



ANNUAL REPORT
OF
MEDICAL DEPARTMENT ACTIVITIES
1944
DIVISION SURGEON
1ST U.S. INFANTRY DIVISION
APO 1, U.S. ARMY
INDEX
PRE-INVASION PERIOD, 1 JANUARY 1944 TO 6 JUNE 1944 1
REORGANIZATION AND REEQUIPMENT 2
SANITATION AND HEALTH 4
INVASION AND NORMANDY CAMPAIGN, 6 JUNE 1944 TO 19 JULY 1944 7
EVACUATION 8
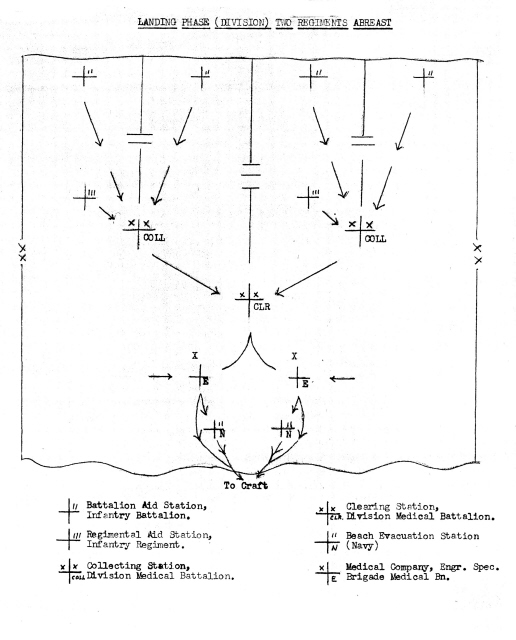
Landing Phase (Diagrammatic) 8a
SUPPLY 10
PERSONNEL 10
SANITATION AND HEALTH 10
EVACUATION 13
Letter of Division Surgeon, SUBJECT: Evacuation of Patients 14a
SUPPLY 15
SANITATION AND HEALTH 16
BATTLE OF GERMANY, 12 SEPTEMBER 1944 TO 31 DECEMBER 1944 18
EVACUATION 21
SUPPLY 24
PERSONNEL 24
SANITATION AND HEALTH 25
Letter of Division Surgeon, SUBJECT: Trench Foot 29a
CONCLUSIONS AND RECOMMENDATIONS 31
ANNEXES:
Annual Report: - Division Psychiatrist.
Annual Report: - Division Dental Surgeon.
In compliance with AR 40-1005 and letter AG 319.1 (9-15-42) EG-M, War Department, 22 September 1942, Subject: `Annual Reports, Medical Department Activities`, the following report is hereby submitted. This report covers the period 1 January 1944 to 31 December 1944. It will cover the pre-invasion period, D-Day landings on the continent, and the subsequent campaigns in France, Belgium and Germany.
On 1 January, 1944 the division was located in the Southern Base Section, England, with the units widely dispersed in the vicinity of Axminster, Swanage and Blandford. The division arrived in this area 8 November 1943 from Sicily and entered upon a period of reorganization and training for future combat, which was proven by later events to be the invasion of the continent.
Combat teams were kept intact but medical service for this situation was not normal. Unit dispensaries were maintained in all areas and evacuation was direct to nearby Station and General Hospitals. Organic medical transportation of the division (3/4 ton ambulances) were used for the evacuation of patients from division units to hospitals.
In general, medical supplies and equipment were adequate and easily obtained from medical supply depots located in the Southern Base Section.
PRE-INVASION PERIOD, 1 JANUARY 1944 TO 5 JUNE 1944
Training in the medical service of the division was easily converted from technical to tactical subjects and primarily interpreted in terms of preparation for combat. The majority of the medical personnel at this time were considered as `well trained` because they had undergone some combat duty and had taken part in the intensive training program which had been, completed in Sicily following the Sicilian campaign. A great part of the early technical training consisted of chemical warfare subjects (identification of gas and treatment of gas casualties). In connection with this training, all men in the division were put through the `Gas Chamber`. Many of the medical department enlisted personnel were given the opportunity to attend schools for Sanitary Technicians and Medical and Surgical Technicians. Several Medical Officers who had come to the division following the Sicilian campaign were given the opportunity to attend the Medical Field Service School at Shrivenham. Those officers who had had combat experience were given the opportunity to attend certain professional schools such as School in Plaster Cast Technique, School in Maxillo-facial Surgery, and School in Neuro-psychiatry. In connection with this latter school and with the change in T/O dated July 1943 assigning a division psychiatrist, one Medical Officer of the division was trained for this duty at this school. (See report of Division Psychiatrist). As the training progressed more emphasis gradually was given to hardening exercises and exercises designed to prepare men for amphibious operations. Road marches, supervised athletic programs, and cross-country litter-bearing were participated in by all medical units of the command. `Speed marches` designed to enable each soldier to complete four (4) miles in forty-five (45) minutes, five (5) miles in one (1) hour, nine (9) miles in two (2) hours and sixteen (16) miles in four (4) hours were instituted.
2
These hardening exercises were completed with a twenty-five (25) mile road march in eight (8) hours. Not only the enlisted personnel but also the officer personnel of the division participated in this type of training.
The first amphibious exercise to be held, putting into practice the above program, took place on approximately 8 February 1944 and involved the medical service of one combat team. This exercise took place at the United States Assault Training Centre (USATC) at Woolacombe, Somerset, England. Those medical units which remained behind in their bivouac areas concerned themselves with amphibious operations using local terrain as simulated beaches. At the completion of the exercise at the USATC critiques were held to correct any errors or deficiencies which had appeared during the exercise. Further instruction was carried out in teaching the men the newer phases of casualty handling and evacuation as presented by the instructors at the USATC. Newer and more specialized equipment which had been used at the USATC was discussed and demonstrated to the key medical personnel of the division. This demonstration included ships-to-shore evacuation by means of `DUKWs` and the transportation of medical supplies from landing craft to beach by means of waterproofed 80 mm. mortar shell cases.
Intensive training along the above lines continued up until the 25 April 1944 when the so called Fabius exercise began. This also involved a practice amphibious operation on the southern coast of England. The entire division medical service participated and the problem was based on the `Neptune` plan which was name given to the actual invasion of the continent on 6 June 1944. Following the completion of this exercise the units returned to their bivouac areas and again the deficiencies which showed up in the exercise were corrected. The period following this exercise was devoted to putting the finishing touches in preparation for the `Neptune` operation. Starting 15 May 1944, the various units of the division began their departure to their respective marshaling areas on the southern coast of England; they were divided into the assault and the follow-up elements. While in the marshaling areas, small unit training continued with special reference to first-aid in combat. The use of the parachute pack, seasick pills and halazone tablets which were supplied to each soldier in the marshaling area was taught. This completed the final phase of training and planning for the invasion of the continent.
REORGANIZATION AND REEQUIPMENT:
The major changes in the T/O at this time (T/O & T/E dated 9 July 1943) consisted in the establishment of a Special Troops Medical Detachment and the appointment of a Medical Officer as a Division Psychiatrist. Changes among the Medical personnel consisted mainly in a reduction within the Regimental Medical Detachment and Medical Battalion. In view of this fact few new replacements were received and therefore the division medical service was fortunate in having a majority of its personnel well trained and with previous combat experience. Immediately prior to the D-day landing, the division was authorized a fifteen percent (15%) increase in Medical Department personnel over and above the T/O. This was to insure adequate and immediate replacement for the casualties expected to occur on and immediately subsequent
3
to D-day.
Under the new T/ (T/O & T/E dated 9 July 1943) the following changes of equipment took place.
1. Thirty (30) ambulances (3/4 ton, field) were authorized for the division on basis of ten (10) per Collecting Company. This represented a reduction of twelve (12) ambulances from previous T/E and it was anticipated that to make up for the decrease other organic transportation of medical units would have to be used for motor evacuation. From past experience it had been learned that 1/4 ton truck, 4 X 4, (`jeep`) lent itself to evacuation for walking and litter patients. Following a detailed study, litter racks were constructed for these vehicles in the Battalion Medical Sections and in the Collecting Companies. These racks allowed the transportation of three litter patients, two (2) over the hood and one (1) across the rear axle. They were constructed permanently to the jeep in such a way as not to interfere with, it being used for other purposes. The only demonstrable disadvantage was that litter patients were `carried` crosswise therefore extending beyond the natural width of the vehicle. However, in actual practice this disadvantage could easily be overcome by careful drivers and therefore this plan was adopted throughout the division. The D-day landings and subsequent combat have proven that these so-called `Jeep` ambulances are practicable and have a definite advantage in motor evacuation of litter patients.
2. Unit Medical Equipment Packs were received.
3. One (1) Otoscope, one (1) Ophthalmoscope, and one (1) Sphygmomanometer were authorized for each Regimental and Battalion Medical Section, each Separate Battalion Medical Section, each Collecting Company and each Clearing platoon (Total: 24 of each).
4. Two additional medical chests were added to the Clearing Company namely Chest, laboratory, field, and Chest, plasma.
5. Although previous T/E had authorized Gas Casualty Chests and Sets, the division received these items for the first time.
It was felt that certain articles on the new T/E and which had never been used by the Clearing Company in previous campaigns were of no value. Authorization was requested and granted to turn these items in, namely Carrier, field, collapsible (`wheeled litter`) and Kits, medical, private.
Certain supplies over and above authorized T/E and equipment were issued specifically for the D-day operation as follows:
(1) Each Battalion Medical Section
|
Litters |
12 |
|
Blanket Set, small |
2 |
|
Splint Set |
1 |
|
Water-proofed shell cases containing morphine syrettes, sulfanilamide crystals, plasma, dressings, and bandages. |
|
4
(2) Each Collecting Company
|
Splint Set |
2 |
|
Water-proofed shell cases (for contents see above) |
16 |
(3) Clearing Company
|
Splint Set |
6 |
|
Blankets |
600 |
|
Litters |
200 |
In connection with the emphasis placed upon Chemical Warfare, gas mask spectacles (inserts) were provided and fitted for two hundred thirty-seven (237) enlisted men and officers of the division.
Prior to embarkation each soldier was issued at the marshaling area the following items: One (1) parachute pack, halazone tablets, and sea sickness pills. No critical shortages of T/E or equipment and supplies authorized in excess of T/E existed prior to embarkation.
SANITATION AND HEALTH:
The division experienced during the greater part of the period a cold climate with moderate rainfall. For the most part the majority of troops were housed in military barracks, public buildings, Nissen Huts, and winterized tents. On the whole the quarters for the enlisted personnel were `cramped` and the basic minimum floor-space allotted for each man was reduced to thirty-five (35) sq. ft. per man by direction from the Office of the Chief Surgeon, ETOUSA. The climate plus the relative overcrowding in the soldiers` quarters had a direct effect on the health of the command in the incidence of respiratory diseases. Insects during the period were non-existent and therefore no problem.
Water Supply:
Water supply was adequate for all purposes (washing, bathing and drinking) and was obtained from local municipal sources. All drinking sources were required to have a bacteriological examination and those sources found to be non-potable were chlorinated by the division engineer water units. Certain non-potable sources were corrected by British engineers by the installation of new piping.
Waste Disposal:
Latrine facilities throughout the command were of two types, bucket type and flush toilets. No difficulties were experienced with the latter type other than the usual repairs and cleaning out of septic tanks. The bucket type latrine however, was consistently unsatisfactory. The emptying of the latrine buckets was the responsibility of local civilian contractors who were supposed to make at least one (1) daily collection and in some instances where the number of buckets were inadequate, as many collections as were necessary to prevent the buckets from overflowing. Very few of these civilian contractors handled the collection properly. In many instances, the buckets were not collected as often as required and consequently there was spillage and pollution around the latrines. Other contractors collected the buckets often enough but failed to clean the buckets and disinfect them chemically as was required by contract. In other instances the
5
human waste had to be disposed of by the respective units and this was done by burial. The major criticisms were therefore:
1. Too few buckets allotted to the troops (5%).
2. The failure of the `Collection system`.
3. The pollution of the latrine area during the emptying of the buckets.
All kitchen wastes were sorted out according to existing directives, kept in covered metal containers, and then hauled away by local civilian contractors in much the same way as human wastes. The same deficiencies existed in this system as existed in the collection of bucket latrines. Cans were allowed to overflow because of failure to collect them regularly; pollution and spillage around the kitchen area resulted from improper handling of the cans; and in many instances cans were returned by contractors unclean and leaking.
Messes:
Because of the shortage of kitchen facilities battalion kitchens were the rule. These kitchens were British in character and generally failed to measure up to American military standards. First of all storage space for perishables and non-perishables was inadequate and poorly ventilated. In an effort to conserve the field ranges (stoves), the British coal stoves were used. The use of coal in the kitchens resulted heavy smoke and coal soot. All the kitchens showed evidence of being used prior to arrival of the division. Therefore, the general cleanliness of kitchens was a major problem. In spite of these disadvantages kitchen sanitation was maintained at relatively high level.
Food:
Type `A` ration was issued for practically the entire period prior to embarkation excepting in tactical exercises when emergency rations were used (`B`, `D`, & `K`). In all respects the ration issue was satisfactory in quality and quantity; mess personnel were competent and the majority of cooks had previously attended Cooks and Bakers School. Because of this food was well prepared and wastage was rare. Although no refrigeration facilities existed, meats were received in frozen condition and immediately consumed. At no time during the pre-invasion period was it thought that vitamin supplements were necessary. A quartermaster bakery unit was attached to the division during this time and it supplied the division with fresh bread daily.
There was only one instance where poor mess management and sanitation affected the command. Just shortly prior to embarkation and while one battalion of an infantry regiment was in the marshaling area, about 30% of the command suddenly developed an afebrile diarrhea. This marshaling area was commanded and operated by an SOS unit from Southern Base Section. A careful investigation revealed that all the cases of diarrhea were messing at one kitchen and that this kitchen failed to provide adequate mess-kit washing facilities for the number of personnel that it fed. An immediate correction of this deficiency resulted in a clearing up of the situation and no new cases of diarrhea were reported thereafter. None of the men effected with the diarrhea were lost to the command for the D-day landings.
6
DISEASES:
Infectious Hepatitis (Jaundice): In retrospect, cases of infectious hepatitis had started in the fall of 1943 while the division was in Sicily. The incidence of this disease increased and continued even after the arrival of the division in the United Kingdom. However, there was a gradual decline in the rate beginning with the month of January 1944 at which time there were forty-three (43) cases as compared to one hundred forty-four (144) for the month of December 1943. The month of February 1944 showed only six (6) cases of Infectious Hepatitis and from that time on only sporadic cases occurred throughout the command.
Respiratory Diseases: The start of the year in the United Kingdom was characterized by the large number of respiratory diseases of all types and although there were four hundred fifty-eight (458) cases reported in January 1944 as compared with six hundred twenty-eight (628) cases in December 1943 this still represented a high rate. It is believed that the causes of the high incidence of these diseases were (1). the change of climate from a more or less sub-tropical climate to a north temperate) (2). the overcrowding of troops in billets and (3). the poor heating and ventilation, facilities in the billets.
All possible measures were taken to prevent the spread of these diseases. Head-to-foot sleeping was put into effect in all sleeping quarters. When practical, shelter halves were used to make sleeping cubicles. Proper ventilation, especially during sleeping hours was effected and supervised by the Charge of Quarters in unit billets. Cases of respiratory diseases that were kept on a `Quarters` status were isolated and cared for at unit dispensaries. All food handlers received a daily health inspection before reporting for duty and if any were found suffering from a `cold`, they were immediately sent to sick call for treatment and disposition.
Under this strict control, respiratory diseases gradually declined and at the end of May 1944 prior to the invasion of the continent, the number of respiratory diseases had declined to less than fifty (50) cases monthly.
Malaria: In the early part of the pre-invasion period, Malaria which had been a problem in Sicily and in the first several weeks in the United Kingdom appeared to have died out. However, an increase in Malaria throughout the division occurred in the latter part of March and from that point on continued to increase. Likewise there was a notable increase in Fever of Undetermined Origin (FUO), many of which were later diagnosed in hospitals as Malaria. These cases were obviously Malaria, chronic, recurrent because of the absence of the malaria-bearing mosquito in the United Kingdom. Furthermore, many of these cases were of the so called `Latent Type` occurring in those individuals who had taken atabrine and quinine prophylaxis and who had had no attacks of Malaria or FUO prior to this time. Because of the increase of Malaria suppressive atabrine therapy was instituted for all personnel having a past history of Malaria (Ltr. Hq, First US Army dated 21 May 1944). This disease resulted in the loss of a substantial number of military personnel just prior to the embarkation and landing on the continent.
7
Communicable Diseases: For the most part communicable diseases consisted of sporadic cases of Meningitis (Cerebro-spinal), Mumps, and Measles. None of these diseases became epidemic and were easily handled by so called `working` quarantine. All immunizations against Typhus Fever, Typhoid Fever, Tetanus and Small Pox were completed prior to D-day.
Venereal Diseases: Excepting for the month of May 1944 when there were thirty-two (32) cases of venereal disease (rate/1000/annum - 25.2 ) these diseases were no problem. In general the monthly rate/1000/annum averaged about ten (10). However, because of the fact that venereal diseases were quite prevalent in the United Kingdom, measures were being taken all the time to keep these diseases under control and at a minimum. Personnel going on pass or furlough were informed of the location of "pro-stations" available to them; individual `pro-packets` were issued to all personnel desiring such; sex hygiene lectures were given periodically: sex hygiene films were shown as part of the training program. It is believed that the marked increase in venereal diseases that occurred in the month of April tended to bear out past experience in the division when combat is imminent, troops become lax in their venereal discipline and tend to assume a fatalistic attitude toward the future. Moreover, as the invasion of the continent became more imminent, troops were restricted to the so-called `banned areas` and an influx of professional prostitutes into these areas was noticed. The month of May 1944 showed only five (5) cases of venereal disease but this low rate is explained by the fact that the division was in a marshaling area and restricted from contact with civilian or other military personnel.
INVASION AND NORMANDY CAMPAIGN, 6 JUNE 1944 TO 19 JULY 1944
On 6 June1944, the 1st US Infantry Division and attached landed on the continent (Normandy). A heavy naval and air bombardment preceded the assault on the beach which was carried out by one combat team of the division and by one combat team of the 29th Division attached. The naval bombardment had failed to knock out several enemy concrete emplacements which were situated and built in such a manner as to resist all heavy gun fire except a direct hit. In addition unfavorable weather had reduced the effectiveness of certain `secret` support weapons. The fire directed against the assaulting troops was so intense as to prevent a penetration of these emplacements until anti-tank weapons could be landed. H-hour had been 0630 and it was not until 1000 hrs that the enemy positions on the cliff overlooking the beach were destroyed or captured. Although the enemy continued to resist fiercely, the assault troops and supporting troops were finally able to secure the small key village of Colleville-Sur-Mer. By the 9th June 1944 the hard shell of enemy resistance had been broken. Although the enemy began to dig in, set up road blocks, erect wire entanglements, and sow numerous mine fields, he was unable to prevent the division`s advance to Caumont. Throughout the entire period enemy air activity was negligible except for single enemy bomber attacks occurring after dark. The division remained in a defensive position at Caumont until the 15th July 1944 when it was relieved by the 5th U. S. Infantry Division.
8
EVACUATION:
The medical plan for D-day had anticipated the following evacuation plan:
1. The Company Aid men to go ashore with their respective companies to tag the wounded, render first aid, and if possible mark the location of the casualties
2. The Battalion Aid Station Sections to follow with certain equipment and twelve (12) litter bearers, and support the assaulting battalions. They would render further medical treatment and attempt to group casualties to collecting points for later evacuation to the beach.
3. The Naval Medical Sections (Shore Party) to land approximately at the same time as the Battalion Aid Stations, establish a Beach Evacuation Station, receive casualties from the beach, administer first-aid, and effect seaward evacuation.
4. The Collecting Companies to land next at a time when the attack had moved off the beach; the litter bearer platoons to land first to aid the evacuation of the Battalion Aid Stations. The Collecting Station Platoon to follow, proceed to a station site and receive all casualties from the front. The Ambulance Section to land next.
5. Soon after the landing of the Collecting Company, Medical of the Engineer Special Brigade to cone ashore with its equipment and personnel intact, and perform the following services: (a). Receive casualties from Collecting Stations. (b). Provide treatment for non-transportables thru its attached surgical teams, and the treatment and seaward evacuation of transportable casualties. To cooperate with the Shore Party in loading all craft used for ship-to-shore evacuation. (c). To operate a medical supply dump. The Naval Beach Evacuation Station and the Medical Company of the Engineer Special Brigade to remain in the beach area regardless of the movements of the Army Medical units. The Medical Company of the Engineer Special Brigade at this phase of the operation to substitute for the Division Clearing Station.
6. The Division Clearing Station to land as soon after the Medical Company depending upon the forward progress of the infantry. Once this had landed and set up, medical service of the division became normal.
7. The rear evacuation was to be kept under control of higher headquarters which was to make the following medical facilities available:
Field Hospitals
Evacuation Hospitals
Ambulance Companies
Collecting Companies
Clearing Companies
Supply Depots
Auxiliary Surgical Groups
Diagramatically this evacuation plan is represented as follows:
8a
9
In spite of the pre-invasion planning and exercises, the medical service and evacuation on D-day until D plus 3 was quite confused. Many of the beach medical units and also medical units of the division were not put ashore according to plan and others were landed by mistake on wrong beaches. Likewise the tactical situation failed to progress as anticipated and this served to alter the landing tables of the medical units. Many of the medical units of the division and of the amphibious medical battalion were unable to bring their supplies and equipment ashore, which were lost in the sea or damaged by enemy activity. Within the division medical service then first-aid to the wounded was provided by the Company aid men who had come ashore with the assault infantry companies. Litter bearers from the Battalion Sections and Collecting Companies followed close behind and collected the casualties and prepared them for their evacuation.
Casualties were evacuated from shore-to-ship by whatever means available (assault boats, DUKWs, and any other available craft). Priority was given to non-transportables. Of necessity many of the casualties remained on the beach under care of the Division Clearing Company personnel and of medical personnel from other units. Although one platoon of the Division Clearing Company came ashore at 1730 hrs on D-day and the second platoon joined it at 2130 hrs, neither of the platoons failed to function on this day. The entire company personnel assisted in clearing the beach of casualties and thereby functioning as an emergency collecting unit. On D plus l at 0630 hrs, the Division Clearing Station was established and opened on the bluffs just east of Vierville-Sur-Mer. From this time on division medical service was normal, namely from Battalion Aid Stations through Clearing Station. Furthermore, there were no facilities on the beach for handling non-transportable casualties or other seriously wounded patients. To effect this evacuation and treatment, the following plan was put into effect. Two of the auxiliary surgical teams, which were ashore at this time but which were unable to operate because they lacked equipment, were secured and set up at the Division Clearing Station, using the Division Clearing Station surgical instruments, supplies, tentage, etc. They proceeded to care for the wounded and continued to do so until D plus 3 at which time they were able to join their parent unit. To prevent the casualties from piling up at the Clearing Station and to facilitate the evacuation to shore and to ship, Clearing Station personnel were used as litter bearers to carry litter patients to the shore where the amphibious medical battalion had set up small collecting points. Walking wounded were likewise directed to the same shore points and in some cases were drafted as additional litter bearers. The litter haul from the Clearing Station site was approximately one thousand (1000) yards down the bluff and over rather difficult terrain. To supplement the litter bearers, twenty-four (24) German prisoners were obtained from a nearby prison cage. The shore collecting points at this stage took over the responsibilities of getting casualties to the ships; DUKWs were brought to the Clearing Station, loaded up with litter patients and dispatched directly to the ships. The evacuation of the Clearing Station from D-day to D plus 3 remained under division control, after which it passed into the hands of the amphibious medical battalion which had meanwhile been able to locate its equipment and set up.
After D plus 3, the tactical progress of the division was rapid, moving in the direction of Caumont and arriving in that vicinity on June 12, 1944. From D plus 3 on evacuation was normal and the Division Clearing Station was evacuated by First Army Collecting Companies.
10
After a few days in the vicinity of Caumont when it became apparent that the division was to occupy a defensive position, the Clearing Station expanded to its full capacity and instituted the policy of holding minor casualties and diseases which could be returned to duty within five (5) days. Soon after the arrival at Caumont, a Field Hospital Platoon was set up close to the Clearing Station and in support of the division. Their primary function was to handle non-transportable casualties. In this situation evacuation in the division was rapid due to the proximity of the Collecting Stations, (within five (5) miles) and also because of the good road network. It was in this position that the Clearing Station came under enemy artillery fire for the first time. Apparently the enemy fire was directed at artillery located in the vicinity of the Clearing Station. Late in the afternoon of July 9, direct hits were recorded, causing no casualties. Some damage to vehicles resulted. On the 15th July, the entire division was relieved at Caumont by the 5th U. S. Infantry Division and moved to the vicinity of Columbiers. Here, it reorganized and reequipped, completing this on19 July 1944. One platoon of the 47th Field Hospital which was in support of the division moved to this site also but did not operate. Evacuation during this short period was normal.
SUPPLY:
Although the plans for supply did not work as intended, still sufficient supplies were available from D-day to D plus 3 at which time the Division Medical Supply Section set up and took over the normal supply of the division. From D-day to D plus 4, items which were intended for the advance section of the First Army Medical Dump were unloaded on the beach and in the vicinity of the Division Clearing Station. In addition the Navy had unloaded on the beach extra supplies consisting of dressings, plasma, litters, blankets, and splints. The expendable supplies were in water proofed rubber bags. These were immediately available to the functioning medical units. The supply within the division medical service was at no time critical in spite of the large number of casualties. There were very few losses of non-expendable items and the expendable supplies which had been taken ashore with the division medical units were adequate. The Division medical Supply Section came ashore on D plus 3, and was set up and functioning on D plus 4. From this point on all requisitions for medical supplies were filled from the Division Medical Supply Section which in turn submitted its requisition through channels to Army Medical Supply Depots.
PERSONNEL:
No changes in T/O occurred at this time. For the first time since being overseas and in combat the division suffered two (2) fatal casualties among Medical Department Officers due to enemy action. Both of these were Captains, MC, and both were Battalion Surgeons. The first one was seriously wounded on D-day and subsequently died in a hospital in the United Kingdom; the second was killed by a mortar shell in the Caumont area.
SANITATION AND HEALTH:
The period covered by this part of the report was characterized by moderate to heavy rainfall. So far as the tactical situation permitted, troops were housed in public buildings and civilian establishments. Toward the latter part of the period, flies began to appear in large numbers. Fly control measures were instituted at this time which consisted primarily of spraying latrines and kitchen areas with weak solution of creosol. Spraying was accomplished by
11
using a three (3) gallon as decontaminating pump. The kitchen trucks which had been screened in and fly-proofed prior to the invasion were now used. Unit surgeons made frequent sanitary inspections to assure themselves that fly control measures were adequate and as a result of this no increase in fly-borne diseases resulted.
Also in the latter part of this period, there was a noticeable increase of mosquitoes in the division area. Because of the high incidence of Malaria the proper identification of these mosquitoes was important. Several specimens were thereupon captured and taken to the 10th General Medical Laboratory, where they were identified as a variety of Culex.
Water Supply:
All water used for drinking and cooking was chlorinated according to Army regulations by division engineer water units. Primary sources of water supply were the streams within the division area.
Waste Disposal:
Latrine facilities were primarily straddle trenches and `cat holes`. When buildings were used, some flush toilets were available. All kitchen wastes were disposed of by either burial or incineration. Trash, rubbish, and cans were likewise disposed of by incineration. In some of the local town areas trash dumps were established.
Messes:
Kitchen trucks were used in the preparation and cooking of food. For the most part these kitchens were kept together either in the Battalion or Regimental Field Train along with the other service elements of the combat unit.
Food:
During the early part of this period the ration was of the Field Type (`C`, `D`, `K`, `5-in-1`, and `10-in-1`). The menus from those rations were not sufficiently varied but were satisfactory as to quality and quantity. Small gasoline stoves (single-burner type) were part of the equipment of each squad of a rifle company. These stoves enabled the men to prepare hot meals for themselves when the tactical situation prevented hot meals from the company kitchens being served to them. As the campaigns got under way the `B` ration came into use and the emergency rations were consumed only when the tactical situation required. Fresh meats were received in frozen condition and consumed immediately. Some of the units supplemented their messes by local purchases of eggs and certain types of vegetables and fruits; local purchases of milk, butter, cheese, and other dairy products were prohibited.
Diseases:
Malaria: Malaria, and FUO`s continued to show an increase from the day of the landings and were the major disease problems of the command. During
12
the month of June, two hundred sixty (260) cases of Malaria and one hundred sixty-three (163) cases of FUO`s were reported; during the month of July three hundred sixteen (316) cases of Malaria and one hundred twenty-eight (128) cases of FUO`s occurred. At no time was there evidence to show that these cases of malaria were other than chronic, which had been initially incurred in the Mediterranean Theatre. All efforts were made to control incidence of the disease by use of atabrine prophylaxis which was being given to all personnel who had been in the Mediterranean Theatre.
Venereal Disease: During this campaign, venereal diseases were no problem. No cases were reported for the month of June and only one (1) new case was reported for the month of July. All towns in the division area were placed `Off Limits` to all division personnel. This was enforced by military police. Consequently, social contact between military personnel and civilian population was kept at a minimum.
Communicable Diseases: Communicable diseases were of no consequence during the defensive period in the vicinity of Caumont. Immunizations were brought up to date according to existing directives from higher headquarters.
MARIGNY BREAKTHROUGH, EXPLOITATION, AND THE CAMPAIGN OF NORTHERN FRANCE AND BELGIUM, 20 JULY 1944 TO 11 SEPTEMBER 1944:
The plan for the Marigny breakthrough called for sudden penetration in the enemy lines; by several US divisions, including the 1st US Infantry Division. This breakthrough was to. Be preceded by a heavy aerial bombardment during which six thousand (6000) tons of bombs were to be dropped on the enemy.
The initial drive was south toward Marigny and then toward Coutances. By 31 July 1944, Coutances had been seized and the division had advanced south of the town to regroup for exploitation of the operation. On 1 August 1944 the division had started driving toward Mortain in order to create a corridor thru which allied armour could pass to attack the Brittany Peninsula. Shortly after midnight on 1 August 1944 the enemy attacked the division with elements of his air force. Numerous anti-personnel bombs were dropped in unit CP`s and the division CP, which at that time was located about three hundred (300) yards from the bivouac area of the Clearing Station and the supporting Field Hospital. Over two hundred (200) casualties occurred from this raid.
The division continued to move rapidly will light enemy resistance until it reached the vicinity of Mortain, where the enemy put up stubborn resistance. This sector was shortly thereafter turned over to a combat team of another division thus allowing the division to extend its zone of operation south of Mortain to the vicinity of Mayenne. The division remained in the vicinity of Mayenne until 13 August 1944 when it began an attack north and west toward Le Ferte-Mace. By 17 August 1944, the division had penetrated the Foret D`Andaine and secured its objective. Its position here served to aid in closing the Falaise-Argentan pocket which had been created by an encircling movement of British and American troops. However during the following six (6) days, there was little enemy contact.
13
On 24 August 1944, the division began its move across France into Belgium. The first move took the division to the vicinity of Chartres; enemy opposition was practically nil. On 27 August 1944, the division crossed the Seine River just south of Paris, still meeting very little opposition, and still continuing to advance rapidly with few casualties. By 30 August 1944 the division had advanced through Chateau Thierry, Soissons, and Laon. These movements constituted the pursuit of a fleeing and disorganized enemy.
By 2 September 1944 the division had arrived in the vicinity of Maubeuge south of Mons in the vicinity of the Franco-Belgian border. Meanwhile at the same time the 3rd Armoured Division which was operating on the right flank of the division had penetrated into Belgium east of Mons thereby cutting off the escape route of approximately five (5) German divisions. This tactical situation there upon produced one of the most costly single defeats suffered by the German army in the entire campaign and at the same time also created some of the most serious problems of evacuation and supply for the division medical service. This battle became known as `The Mons Pocket` which was fought from the 2nd to 6th September 1944. When the final reports of the disaster could be correlated and a reasonably accurate total made, it was found that over seventeen thousand (17,000) German prisoners had been taken and at least two thousand (2,000) Germans had been killed. One thousand seventy-nine (1079) enemy wounded had been cleared through the Clearing Station. It was evident that the total of five (5) German divisions had been almost completely destroyed. During the 6th and 7th September 1944, the division moved rapidly east from Mons to seize the city of Namur, Huy, and eventually Liege, all cities on the Meuse River. Opposition was light up to this point but as the combat columns of the division proceeded towards the German border enemy opposition began to stiffen and the Germans began to prepare strong defenses. However, enemy resistance was unable to stem the forward surge of the division and by 11 September 1944 the division had pushed in force to the `Siegfried Line` at a point approximately six (6) kilometers west of the city of Aachen (Aix-La-Chapelle), the first large German city in the path of the division.
EVACUATION:
The plan for the Marigny breakthrough anticipated no problems of medical evacuation within the division and during this phase of the operation evacuation was normal. One platoon of the 47th Field Hospital which was in support of the division followed along with the functioning platoon of the Clearing Station and set up as required to handle non-transportable casualties. Most of the time, because of the light casualties, this Field Hospital Platoon did not operate and was kept in mobile reserve. Evacuation of the Clearing Station was effected by on Army Medical Group to evacuation hospitals which were initially located within fifteen (15) miles of the Clearing Station. By 17 August 1944 the division was located in vicinity of Bagnoles de L`Orne and here the Clearing Station took over a large hotel which had been used as a hospital by the enemy and was suitably marked with the Geneva Red Cross. Operating room facilities were available
14
here but no German equipment or supplies of any consequence had been left behind by the enemy. The Field Hospital Platoon, which at that time was in mobile reserve, became immobilized by casualties from other units in this area. Consequently on 24 August 1944 when the division began its move across France into Belgium, it did so without the support of the Field Hospital Platoon. Relatively few casualties occurred in this drive and the Clearing Station merely established a `skeleton` set up consisting of one (1) large ward tent (combined Admissions, Treatment, and Evacuation). An idea of the rapidity of the operation can be gathered by the daily movements of the Clearing platoons which employed `leap-frog` tactics as follows:
AUGUST 25 - 60 miles
AUGUST 27 - 25 miles
AUGUST 28 - 23 miles
AUGUST 29 - 27 miles
AUGUST 30 - 27 miles
AUGUST 31 - 28 miles
Total: 190 miles
This rapid movement had left the evacuation hospitals far to the rear and in order to maintain some form of close hospital support for divisional clearing stations, field hospitals were now utilized as small mobile evacuation hospitals located between divisional clearing stations and the evacuation hospitals. This then was the medical evacuation as it existed when the division began the battle of the `Mons Pocket`.
One (1) Clearing Platoon had meanwhile moved to a position just south of Maubeuge and had remained mobilized here anticipating a further move across the Belgian border. However, shortly after its arrival here, hundreds of enemy wounded began to clear to this point; frantic calls and messages from first and second echelons of the medical service reported that hundreds of German casualties were still being collected from the battlefield and would shortly arrive at the Clearing Station. To effect this movement of casualties back to the Clearing Station, the units employed whatever type of organic transportation that was available (3/4 ton, 1 1/2 ton and 2 1/2 ton trucks). In addition captured German vehicles and ambulances were also used. A detailed report on the evacuation of the casualties in the `Mons Pocket` and the serious difficulties encountered at this time are shown in a report of the Division Surgeon, addressed to the CG, 1st US Inf Div, APO 1, US Army. A true copy of this report is included here:
14a
HEADQUARTERS 1ST US INFANTRY DIVISION
Office of the Division Surgeon
APO 1, U. S. Army
7 September 1944
SUBJECT: Evacuation of Patients
TO : Commanding General, 1st US Infantry Division, APO 1, U.S. Army
On September 3rd at 1715 hours the First Medical Battalion (less A, B, C, Company and 1st Platoon `D`) arrived at new site south of Maubege GSGS (1/50,000 Sheet 88 3055895) where approximately 50 enemy casualties were found awaiting evacuation. A clearing station was established at once. Truckloads of wounded prisoners proceeded to dome in so that by mid-night over 350 casualties crowded the area. At 2000 hours the 1st Platoon of `D` joined the company at this area and its resources end personnel were added to those of the functioning platoon (2nd).
At approximately 1800 hours we informed Sgt. Wm Kral (578th Ambulance Company whose 10 ambulances were in the process of evacuating us) to inform his Headquarters of the critical situation that was arising. Informal reports from Regiments and our collecting companies indicated casualties well up in the hundreds. About 1910 hours the Division Surgeon called for 20 ambulances from Corps.
About midnight 2-2 T. Trucks, 2w/C, 5 ambulances from the 3rd Platoon, 578th Ambulance Company and 2 ambulances from 450th Ambulance Company, arrived. The trucks made one trip, the ambulances made 2 trips and did not return thereafter.
Early in the morning of September 4th 7 ambulances from 491st Ambulance arrived and remained with us until the evening of the 5th. On the morning of the 4th we were informed via message from G-4 to expect 30 ambulances, 200 litters and 300 blankets via 51st Medical Battalion, within 3 hours. (Message signed by Lt. Col. Eymer at 0955B).
All that day (4th of September) casualties continued to pour in. Our own transportation was utilized to help the collecting companies and to evacuate selected cases to the P.W. cage after treatment. At 1800 hours the 1st Platoon and Headquarters and Headquarters Detachment moved to new position south of Mons at 315082 where almost immediately enemy casualties proceeded to pour in. At 2100 hours the following message was radioed to G-4 `30 Ambulances not yet arrived, Situation critical. 425 enemy and 20 Americans at old site. 132 enemy at new site. All awaiting evacuation`. At this point Division Medical Service was at an absolute standstill. Any serious enemy action would have been disastrous - we were absolutely immobile with 12 miles separating both platoons and gasoline almost unavailable.
14b
Evacuation of Patients (Cont`d)
On the morning of September 5th 5 additional ambulances arrived from 578th Ambulance Company with 100 litters and 300 blankets. At 1100 hours 4 2 T. Trucks from the clearing company undertook to evacuate the station at the old site (S of Maubege). Two trips were made (the first 120 tiles the second 40 miles). At the same time 2 Headquarters 2 T. Trucks and a captured enemy truck evacuated sitting wounded from the station south of Mons . (One 130 mile round trip was made.)
At about 1800 hours September 5th 10 2 T. Trucks from Army arrived, 3 worked at the Maubege site, 7 at the Mons site making 2 trips each. (By this time the distance involved was shortened by the opening of a Medical installation at La Capelle). The old site Maubege was cleared by 2000 hours.
Shortly after midnight of the 5th, 11 more 2 T. Trucks, 5 1T. Trailers and 10 ambulances arrived and by 0410 hours of the 6th the present site (south of Mons) was completely evacuated.
/s/ James C. Van Valin
JAMES C. VAN VALIN,
Col, Med. Corps,
Division Surgeon
A TRUE COPY:
[signed]
MAURICE S. SCHMIDT
1st. Lt, MAC
Office Executive
15
EVACUATION:
At the stage of greatest confusion the question arose as to the necessity of moving one (1) Clearing Platoon to another location in support of other division troops. In order to get: one (1) Clearing Platoon mobilized for this prospective move, a reconnaissance was made in the town of Maubeuge for a building which could be used as a hospital to hold the enemy wounded. A civilian hospital used by F.F.I. (Free French Forces of the Interior) and staffed by one French male nurse and several French female nurses was found. Fortunately the tactical situation changed and it did not become necessary to carry out this emergency plan. By the morning of 6 September 1944, the evacuation situation had been finally restored to normal and on this day, one (1) platoon of the Clearing Station was able to be mobilized for a forward move in support of the division. A final estimate of the number of casualties evacuated through the Clearing Station during this battle showed one thousand, seventy-nine (1079) enemy wounded and one hundred fifty-two (152) American wounded. The emergencies created by the situation which arose in this area undoubtedly shoved certain deficiencies in the evacuation system. Granted that this situation was an unusual one and not too likely to occur too often, still one must agree that the evacuation system must be sufficiently mobile and elastic to handle any emergency that arises. One can easily picture the confusion that existed at the Clearing Station during this period when as many as five hundred (500) enemy wounded were lying outside the tents awaiting evacuation. One can further speculate on how much more serious this could have been if the weather had been inclement, and going still a step further if these wounded had been our own instead of enemy. The capture of this large number of enemy wounded had bagged about a dozen German Medical Officers and about twenty four (24) German medical soldiers. This captured personnel was utilized for treating and caring for enemy wounded and were in some measure responsible for speeding up treatment of casualties here. The question of the failure of property exchange which occurred in relation to litters and blankets will be taken u below under heading of SUPPLY.
Following the battle of `The Mons pocket` [35 miles south of Brussels ] and as the division advanced to the Siegfried Line on the German Border, evacuation within the division remained normal. Meanwhile, evacuation hospitals had moved into Belgium and the long distances from the Division Clearing Station to hospitals had now decreased. The division had arrived in the vicinity of the German border and the entire Clearing Station functioned with a Field Hospital in support. Between this phase of the operations and the beginning of the battle of Germany certain changes took place in the medical support of the division by Army Medical Groups. These changes will be discussed under `The Battle of Germany`.
SUPPLY:
During the short period prior to the Marigny breakthrough, the divisional medical service had been reequipped and resupplied with items used up or lost in previous combat. Therefore, with the start of this operation there was no grave shortages of medical items. In view of the fact that the casualties during this operation were relatively light, there was no
16
drain on medical supply; furthermore, Army Medical Supply Depots were initially located within a distance which allowed easy and quick replenishment of supplies. Property exchange was normal and the Division Medical Supply was able to keep on hand an authorized overage of litters, blankets, and splints. No problems of supply or supply exchange occurred until the division took part in the battle of `The Mons Pocket`. The tactical situation at this time and the tremendous number of enemy casualties treated at and evacuated from the Division Clearing Station has been previously discussed. It was at this point that certain items of supply were completely used up and property exchange, especially of litters and blankets became faulty and broke down completely. In addition the functioning Army Medical Supply Dumps had been left far behind during the rapid pursuit of the enemy across France. It appears that the property exchange of blankets and litters first broke down at the field hospitals. Here patients were accepted on litters with blankets but no litters or blankets were given back in return. Written `I O.U`s` were given to the ambulance drivers who complained about this practice but these same ambulance drivers were there upon given excuses that hospital property exchange of these same items had broken down at the rear medical installations. The blame was finally put on the evacuation facilities at the `air strips` where it was reported that litter patients were being flown to the United Kingdom but that no litters or blankets were being returned in exchange. It is no wonder that within a very short time all the basic load of litters and blankets plus the excess load of litters and blankets were almost exhausted within the division. At one stage of the evacuation it was necessary to instruct ambulance drivers that in the case of a litter patient if the hospital was unable to effect an exchange of litter and blankets, the patient was to be left at the hospital without the litter and blankets, which were to be returned to the Clearing Station. This critical supply situation was not completely relieved until the morning of 5 September 1944 at which time the Clearing Station received one hundred (100) litters and three hundred (300) blankets. Within forty-eight (48) hours litters were available at Army Medical Supply Depots which meanwhile had moved closer to the Clearing Station site.
Following the battle of `The Mons Pocket` and with the resupply of litters, blankets, splints, bandages, dressings, and plasma, Division Medical Supply was again able to furnish normal supply service on the division`s continued drive across Belgium to the German border. Shortly after the arrival of the division at the Siegfried Line and prior to the battle of Germany, Army Medical Supply Depots set up in the vicinity of Eupen within ten (10) miles of Division Medical Supply and here the requisitioning and supply of all medical items once more assumed normal character.
PERSONNEL:
The only important changes in personnel which occurred during this period were those which had been created by recent changes in T/O. This major change was that which provided one MAC officer (1st Lt.) to assume the duties of Assistant Battalion Surgeon. With this change in the T/O
17
of the Regimental Medical Detachment one (1) Medical Corps Officer assumed the duties of Assistant Regimental Surgeon. Other changes which were not put into effect at this time because they were disapproved by the Division Surgeon, were those turning over the duties of S-3 of the Medical Battalion to an MAC officer (Captain), replacing the Medical Inspector (Major, MC) with either a Sanitary Corps Officer or MAC officer in the rank of either Captain or Major, and removing the Division Veterinarian (Major, VC). These changes involved the requisition of nine (9) MAC Officers who arrived at the division at various intervals. The complete change over was effected by 2 September 1944. Although it had been contemplated with the new T/O changes there would be created an excess of Medical Corps Officers for use in other medical units, no transfers were made and at the end of this period an overage of four (4) Medical Corps Officers existed.
SANITATION AND HEALTH:
The remainder of the month of July and the entire month of August were characterized by hot summer weather and very light rain fall. Roads and bivouac areas were for the most part dry and dusty. Although buildings were available for housing, the weather and the rapid progress of the tactical situation favored the use of open fields and wooded sections for bivouac of troops. This preference for open bivouac areas was further dictated because of the large number of flies which were to be found in and around civilian homes and farms. Fly-control measures within these bivouac areas were continued. Latrine and kitchen discipline was rigidly enforced and consequently fly-borne diseases were kept at a minimum. Mosquitoes were not too prevalent except in certain areas and these were again identified as the Culex variety. At the close of this period the climate underwent a change. Cold weather prevailed and rain fall became heavy. With this decided change in weather, troops again began to billet in civilian establishments and public buildings. Many of the divisional units which were bivouacked in open fields were forced out of these areas to seek cover and protection from the weather in buildings.
Water Supply:
Water discipline continued to be excellent and all water used for drinking and cooking was obtained from controlled water distribution points provided by the division or other military organizations. The streams and fresh water ponds were the primary source of water supply utilized for these purposes. Bathing and laundering were prohibited in these water sources which provided the water used for drinking and cooking.
Waste Disposal:
Again latrine facilities consisted of straddle trenches, `cat holes` and where buildings were available some flush toilets were found and used. All kitchen wastes, trash, rubbish, and cans were disposed of either by burial or incineration. Certain areas within town limits which had been used by the civilians as trash dumps were similarly used by the division. It may be
18
noted at this time that the French and Belgians near these trash dumps made it a practice of `salvaging` much of the rubbish dumped by military units especially wooden crates, card-board boxes, tin cans etc.
Messes:
Messing facilities and kitchens were handled exactly the same as in the previous period.
Food:
This period of operation saw the consumption primarily a `B` ration. The emergency field rations were used only when the tactical situation required. Fresh meats, fresh bread, and butter etc, became a frequent issue and because of a good variety in the ration issue supplementing the messes by local purchases practically disappeared; at no time was it felt that the diet should be supplemented with vitamins.
Diseases:
Malaria: Malaria and FUO`s showed no evidence of decreasing and during the month of August there were reported three hundred ninety-two (392) cases of Malaria and one hundred forty (140) cases of FUO`s. All efforts were still directed toward controlling the disease by use of atabrine prophylaxis. It is felt that a weakened resistance of the men due to continued combat was a contributing factor to the increased incidence of the disease. It was further believed that none of these cases were other than an exacerbation of chronic malaria which had had its origin in the Mediterranean Theatre.
Venereal Disease: As in the month of` July only one new case of venereal disease was reported for the Month of August. This low venereal rate was attributed to the fact that the division was in combat, and that social contact between military personnel and civilian personnel was practically non-existent.
BATTLE OF GERMANY, 12 SEPTEMBER 1944 TO 31 DECEMBER 1944:
Having reached the Siegfried Line the tactical mission now confronting the division was the breaching of this formidable defense. The Siegfried Line is best described as a system of defense made up of several `belts` manned by pill boxes, machine gun nests, barbed wire tank traps, `dragons teeth` and other field fortifications. Without any let up the division started its push through the Siegfried Line on 12 September 1944. The push forward was relatively slow and in the face of a more organized German defense. Artillery was much more active and the troops manning the Siegfried Line were apparently of a higher calibre than the division had encountered since its breakthrough at Marigny. However in spite of the determined defense and the small infantry end tank counter-attacks, the Siegfried Line was completely breeched on the 15th of September 1944 by one (1) regiment of the division. However two days later an entire
19
new German division which was one of the best we had encountered to date in the European campaign took up a position in front of the division centre. The defense set up by this unit was stubborn and well coordinated, and the terrain lent itself to defensive tactics. The push toward the big industrial city of Aachen was slow and every house in the small towns on the road to Aachen was stubbornly defended. By 1 October 1944 Aachen was contained on three sides, West, south and east. Meanwhile the enemy had refused to offer to surrender and prepared to defend the city. The ensuing battle became known as `The Battle For Aachen`. It lasted until the 21 October 1944 at which time the city was surrendered. The total number of prisoners taken by the division was almost six thousand (6000). The slow and methodical clearing of this city by the division served to keep casualties relatively low. It was the first time since being in combat in this wav that the division had fought this type of battle, namely house-to-house and street-to-street fighting which occurs in the prepared defense of a large city. Futhermore this type of fighting produced certain problems of evacuation which will be discussed below.
With the surrender of Aachen operations died down to active patrolling and the enemy`s improvement of his defensive positions. The next mission of the division can be described as the attack toward the Roer River. This river was one of the natural barriers protecting the city of Cologne and the Ruhr industrial sector along the Rhine River. On the 10th November 1944 the division moved to the Stolberg area for this attack. Due to extremely heavy rain fall which created tremendous problems of movement and transportation the attack was postponed until the 16th November 1944. The area of attack was northeast through thick woods (Hurtgen Forest), and with few passable roads. Several hills in the heavy forest provided natural advantages to the enemy; the town areas were well fortified and the enemy had made use of his time to lay intensive mine fields, set up rows of barbed wire, and to dig in among the heavy trees and dense underbrush. The subsequent operation was one of the most difficult the division had engaged in on the continent.
The following conclusions taken from selected intelligence reports of G-2, 1st US Infantry Division, will describe in brief the difficulties encountered by the division.
`a. There is no doubt that enemy resistance to the 1st US Infantry Division offensive of 16 November, was as tenacious and determined as any encountered in the Division`s campaigns. By virtue of his stubborn reluctance to give up so much as a foot of defendable ground, the enemy was able to inflict a considerable number of casualties on our troops. In this he was aided by a terrain which was as unrelenting as the enemy himself. The deep woods in which the 26th US Infantry forced its way precluded the use of any support weapons except those which could be carried through the mud and underbrush on a man`s back. Enemy mortar and artillery fire, even heavier during this offensive than the concentrations laid on the VERLAUTENHEIDE Ridge in the Battle for AACHEN, was increased in effectiveness by the high percentage of tree bursts obtained in the woods. Furthermore, the enemy was retreating over terrain which he knew intimately, and on which he had registered his artillery. At the close of the period it was estimated that the enemy artillery was equal in number to our own, the first time that such an unadvantageous ratio had prevailed.
20
b. The morale of the enemy troops, by all previous experience, should have been shaky. It was not. Small groups, surrounded and cut off, refused to surrender. If the German command often sent suicidally small forces to perform what should have been battalion or even regimental missions, at least those forces fought until they were exterminated. Never before has the 1st Division encountered an enemy regimental commander personally directing local counter-attacks, yet it happened during this operation, when the colonel commanding the 104th Regiment was captured fighting an isolated and essentially hopeless engagement.`
It was estimated that over three thousand (3000) prisoners were captured by the division and two (2) divisions almost completely destroyed.
By 6 December 1944, the division had completed its penetration of the Hurtgen Forest. and had reached its objectives on the main east west road from Aachen to Duren at a point about four (4) miles from Duren . Here the division was replaced in the line by the 9th US Infantry Division and withdrawn to an area west of Aachen to undergo a so-called rest period, which incidentally was the first time since the D-day landings on the continent 6 June 1944 that the division had been officially withdrawn from the line. However, this rest period favored only two combat teams of the division since one combat team was attached to V Corps to take up a defensive sector in the Monschau area. During the rest period short passes and leaves, (48-72 hrs) were granted to enlisted personnel and officers. Recreational trips were made to Paris and other large cities in Belgium. Reorganization in every sense of the word was put into effect.
On 13 December 1944 the one combat team which had been on detached service returned to division control and likewise started its rest period. But on 16 December 1944 with the start of the counter-offensive by Rundstedt against the First US Army, the division was placed on a six (6) hour alert, and on the morning of 17th December 1944, one combat team of the division moved into a defensive sector just south of Monschau (Ardennes Forest) to protect Liege. This one combat team was followed by the rest of the division within twenty-four (24) hours. One (1) combat team took up its position east of Malmedy and the other combat team was given the mission of rounding up or destroying German parachutists which had been dropped in the vicinity of Eupen.
These paratroopers failed to accomplish their mission which was primarily to block the arrival of reinforcing troops. A strong crosswind and an inadequate briefing of the JU-52 pilots scattered the units and their weapons and equipment over an area far wider than planned. Much of the equipment was lost and damaged; radios were knocked out and failed to function. About all these paratroopers accomplished was a harassing of a few isolated vehicles and the taking of a few prisoners. Under these circumstances it was not long before the majority of parachutists had been rounded up and for many days members of this group kept showing up all over the area and turning themselves into whatever American troops they could find. By the 19th December 1944 this combat team had carried out its mission and had taken its position in the line.
21
The following data on this military situation has been taken from G-2 periodic report #201, 1st US Infantry Division.
`On 16 December 1944 the enemy launched a high-geared meticulously planned counter-attack on the centre of the First US Army line between Monschau and Echternach The ultimate objectives of this drive were the allied supply port of Antwerp and the big communications center of Brussels intermediate; objectives were the Meuse River and the city of Liege. One of the primary objectives and the one most necessary for the success of this operation was the seizure of the enormous American supply dumps in Liege, Verviers, and Eupen area. The initial attack was spearheaded by the 1st SS Panzer Division and 12th SS Panzer Division. Initially the breakthrough was carried out according to plan. The 1st SS Panzer had pushed deep into this sector and was followed by the 12th SS Panzer whose mission apparently was to roll back the northern flank and advance toward the American supply dumps. This was the situation that existed when the division (initially one (1) combat team) arrived in this sector. The first attacks of the 12th SS Panzer were beaten off on the 17th December 1944. On the 19th December 1944 more heavy counter-attacks were beaten off with losses to the enemy in both personnel and materiel. By this time the 1st SS Panzer which had penetrated deeply was in serious straits because of the 12th SS Panzers` failure to clean up the northern flank. The 3rd Parachute division (German) was brought in on the 20th December 1944 to support the enemy`s frantic attempts to break through this position and on the 21st December 1944 the enemy`s major assault was launched. After a day of heavy fighting the attack was defeated and although in the subsequent days, he still continued to attack fiercely, he achieved no success. With the collapse of his plan to force his way north, the enemy subsided into the defense, bringing up Infantry units to dig in and hold the line while the badly mauled 12th SS Panzer was withdrawn for repairs.`
EVACUATION:
Up until the beginning of the battle for Aachen evacuation was well organized and quite normal. The vicinity of Eupen was set up as the center of all medical installations including hospitals for patients with special diseases or casualties. Evacuation hospitals took the majority of patients and casualties; 622nd Separate Clearing Company was designated as the Exhaustion Center and accepted all Neuro-psychiatric (NP) cases; 91st Medical Gas Treatment Battalion took care of Malaria, communicable and contagious diseases and self-inflicted wounds (SIW`s); 633rd Separate Clearing Company received patients with respiratory diseases. In addition, the Corps Clearing Station (50th Medical Battalion) was set up to act as a holding platoon for patients who would be able to return to duty within ten (10) days; these patients returned direct to duty back through the Division Clearing Station. Because of this specialized handling of patients, evacuation was controlled through an Ambulance Regulating Point which triaged the patients and dispatched them to the various hospital installations. Field hospitals were likewise located in same general vicinity but most of them kept in mobile reserve. At this time the division was being supported by the entire complement of a Field Hospital. This was a decided improvement over previous plans
22
when the division was supported by only one platoon of a Field Hospital. Because of the fact that the Division Clearing Station was within five (5) miles of the nearest evacuation hospital the Field Hospital did not function and non transportable patients were evacuated directly to the evacuation hospital.
The Division Clearing Station did not move at anytime during the penetration of the Siegfried Line and the capture of the city of Aachen. Only one combat team of the division was actually engaged in the house-to-house and street-to-street fighting within the city limits of Aachen. Previously evacuation forward of the Battalion Aid Stations was generally accomplished by `jeep` ambulance or litter bearers. Within the city itself, `jeeps` could be used almost exclusively in retrieving wounded and returning them to the Battalion Aid Stations. However, with the large amount of debris, especially glass, which cluttered up the streets of the city, frequent tire punctures of the `jeeps` occurred. As many as twelve (12) punctures were reported in one day by the driver of one of these `jeep` ambulances. To prevent the slowing up of evacuation, `weasels` (tracked `jeeps`) were substituted and worked out very well. These tracked `jeeps` were able to cross any difficult terrain and could be improvised to hold two (2) litter patients. At times during the advance through the city the Battalion Aid Station was split. Telephone communication was maintained between these stations and the rifle companies so that the Battalion and Assistant Battalion Surgeon could immediately dispatch a `weasel` or litter bearers to a point where casualties had occurred. This tended toward a smooth and rapid evacuation. All possible protection was given to the Battalion Aid Station by installing them in well-protected cellars or air-raid shelters.
The medical plan for the attack towards the Roar River which began on 10 November 1944 anticipated that because of the terrain, the weather, and the poor road network the use of motor transportation for evacuation of casualties within the forward areas would almost be impossible; therefore, extra litter bearers were obtained from higher headquarters and placed with each Collecting Station to assist in the evacuation forward of the aid stations. Initially, eighty (80) litter bearers were obtained but by the time that the division had penetrated the Hurtgen Forest, approximately two hundred forty (240) litter bearers had been employed. Litter carries were very difficult and averaged two thousand (2000) yards. Enemy artillery and mortar fire which create bursts in the forest caused a large number of casualties among these litter bearers. These two hundred forty (240) litter bearers were not used at one time but constituted the number of personnel needed to maintain approximately eighty (80) litter bearers in all Battalion Aid Stations at all times. At times when casualties were even greater than could be handled by this complement of litter bearers, basic infantry were drafted for duty as litter bearers. Casualties during this period were heavy. To conserve the use of ambulances, other organic transportation (3/4 ton, 1 1/2 ton and 2 1/2 ton trucks) were used to evacuate walking wounded not only from Collecting Stations to Clearing Station but also from Clearing Station to hospitals. In addition to being heavy, many of the casualties were very severe. One Field Hospital Platoon set up close to the Clearing Station and all non-transportable patients were evacuated there and treated. On 21 November 1944, the Clearing Station treated and
23
evacuated five hundred one (501) patients (including enemy casualties) in a twenty four (24) hour period.
On 5 December 1944 following the completion of its mission in the attack towards the Roar River, the division was relieved and bean its return to its rest area by infiltration. This relief and return to rest area involved only two combat teams. One combat team was now detached from the division to take up a defensive sector in the vicinity of Monschau. In view of the fact that this combat team would be dispersed quite widely a special system of evacuation was put into effect. The Collecting Station attached to this combat team was in a position to evacuate only two (2) of the Battalion Aid Stations of this combat team. It was able to clear these patients through a Clearing Station of another infantry division. The other battalion of the combat team carried out its evacuation direct from Battalion Aid Station to hospital. To accomplish this extra ambulances from the Collecting Station were attached. This system of evacuation was no problem except from the standpoint of administration with respect to reports on casualties. Evacuation of this detached combat team reverted to normal when it again went under division control on 16 December 1944 with the beginning of the German counter-offensive through the Ardennes Forest , the division was immediately committed to defend part of the northern boundary of this salient. Because of the confused situation, no Clearing Station was moved to this sector to effect evacuation. The one combat team which first arrived in this area evacuated through its attached Collecting Station to Clearing Station of other infantry units nearby. The second combat team which was committed to the same sector shortly thereafter effected its evacuation in, the same manner. However, the third combat team which had the mission of protecting the city of Eupen from parachutists, because of the closeness of hospitals in Eupen evacuated directly from Collecting Station directly to hospital. After several days when the tactical situation had cleared and when the entire division joined together to set up a defense, one platoon of the Clearing Company was moved down into this area and resumed normal evacuation of patients.
During the early days of the counter-offensive when the threat to Eupen was serious, many of the hospital installations moved out, thus creating a lack of facilities for holding patients or casualties; thereupon the platoon of the Clearing Company which was north of Eupen was set up as a holding platoon to handle patients who were expected to be ready for duty within seven (7) days. This platoon expanded to a capacity of seventy-five (75) beds. Between the 24th and 28th of December 1944 the, forward operating Clearing Station underwent shelling by enemy artillery apparently directed against artillery batteries located in the vicinity of the Clearing Station. Several of the ward tents were pierced by shell fragments, some of the vehicles were damaged, and the house which was being used as the treatment station was damaged by shell fragments. Because of this the Clearing Station moved back to a new location out of enemy artillery range. On the last day of the year the evacuation setup for the division was normal; no Field Hospital was in support of the division at this time. Evacuation hospitals were located about five (5) miles from the Clearing Station. Because of the limited hospital facilities except for those patients held in our own Clearing Station, evacuation was total.
SUPPLY:
At no time during this period was any difficulty experienced in procuring medical supplies. The Army Medical Supply Depots were well stocked and able to fill the entire needs of the division. With the change in the treatment of `New` Gonorrhea with Penicillin this drug was easily obtained from evacuation hospitals. For a short period of time certain biological products were critical especially Typhus Vaccine but the shortage soon eased. When the German counter-offensive of 16 December 1944 had broken into the First Army lines it overran a numbed of medical installations especially field hospitals. When the division had taken back some of the lost ground in this area it recovered some of this field hospital equipment. This included microscopes, haemocytometers, surgical instruments, generators, tentage and etc. This recaptured equipment was turned into higher headquarters through channels.
PERSONNEL:
No critical shortages of medical department personnel existed at the start of this operation. By normal attrition, the excess in medical officer personnel had been reduced to a point equal to the T/O. Early in the period a system of rotation for Medical Corps Officers with long combat service was instituted by higher headquarters. These men were to be transferred to a General Hospital in the Communications Zone and were to be replaced by young recent medical school graduates. The names of nine (9) Medical Corps Officers and one (1) Dental Corps Officer were submitted. The rotation was carried out and by 10 December 1944 had been completed. Two (2) of the officers transferred to the division in this rotation po1icr were definitely unsatisfactory for combat duty. One was almost forty (40) years of age and both were marked `Limited Service` on their Officers` Qualification Card (66-1). The names of these two medical officers were submitted to higher headquarters for transfer out of the division because of their physical condition and this was effected at a later date, when they were replaced by two (2) other Medical Corps Officers. All these Medical Corps officers were assigned as Battalion Surgeons in a Battalion Aid Station or as a company officer in a collecting Station. None of these new officers had had any previous field training or combat experience. They were tutored by the experienced Medical Corps Officers in the division and gradually indoctrinated into combat medical service. To date the majority of these men have proved satisfactory and have already completed several weeks of combat. Early in this period the duties of the S-3 of the Medical Battalion and the duties of the Medical Inspector in the Division Surgeons` Office were assumed by M.A.C. Officers. At about the same time, the Division Veterinarian, who had been in excess since the new T/O of July 1943, was transferred from the division. On 11 November 1944 Colonel James C. Van Valin (Division Surgeon) was transferred from the division and his duties were assumed by Lt. Colonel (then Major) John Ficicchy Jr. During the heavy fighting in the Hurtgen Forest several M.A.C. officers were evacuated out of the division because of wounds or diseases. To replace these men immediately, non-commissioned medical personnel were assigned their duties and later on received battlefield appointment to 2nd Lt. M.A.C. Up to the
25
close of this period five (5) such battlefield appointments have been made. The M.A.C. Officers appointed by this method have worked out most satisfactory and it is intended that this plan will be followed out in the future when vacancies in the Medical Administrative Corps occur. In the early part of December a board of officers was held to examine candidates for commission to 2nd Lt. M.A.C. This board had completed its examinations by the end of this period but at that time no appointment by this method had been made. During the rest period following the attack to the Roer River, a large shortage of enlisted personnel existed in the division. This shortage had been created by casualties and diseases occurring in the campaign. However, by the 16th December 1944 when, the division was committed to stem the German counter-offensive the T/O shortages had been made up by the return of Medical Department personnel from hospital to duty and by requisitions through G-1. At that time the division medical service showed twenty-three (23) medical enlisted personnel over T/O.
SANITATION AND HEALTH:
The start of this period was characterized by cold weather and heavy rainfall. Drainage was poor due to the heavy rainfall and type of terrain. For this reason the majority of troops secured buildings of all types for billets and C.P.`s. During the attack to the Roer River rainfall was the heaviest that the division had experienced at any time. The Hurtgen Forest became a veritable quagmire and because of the tactical situation men were forced to live outside under the most trying conditions. With the arrival of December the temperature dropped to freezing and snow fell on several occasions. It was during this latter part of the period with freezing temperature and snow that the division was committed against the German counteroffensive. The majority of troops with the exception of service troops were required to spend days in foxholes. At the close of this period real cold winter weather had set in with temperature ranging around fifteen (15) degrees.
Water Supply:
All water used for drinking and cooking continued to be obtained from controlled water distribution points operated by division engineers. Bathing facilities were available at military shower points, approved civilian bathing facilities, and nearby hospitals; laundry facilities were provided by a quartermaster laundry company attached to the division. Much of the personal laundry of officers and enlisted personnel was done by civilians. In one of the towns where the local municipal water supply was in operation a specimen taken at random from a tap and examined bacteriologically at the 10th General Medical Laboratory revealed this source to be `non-potable` and was put `Off Limits` for drinking and cooking purposes.
Waste Disposal:
Latrine facilities again consisted of straddle trenches, `cat holes`, and
26
flush toilets where available and operating properly. Kitchen wastes, trash, rubbish, and cans were disposed of by burial or incineration. As the weather became colder the ground hardened and snow fell; disposal by burial became impossible and consequently incineration was used; when this was not possible, dumping in selected areas was established. The local population continued to `salvage` much of the rubbish dumped by military units.
Messes:
Kitchen facilities during combat were generally established in Battalion Field Train areas and from there transported in marmite cans to the front line troops. Where possi1le, field trains were set up in buildings approved by the unit surgeon. Service troops of the division in general utilized buildings for their kitchens and messes.
Food:
`B` ration continued to be issued supplemented by emergency rations as the tactical situation required. At least two hot cooked meals per day were consumed by the troops. The issue was satisfactory as to quantity and quality, there being plenty of fresh meat and fresh bread, butter, flour, fresh fruits, and on a few occasions fresh eggs. With this type of ration it was possible to prepare a variety of menus and to prepare the food to suit the appetite of the troops. Since the local food situation was most critical and strict rationing was in effect, there was practically no supplementing of messes by local purchases. On rare occasions where the tactical situation allowed only the consumption of emergency field rations, vitamin supplements (multi-vitamin pills) were used on the recommendation of unit surgeon.
Diseases:
Malaria: The month of September showed a decided decrease in Malaria, and FUO`s, there being one hundred ninety-eight (198) cases of Malaria and fifty-eight (58) cases of FUO`s. This decrease continued throughout the month of October -- one hundred eighty-three (183) cases of Malaria and thirty-two (32) cases of FUO -- through the month of November - one hundred twenty-three (123) cases of Malaria and fifty-three (53) cases of FUO -- and the month of December - ninety-seven (97) cases of Malaria and forty-two (42) cases of FUO. This gradual decline in the incidence of this disease probably represents a seasonal decline such as was experienced by the division during the same season one year ago. Atabrine prophylaxis is now being used only by those individuals who have had several recurrent attacks while on the continent. The policy of giving atabrine to all men who had been in the Mediterranean Theatre has gradually gone out of operation. This has been a gradual change brought on by the large turn over of personnel in the division resulting in a large number of reinforcements who have never had military service in malarial areas.
27
Venereal Diseases: With the start of the Battle of Germany, venereal diseases began to increase markedly reaching forty-seven (47) cases for the four (4) week period of November and also forty-seven (47) cases for the five (5) week period of December. As this venereal rate showed definite increase from month to month, every effort was made by the medical department to acquaint the men with the dangers of venereal disease and stress the importance of venereal prophylaxis, both chemical and mechanical. Prophylaxis Stations were maintained in all unit dispensaries. Towns which were `On Limits` for authorized recreation were well covered by pro-stations established by higher headquarters. Men going on pass to these recreational centers were given location of these pro-stations and given the opportunity to avail themselves of condoms. Many towns were "Off Limits" and the Military Police through the Division Provost Marshal carried out the enforcement of this policy. Likewise the military police apprehended prostitutes and turned them over to local police authorities. All houses of prostitution were closed to military personnel. A careful survey of the contacts causing these venereal diseases was made by the Division Venereal Disease Control Officer who discovered that a majority of these venereal diseases were picked up in large cities on the continent to which the troops made authorized recreational visits; these cities included Paris, Liege and Verviers. In attempting to analyze the reasons for this increase there appears to be several reasons. Psychologically, troops who have been in combat for a long period of time such as this division develop an indifference to the dangers of venereal disease as compared to the dangers they have experienced in actual combat and even though well informed on the dangers of venereal disease and the necessity for venereal prophylaxis, they make no effort to protect themselves. Furthermore, the War Department policy of not penalizing a man by loss of time or loss of pay had undoubtedly done much to foster laxity on the part of the individual. In addition, the new Penicillin treatment which was instituted in the division in the early part of September, produced such excellent results with such a minimum of time and discomfort that the enlisted men accepted venereal disease (Gonorrhea) as a less serious disease than a `common cold`. To date the treatment of Gonorrhea with Penicillin with the patient on a duty status has proved most satisfactory and it is estimated that over ninety (90%) percent of the `New` Gonorrhea recover.
Communicable Diseases:
Diptheria: Within the areas which the division occupied during this period many cases of diptheria among civilian population were reported. To prevent this condition from spreading among military personnel, all efforts were made to isolate suspicious cases of sore throat and to obtain a throat culture through the 10th General Medical Laboratory.
In spite of the fact that many troops were billeted in civilian houses, Scabies was not a common disease among the troops. The same can be said about Pediculosis and so far as is known, no case of Typhus Fever was ever reported in the military personnel of the division.
28
In the latter part of November a circular from higher headquarters Subjects "Typhus Immunization", directed that by the 20th December 1944, all members of the command would be inoculated against Typhus Fever. A shortage of vaccine which existed at the Medical Supply Depot until the 11th December 1944 and the tactical situation after that date prevented the complete immunization of the division. However, seventy-five (75%) percent of the command was able to be immunized and it is anticipated that at the earliest opportunity the unfinished immunizations will be completed
Trench Foot: The first cases of Trench Foot in the division were reported the later part of October 1944. As mentioned above the climate at this time was cold and wet; bivouac areas were muddy and rainfall was leery heavy. Overshoes were not available and men were unable in some cases to take proper are of their feet. It was not until the start of the attack toward the Roer River that Trench Foot began to occur regularly and show a gradual increase. Those conditions which predisposed to Trench Foot were present during this campaign. For the month of November, one hundred forty-nine 149) cases of Trench Foot were reported. In order to prevent its occurrence certain preventative measures were instituted and overshoes were requisitioned for the combat troops. Unfortunately, the issue of overshoes was unsatisfactory in that large all sizes were not available and at a much later date when overshoes did become available, they were of the canvas type which experience had shown were permeable to water. However each man was instructed in the proper daily care of his feet, and made to understand how important this preventive care was. Each soldier was supplied with a minimum of five (5) pairs of socks; laundry service for socks was provided by the division quartermaster; `drying tents` were established accompany level. The following is a directive issued to the troops on this subject:
13 November 1944
PREVENTION OF TRENCH FOOT
1. Each company will provide a shelter with stove and rack for drying socks (`Drying Tent`). An orderly will be detailed to rinse out socks in a solution of hypochlorite (1 ounce to 25 gals. of water) and dry them.
2. Socks will be turned in daily for rinsing and drying. Each man will be issued a dry pair of socks daily.
3. Men will remove shoes when sleeping.
4. Shoes and socks will be removed thrice daily and the men will massage each others feet for at least five (5) minutes.
29
5. Battalion Surgeons will inspect each company daily to insure that feet are being massaged, socks being treated and that socks are available.
6. Battalion S-4 will insure that each man has five (5) pairs of socks.
7. Overshoes will be worn.
8. Daily foot inspections will be held and blisters and other foot lesions will be treated promptly.
9. Socks will be marked by sizes so that each man will be issued socks that fit him.
All these cases of Trench Foot that occurred were treated as litter patients. Shoes and socks were removed, and where feasible `cradles` were placed on the litters to keep the pressure of blankets off the feet during transportation. All men who had a diagnosis of Trench Foot were evacuated to hospitals. However, after a survey of hospitalized cases showed over fifty (50%) percent of cases diagnosed as Trench Foot not to be Trench Foot, and that this diagnosis could easily be malingered, the following policy was then put in force.
29a
HEADQUARTERS 1ST US INFANTRY DIVISION
Office of the Division Surgeon
APO 1, U.S. Army
28 November 1944
SUBJECT: Trench Foot.
TO : All Unit Surgeons and Attached, 1st US Inf Div.
At a conference on Trench Foot held by First Army Surgeon, it was reported that 50% of cases arriving at Army Hospitals with a diagnosis of `Trench Foot or Immersion Foot` were subsequently proven not to be Trench Foot, and returned to duty. Furthermore, it was learned that this diagnosis easily lent itself to malingering by personnel acquainted with the subjective symptoms of the disease.
In order to correct the above conditions, the following policy has been recommended by Surgeon, First Army, and will be followed out by the respective units concerned:
1. Regimental Aid Stations, Battalion Aid Stations and Unit Dispensaries.
Unit Surgeons will assure themselves that the term Trench Foot or Immersion Foot does not appear on the E.M.T. of patients unless objective signs are present. In cases where the diagnosis is suspected but not evident, the term `Under observation, undiagnosed` will be used. In talking with the patient concerned the term Trench Foot or Immersion Foot will be avoided. However, the evacuation of the patient will be effected by litter with all footwear removed and where possible with cradle on litter to prevent pressure of blankets on the feet.
2. Clearing Station.
All cases arriving at the Clearing Station with a diagnosis of Trench Foot or Immersion Foot, or `Under observation, undiagnosed` will be carefully examined by a Medical Officer. If no objective signs of the condition such as swelling, redness, blistering, etc, are present, the case will be held in the Clearing Station for 48 hours. If no signs appear during that time the patient will be returned to duty and a diagnosis other than Trench Foot or Immersion Foot will be put on the E. M. T. (i.e., `Under observation, undiagnosed`, Trichophytosis, etc). If signs of the disease do appear, the patient will immediately be evacuated to an Army Hospital. While
29b
Ltr, Hq, 1st US Inf Div, Off of the Surg, 28 Nov 1944, Subject: "Trench Foot" continued:
in the Clearing Station, treatment of these cases will be carried out in accordance with current Army directives.
Medical Officers in the Clearing Station will avoid usage of the term Trench Foot or Immersion Foot, where the diagnosis is not positive.
JOHN FICICCHY JR.,
Major, Medical C.,
Division Surgeon.
30
Although the statistics for Trench Foot for the Month of December show an overall increase, the latter part of the month definitely shows a decrease and in spite of the fact that during this period the division was in combat under most difficult conditions which predisposed towards this condition.
It is a known fact that Medical Department Personnel, both officers and enlisted men, are not immune to enemy gun fire, artillery fire or strafing planes. Experience has shown that casualties among company aid men and litter bearers are relatively as high as those suffered by the infantry. It is our experience in the division that of all the service units, the Medical Department has incurred the greatest casualties. This fact is at the present time being recognized; proof of this is shown by the number of bills being presented to Congress to create a Medical Valor Badge for front line medical personnel designed to give them an increase in pay comparable to the infantry soldier who wears the Combat Infantry Badge. A table of the cumulative casualties suffered by the medical personnel of the division from 6 June 1944 to 31 December 1944 follows:
CUMULATIVE CASUALTIES, 6 JUNE 1944 TO 31 DECEMBER 1944
| KIA | WIA | OTHERS | TOTAL | |
|
M.C. | 1 | 14 | *1 | 16 |
|
D.C. | 0 | 1 | 0 | 1 |
|
MAC | 1 | 6 | 1 | 8 |
|
ENL PERS | 50 | 369 | 78 | 497 |
|
TOTAL | 52 | 390 | 80 | 522 |
*This Medical Corps Officer died in a hospital following severe wounds incurred on D-day.
Awards and decorations are indicative of bravery and long faithful service in the performance of one`s duties. The medical personnel of this division have received their share earned under the most difficult of combat conditions. The following table shows the awards and decorations received by Medical Department personnel during the year 1944.
| Officers | EM | Total | |
|
PURPLE HEART | 17 | 144 | *196 |
|
/CLUSTER | 3 | 32 | |
|
BRONZE STAR | 46 | 345 | 401 |
|
/CLUSTER | 3 | 7 | |
|
SILVER STAR | 18 | 124 | 155 |
|
/CLUSTER | 3 | 10 | |
|
LEGION OF MERIT | 1 | 0 | 1 |
|
/CLUSTER | 0 | 0 | |
|
DISTINGUISHED SERVICE CROSS | 5 | 2 | 7 |
|
/CLUSTER | 0 | 0 | |
|
SOLDIER`S MEDAL | 0 | 1 | 1 |
* This figure represents the awards presented by the division. It is estimated that about 325 more PURPLE HEART awards were received by personnel in hospitals.
31
CONCLUSIONS AND RECOMMENDATIONS:
In the months of campaigning by the division many lessons have been learned, the majority of these by experience. As problems have arisen in the medical service of the division, they have in general been carefully studied and in most instances solved. Although the solution of these problems may not be `the solution` yet they have been tried out in actual combat and have been found work out most satisfactorily.
Evacuation:
In my opinion, the cardinal principle of evacuation within the division medical service, is speed. Because of this we have tried to utilize motor transportation as close as possible to the spot where the casualty is first treated by the aid man. It was for this reason that `jeep` ambulances were constructed for first and second echelon medical service. The system of evacuation as carried out in this division is as follows:
The `Jeep" ambulances which are with the Battalion Aid Stations are generally used forward of these installations in order to pick up casualties and return them rapidly to the Battalion Aid Stations. When the terrain is such that these `jeeps` cannot be utilized in this fashion, litter bearers are then used. At times it is feasible to have a litter haul plus a `jeep` haul to the aid station by establishing `jeep` collecting points. The `jeeps` in the Collecting Station are used to supplement ambulances of the Collecting Station. To my knowledge at no time have the litter bearers of the Collecting Station ever been used to carry patients from Battalion Aid Stations to Collecting Stations. In combat when the tactical situation demands the use of many litter bearers forward of the aid station, those of the Collecting Station are attached to the Battalion Aid Sections and used to supplement the litter bearers of the aid station themselves.
When combat teams of the division go into combat, the Collecting Companies of the Medical Battalion are attached to them for tactics and supply. Administrative control is maintained through the medical Battalion. This then places
32
the Collecting Station under command of combat team commander through the Regimental Surgeon. It is the combat team commander who directs the movements and the location of the Collecting Station. With this type of organization it is then customary to place one of the Collecting Company ambulances with each Battalion Aid Station and in some cases one (1) ambulance is attached to the Field Artillery Battalion Aid Station and the Regimental Aid Station. This then leaves a complement of five (5) ambulances at the Collecting Station for evacuation from there to the Clearing Station. Because of the fact that the functioning Clearing Station is kept as far forward as the tactical situation permits, this distribution of ambulances does not place too great a burden on the evacuation from Collecting Station to Clearing Station.
The Clearing Company works as two (2) separate platoons one of which remains in mobile reserve while the other operates. When a movement forward occurs, the platoon in reserve moves to the new site and sets up. The other platoon then clears its station of casualties, loads up, and then becomes the mobile reserve platoon. If movement is rapid as it was in the drive across France and Belgium, this maybe a daily occurrence. This system of movement is known as `leap-frogging`; in cases where movement is relatively slow the mobile platoon is generally moved to the vicinity of the functioning platoon and there remains in mobile reserve. The Clearing Station is evacuated by ambulances supplied by supporting ambulance companies from higher headquarters. In this system of evacuation many times there are too few ambulances to maintain a rapid flow of casualties from the Battalion Aid Station to the Clearing Station. We therefore make it a policy that when casualties are heavy, organic transportation within the medical service will be used. This applies especially to walking wounded patients. This evacuation is sufficiently elastic to allow a variation according to terrain and tactical situation. The average evacuation interval from the time that a casualty is picked up to the time he arrives at the Clearing Station is one (1) hour. Treatment of casualties at first and second echelon medical service is entirely of a first-aid and supportive nature. The Clearing Station does little more than to supplement the treatment already given and sort out the patients for further evacuation. This emphasis on rapid evacuation by motor transportation could be improved by increasing the number of ambulances within a division from thirty (30) (present T/E) to a minimum of thirty-six (36). This would then provide twelve (12) ambulances to each Collecting Company and would allow enough ambulances to cover the Field Artillery Battalions and Special Troops Medical Detachment in combat and in garrison.
The present T/E has made a change in the vehicles of a Battalion Medical Section by eliminating one (1) 1/4 ton 4 x 4 truck (`jeep`) and 4 ton trailer and substituting therefore a 3/4 ton truck, cargo. As has been shown above, the `jeep` of a Battalion Aid Station in combat is used more as an evacuation vehicle rather than a cargo vehicle and eliminating one of these, seriously hampers the speed of evacuation as set up in this division. It is my recommendation that the two (2) 1/4 ton trucks (`jeeps`) be kept in the Battalion Medical Section and that a 3/4 ton truck, cargo, be added to substitute for the two (2) 1/4 ton trailers which were on the previous T/E. This would then give Battalion Medical Sections two (2) 1/4 ton trucks (`jeeps`) without trailers and one (1) 3/4 ton truck, cargo.
33
SUPPLY:
In this campaign the system of supply has in general worked out quite satisfactorily. The maintenance of well stocked supply depots close to divisional units facilitates requisitioning; and rapid replenishment of depleted stocks. There is no doubt that there are many drug items which do not find favor among medical officers and which could be deleted; and on the other hand there are a number of drugs which are not listed in the catalogue supply which are very often asked for by medical officers. Some of the non-expendable items which have never been used by the division medical service are:
Carrier, field, collapsible (`wheeled litters`)
Kits, medical, private (of the Clearing Company)
Prior to the invasion of the continent authority was granted by higher headquarters to turn these items in and at no time during combat has the need for these ever arisen.
The present T/E for generators provided for the Medical Battalion the following:
Electric Lighting Equipment Set, No 3, (3-KVA) - 2
Electric Lighting Equipment Set, No. 2, (1 KW) - 4
Experience has shown that the Electric Lighting Equipment Set No. 2, (1 KW) has been unsatisfactory in its performance due to the number of repairs required to keep it operating for long periods of time. The Electric Lighting Equipment Set No. 3, (3-KVA) however has been most satisfactory and has been used as long as five hundred seventy-six (576) hours steadily without major repairs. It is my recommendation that another Electric Lighting Equipment Set No. 3, (3-KVA) be substituted for the four (4) Electric Lighting Equipment Sets, No. 2, (1 KW). This would then furnish each Clearing Platoon with one
(1) 3-KVA, and another to rotate at intervals or when one of the generators fails to operate. Regardless whether this change is made, the present T/E which authorizes two (2) of the Electric Lighting Equipment Sets, No. 3, (3-KVA) should provide for trailers on which these generators could be mounted permanently. This would undoubtedly prolong the life of the generator.
PERSONNEL:
The one major conclusion to be drawn from the present T/O set up which has been tried out under combat conditions, is that Medical Administrative Corps Officers and Sanitary Corps Officers are able to do many of the duties which were previously assigned to Medical Corps Officers and thereby conserve the so called professional specialist. In this division, the MAC`s acting as Assistant Battalion Surgeons have done their work in an excellent manner. After a though training in first-aid and medical administration under the direct supervision of a medical Officer they are able to treat casualties, handle transportation, make out reports, and do other duties which are necessary in a Battalion Medical Section. It is generally agreed that one (1) Medical Officer in a Battalion Aid Station is necessary in order to exercise professional judgement and skill
34
in certain cases. One other thing, which has been demonstrated in combat is that well trained non-commissioned medical department personnel (Surgical and Medical Technicians) are able to take over these MAC duties. This has been proved by our experience.
One of the biggest personnel problems which has come up in the division during combat has the `plight` of the Battalion Surgeon. At the start of this campaign all the Battalion Surgeons had had previous combat experience. A number of them had been through the North African and Sicilian campaigns, practically all of them had received one or more decorations for gallantry in action and some had been wounded. A number of these `old timers` were approaching forty years of age and were reaching a point where physically and some cases mentally they were unable to carry out their duties. It was impossible to rotate them within the divisional medical service because the other Medical Corns Officers in the division had either been tried as Battalion Surgeons and did not work out satisfactorily or physically were not able to carry out these duties. On the D-day landings one of the Battalion Surgeons was seriously wounded and subsequently died in a hospital; another Battalion Surgeon was wounded and never returned to duty with this organization. Subsequent to that one other Battalion Surgeon was killed and many others wounded. Although rotation of Medical Officers from combat units to hospital had been talked about nothing was done until late in the year. At this time, the division received young recent medical school graduates and rotation was accomplished for several of these old Battalion Surgeons. Although the new arrivals were young and healthy, they lacked any training in field medical service and none of them were in any way acquainted with the duties of a Battalion Surgeon. As far as the medical service of the division is concerned, these medical officers could only be used in first and second echelons of medical service, that is, either in the Battalion Aid Station or Collecting Station. During combat, there is no time during which these men can receive adequate training in their duties and yet in spite of this, these men were indoctrinated by a system of tutoring by which an experienced Battalion Surgeon would remain with the Medical Officer until such time it was felt that he could take over the duties himself. Many of these new men had had previous assignments the general hospitals and had developed a `hospital complex` in other words a feeling that they were not fitted for this type of combat duty. In my opinion this system is an injustice to both the trained and untrained Medical officer. The experienced Medical officer after `serving his time` with combat troops where professional work is limited feels that he is entitled to some type of hospital service where he can again become a `doctor`; the officer inexperienced in combat service feels bitter because after having been in a hospital for a relative long period of time he develops the attitude that it is the only duty for which he is fitted. It is my opinion that the type of men needed for the front line combat service should be young, healthy, and preferably not a `specialist`. I feel like many other division surgeons that it is not difficult for a doctor to perform professional duties at a hospital for after all this type of work is merely an extension of either his internship or private practice; but I am convinced that it is most difficult for a Medical Officer without special training to take over the duties of a Battalion Surgeon. I would also recommend that frequent rotation for Medical Corps Officers, preferably every six (6) months to a year, be instituted to effect a change of Medical Officers from hospitals
35
to field units and vice-versa. I feel certain that this would improve the medical service in both the hospitals and the field units and at the same time go a long way towards upholding the morale of the combat Medical Corps Officers.
SANITATION AND HEALTH:
The major disease, problem within the division is Malaria, chronic, recurrent. We have had evidence to show that the loss of man-days from this disease has been extremely high. We have likewise been through various systems of treatment. The early therapy of this disease provided for a short hospitalization of usually 7 to 10 days at which time under quinine or atabrine, the patient became symptom free and returned immediately to duty. We have likewise seen the situation where men with this disease are evacuated to the Communication Zone and undergo longer periods of hospitalization, treatment, and convalescence. The majority of these men likewise eventually return to duty. This latter method of treatment seems to offer some assurance after the patient returns to duty, that he is less liable to undergo recurrent attacks of malaria; and yet it is not at all uncommon to find even at this late stage many, cases of recurrent malaria which exhibit evidence of low grade anemia, weakness, and debility and who continue to be evacuated to hospitals and continue to be returned to duty. In some cases we have attempted to administratively place these men on a `Limited Service` in order to prevent their being returned to either this division or any other combat unit, but this has not worked out well. These particular patients (and they do continue to be patients) in time lose their value to the division because they cannot be depended upon to be ready for duty when they are needed most. It seems to me that men who have had recurrent attacks of Malaria for as many as six (6) to twelve (12) times and have been evacuated to hospitals repeatedly should be given some sort of consideration towards either returning to the Zone of the Interior for long and complete hospitalization or being placed in service with a non-combat unit.
JOHN FICICCHY JR.,
Lt. Co1., Med C.
Division Surgeon
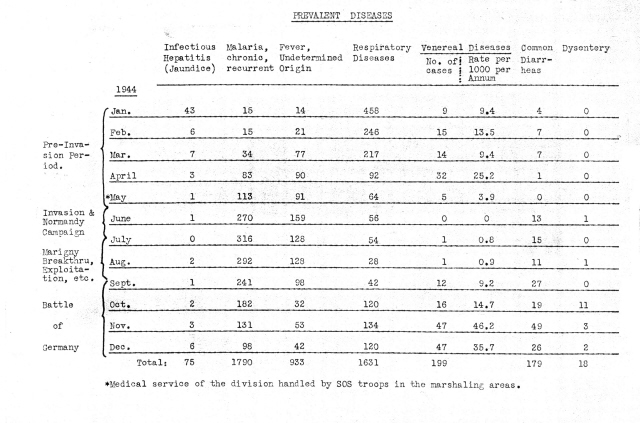
ANNEX
REPORT OF DIVISION PSYCHIATRIST
HEADQUARTERS 1ST US INFANTRY DIVISION
Office of the Division Surgeon
APO 1, U.S. Army
19 January 1945.
SUBJECT: Annual Report.
TO : Division Surgeon, Hq., 1st US Inf. Div.
INTRODUCTION
For the purpose of this annual report it is deemed advisable to divide the year into two chronological periods and to close the report with pertinent remarks, impressions and conclusions reached as a result of the years work. D-Day of the European Invasion is the logical point to make this division in time. The few months prior to June 6, 1944 were devoted to orientation, `weeding out` and preparation for the attack. Since June 6 we have carried out in practice some of the theories developed during the first half of the year. As the position of the Division Psychiatrist is without precedent in this war, many new ideas and improvements on old theories have come about. There has been little opportunity to compare figures and results except thru reading of journals and reports from other theatres, most of which antedate the `realization` of the necessity for a psychiatrist at the division level. For this reason, remarks will be made as the situations were unique for this organization and for this doctor.
PRE-INVASION (Jan. 11 to June 6)
The year began with a month`s schooling at the ETO School of Military Psychiatry completed on 12 February 1944. Returning to the division, the first activity was one of orientating the medical and infantry officers as to the duties of a psychiatrist. This was accomplished (1) by informal talks to regimental medical officers discussing the subject, treatment of combat neuroses, and making tentative plans for the future. (2) by lectures to all infantry officers in the division. This was accomplished in a number of informal talks to groups which included particularly company grade and personnel officers. The outline of this lecture is reproduced below and is based on treatise on the subject of combat exhaustion by Major Fabing of the ETO School of Military Psychiatry. An attempt was made to translate the exhaustion in terms for the lay-officer`s consumption and to stress in addition the personnel aspects of other psychiatric conditions, and finally, the problem of reassignment. Officers were encouraged to send disciplinary problems to the psychiatrist especially chronic offenders. They were asked to write letters stating wherein the soldier was undesirable in the company. One feature in particular was stressed; namely, that all cases should be sent to the battalion surgeon for his advice and indorsement. We here have felt that all such cases should be kept in medical channels and that the psychiatrist should act as a consultant, and should never see cases referred directly.
OUTLINE OF LECTURE TO INFANTRY OFFICERS
I - TERM OF CHOICE
II - SIZE OF THE PROBLEM
III - CAUSE
a. Physical Condition of Soldier
(1) Illness
(2) Hunger
(3) Thirst
(4) Fear
2
b. Physical Status Tactical Situation.
(1) Retreat
(2) Being Pinned Down; Mortars, 88`s, Strafing.
(3) Temperature
(4) Prolonged Engagement
c. Psychological Factors.
Lick of confidence
d. Constitutional Makeup of Soldier
(1) Mental deficient
(2) Psychopath
(3) Alcoholic
(4) Chronic neurotic
`He doesn`t deserve the boat ride to the battle because he won`t be there long enough to be of any value to the outfit`.
IV - PREVENTION
(1) Leadership
(2) Adequate training
(3) Disciple
(4) Unit spirit
(5) Action
(6) Proper placing of personnel
(7) Early recognition of neuroses
V - PRODROMES
(1) Alteration in temperament of personality
(2) Tobacco and alcohol
(3) Emotional instability
(4) Discipline
(5) `Startle response`
(6) Efficiency
(7) Concentration
(8) Depression and guilt
(9) `Nerves`
(10) Sweating
(11) Diarrhea
(12) Urinary frequency
(13) Insomnia with battle and dreams
(14) Pains `all over`
(15) Weight loss
VI - CLINICAL TYPES
a. Reactive Depression
b. Terror State
(1) Panic
(2) Stupor
c. Anxiety State
d. Hysteria
(1) Amnesia
(2) Conversion
(3) Fugue
VII - TREATMENT
VIII - MEDICAL CONSIDERATIONS
The next job was that of liaison between the Station and General Hospitals which was carried out by personally contacting the psychiatrist at these various installations such as the 315th and 306th Station Hospitals and the 5th and 94th and the 28th General Hospitals. It was found that much reduplication was avoided by having verbal understandings and further, that time and hospital space was saved because a properly `worked-up patient` could be immediately disposed of by the ward doctors. Up to this time it was not unusual for a patient, who had been admitted for `reclassification`, to remain in the ward for two and three weeks. The ward officer was afraid to send him to the General Hospital without data from the soldier`s unit, and he knew as well that the soldier was not wanted in the organization, else he would not be a patient for `reclassification`. The problem was solved by having all such cases sent to the hospitals thru the psychiatrist who sent letters and data necessary. From then on cooperation was excellent and rarely did we find ourselves in disagreement on the disposition of a psychiatric case.
2
It is the custom here to have each candidate for General Courts-Martial examined by the psychiatrist. The examination includes an interview to determine soldier`s background and an attempt is made to correlate this with his Army record and to advise the reviewing authorities as to the soldier`s value to the service. A statement is made as to the man`s sanity at the time of the alleged complaint. When the offense is of a serious nature, another opinion is sought. Relationship with the Judge Advocate is quite informal and liaison is maintained by almost daily conference or conversation. In questions of borderline intelligence, the Kent Emergency Test or a Standard Scaled Information Test is employed. Now and then charges have been `dropped` and patient hospitalized for mental deficiency, alcoholism or sexual perversion etc. In such instances it was found that lay-officers had to be enlightened and reeducated before they were convinced that the men were not subjects for discipline. An attempt was made to explain the apparent dilemma of the homosexual in the Army, and the fact that homosexuals are `sick` men and not always bad soldiers.
During these first six months an attempt was made to get rid of all men who for any psychiatric reason would be unfit for combat or likely to break early therein. It seemed that with this type of patient, previous experience of three campaigns was helpful in deciding what men, regardless of physical aspect, would be worthless. It was not always possible to convince company officers who, like many medical officers, feel that as long as a man can stand, he makes an efficient soldier. Past experience had taught us what a soldier goes thru on the front and also that this infantry war is not one that allows of morons, psychopaths, alcoholics and neurotics. War, like football, has become a fast moving `game` of the individual. No more hand to hand combat, but rather long range precision instruments are the rule. Men work alone or in isolated groups and are no longer driven `over the top` like cattle. No longer can we say `anyone is good enough for the infantry`. In a word, we want smart soldiers. We avoid the mental deficient and the psychopaths because in this war they are hazards to themselves and the service, despite the fact that physical health is good and they are willing.
Having completed the orientation and `weeding out process`, we thought about the handling of `exhaustions` in the coming invasion. Medical officers at all levels were instructed to have an adequate supply of Sodium Amytal and to retain as many men (at each of the levels) as seemed reasonable. There again previous experience was our best teacher and we went into France with only one question - how much treatment can be done at the Clearing Company level
During the period January 11 to June 6, one hundred Psychiatric Examinations were conducted:
|
I General Courts-Martial |
44 |
|
II Miscellaneous |
19 |
|
III Reassignment to non-combatant duties |
|
|
(a) Homosexuality |
4 |
|
(b) C.P.S. Inadequate |
11 |
|
(c) Constitutional Psychopath |
3 |
|
(d) Chronic Alcoholism |
2 |
|
(e) Post Concussion Syndrome |
1 |
|
(f) Mental Deficiency |
5 |
|
(g) Psychoneurosis |
9 |
|
(h) Anxiety State |
7 |
|
(i ) Dementia Precox |
2 |
|
(j) Within same unit |
3 |
|
TOTAL |
100 |
All pertinent capers have been filed and are available on any of the cases in the above tabulation.
4
INVASION AND AFTER (June 6 to Dec 31)
For the first few days after D-Day the neuropsychitric casualties were negligible. The tactical situation did not allow of any specific or prolonged treatment of the few `exhaustions` admitted. It was immediately evident that only when the Clearing Company was in a stable situation for at least five days, would it be practical to retain patients at this level. Time and again we were near heavy artillery which made sedation impractical. It was customary to see each casualty, give assurance and then give grs IX of sodium Amytal and evacuate. With the establishment of the Caumont salient the situation did stabilize and we were able to keep some twenty to thirty soldiers for periods up to seven days. With the help of four enlisted men who were specially trained for the work, we observed these men to the end so that in a period of treatment we could (1) decide which of them could be returned to duty; (2) which would require more extensive treatment at the Exhaustion Center; (3) which of them were unfit for further combat duty. During the day the men were free to roam about and go to the movies each night. Sleep was assured with from IX to XV grs of sodium amytal each night. The men were interviewed individually and in groups and rations were available when any of them felt like eating. It seemed best to run a `demilitarized` rest center. Assistants were trained to report on the activities and attitudes of questionable personalities. All mail was censored by the psychiatrist without the knowledge of the correspondents. If, after 72 hours, the soldier did not improve, he was sent to the Exhaustion Center with specific recommendation as to treatment and prognosis. Initial differences of opinion with the officers of this Center were ironed out during the first week. It was not easy to convince inexperienced medical officers that many of the `anxieties` were not as good as they appeared, and too, that one must experience gun fire to understand startle reactions and also must have some idea of life `on the front` before he can intelligently judge which man can or cannot go back to full duty. Lacking this experience he must give weight to the advice of men who have. The `air cleared` and thereafter we worked very smoothly. The division psychiatrist attended disposition board meetings at the `Center` and suggestions were made.
One problem seemed unique in that we had a number of men who had completed three campaigns and were showing the effects of too much combat. These men had reached the `saturation point` of combat experience and were battle weary. It was thought best that these men should be reassigned after observation and treatment. The attitude of many was that such men were experienced and could not be spared. Then too, a high percentage of these `old timers` were non-commissioned officers, the very `core` of the fighting unit. We were accused of being over-sympathetic and the patients were thought to be `malingerers` and `cowards`. However, the problem solved itself and, like the man who has had a leg blown off, `opinion` could never bring it back. These men were evacuated and reassigned as was proper.
Direct evacuation to hospital or exhaustion center was the rule for the weeks from the August `breakthru` to the onset of the Aachen offensive in October and the Hurtgen Forest battle in November. The last two `affairs` gave us new highs in NP casualties. Up to ten men were held at the Clearing Company for an observation period of 48-72 hours. December gave us von Rundstedt`s offensive and an expected increase in NP casualties.
5
During the period June 6, to December 31, 1944, one-hundred and forty-eight Psychiatric Examinations were conducted.
|
I General Courts-Martial |
47 |
|
II Miscellaneous |
13 |
|
III Reassignment to non-combatant duties |
|
|
(a) Homosexuality |
1 |
|
(b) C.P.S. Inadequate |
11 |
|
(c) Constitutional Psychopath |
9 |
|
(d) Chronic Alcoholism |
5 |
|
(e) Mental Deficiency |
5 |
|
(f) Psychoneurosis |
11 |
|
(g) Anxiety State |
31 |
|
(h) Dementia Precox |
3 |
|
(i ) `Saturated` with combat |
22 |
|
TOTAL |
158 |
These cases for reassignment constitute a group of soldiers who required special interviews and who were sent to this office with specific information from their respective commanding officers and battalion surgeons. The group of 22 (i) are men admitted with mild or moderate anxiety. It was thought that special letters would be necessary to insure that they would not be sent back to duty. Many others of this type were evacuated with a simple note on the EM Tag, because their symptoms were so severe that corroboration did not seem necessary.
Table shows totals of all types casualties admitted to the Clearing Company from Division and attached troops.
| Month | NP | SICKNESS | B. I. | WOUNDS | TOTAL |
|
June | 157 | 1014 | 182 | 950 | 2303 |
|
July | 104 | 1280 | 200 | 501 | 2085 |
|
August | 131 | 1104 | 283 | 629 | 2147 |
|
September | 141 | 781 | 219 | 762 | 1903 |
|
October | 279 | 1113 | 394 | 995 | 2781 |
|
November | 650 | 2146 | 657 | 2707 | 6163 |
|
December | 188 | 1080 | 300 | 546 | 2114 |
|
TOTAL | 1650 | 8518 | 2235 | 7090 | 19496 |
|
Month |
% NP (Wounds & NP) |
|
June |
14 |
|
July |
17 |
|
August |
17 |
|
September |
15.5 |
|
October |
22 |
|
November |
19 |
|
December |
25 |
|
Overall % |
18.5 |
|
Month |
% NP (Total Casualties) |
|
June |
6.8 |
|
July |
4.9 |
|
August |
6.0 |
|
September |
7.5 |
|
October |
10.0 |
|
November |
10.5 |
|
December |
9.0 |
|
Overall % |
7.5 |
These wounds are the result of direct enemy action and do not include battle injuries or self inflicted wounds. A graph by day shows that NP casualties follow the curve of wounds with a 24 to 48 hour lag. In December the increase in percentage seems to be due to the snow and sub zero temperatures as evidenced by increase in sick rates and `trench foot`.
6
I IMPRESSION ON TYPE AND TREATMENT
In this division the large majority of NP casualties that filtered back to the Clearing Company were more anxiety states than physical exhaustions. This same majority was in need of more prolonged treatment than was or is practical at this level. Awareness on the part of battalion surgeons and company commanders effected a rotation of men to kitchen trains or to the Collecting Companies where there was relative quite. The soldiers who were necessarily sent to Clearing Company were accompanied with notes or suggestions as to prognosis and disposition. Cooperation was remarkable and at a high level. It can be said at this point that cooperation, from the divisional commander down to platoon leader, played a big part in the successful handling of the NP problem.
Hunger, thirst, exposure and the other physical hazards did not obtain as causes, but for the most part enemy artillery from tanks and heavy guns were the chief complaint of the anxiety patient. At Caumont, the factor of fixed and prolonged defensive fighting played a big part. The boys complained that they could not `strike back`. In the other three high casualty periods (Aachen, Hurtgen, and the December `breakthru`) continuous action of the heaviest type was the main factor. Men went for 8 to 10 days without sleep altho rations were usually available. Sleep loss together with forest fighting in which every foot of ground is contested and where in enemy artillery shells hit trees, and were in effect air bursts from which there was no escape. Appended to this report is a breakdown of 500 cases as to type.
II MALINGERING
Brief mention is made of malingers because we didn`t see any here. It is remarkable that so many infantry officers and some ranking medical officers still think that much of our psychiatric symptomatology is `put on`. With this in mind, we spent long hours with hundreds of patients before recommending disposition. We have yet to meet a liar. If you spend the time, you will eventually break down defenses and find that the soldier is worried about his own nervousness rather than afraid of the enemy. Borderline social and economic backgrounds were definite factors in the histories of men whom we judged unfit for further `front line` duty. None of these men were deliberately falsifying their complaints.
III ROTATION OF PERSONNEL
A word on `rotation` as it should apply to this division. Manx articles have been written on the advisability of rotating experienced men out of combat - so that others may be promoted, and the men rotated will have a needed change of environment. It matters little whether the rotation involves going home, tho where possible, this should be carried out. This rotation should be a reward and a promise of reward and should. be an established policy. Rotation was started but when we came into the ETO, `all bets were off `. Now, what happens when you take a half dollar away from a baby after she drinks the milk which you have paid her to drink She balls and screams blue murder. Soldiers feel the same, but the effects are translated into inefficiency and lower standard of morale which is not always discernible. They resent the promise that was not kept. It is poor personnel management. It would be better to have no policy than to have one and not carry it out. There are other results of this disregard for the fact that a soldier does get war-weary after months of combat with nothing in the future but more combat. Within 18 hours I have examined three men who are being tried for desertion. They were
7
two staff sergeants and one `buck` sergeant. They had been thru all our campaigning up to November 11, when they `took off`. One man had a Silver Star and Bronze Star from the African Campaign. All were recipients of at least one decoration. It is a sad commentary on our rotation system when three excellent soldiers have to `desert` to get away from action; when after four years of service with a unit they end up as privates and are being tried for such a serious breech of discipline. We can show many other examples of the detrimental effects of `over-doing` combat.
IV MORALE
Morale or fighting spirit, which Napoleon considered 75% of inning, has not been the subject of investigation, but it is quite evident that a majority of the men feel that they are in one of the finest of divisions. The record and publicity given to our exploits is readily available. The key officers are experienced. These with other factors explain the impression which men in and out of the division describe as `I don`t know what it is, but somehow the 1st can receive orders, get on the road, and obtain an objective with ease and a lack of confusion not seen in other outfits I have supported`. Nothing can inspire confidence like the knowledge that your outfit is the best in fact; that it is the senior fighting unit; that it has accomplished its missions with lows if not the lowest casualty rates.
A warning at this point: The feeling of superiority is beneficial, but can be a boomerang. Many men realize how well they have performed and that their outfit is and has been used to correct many critical situations. They have been told that they hold a number of `firsts` - in this war and the last, but no judicious soul has seen fit to come out and tell them that when the fighting is over they may be the first to go home. This one sided philosophy of `you do your job well and we`ll see to it that you are penalized` can strike back. Who can say it hasn`t Who can say that this or any division is 100% efficient however good it looks on the parade ground The boys realize that in Africa there was no one to relieve them; that in Sicily they acre the `keystone` division and put in that position for a purpose; that in Normandy, they were first to hit the beach. Their penetration of the beachhead was deepest. They took the first German city of any consequence. Does anyone think that they would be any less efficient if they were told that they`d be the first to go home They are, at least, entitled to hope!
It does not matter that other divisions have seen as much duty overseas or have had as many combat days as ours. We have fostered the `firstness` theory and if the attitude is to be maintained, the theory must be carried thru to a logical conclusion - home first!
The `bubble can burst` - for example: Of 200 NP cases admitted consecutively from November 23 (Hurtgen Forest) 62 (30%) were `old timers`. Of this 62, 34 were officers and noncoms, all with exemplary records. The breakdown was as follows of the 62 men with extensive combat experience.
|
T/Sgts |
5 |
|
S/Sgts |
11 |
|
Sgts |
8 |
|
Cpls` |
6 |
|
Officers |
4 |
|
Pvts |
28 |
|
TOTAL |
62 |
These men joined the division during or before the Tunisian Campaign.
In other words, by keeping these old men in `overtime` we are faced with the loss of the very heart of the organization, all at once. Rotation would have
8
allowed the change to progress slowly and would have made for greater efficiency in the long. Run.
V REINFORCEMENTS
Along the same lines is a consideration of the so-called reinforcement system. The change of name recently effected is well advised. The name `replacement` had become stigmatic and with good reason. If there is one outstanding morale breaker, it is the `system` by which men are picked out and sent to the front. The new man gets little if any preparation for actual combat; no indoctrination, as it were. The new man is shunted from pool to ship to cattle car to a strange unit, and, in all probability, will arrive on the active front, at three in the morning A case in point is that of a group of replacements (about 20) who arrived on the front some time after dark and never reached the company. They were lost, wounded or killed. What could be worse for reinforcement than arriving at his first assignment in the dark; being put to work by non-corns who have never seen him; not knowing the situation; bewildered and panicky before he`s had a chance to get his `feet on the ground`. This throws an additional strain on the squad and platoon leader. More than one sergeant has described the effect of these ill-prepared reinforcements. `These kids watch your every move. If you dig a foxhole, they dig one. If you open a C ration, they will. Wherever you go, their eyes follow. If you feel a bit nervous, you don`t show it, or you`ll lose every one of them. Some of these kids have never heard a gun. You have to place each of them and show many how to use the weapons. After a day or two of this, you`re `done`. When you see them die because they don`t know enough to duck, it gets you.`
Replacement pools are soulless `stopovers` where men returning to duty from hospitals are `passed off` as men for the infantry who can put up with the worst possible conditions. Soldiers will take a tough assignment on the `front` without a murmur, but they resent the neglect and impersonality of replacement pools for from the fighting. You can`t teach a man to be a tough or hard fighter by making him miserable. The worst criminals are given a good meal before they are sent to the chair. Why not a bit of kindness and consideration for the soldiers who are going out to fight and die for their country
VI MEN RETURNED TO FULL COMBAT DUTY
Of 100 consecutive cases observed and treated at this station or exhaustion center, twenty seven (27) are known to have returned to fill combat duty and remained as efficient soldiers. It is our opinion that this is a high average and that the all-over figures would show that not more than 15% of all men admitted here ever returned to full efficiency.
Of 100 consecutive cases admitted during the Hurtgen Forest Offensive, the records show:
|
Directly to duty |
4 |
|
Prognosis good |
10 |
|
Prognosis fair |
25 |
|
Prognosis poor |
57 |
|
Not NP |
4 |
|
Total |
100 |
96 of these men were evacuated for further treatment with prognosis as shown. We feel that the `fair` and `poor` group are, for practical purposes, through with combat. As no system of follow-up has been effected, this `impression` cannot be proven. We are inclined to doubt figures of 40% to 50% return to `duty`, if duty is defined as full combat efficiency. The apparent discrepancy
9
may be due to the prolonged combat, time away from home, `turnover` and consequent high replacement figures in this division. It is unfortunate that comparative percentages are not available; that there has been nothing in the way of liaison between division psychiatrist even in the same sectors; that a composite picture might be viewed by each of us.
JOSEPH J. BRADLEY,
Major, Med. Corps,
Div. Psychiatrist.
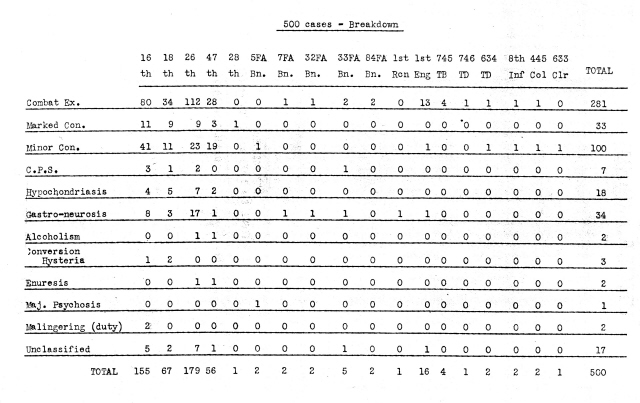
ANNEX
REPORT OF DIVISION DENTAL SURGEON
HEADQUARTERS 1ST US INFANTRY DIVISION
Office of the Division Surgeon
APO 1, U.S. Army
25 January 1945.
SUBJECT: Annual Dental Report for 1944.
TO : Division Surgeon, Hq., 1st US Inf. Div.
The beginning of the year found the division in England getting the well needed rest after the African and Sicilian Campaigns. All of our efforts were now directed toward getting the men in the division dentally fit for the invasion. Col Craven, 1st Army Dental Surgeon helped considerably into our area rolled the Mobile Prosthetic and Operative Clinics. These were fully manned and helped the division especially with prosthetics. Over 200 dentures were made. Our only regret was that they didn`t stay long enough for they were withdrawn on the 18 January 1944 to be sent to other divisions. Our own prosthetic clinic was set up in Dorchester which was approximately in the center of our area. All men needing prosthetic service would contact the laboratory and arrangements would be made by appointment to service these men. The laboratory in Cheltenham added greatly to the efficiency for they would process all cases that we were unable to do. By direct telephonic communication we were able to contact the laboratory and get some critical supplies such as teeth and precious metals. The division dentists concentrated on operative dentistry, getting the men ready for D-Day. At the prosthetic clinic an operative clinic was set up to take care of all prosthetic cases prior to impression taking. This clinic also served. the Special Troops that were located in Dorchester . During this pre-invasion period some of the dentist attended the regular monthly meetings in London. None of the officers attended any of the schools.
During the invasion period one dentist landed with regimental headquarters section and the other regimental dentist traveled with the collecting company. During the landing the dentists helped the battalion surgeons in treating casualties on the beach and at the regimenta1 aid stations. After the first twelve days the dentists were able to set up their #60 chests at the collecting companies. The regimental dentist worked out of his dental kit. Whenever the clearing company remained in one area for a period of three days or longer the #61 and #62 chests were set up in a pyramidal tent. After the breakthrough at St. Lo the dentists worked mainly out of their kits in the dash across France. After entering Belgium the dental service was very fortunate by getting a circus trailer which was converted into a Mobile Prosthetic Laboratory. The men in the division are able to receive this service now whenever the clearing company stays put, be it only for one day. The clinic is manned by Capt. Fleminberg and three technicians. He concentrates solely on prosthetics. One of the regimental dentists moves back to the clearing company during combat and acts as one of the platoon dentists.
2
This system works well since during combat only one of the regimental dentist is able to set up and he lives and works with the collecting company. The artillery and the engineers have their emergency dentistry done at their combat team dentist. For extensive dental service these units send their men buck to their own dentist who usually sets up with their headquarters or service sections. Capt. Weinstein was attached to division in September 1944 and he is the dentist for the 103rd (AW) AAA Bn. He visits his units which are attached to each artillery battalion. While in each area he also treats any dental cases in the artillery.
The supply situation has been good except for a few items which we were unable to obtain. At the division medical supply we have one chest, which is all dental. This chest usually has enough supplies for a thirty day reserve. Teeth for prosthetics and stone for pouring models were two of the tiers that were critical. We used captured enemy teeth supplies and plaster of Paris instead of stone. Captured enemy foot engines have been functioning in the division. Some engine of this nature should be part of at least two #60 chests in the division. Since the clearing company has generators as part of their T/E, electricity would be no problem. It is obvious that it would be much more efficient and pleasant with such an addition. Contra-angles is one piece of dental equipment that break in the field. It would be advisable that a supply of contra-angle gears be on hand at the medical supply and thus many of these could be serviced quickly. The equipment in the #60 chest is adequate. However, replacements for non-expendables are difficult to obtain. Scalers of all types are particularly the ones that need replacing.
During the year two of the dentist were promoted from Lt. to Capt. One of the dentists was wounded in action and did not return to the division. Another dentist received the Purple Heart but remained on duty. Two of the officers were evacuated for medical reasons and are now back in the States on limited duty.
The dentist of the division have been cited with two Purple Hearts, five Bronze Stars, one Soldiers Medal and a Unit Presidential Citation with a Cluster.
During the year 14,358 restorations were placed. There were 3, 334 extractions and 243 cases of Vincents. These cases were not proven Vincent cases since no smears were taken. However, they were counted as such since they received the Vincent treatment. The prosthetic clinic placed 19 dentures. This number included reconstructions, repairs and new dentures. There was one case of interest. For the first time in the last four years an obturator was made for a cleft palate case. Ordinarily this man would be lost to his unit as well as many other prosthetic patients. It is most advisable that each division has a self contained unit to take care of these cases.
My conclusions and observations would be the following:
(1) The prosthetic clinic should be mobile and a self contained unit. It should have its own T/O of one officer and three technicians with appropriate ratings. It should not have to rely on other units for electricity but should have its own generator.
3
(2) When the division is pulled out of the line it has been for short periods lasting for from eight to ten days. During this period the division dentists are swamped with operative dentistry. It would be advisable if there was a pool of dentists in Corps or Army reserve who could be sent into a centrally located area of the division during this period. They should have their own equipment and supplies and assistants. Many more men of the line would thus receive treatment. The likelihood of these men becoming a casualty during combat because of dental defects would be minimized.
(3) That provisions be made where dental officers could be rotated from field units to fixed installations, younger dental officers should be assigned to divisional units. Five dental officers have been with the division over four years and two have been with the division over two years. The morale of the dental personnel would be greatly increased if some form of rotation or promotion would be instituted.
(4) I have allays felt that division artillery should have a T/O of two dentists. If the men were all Class IV to begin with it may be possible for one man to treat a division artillery. However, many men need complete rehabilitation dentally and I feel it could take at least two dentists to treat the number of men that comprise the artillery.
MICHAEL KOWAL
Major, DC
Div. Dental Surgeon
SOURCE: National Archives and Records Administration, Record Group 112, Records of the US Army Surgeon General`s Office, World War II Records, 1st Infantry Division, Division Surgeon, 1944-1949, Box 388.
![]()