional muscle-tendon transfers were performed. Over a four-year period at Brooke General Hospital, 155 patients had multiple tendon transfers for isolated or combined nerve lesions of the upper extremity (tables 20-26) (Omer 1974b). The team approach utilized at all Army General Hospitals and most Army Station Hospitals included surgeons, physical therapists, occupational therapists, orthotic and prosthetic technicians, plaster technicians, social workers, and others interested in the total rehabilitation of the patient. The patient was on a ward near others with similar injuries. The patients gave each other peer support and friendly competition.
172
{kind=link}
173
{kind=link}
174
TABLE 19. - Earlytendon transfers as internalsplints 1
TABLE 20. - Median nerve palsy 1, 2, 3
175
TABLE 21. - Radial nerve palsy 1
TABLE 22. - Ulnarnerve palsy 1
176
TABLE 23. - Combinedlow median-lowulnar palsy 1, 2
Tendon transfers may enhance the rehabilitation of patients with peripheral nerve injuries and paralysis of the lower extremity. The successful tendon transfer should have only one basic objective, such as eliminating a deforming force that will produce further imbalance, replacing a single lost motion, or producing stability. In contrast to the upper extremity, in the lower extremity stability against gravity is much more important than mobility and range of motion. The best reconstructive procedure in many patients with lower extremity nerve loss was an effective orthosis. At Brooke Army Medical Center, electromyograms demonstrated voluntary motor unit action potentials following tendon transfer, but full active dorsiflexion was rarely restored even following months of reeducation.
Motor reconstruction should be done before and at the same time as sensory rehabilitation in the upper extremity, because precise sensibility depends upon total extremity homeostasis and activity (Omer 1974b). However, one should not transfer any muscle that has had a functional nerve deficit.
177
TABLE 24. - Combinedhighmedian-high ulnarpalsy 1, 2
TABLE 25. - Combined high median-radial palsy 1, 2
178
TABLE 26. -Combined high ulnar-radial palsy 1,2
Sensory Function
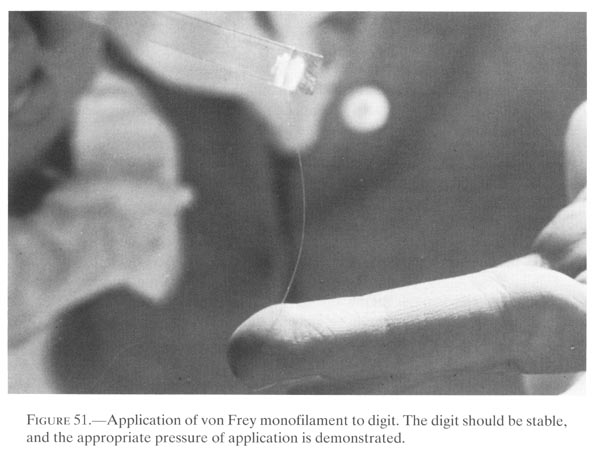
Major contributions in the evaluation of sensibility, sensibility reeducation, and the reconstruction of sensory capabilities were accomplished at Army Medical Centers during the Vietnam War (Omer 1968; Omer 1971; von Prince and Butler 1970). Omer and associates at the Brooke Army Medical Center developed a battery of tests for sensibility that was based on the work of von Frey, Weber, Minor, Seddon, Tinel, Moberg, Wynn Parry, and others. The test battery was designed to evaluate spontaneous recovery of regenerating nerves in the upper extremity, and more than 26,900 individual tests were performed between 1966 and 1970 at the Brooke Army Medical Center (Omer 1980). The minimum test battery included:
- Light touch two-point discrimination distance or light touch recognition of calibrated von Frey monofilaments (fig.51).
- Tinel's percussion test, utilizing a tuning fork (40 Hz) for consistent percussion.
- Dye tests, such as cobalt-chloride, for gross evaluation of sweating as the indicator for sudomotor activity.
- Electromyography.
- Voluntary muscle contraction test on Highet's scale with measured arc of motion.
- Gross hand grip in pounds.
179
{kind=link}
- Tip and key finger pinch in pounds.
- Object recognition tests.
- Timed pick-up test utilizing nine objects.
This test battery was utilized, with modifications, at all Army Medical Centers by the end of the Vietnam War. The occupational therapists and physical therapists, who did most of the tedious work, would transfer to other hospitals and initiate new programs for sensibility evaluation and education (Werner and Omer 1970; Reid 1977). Von Prince and Butler (1970) developed the 'normal' ranges of light touch to deep pressure sensibility as measured by the von Frey hairs; Werner and Omer (1970) outlined a technique for measuring sensibility with the two-point discrimination test and established the timing of the picking-up test with a standard number of objects (Omer 1968).
Raymond M. Curtis, as Consultant in Hand Surgery to the Surgeon General, had an active clinical role at Walter Reed Army Medical Center and the Johns Hopkins University program. Curtis and associates developed programs for reeducation of sensibility in the hands (Dellon, Curtis, and Edgerton 1971 and 1974). The pattern of sensory recovery was mapped at regular intervals, using the following:
- Recognition of constant and moving touch.
- Perception of vibration at 30 and 256 Hz by tuning fork.
- Two-point discrimination distance.
180
Several objects are used for retraining sensibility:
- Fingertip of normal hand.
- Pencil eraser or another soft object, for early-phase reeducation.
- Various sizes of square, hexagonal, and round objects, such as nuts and washers.
- Keys, coins, safety pins, and similar objects used in daily living, for late-phase reeducation.
Early-phase reeducation is begun over the areas in which no two-point discrimination has returned, but vibration is perceived. The retraining objects can be either a pencil eraser or a fingertip of the normal hand. The patient attempts to perceive the constant touch aspect of the object. A retraining session lasts 10 to 15 minutes and is done 3 to 5 times a day. The patient observes the object, thinks how it feels, turns his head, closes his eyes, and verbalizes the sensibility. Once the constant touch is perceived, late-phase reeducation is begun. The patient moves an object back and forth between the thumb and fingers in the normal hand, shifts the object to the injured hand, and attempts to identify the object with his eyes opened and then closed. The improvement in two-point discrimination has remained intact over several years (Reid 1977). Reeducation concepts were taken by Curtis' military Fellows in Hand Surgery to all Army Medical Centers, where the techniques were in use during the Vietnam War.
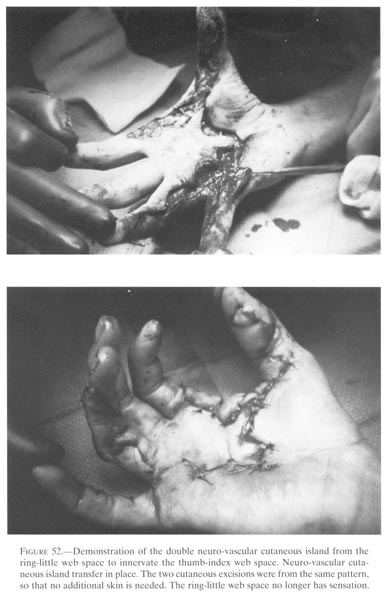
Surgical procedures to restore sensibility following irreparable nerve damage concentrated on replacing precise prehension in upper extremity. The neurovascular island flap was utilized to transfer full-thickness skin and subcutaneous tissue with an intact nerve supply. The operation should be done after indicated tendon transfers have been accomplished and the patient has supply tissues with an established range of motion for the involved extremity. Omer and associates (1970) reported a series of 15 patients with high median palsy treated with neurovascular cutaneous island pedicle flaps. They emphasized that sensibility will diminish unless there is normal motor activity for precise prehension. The Brooke Army Medical Center team described a double cutaneous island from the ring and little finger on a common digital artery-nerve pedicle that provided precise sensibility to the volar aspect of the thumb and thumb-index web (fig.52) (Omer et al. 1970). Patients with high median palsy and high ulnar palsy lost all capacity for precise prehension. In these patients, Omer (1974b) filleted the index ray through the proximal second metacarpal. The insensitive skin distal to the level of the proximal phalanx of the index finger is discarded. The insensitive palmar skin proximal to the index and long fingers is excised. The filleted index finger dorsal palmar flap is then fitted into the palmar defect to provide sensation through the superficial radial nerve.
Prosthetic devices for patients with sciatic palsy were carefully padded to re!ieve the sole of the foot from excessive pressure. Well protected feet did not develop ulceration under supervised ambulation. Special shoes were developed to avoid localized pressure. Amputation is not indicated in any traumatic nerve palsy in the lower extremity unless there is chronic and severe secondary ulceration and infection.
181
{kind=link}
182
LONG-TERMFOLLOW-UP OF COMBAT-INCURRED PERIPHERALNERVE INJURIES AT FITZSIMONS ARMY MEDICALCENTER
ColonelWilliam W Eversmann, Jr., MC, USA(Ret.)
A long-term follow-up study of combat-incurred peripheral nerve injuries was begun at Fitzsimons Army Medical Center in 1967 by Brown and continued by Burkhalter and Eversmann until its termination in 1983. Patients who had incurred traumatic peripheral nerve injuries either in the Republic of Vietnam or within the local community were registered in this comprehensive study to evaluate the long-term results of their treatment at Fitzsimons. Over 85 percent of these patients had sustained combat-incurred injuries to peripheral nerves during their duty in the Republic of Vietnam and had required initial treatment either in the Republic of Vietnam or before arriving at Fitzsimons and often both. At Fitzsimons, all had required additional surgical treatment involving nerve exploration, which was in most cases combined with neurolysis, nerve suture, free nerve graft, or pedicle nerve graft in an attempt to restore some neurological function.
Following surgical treatment, patients were followed at Fitzsimons Army Medical Center as long as was feasible. If and when the patient left the immediate area of Denver, Colorado, follow-up was continued through a questionnaire. A standard set of questions was developed for each level and type of nerve injury in an attempt to evaluate the patient's functional capability and neurological result following surgery. A file of current addresses was maintained with the help of the Disability Services for Retired Military Members and the Veterans Administration so that the questionnaire could be sent to these patients to survey their progress three to four times a year.
Whenever possible, the patients in this study were invited to return to Fitzsimons Army Medical Center for detailed follow-up evaluation. But they represented a highly mobile population of young individuals, and relatively few were able to do so. Because of the method of follow-up on many long-term patients, a detailed quantitative sensory and motor assessment of their condition throughout the entire period of the study was not always possible, and a statistically significant evaluation of these nerve injuries cannot be formed. Nevertheless, through the study of the available records, including hospital summaries, detailed medical evaluations of the affected extremities, questionnaires, and, whenever possible, detailed long-term follow-up examinations, some information on the long-term results of combat-incurred peripheral nerve injuries can be provided. And certain principles of treatment that were followed throughout the study can be evaluated by means of the patient's responses to the questionnaire and the follow-up examination of those patients who were geographically available.
Contained within this study group are a total of 681 patients. Among them, 198 had injuries to the ulnar nerve. An additional 151 suffered damage to the median nerve. The radial nerve was injured in 39. One or more digital nerves were involved in 93 patients, and the brachial plexus in 17. One hundred thirty-two patients had injuries to major peripheral nerves of the lower extremity, either the sciatic nerve,
183
the posterior tibial nerve, or the peronealnerve, and 51 had multiple nerve injuries in either theupper or lower extremity, or a combination thereof.
The following information can be gleaned from this series: Whether external on the peripheral nerve, internal using microscopic dissection of the fascicular structure, or used following saline injection of the epineurium and epineurotomy, neurolysis procedures seem to be generally successful where indicated. Occasionally, a well-documented, dramatic response of return of function, including two-point discrimination, was observed. This return of function occurred after neurolysis when for weeks or months before surgical exploration no gain of neurological function had occurred in the peripheral nerve trunk. In no instance within these 681 patients was a postoperative causalgic syndrome created by the neurolysis, although it might have been present before neurolysis and recurred afterwards.
On multiple occasions throughout this study, attempts to integrate electrodiagnosis into the surgical procedure in order to identify intact fascicular structure were generally unsuccessful except when used to identify motor nerves during surgical dissection. Micro-needle electrodiagnostic techniques were not employed in this series, and macro-techniques did not seem to add significantly to surgical diagnosis, intra-operative technique, or additional successful recovery of the peripheral nerve.
Approximately 15 percent of the patients in this series underwent primary rather than secondary repair of peripheral nerves. Many of the primary repair patients were suffering from locally generated trauma rather than combat wounds, a fact that might have been significant because the injury in these instances was often less severe. But although multiple factors may have contributed to the outcome in cases treated primarily with nerve suture, in general these patients apparently responded better to peripheral nerve suture than did those who underwent secondary neurorrhaphy.
One method of repair of peripheral nerves that had suffered partial laceration, a type of injury commonly found in fragment wounds, consisted of exteriorizing intact fascicular structure and simply suturing the divided fascicular structure in a so-called loop or D-type of nerve suture. The intact fascicles are allowed to lie relaxed in the adjacent tissue while the divided fascicles are sutured end to end by fascicular suture to restore their continuity. The sutured fascicles are generally those that are shorter, and thus the intact fascicles form a loop or the rounded portion of a D. In most patients, a portion of the peripheral nerve's function is maintained or returns after injury, but because of division and scarring of fascicular tissue and the formation of a modified neuroma in continuity, full neurological function does not return. In this series, this type of peripheral nerve repair did not usually result in loss of neurological function from the preoperative state, but it seemed to have no value in restoring additional neurological function from the preoperative state. The experience of these patients suggests that a loop or D-type of nerve suture may have no value in the secondary treatment of peripheral nerve lacerations that involve only a portion of the peripheral nerve.
In a small number of patients, no neurological function returned after an initial secondary repair of the peripheral nerve. Some then underwent a second exploration of the peripheral nerve and a repeat secondary neurorrhaphy of the nerve after excision of neuroma. As a general rule, the results of a second nerve repair were poor, since the nerve suture had to be placed within a bed that was often poorly vascularized with dense, deep scar about the nerve repair. Many patients did not feel that the results justified the additional operative procedure. One would
184
have to conclude, therefore, that if initialnerve suture was unsuccessful in restoring someneurological function, a repeated nerve suture with excision ofadditional neuroma was of verylimited value.
Throughout this study of 198 injuries to the ulnar nerve and 151 to the median nerve, the median nerve provided both a higher incidence and a greater degree of cold intolerance than either the ulnar or radial nerve. When present, cold intolerance did not decrease with time in patients who were followed ten to twelve years after nerve suture, a situation that was particularly true in the median nerve. The incidence of cold intolerance was more frequent with the ulnar nerve than the radial nerve, but the number of cases of radial nerve damage in the series is small compared to that of ulnar nerve damage. The incidence of cold intolerance, therefore, seems to be related to the greater sensory function of the nerve or to a combination of sensory function and vascular integrity of the peripheral nerve segment.
Heroic efforts to bridge major gaps in peripheral nerves by mobilization of the nerve several inches proximally or distally generally resulted in poor recovery, possibly, in part, because of a severely scarred surgical bed in which the nerve lay or, conceivably, because of traction on the peripheral nerve with joint mobilization postoperatively. In none of the cases did mobilization of the joints of the extremity in the postoperative period create a reduced function in the peripheral nerve at the time the joints were mobilized. No critical period of mobilization or length of dissection of either the proximal or distal stump of the peripheral nerve could be identified from these data. A few patients, particularly those with injuries to both nerves of the forearm, underwent pedicle nerve grafting using the St. Clair Strange technique, in which, in a series of operations, the ulnar nerve is used as a pedicle graft to bridge a gap of the median nerve. This approach created surprisingly useful function, function that often seemed better than that produced by free nerve grafting to the median nerve, particularly when the nerve graft lay in a scarred bed. Although the cases of both free nerve grafting and pedicle nerve grafting were few, the general impression of the cases treated by these methods is that pedicle nerve grafting where appropriate and indicated, using the St. Clair Strange technique, is to be preferred over free nerve grafting.
In several well studied cases, repeatedly documented by detailed physician examinations of the hand, a return of interosseous muscle function and, thus, of intrinsic function of the hand was clearly demonstrated more than two years after above-elbow suture of the ulnar nerve. The longest documented period before return was eight years after nerve suture. The patient had been examined in a detailed fashion some six years after nerve suture and found to be without intrinsic function. Two years later, however, he had sufficient return of the intrinsic function of the hand in the interosseous muscles to reduce a claw deformity of the fingers resulting from ulnar paralysis. At least one patient with an injury at the brachial plexus level had a late return of intrinsic function of the hand multiple years after injury, although in this case the ulnar nerve may not have been divided. These well documented late returns of neurological function to the intrinsic muscles of the hand are contrary to all results previously reported in the medical literature.
Because some 349 patients in this series had either median or ulnar nerve neuropathy, a relatively large number of patients had undergone intrinsic transfers for the abductor pollicis brevis because of median nerve injury or to relieve intrinsic
185
palsy resulting from ulnar neuropathy. Manyof these patients returned for long-term follow-up 8to 12 years following their nerve suture and intrinsic transfers.Although a multitude of tendontransfer techniques were used in these patients, a few transfers wereused more commonly thanothers and could be followed some 8 to 12 years after the transfer hadbeen performed.
The so-called opponens transfer to replace the abductor pollicis brevis used either the flexor digitorum superficialis of the ring finger routed with a variety of methods to perform opposition of the thumb and replace the abductor pollicis brevis or the extensor indicis proprius routed around the ulnar border of the wrist, after the method of Burkhalter (Brown 1969; Burkhalter 1974; Omer 1968). The transfer continued to function satisfactorily in patients seen in long-term follow-up and to provide excellent positioning of the thumb for grip and grasp. The extensor indicis proprius transfer apparently had no significant tendency to lose function by stretching out, nor did the flexor digitorum superficialis of the ring finger transfer exhibit any apparent significant incidence of loss of extension of the MP joint of the thumb with long-term evaluation. As performed by many individual surgeons, both transfers continued to maintain an acceptable and even excellent degree of positioning function for the thumb.
Tendon transfer to replace intrinsic function lost by ulnar palsy could similarly be followed for the long term in this study. The most common transfer performed was a power grip transfer using the extensor carpi radialis longus prolonged with a tendon graft, passed volar to the transverse metacarpal ligament, and inserted with a bony insertion at the proximal phalanx (Burkhalter and Strait 1973). Most patients found that the goal of the transfer had been reached and that their strength of grip had been maintained. Eight to twelve years after nerve suture and tendon transfer, they continued to be pleased with the transfer for power grip. A few patients found that they had increased wrist extension while, at the same time, their wrist flexion was limited. The limitation of wrist flexion was not troubling, nor did these patients associate any functional deficit with the loss. No examined patient who had undergone this tendon transfer had noted any deterioration of hand function in the several years after the transfer had been performed.
Because of the wide variation in tendon-transferring techniques for other tendon transfers used in these patients, it was not possible to ascribe any other generalizations to the long-term function of tendon transfers.
SUMMATION
George E. Omer, Jr., M.D.
Injuries of peripheral nerves were severe complications of the extremity wounds incurred in Vietnam. Peripheral nerve injuries provided a major stimulus to improve management of the total extremity. Army surgeons developed clinical and electrodiagnostic techniques to evaluate the extent of nerve involvement and the potential for spontaneous recovery. Associated painful syndromes were aborted with new anesthetic techniques or managed with aggressive surgery and followed with intensive functional use.
186
The disrupted peripheral nerve usually had a delayed repair utilizing surgical techniques antedating current magnification, instruments, and suture materials. Approximately 45 percent of sutured nerves resulted in measurable progressive functional return. A few patients demonstrated excellent peripheral nerve regeneration, which could be related to the extent of injury, time of nerve repair, age of the patient, and surgical expertise in major medical centers. Second nerve repairs and free nerve grafts had disappointing clinical results.
More than half of the disrupted nerves did not regain clinical function and many surgical procedures were developed that utilized tendon transfers to enhance rehabilitation. The more successful tendon transfers involved the forearm and hand. Army surgeons made major contributions in the evaluation of sensibility, sensibility reeducation, and the reconstruction of sensory capabilities. Through the experience and judgment based on large numbers, principles were developed for the reconstruction of extremities.
REFERENCES
Baker, A. G., and Winegarner, F. G. 1969. Causalgia, a review of twenty-eight treated cases.American Journal of Surgery 117:690-94.
Brown, P. W 1969. Ulnar Intrinsic Palsy of the hand. Proceedings Am. Soc. Surg. Hand. J. BoneJoint Surg. 51A:800.
______. 1970a. Rehabilitation of bilateral lower extremity amputees. J. Bone Joint Surg .52A:687-700.
______. 1970b. The time factor in surgery of upper extremity peripheral nerve injury. Clin.Orthop. 68:14-21.
Burkhalter, W. E. 1974. Early tendon transferin upper extremity peripheral nerve injury. Clin.Orthop. 104:68-79.
Burkhalter, W E., and Strait J. L. 1973.Metacarpophalangeal Flexor replacement for intrinsic-muscleparalysis. J. Bone Joint Surg. 55A:1667-76.
Burkhalter, W E.; Butler, B.; Metz, W.; andOmer, G. E., Jr. 1968. Experiences with delayedprimary closure of war wounds of the hand in Vietnam. J. Bone JointSurg. 50A:945-54.
Burkhalter, W. E.; Christensen, R. C.; andBrown, P. W. 1973. Extensor indicis propriusopponensplasty. J. Bone Joint Surg. 56A:725-32.
Bzik, K. D., and Bellamy, R. F. 1984.Editorial: a note on combat incurred statistics. MilitaryMedicine 149:229-30.
Canty, T. J., and Bleck, E. E. 1958.Amputation stump pain. U.S. Armed Forces Medical Journal9:635-47.
CINCPAC-2. 1968. Commander in Chief, Pacific.Second CINCPAC Conference on WarSurgery. Tri-service conference on war surgery conducted at John HayAir Base,Philippines, 25-28 March 1968.
Dellon, A. L.; Curtis, R. M.; and Edgerton, M. T. 1971. Reeducation of sensation in the hand following nerve injury. Proceedings, Am. Soc. Surg. Hand. J. Bone JointSurg. 53A:813.
______. 1974. Reeducation of sensation in the hand after nerve injury and repair. Plast.Reconstruct. Surg. 53:297-305.
Ewalt, J. R.; Randeli, G. C.; and Morris, H.1947. The phantom limb. PsychosomaticMedicine9:118-23.
Frazier, S. H., and Kalb, L. C. 1970.Psychiatric aspects of pain and the phantom limb. Orthop.Clin. North Am. 1:481-95.
187
Highet, W. B., and Sanders, F. K. 1943. Theeffects of stretching nerves after suture. Brit.J. Surg. 30:355-69.
Kline, D. G. 1980. Evaluation of the neuroma in continuity. In Management of peripheral nerveproblems, eds. G. E. Omen, Jr., and M. Spinner. pp. 450-61. Philadelphia: W. B. Saunders, Co.
Kline, D. G., and DeJong, B. R. 1968. Evokedpotentials to evaluate peripheral nerve injuries.Surg. Gynecol. Obstet.127:1239-48.
Lankford, L. L. 1980. Reflex sympatheticdystrophy. In Management ofperipheral nerveproblems, eds. G. E. Omer, Jr.,and M. Spinner. pp. 216-44.Philadelphia:W.B. Saunders, Co.
Lui, C. T.; Benda, C. E.; and Lewey, F. H. 1948. The tensile strength of human nerves-experimental, physiologic, and histologic study. Arch. Neurol. Psychiatr. 59:322-36.
Omer, G. E., Jr. 1968. Evaluation and reconstruction of the forearm and hand after acute traumatic peripheral nerve injuries. J.Bone Joint Surg. 50A:1454-78
______. 1971. Assessment ofperipheral nerveinjuries. In Symposium on the hand,eds. L. M.Cramer and R. A. Chase., Educ. Found. Am. Soc. Plast. Reconstr. Sung.vol. 3. pp. 1-13.St. Louis: C. V. Mosby Co.
______. 1974a. Injuries tonerves of the upperextremity. J. Bone Joint Surg.56A:1615-24.
______. 1974b. Tendon transfersin combinednervelesions. Orthop. Clin. North Am.5:377-87.
______. 1975. 'Survey ofperipheral nerveinjuriesand management techniques.' Committee of theHistory of Orthopaedic Surgery in Vietnam, May 14, 1975.
______. 1976. Nerve injuries:primary vs.secondarysuture vs. nerve grafts. DallasMedical Journal62:401-03.
______. 1980. Sensory evaluationby the pick-uptest.In Nerve repair and regeneration,ed. D. J. Jewettand H. Relton McCarroll, Jr. ch. 27, pp. 250-51. St.Louis: C.V.Mosby Co.
______. 1981. Methods ofassessment of injuryandrecovery of peripheral nerves. Surg.Clin. NorthAm. 61 :303-19.
______. 1982. Results of untreated peripheralnerveinjuries. Clin. Orthop.163:15-19.
______. 1984. Managementtechniques for chronicpainof the upper extremity. Bull. Hosp.J. Dis.44:381-405.
Omer, G. E., Jr., and Seymour, D. W. 1969. 'Ayear of trauma at the Brooke Army MedicalCenter-1968.' Presented at the Society of Military Orthopedic Surgeons,1969, and U.S.Medicine, November 1, 1969, p. 9.
Omer, G. E., Jr.; Day, D. J.; Ratliff, H.;and Lambert, P. 1970. Neurovascular cutaneous islandpedicles for deficient median-nerve sensibility. J. Bone Joint Surg.52A:1181-92.
Omer, G. E., Jr., and Thomas, S. R. 1971.Treatment of causalgia: review of cases at BrookeGeneral Hospital. Texas Medicine.67:93-96.
______. 1972. Peripheralperiodic infusionsympathectomy for the treatment of causalgia. Proceedings of theAmerican Society forSurgery of the Hand. J. Bone JointSurg.54A:898-99.
Omer, G. E., Jr., and Thomas, S. T. 1974. Themanagement of chronic pain syndromes in theupper extremity. Clin. Orthop.104:37-45.
Rakolta, G. G., and Omer, G. E., Jr. 1969.Combat-sustained femoral nerve injuries. Surg.Gynecol. Obstet. 128:813-17.
Reid, R. L. 1977. Preliminary results ofsensibility reeduction following repair of the mediannerve. Am. Soc. Surg. Hand Newsletter15.
188
Rich, N. M., and Spencer, F. C. 1978.Vascular trauma. pp. 125-55.Philadelphia: W.B. Saunders, Co.
Rothberg, J. M.; Tahmoush, A. J.; andOldakowski, R. 1983. The epidemiology of causalgiaamong soldiers wounded in Vietnam. MilitaryMedicine. 48:347-50.
Sunderland, 5. 1972. Nerve and nerveinjuries. pp. 785, 837, 923, 1075. Edinburgh:Churchill Livingston.
Von Prince, K., and Butler, B., Jr. 1967.Measuring sensory function of the hand in peripheralnerve injuries. Am. J. Occup.Ther. 21:385-95.
Werner, J. L., and Omen, G. E., Jr. 1970.Procedures evaluating cutaneous pressure sensationof the hand. Am. J. Occup. Ther. 24:347-56.
White, J. C., and Sweet, W H. 1969. Pain andthe neurosurgeon: a forty year experience.Springfield, Ill.: Charles C. Thomas.
Woodhall, B., and Beebe, G. W, eds. 1956.Peripheral nerve regeneration.VA MedicalMonograph. pp. 5, 191, 311-40, 498. Washington: GPO.
Associated References
Omer, G. E., Jr. 1990. War injuries of thehand. In Tubiana, R., ed., The Hand.vol. 3, ch. 82, pp.903-24. Philadelphia: W. B. Saunders.
______. 1991. Nerve injuriesassociated withgunshot wounds of the extremities. In Gelberman, R.H., ed., Operative nerve repair andreconstruction. vol. 1, ch. 45, pp.655-70.Philadelphia: Lippincott.