



AMEDD Corps History > U.S. Army Dental Corps > United States Army Dental Service in World War II
EARLY SHORTAGES OF DENTAL SUPPLIES
The critical shortage of dental equipment and supplies was probablythe most serious difficulty faced by the Dental Service during the first2 years of mobilization. There is ample evidence of the extent of thisshortage. The Committee to Study the Medical Department of the Army reported,about November 1942, that "there are serious deficiencies in certaincritical items of equipment and supplies. Dental officers ... have beenhandicapped by an appalling lack of certain materials and equipment."A survey of 199 Air Force stations in December 1942 revealed that only26 were without serious shortages which ranged from instruments to chairs,units, x-ray machines, and field chests,2 and the followingreports were typical of many received in the Dental Division during theearly part of the war:
The July (1941) Report of Dental Service from Camp Davis,N. C., reveals the fact that for some time construction of both DC-1 andDC-2 dental clinics has been completed, and that only four handpieces,all of which were borrowed from other stations, were available. This meansthat at this station, where twenty dental officers are on duty with thestation complement, the services of only four can he utilized in a professionalcapacity at one time. This situation has existed at Camp Davis for manymonths. . .3
The dental clinic No. 1 at Camp Livingston, La., has notbeen activated due to the lack of cabinets, sterilizers, handpieces, andlights. Requisition was made for these items in December 1940. (This reportwas made in October 1941.)
Overseas, where the shortages were further aggravated by delays andlosses in shipping and by difficulties of storage and distribution, thesituation was for a while even worse.4 The dental surgeon ofthe European Theater of Operations (ETO) reported in November 1942 that30 percent of the dental officers in England had no equipment.5In December 1942, 39 dental officers in the Middle East theater had a totalof 6 field sets, 2 units and chairs, 1 incomplete laboratory, and a fewmiscellaneous items purchased locally.6 In
1A general discussion of the organization andoperation of the medical supply service has been written under the title,"The Procurement and Distribution of Medical Supplies in the Zoneof the Interior during World War II," by Capt Richard E. Yates. Thischapter deals only with aspects of the supply problem which were of particularconcern to the Dental Service. HD.
2Memo, Col George R. Kennebeck for Brig Gen David N. W. Grant,11 Jan 43. SG : 444.4-1.
3Memo, Brig Gen Leigh C. Falrbank for Finance and Supply Div,SGO, 29 Aug 41. SG : 444.4-1 (Camp Davis)C. (At the time of this reportthere were about 15,000 men at Camp Davis.)
4Medical supplies for Europe waited in the channel for as longas four months while high priority munitions were being unloaded. SeeHistory of the Dental Division, Headquarters, ETOUSA, 1 Sep-31 Dec44. HD: 319.1-2 (ETO).
5Personal ltr, Col William D. White to Brig Gen Robert H. Mills,2 Nov 42. HD: 730.
6Personal knowledge of the author who was dental surgeon ofthe Middle East theater in December 1942.
166
December 1942 the North African theater was short 37 percent of itsauthorized MD Chests No. 60.7 8 In January 1943 the Directorof the Dental Division, SGO, stated: "We have no chests 60 at all,it seems, to issue to troops in this country."9
Serious deficiencies of supplies and equipment involved shortages ofthe following important items:
Burs. The War Production Board (WPB) reported in 1943 that stocksof dental burs in the hands of civilian dealers averaged only 33 percentof prewar levels, and that 88 percent of all dentists complained of difficultyin obtaining this essential item.10 Total output in 1943 wasestimated at 48 million while total requirements were placed at over 93million, of which 52 million were requested by the Armed Forces.11In spite of the fact that the Army was given only 15 million in 1943instead of the, 35 million requested, final allocations to the Armed Forcesstill totaled more than half of all production for the year.12As late as November 1944 WPB considered construction of a new bur factoryat Government expense, though the project was dropped when it became apparentthat low output was due more to the lack of materials and labor than toinadequate capacity.13
Heavy clinical equipment. Production of units, chairs, x-raymachines, and other large clinical items had naturally been small in peacetimesince they could be classed as capital goods which required replacementonly after many years of use. In 1940, civilian dentists purchased onlyabout 2,000 units and 2,500 chairs.14 In 1943, however, theArmy alone required about 5,500 units and 5,000 chairs.15 Theproduction of individual companies manufacturing these items was increasedfrom 50 to 300 percent16 but capacity was severely strained.In April 1943, delivery of 1,697 units, of 8,359 contracted, caused certainmanufacturers to be classed as "delinquent."17
Dental field chests. During the early part of the war many unitswere sent overseas without field dental equipment, or with chests whichwere incom-
7Ltr, Col Egbert W. V. Cowan to Chief Surg,NATOUSA, 13 Mar 43, sub: Dental needs in the Theater of Operations. Onfile as incl to pers ltr, Col William D. White to Brig Gen R. H. Mills,7 Apr 43. HD: 730.
8Personal ltr, Brig Gen R. H. Mills to Col. William D. White,18 Jan 43. HD:730.
9See this chapter, p. 180 for contents of M. D. Chest No. 60.
10Special problems discussed at War Service Committee meeting.J. Am. Dent. A. 31 : 445-450, 15 Mar 44.
11Memo, Col Clifford V. Morgan, Chief of Materials Br, ProductionDiv, SOS, for SG, 6 Jan 43, sub: Dental burs-production and requirements.SG: 444.4-1.
12Memo, Col F. R. Fenton, Resources and Production Div, SOS,for SG, 24 Feb 43, sub: Dental burs-proposed allotment. SG: 444.4-1.
13Ltr, Senator Harold Burton to Mr. Highland G. Batcheller,Vice Chairman of Operations, WPB, 10 Nov 44. SG: 444.4-1.
14Info, Medical and Health Supplies Section, Consumer ProgramsBranch, WPB, for Col C. F. Shook, 18 Sep 42. The original of this lettercannot be located. The source of the figures given was said to be the AmericanDental Trade Association.
15Ltr, Maj J. E. Rice to Chief, Reqmts Br, Resources and ProductionDiv, Hq, ASF, 5 Apr 43, sub: Allocation of dental operating units and chairs.SG: 444.4-1.
16Annual Report of the Army Medical Procurement Office, fiscal1944. HD: 319.1-2.
17Incl to memo, Lt Col C. G. Gruber for Chief, Health SuppliesSection, Production Div, ASF, 10 Jun 43, sub: Report on dental supplies.SG: 444.4-1.
167
plete in essential items.18 This particular deficiency wasone of the most critical encountered Since it was extremely difficult tomake any informal arrangement for obtaining dental care in the areas firstoccupied by American troops.
Handpieces. The production of handpieces, especially of the Contra-angletype, was such a specialized operation that expansion of facilities wasslow and for many months output lagged behind wartime needs. In many otherwisefully equipped clinics the dental officers could perform only the operationspossible with the simpler straight handpiece. At times, in early 1943,dental officers scattered over thousands of miles of desert in the MiddleEast theater had only a single contra-angle handpiece per dentist, andthere was not one replacement in the theater. These shortages resultedfrom a number of factors among which the following were most important:
1. The Armed Forces took nearly one-third of the Nation's active dentists.In addition to providing these men with complete outfits, adequate reservestocks had to be assembled for future operations as the loss of dentalsupplies was inevitably high under combat conditions. (The dental surgeonof the ETO reported that 40 complete field outfits were lost while in shipmentto his area.)19
2. The Supply Division, SGO, suffered from a lack of officers trainedin dental supply. The director of that division stated in September 1942that "The dental supply program has been materially retarded due toshortage of personnel capable of negotiating contracts for the MedicalDepartment."20 The Director of the Dental Division, SGO,noted that difficulties encountered had been "in part due to the inexperienceof supply personnel in evaluating dental needs and requirements."21
3. Requirements for lend-lease aggravated shortages in some of the mostcritical items. Late in 1942 when units were being shipped without theirdental field chests, the British Army was supplied with 200 of these scarceitems under previous commitments.22
4. In peace, the United States had depended to a considerable extenton imports of dental items from European countries. For instance, Americanindustry had produced only from 6023 to 70 percent of the 33million burs used each year prior to World War II. With the outbreak ofhostilities these imports were immediately cut off not only to the UnitedStates, but to its allies and to South and Central America.
18Personal ltr, Col William D. White to MajGen Robert H. Mills, 22 Oct 43. HD: 730.
19See footnote 4, p. 165.
203d ind, Assistant Chief of the Supply Div, SGO, 19 Sep 42,on Ltr, Lt Col James P. Holliers. SG: 444.4-1.
21Final Report for ASF, Logistics in World War II. HD: 319.1-2(Dental Division).
22Personal Ltr, Brig Gen R. H. Mills to Col William D. White,28 Nov 42. HD: 730 (ETO).
23President J. Ben Robinson discusses personnel and supply problemsarising out of the war. J. Am. Dent. A. 30: 163-166, 13 Jan 43.
168
5. High wartime wages swelled the demand of the civilian populationfor dental care which it had not received in the years of depression precedingWorld War II.
6. The threat of future shortages probably resulted in some hoardingof dental supplies. At a conference of dental manufacturers in September1942 the representative of one firm noted that his company alone was undercontract to provide 261,000 instruments for the Army, and he expresseddoubt that such a number was actually required.24 The Directorof the Dental Division immediately pointed out the elimination of manydental items from the supply lists of the Army, and claimed, in turn, thatthe Navy had ordered as many burs as the Army though it had only one-fourthas many dentists.25
In December 1942 a representative of the Supply Division, SGO, claimedthat large quantities of surplus burs were in the hands of the schools,supply houses, and the profession, and asked the Association of DentalManufacturers of America to attempt to collect these for military use.The Association issued a bulletin to its dealers asking that customersbe impressed with the need for turning in excess stocks as an alternativeto a complete "freeze" on sales to civilians, but this actionproduced more criticism than burs. The president of the ADA protested vigorously,both at the supposed threat of a "freeze" on civilian sales,and at the implication that civilian dentists were guilty of what was delicatelycalled "anticipatory buying."26 The Supply Division,SGO, replied that it had never intended to hint that hoarding had occurred,and that its action had really been expected to impress the manufacturerswith the need for intensive efforts to increase production.27In any event, the attempt to collect burs from civilian sources producedonly about 2,100 packages, and the effort was soon dropped.28
It is difficult to deny, however, that hoarding of scarce supplies waspracticed both by civilian and military users. The chairman of the MedicalSupplies Commission, Army and Navy Munitions Board, reported that civilianpurchases of burs in 1941 had been 70 percent higher than in any previousyear, in spite of the number of dentists and patients in the Armed Forces.29In 1943 total requirements for burs were placed at nearly 94 million, comparedwith an average prewar demand for about 33 million burs. The Army, alone,asked for over 35 million burs in that year, or more than the normal totalpeacetime requirement, and combined requests of the Armed Forces totaled52 million burs.30 The clashes reported above, between the Army,Navy, civilian practi-
24Memo, Col C. F. Shook for Col F. C. Tyng,3 Sep 42. HD: 444.4-1 (Dental).
252d ind, Dir. Dental Div, to Memo cited in footnote 24, 16Sep 42. HD: 444.4-1 (Dental).
26(1) Ltr, Dr. J. Ben Robinson to Col F. C. Tyng, 29 Dec 42.SG: 444.4-1. (2) See footnote 23, p. 167.
27Ltr, Col F. C. Tyng to Dr. J. Ben Robinson, 10 Jan 43. SG:444.4-1.
28Ltr, Dental Manufacturers of America to Col F. C. Tyng, 29Jan 43. SG: 444.4-1.
29Ltr, Lt Col C. F. Shook to Hon Leslie C. Arends, 23 Jan 42.9G: 444.4-1.
30Info memo, Safety and Technical Equipment Division, HealthSupplies Committee, WPB, 5 Jan 43. SG: 444.4-1.
169
tioners, and the manufacturers, are significant mainly because theyshow that users tend to overestimate their needs when supplies are uncertain,and because they indicate the need for disinterested control of distributionwhen production is inadequate to meet all demands.
In the final analysis, wartime shortage of dental supplies was due primarilyto increased demand rather than to defects in production. In spite of thedifficulties noted in obtaining labor and materials, the output of dentalitems soon exceeded peacetime rates. The manufacture of burs, for instance,tripled between 1937 and 1944.31 A representative, of The SurgeonGeneral stated that wartime production of dental supplies reached 3 1/2times normal peacetime levels.32 It is apparent that in timeof war the production of dental supplies for civilian needs can be reducedvery little if at all, and that any reduction in the output for civilianswill be more than balanced by the increased demands of the Armed Forces.
ACTION TAKEN TO IMPROVE THE DENTAL SUPPLY SITUATION
Improvement in the dental supply situation depended mainly on an increasein civilian production, and this phase of the problem was largely out ofthe hands of the Dental Division. The latter did cooperate, however, ina number of steps to assure the most effective use of the available stocksand raw materials, of which the following were the most important:
Simplification of Dental Items
Early in the war the Armed Forces, governmental agencies, manufacturers,and the civilian profession cooperated to reduce the number of types, andto simplify the design, of many items produced for dental use. As earlyas February 1942 the Dental Division had voluntarily suggested that forthe duration of the war 81 items, including 33 sizes of burs, be droppedfrom Army supply tables. A total of 134 items were eventually recommendedto be dropped, and most were actually removed from the tables. The requisitionof nonstandard items was also discouraged.33
In June 1942 WPB issued a "general limitation order" restrictingthe production of dental burs to 42 of the most used sizes.34In November 1942 delegates from the Armed Forces, the ADA, the AmericanDental Trade Association, and WPB, agreed on methods for simplifying otherdental items, particularly chairs and units.35 Wood and plasticswere to be substituted for metals
31See footnote 10, p. 166.
32Testimony, Maj Gen George F. Lull before the Senate Subcommitteeon Wartime Health and Education. In Hearings before a Subcommitteeof the Committee on Education and Labor, United States Senate, Seventy-eighthCongress. Washington, Government Printing Office, 1944, pt 5, p. 1672.
33SG Ltr 2, 8 Jan 42.
34WPB General Limitation Order 139, Schedule 1, pt 1254. InFederal Register, 26 Jun 42.
35Memo, Col C. F. Shook for Col F. C. Tyng, 26 Nov 42, sub:Dental Equipment Advisory Committee for the WPB. SG: 334.8-1.
170
wherever possible, and the production of units was to be limited tothe smaller, simpler types similar to the Ritter "Tri-dent."These units provided only the basic essentials: a dental engine, cuspidor,bracket table, warm water syringe, hot and cold compressed air, and operatinglight. The amount of brass and copper used was to be drastically reduced.
With the aid of a committee appointed by the ADA, and with the adviceof all interested parties, the Bureau of Standards also drew up "simplifiedpractice recommendations" aimed at eliminating minor and nonessentialvariations of standard articles. Steps recommended by this agency, suchas the reduction in the number of sizes and types of hypodermic needlesproduced, were generally accepted voluntarily by manufacturers, thoughhad they not it would have been possible to enforce them through WPB'scontrol over the allocation of materials.
Improved Distribution of Dental Supplies
In the early part of the war supply officers with experience in handlingdental items were scarce, resulting in occasional poor distribution ofeven the minimum stocks then available. An especially frequent defect wasfailure to balance the equipment sent to each station; one post might receiveall its units and no chairs, while another received all its chairs andno units. Angle handpieces were furnished which did not fit the particularstraight handpieces issued. To improve this situation the Director of theDental Division recommended in March 1941 that a dental officer be assignedto the Supply Division, SGO.36 Such an assignment was actuallymade in November 1942, but it was terminated in March 1943. Subsequentimprovements in the allocation of dental supplies resulted mainly fromthe increasing experience of medical supply officers.
In July 1941 The Surgeon General directed that stations with excessstocks of dental items would report them for redistribution where moreurgently needed.37 Stations were also directed to turn in anyhandpieces in excess of one per operator, plus a 25 percent station reserve.38
In January 1943 WPB issued a general limitation order controlling theproduction and sale of dental units, chairs, x-ray machines, and sterilizers,39and governmental agencies were thereafter given first priority in the purchaseof such items. Stocks of new equipment already in the hands of jobbersand dealers had to be reported, and 54 chairs and 109 units were obtainedfor the Army from this source.40
The storage and issue of porcelain teeth, involving hundreds of molds,sizes, and shades, offered considerable difficulty in most supply depots.In
36Memo, Brig Gen Leigh C. Fairbank for SupplyDiv, SGO, 17 Mar 41. SG: 210.31.
37SG Ltr 75, 25 Jul 41.
38SG Ltr 83, 25 Aug 41.
39WPB General Limitation Order L-249, pt 3172, 20 Jan 43. InFederal Register, 21 Jan 43.
40Ltr, Maj Robert E. Hammersberg to Purchase Div, Army MedicalProcurement Office, 26 Feb 43. SG: 444.4-1.
171
March 1944 each base medical depot was authorized two dental prostheticclerks who were qualified to handle artificial teeth.41 42 InEngland, teeth were first stocked in 18 separate depots for conveniencein distribution, but without skilled personnel the supply soon became badlymixed. Also, since each depot could keep only a small stock, the supplyof any individual mold might run out quickly, necessitating a canvas ofother depots to locate additional quantities. To eliminate these difficultiesa single depot was finally designated to handle all porcelain teeth, andan expert was brought from the United States to supervise their distribution.
It has already been noted that in the early part of the war units we'reshipped overseas without their authorized dental field chests. This situationwas due primarily to the serious shortage, of this item, but it was aggravatedby the policy of shipping personnel and equipment on different transports,in the mistaken belief that if the equipment failed to arrive promptlythe dentists could readily draw new chests from theater supplies. Thisdifficulty had been encountered in the First World War, and a dental officerwas finally assigned to the New York Port of Embarkation with specificinstructions to make sure that no dentist left the United States withouthis dental equipment.43 Similar action was taken in November194244 but improvement in this situation was slow until overseasdepots were finally stocked with dental field outfits which could be issuedpromptly on arrival. The difficulties encountered in both World Wars indicatethat every effort should be made to have dental equip-ment accompany dentalofficers as part of their personal baggage.
Purchase of Used Equipment
During the period when supply shortages were most acute The SurgeonGeneral was deluged with proposals that he purchase used dental equipmentfor Army clinics. In particular, large numbers of dental officers who werepaying for items lying idle in storage, and who noted the scarcity of thesesame items at the stations where they reported for duty, urged that the,Army solve both problems by purchasing or leasing such equipment. Widowsof dentists, and finance companies, were also eager to unload dental outfitsfor which the market was poor at a time when dentists were entering themilitary service in large numbers. Late in 1942 WPB made a preliminaryinvestigation which indicated that some 11,000 each, chairs and units,could be obtained from dentists entering the Army or Navy; and on the basisof this information it even recommended, for a while, a complete suspensionof the manufacture of the
41For training given enlisted men to qualifythem as prosthetic supply clerks, see ch IV, p. 158.
42T/O & E 8-187, C 1, 24 Mar 44.
43The Medical Department of the United States Army in the WorldWar. Washington, Government Printing Office, 1928, vol III, p. 624 (citedhereafter as The Medical Department . . . in the World War.)
44See footnote 22, p. 167.
172
larger dental items during the war.45 In January 1943 ASFalso urged all its agencies to make maximum use of secondhand equipment.46
Superficially, the proposal to purchase the equipment of dentists enteringthe service appeared to have considerable merit. The attitude of The SurgeonGeneral, however, was one of caution, typically expressed by Brig. Gen.C. C. Hillman, assistant to The Surgeon General, in September 1942:
It appears to this office that medical and surgical suppliesnow in the possession of civilian physicians might better be used to continuethe care of the civilian population than to be acquired for the Army. Formilitary use a certain degree of standardization is essential. You canwell imagine the difficulties that the Medical Supply Division would encounterif they attempted to gather up generally supplies and instruments fromcivilian physicians and with them supply our military hospitals.47
A later statement by Col. C. F. Shook was even more specific:
It is possible that dental units may be acquired in thismanner, but the number is questionable. The plan is an Utopian plan, butit would require more personnel than The Surgeon General's Office has atits disposal, and in many instances [it] would rob professional schoolsand recent graduates of the equipment they need in their profession.48
Under pressure of the great need for dental equipment, however, TheSurgeon General did make an effort, beginning in the fall of 1942, to acquiresecondhand items. In October 1942 he reported that where suitable usedequipment was found it was being purchased,49 though such procurementwas certainly on a small scale, apparently by local supply officers.50On 30 October 1942 questionnaires were sent to 3,000 new dental officers,asking if they owned suitable equipment, and if they would sell it to theArmy at a suggested price of original cost, less 5 percent for each yearof use. (Instruments were not to cost over 80 percent of original price.)51Of the 3,000 officers questioned, only 496 were willing to sell any equipment.Of this latter number, only 184 had items which the Army considered suitable.The remaining equipment was old, was manufactured by firms which had goneout of business, or was otherwise undesirable. It appeared that men withmodern outfits were not anxious to sell. The equipment offered was alsoscattered over 41 states, so that a con-
45Ltr, WPB to Col C. F. Shook, 18 Sep 42. SG:444.4-1.
46Memo, Maj Gen Lucius D. Clay for Chiefs of Supply Services,SOS, 25 Jan 43, sub: Used equipment and supplies in the hands of jobbers,dealers, and users. SG: 400.139-1 (St. Louis Medical Procurement District)M.
47Ltr, Brig Gen C. C. Hillman to editor, Journal of the AmericanMedical Association, 7 Sep 42. SG: 400.139-1.
482d ind, Col C. F. Shook, on ltr 16 Sep 42, to SG from thesurgeon, Camp Adair, Oregon, 1 Oct 42. SG: 440.1 (Camp Adair) C.
49Ltr, Col C. F. Shook to Mrs. Edna Francis, 29 Oct 42. SG:400.139-1.
50Formal authority to purchase used dental equipment withoutthe usual advertising for bids was not granted until January 1943. SeeLtr, Col M. E. Griffin to CO, New York Medical Department ProcurementDistrict, 21 Jan 43, sub: Purchase of second-hand dental equipment fromdentists in the Army. SG: 400.139-1 (St. Louis Medical Department ProcurementDistrict) M. This requirement appears to have been ignored by local purchasingagents, however.
51Ltr, SG to all newly commissioned officers, 30 Oct 42, sub:Acquirement of dental equipment. SG: 444.4-1.
173
siderable administrative organization would have been required to inspectit and advise on acceptance or rejection.
In spite of these unfavorable developments The Surgeon General directedmedical depots, on 12 February 1943, to purchase used items when such actionseemed justified by sound business judgment.52 Results werepoor, however, and in April 1943 The Surgeon General reported that theamount of equipment being obtained did not justify further expenditureof time by military personnel. He stated further that the replies to hisquestionnaire were being turned over to WPB for use in its program of procurementfor civilian needs. WPB9 in turn, followed up 100 offers as a test, andquickly decided to abandon the whole project, leaving the purchase andresale of used equipment to established dealers.53 The Army-NavyMedical Procurement Office reported that only 45 used chairs and 25 unitswere purchased by medical depots in 1943, and all of these were obtainedfrom dealers.54 It is probable that a few second-hand outfitswere purchased locally, by medical supply officers of camps or hospitals,but the number was certainly small, and played a very minor part in meetingtotal requirements. By September 1943 all prospective sellers were beingreferred to civilian agencies.
WPB sponsored a voluntary collection of instruments, as a test, in thevicinity of St. Louis in October 1942, but the drive netted more scrapthan useable supplies.55
Some of the causes for failure of the used equipment program were thefollowing:
1. Dental officers were reluctant to sell equipment without ironcladguarantees that they would be able to purchase the same or correspondingitems at the end of the war. However, World War I experience had shownthat excess dental items had not been available for sale until 2 yearsafter demobilization and the Army was therefore in no position to giveprospective sellers the assurance they required.
2. Much of the newer equipment offered was encumbered with liens whichso complicated purchase that the Legal Division, SGO, advised against anyattempt to procure such items.56
3. The attempt to use miscellaneous types of secondhand equipment involvedserious problems of maintenance. Isolated posts could not convenientlyobtain the parts needed for the repair of older items which might breakdown in use.
52Ltr, SG to COs of all medical depots, 12Feb 43, sub: Procurement by depots-purchase used equipment. HD: 314 (CodeR-3).
53See footnote 30, p. 168.
541st ind, Col. M. E. Griffin, 3 Jun 46, on ltr, Brig Gen ThomasL. Smith to Army-Navy Medical Procurement Office, 24 May 46, sub: Purchaseof dental units and chairs. SG: 444.4-1.
55Ltr, CO, St. Louis Medical Procurement District, to SG, 23Oct 42. SG: 400.139-1 (St. Louis Medical Procurement District) M.
56Memo, Legal Div, SGO, for Col C. F. Shook, 1 Feb 43, sub:Purchase from Army officer of secondhand dental chairs and equipment subjectto liens. SG: 400.139-1.
174
4. Inspection of items offered for sale involved long trips by dentalofficers, and only a small proportion of the outfits offered proved suitablefor purchase.
5. Used equipment was actually more expensive to the Government thannow. One officer inspecting an outfit in New York reported that the pricewas reasonable by retail standards, but that the old chair would cost morethan the Army regularly paid for a new one, and that the small unit wouldcost more than the quantity price for a new senior unit.57 Equipmentwas often offered to the Army only because it was hoped that an even betterprice would be obtained than in what soon became an inflated civilian market.Also, the depots could not issue used items until they had been reconditioned,and such reconditioning, with transportation charges, often cost almostas much as new equipment.58
6. With the productive capacity of manufacturers strained to the limitto meet military needs it was felt that the purchase of used equipmentby the Army would result in a critical shortage of items urgently neededby civilian dentists. It was believed, further, that the sale, maintenance,and repair of miscellaneous used equipment could better be handled by establisheddealers than by the Armed Forces, and that such nonstandard items werebetter suited to civilian needs, especially after the WPB stopped productionof new equipment for civilian use in January 1943.
The easing of the supply situation in 1943 permitted the Medical Departmentto withdraw from a program which had originally been undertaken, as anemergency measure, with strong misgivings.
Local Procurement of Dental Supplies
World War I attempts to obtain dental supplies by local purchase hadnot been encouraging. The American Expeditionary Forces contracted forsome French equipment in 1918, but the French Government was soon forcedto limit sales to items totaling not over 1,000 francs per month to preventa threatened exhaustion of the civilian market. A considerable amount oflaboratory supplies was then purchased in London, but the British War Officequickly prohibited further procurement from that source.59 Itwas apparent that local markets, geared to peacetime needs, could not furnishany significant proportion of the supplies needed by a major force.
In World War II medical supply officers in the Zone of Interior wereauthorized to make emergency purchases of small items not obtainable frommedical supply depots, and this privilege was sometimes extended to includedental units or chairs. The amount of material obtained by such means wasnot an important factor in the overall supply situation in the United States.
57Ltr, Lt Col H. T. Marshall to SG, 14 Jan43, sub: Purchase of secondhand dental equipment. SG: 400.139-1.
58Ltr, Brig Gen R. H. Mills to Dr. McCarthy, 29 Sep 42. SG:444.4-1.
59The Medical Department...in the World War (1927), vol II,p. 115.
175
In overseas areas local purchase was restricted only by the need andby the availability of stocks, and local procurement played a more importantpart in supplying equipment required to establish initial dental installations.Cabinets, lathes, cuspidors, and angle handpieces were obtained in Australia;burs, porcelain teeth, and acrylic resin in Palestine, and general dentalsupplies through reverse lend-lease in England. The Chief Surgeon of theEuropean theater claimed that all the dental burs needed by the UnitedStates forces in England in 1944 could be obtained through local purchase.60The British Army also loaned field chests to the United States Army unitsarriving in the Middle East without dental equipment in 1942 and 1943.Supplies procured abroad were important at a time when equipment was notplentiful, but in general they did not go far to meet the total needs ofthe United States forces overseas. Production in the less industrializednations was often negligible, and stocks on hand were quickly reduced toa point where civilian dental care was threatened. In Cairo, for instance,a single representative of a United States aircraft plant practically cleanedthe shelves of the few dental supply houses, and acrylic resin disappearedinto the black market for the remainder of the war, where it sold for approximately$20 a unit.61 Except in those rare instances where a highlyindustrialized nation could assume full responsibility for supplying oneor more items, local procurement was little more than an expensive andineffective measure to meet emergency needs pending arrival of standardArmy supplies.
Measures to Insure the Maximum Use of Available Items
In April 1942 Brigadier General Huebner, AGF inspector for training,reported that large numbers of men in the field were unable to chew theArmy ration because of dental defects.62 Since deficienciesin dental treatment at that time were due mainly to lack of supplies, theDirector of the Dental Division, SGO, was forced to take radical actionto insure full use of the limited equipment then available. He recommendedthat outfits in critical locations, especially in replacement trainingcenters, be used for from 15 to 24 hours a day, by the employment of 2or 3 shifts of dental officers.63 It is not known exactly howmany dental officers were used on night shifts during this. period, but916 additional dentists were requested at the time the system was initiated,and it is believed that most of this number were so used, at least temporarily.The use of double shifts could only be regarded as an emergency measure,however. The output of dental officers at night was less than during daylighthours, the proportion of broken appointments was nearly doubled,64and patients were
60Cable, Brig Gen Hawley to SG, 26 Oct 43.SG: 444.4-1.
61See footnote 6, p. 165.
62Memo, Dir, Mil Pers, SOS, for SG, 27 Apr 42, sub: Dental suppliesin the field. SPGAP/10282-14 (G-1).
63Memo, Brig Gen R. H. Mills for Exec Off, SGO, 27 Apr 42. SG:703.1.
64Annual Report of the Medical Service, Camp Claiborne, La.,1944. HD: 319.1.
176
tired and hard to handle after a full day's work. It was also difficultto arrange meals and transportation for both dentists and patients at irregularhours. The operation of multiple shifts did accomplish its primary purpose,which was to increase the total amount of work completed in the face ofa crippling shortage of supplies.
In the field the contents of a single M. D. Chest No. 60 were oftendivided so that two officers could utilize one set of equipment. One officermight devote his time to operative procedures while the other handled extractions,gingival diseases, and emergencies. The multiple shift system was alsoused to a limited degree in some theaters until adequate supplies arrived.65
Conservation of Scarce Supplies
Every effort was made to conserve critical items during the war. AfterDecember 1942, dull burs were saved and returned to depots for resharpeningunder contracts with civilian firms.66 Wax was collected, sterilized,and reused in the larger laboratories, and scrap amalgam returned to depotsfor recovery of the mercury and silver content. Items of rubber, brass,lead, tin, or other scarce materials were saved for salvage.
In 1942 about 180 enlisted men were sent to dental manufacturing plantsfor intensive 2-week courses in the maintenance and minor repair of dentalequipment.67
In September 1944 The Surgeon General published a technical manual coveringthe care, lubrication, and repair of dental handpieces.68
The repair of unserviceable handpieces was undertaken on a large scale.At first it was anticipated that manufacturers would assume responsibilityfor the reconstruction of their products, but they proved reluctant touse their overburdened facilities for this purpose and the medical supplyservice had to take over the program. Two shops equipped to rebuild handpieces,were established in the United States in 1944 but shortages of equipmentand personnel hampered early operations so that only 3,500 handpieces werereturned to service that year. By early 1945, however, most of the previousdifficulties had been overcome and in February these shops together reconstructeda total of 2,500 handpieces. Since only about 700 handpieces were receivedfor repair each month this capacity permitted a rapid reduction of thelarge backlog of defective handpieces which had accumulated over the pastmonths.69
65In the Middle East theater and in England,RAF dentists sometimes used their outfits in the mornings and early afternoons,lending them during the late afternoons and evenings to U. S. Army AirForce dentists stationed nearby.
66SG Ltr 176, 8 Dec 42.
67Report of the Dental Division, SGO, for fiscal 1942. HD: 319.1-2.
68TM 8-638, 23 Sep 44.
69The problem of the repair of dental handpieces. Bulletin ofthe U. S. Army Medical Department, 89: 25 June 1945.
177
Substitution of Critical Items
The Army, like the civilian profession, made wide use of substitutesfor critical items of dental supply. Acrylic resin was substituted forvulcanite, though this inevitable change was only hastened by the shortageof rubber. The alginates were used in impression materials in place ofscarce agar compounds. Various substitutes for tinfoil were evolved. Anattempt to use silver in place of nickel for plating instruments was unsuccessful,however, as the coating tended to pit and was subject to attack by mercuryparticles. Very early in the war diamond points were made available, toconserve dental burs. Items of copper were almost eliminated from dentalsupply tables. In general, no item made of critical materials was purchasedfor the Dental Service unless diligent research failed to reveal any acceptablesubstitute.
PACKING AND SHIPPING DENTAL SUPPLIES
General principles for the packing and shipping of dental supplies wereno different from those for other items, and the handling of dental materialoffered few unique problems. Early in the war considerable breakage ofheavy equipment, especially of dental x-ray machines, was reported, butthis situation was remedied as the depots gained experience in preparingmedical items for shipment under wartime conditions.70 The handlingof gold offered some difficulties. It was found that unless such materielwas placed in the custody of a responsible ship's officer, to be deliveredonly to an authorized agent on arrival, it was often "misplaced"either en route or at the docks were it was unloaded.71
EFFECTS OF CLIMATE ON DENTAL SUPPLIES
Considering the wide variations of climate encountered by the UnitedStates troops it is surprising that complaints of damage from extremesof temperature were relatively few. Cements, especially the silicate cements,set so rapidly in the hotter areas that their manipulation offered somedifficulty; when the humidity was high it was impossible to cool glass,slabs to the desired 70 degrees without precipitation of moisture. In thetropics the softer brands of waxes and impression compounds proved unsatisfactory,but materials specifically designed for use in such areas gave no trouble.Anesthetic solutions and x-ray film deteriorated rapidly when they couldnot be stored in cool locations, necessitating care to use oldest stocksfirst and to avoid accumu-lating quantities which could not be utilizedin a reasonable time.72 Small
70For additional data on packing problems seeannual reports of the Supply Division, SGO, for fiscal years 1943 and 1944.HD: 319.1-2.
71Personal Ltr, Dental Surgeon of the China-Burma-India theater,to Maj Gen R. H. Mills, 1 Jul 44. This letter has been seen by the authorbut it was not made a permanent record.
72See Essential Technical Medical Data Reports for China-Burma-Indiatheater, 1943 and 1944. HD: 350.05.
178
carpules (ampules) of anesthetic solution were reported to be undamagedby freezing in the Arctic, though later investigations indicated that therubber plugs sealing such carpules might be pushed out by exposure to extremecold.73 In general, standard items on the supply tables provedsatisfactory under any conditions where dental treatment was practicable.
ZONE OF INTERIOR AND COMMUNICATIONS ZONE EQUIPMENT
Prior to World War I it was planned that in a mobilization only portableequipment would be issued to dental officers, in the Zone of Interior aswell as overseas. By the fall of 1917, however, it was apparent that thispolicy was not economical because dental officers could not operate aseffectively with equipment which had been designed primarily for portabilityas with the more convenient chairs and units used routinely in civilianoffices. Standard chairs, wall-bracket engines, cabinets, instruments,and laboratory equipment were therefore issued to all Zone of Interiortraining camps and to base and general hospitals (fig. 4).74Teams of 10 dentists, with base equipment, were also organized for usein favorable locations overseas.
Prior to World War II it was recognized that field units would requireoutfits which were easily portable and could be used well forward in thecombat zone; on the other hand, it was clear that dentists outside thecombat area should not be required to use equipment designed to be setup in a tent or dugout. It was therefore planned to provide standard baseitems in the Zone of Interior and in fixed and semifixed installationsin the communications zone. (For establishments in that zone, it was expectedthat minor modifications, such as substitution of a mobile engine and cuspidorfor the dental unit, could be effective.) This policy was actually carriedout in the Zone of Interior, where dentists generally worked with equipmentsimilar to that in their own offices. Zone of Interior camps and hospitalshad units, chairs, cabinets, operating lights, x-ray machines, air compressors,and instruments which met normal civilian standards for convenience andreliability.75 In the summer of 1942, however, lack of shippingspace became so acute that drastic restrictions were placed on equipmentfor overseas use.76 The large hospitals and dispensaries ofthe communications zone were thereafter allowed only the dental field chests,augmented with essential laboratory and surgical tools and equipment77though many installations were later able to obtain captured base outfitsor to purchase chairs and engines locally.
73Ltr, Dr. J. Edward Gilda to Maj Ernest Fedor,21 Jul 47. This letter was seen by the author but not entered in permanentfiles.
74See footnote 43, p. 171.
75U. S. Army Medical Department Supply Catalog, 1942.
76Personal Ltr, Brig Gen R. H. Mills to Lt Col Richard F. Thompson,18 Jul 42. HD: 730.
77Memo, Brig Gen R. H. Mills for chm, Medical Department Supplyand Equipment Board, SGO, 25 Sep 43. SG: 444.4-1.
179

Figure 4. Zone of Interior dental Equipment.
The primitive character of the communications zone equipment was soon the target of much unfavorable comment. The Chief Surgeon of the European Theater asked that hospitals and general dispensaries in his area be given at least a minimum of base equipment.78 Another senior medical officer, returning from an overseas inspection trip in November 1943, reported that "Field observations and the opinions of qualified dental officers in the Southwest Pacific Area indicate the need for revision of equipment lists for fixed installations to provide electric engines (portable), wall-bracket operating lamps, and portable cuspidors, small type. It is recommended that the Dental Division be consulted with reference to this matter."79 The Dental Division had already requested reconsideration of the restricting order in September 1943, but the recommendation had been disapproved. A new request for authority to ship mobile dental engines, operating lights, and cuspidors overseas was now made, and this time approval was granted.80 Until then the
78Ltr, Capt F. J. Reynolds, Overseas supplyDiv, NYPOE, to SG, 2 Nov 42, sub: Dental equipment. SG: 444.4-1.
79Report of Col William Wilson on inspection trip to the SouthwestPacific theater. Quoted in: Memorandum to the chairman, Medical DepartmentSupply and Equipment Board from Maj Gen R. H. Mills, 2 Nov 43. SG: 444.4-1.
80Ltr, Capt M. H. Kannal to Overseas Supply Officer, NYPOE,13 Nov 43, sub: Dental equipment. SG: 444.4-1.
180
small amount of base equipment which had arrived overseas before enforcementof the embargo, or which had been obtained locally, had been spread verythin, over a few important installations. Fixed and semifixed units nowbegan to receive items which materially increased their efficiency andoutput.
DENTAL FIELD EQUIPMENT
Dental Operating Chests
The basic dental field equipment issued in the First World War was bulkyand difficult to transport. It was packed in six chests, containing anengine, a chair, a desk, instruments (two chests), and miscellaneous supplies.81A seventh chest containing a cuspidor was added in September 1917.82For overseas use another five chests were added, containing an oil stove,a portable table, a box of medicines, alcohol, and additional supplies.As delivered in France the complete outfit occupied 39.28 cubic feet ofspace and weighed 775 pounds.83 Transportation of this "portable,"equipment was always a problem, and not infrequently the entire outfithad to be abandoned in a hurried move.84
In the period between World Wars I and II the dental field equipmentwas considerably simplified. The Medical Supply Catalog of 1928 listedthree chests, occupying 8.7 cubic feet, and weighing 209 pounds.85The chests contained a foot-engine, chair, and instruments and supplies.Development of a dental field outfit which could be packed in a single,standard, Medical Department chest had been going on at the same time,however, and this same 1928 catalog listed, for the first time, the newM. D. Chest No. 60, which was essentially the item used during World WarII. (Figs. 5 and 6.)
The M. D. Chest No. 60 occupied 5 cubic feet, and weighed from 157 to187 pounds, depending upon variations in the constituent items.86Total cost was approximately $305. This chest contained a wood, aluminum,or steel folding chair, a foot-engine, an alcohol sterilizer, and routineoperative and surgical instruments and supplies to a total of about 160different items. It contained no prosthetic equipment as such supplieswere packed in other chests not available to the smaller units. Issuedto the dental officers of each tactical command allocated dental facilities,it provided the minimum equipment
81Manual for the Medical Department, 1916,Washington, Government Printing Office, 1916 (cited hereafter as Manual... Medical Department).
82Manual ... Medical Department, C dated 29 Sep 17.
83See footnote 43, p. 171.
84The Annual Report of The Surgeon General for 1919 states that"The transportation of dental equipment and supplies has ever beena source of irritation to division commanders, transportation officers,and division surgeons. . . . Much loss of equipment and consequent lossof dental service in several divisions has resulted thereby. The FirstDivision, moving into combat area, in. May 1918, was forced to abandontheir entire dental equipment through lack of transportation facilities.. . . At that time it required the entire resources of our Medical SupplyDepot No. 3 to resupply emergency equipment for this division after itsarrival in the new area." In Annual Report of The Surgeon General,U. S. Army, 1919, vol II, Washington, Government Printing Office, 1920.
85AR 40-1710, 23 Apr 28.
86See footnote 75, p. 178.
181
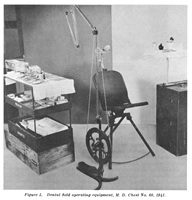
Figure 5. Dental field operating equipment, M. D. Chest No. 60, 1941.
needed for operation of a dental service where mobility was essential. When restrictions were placed on the shipment of more elaborate outfits overseas, Chest 60, augmented, was also supplied to general and station hospitals and general dispensaries of the communications zone. It lacked many of the refinements which made for convenience in operation, but contained the basic elements needed to meet routine needs in the combat zone. Patients requiring major oral surgery or prosthetic replacements had to be sent to more fully equipped installations, such as hospitals or mobile prosthetic teams.
Thousands of dentists who had always enjoyed every convenience in theircivilian offices soon found themselves operating with dental field chestson tropical islands or at. the edge of arctic glaciers. It is not surprisingthat their
182
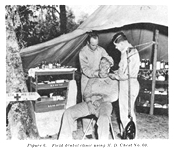
Figure 6. Field dental clinic using M. D. Chest No. 60.
equipment was the subject of much thought and criticism. Many recommendations from the field were highly impractical, failing as they did to consider the realities of procurement, maintenance, and transportation in time of war; others were based on sound observation and suggested changes which were ultimately incorporated into the outfit as the war progressed. Addition of an Electric Dental Engine. Older dentists who had operated foot-engines had no difficulty with the engine in M. D. Chest No. 60. Younger men mobilized in World War II had not had such experience, however, and generally refused to use the foot-engine.87 The Dental Division resisted this trend at first, and as late as September 1943 stated that "The addition of a small electric engine is not recommended. It is no great hardship to operate a foot-engine and it can be used under most any condition. If at fixed or semifixed installations an electric engine is considered necessary, a requisition can be Submitted for item 52530, Engine, electric, portable."88 It was found, however, that dental officers either used their assistants to pump the foot-engine, making them unavailable for their normal duties, or they obtained some type of improvised motor for attachment to their engines. Shops wasted valuable time and materials devising weird contraptions to mechanize this equipment. It was also
87Personal knowledge of the author confirmedby numerous photographs in the files of the Signal Corps Photographic Library.In no photograph is a dental officer shown pedaling his own foot-engine.Dentists either improvised engines or had the assistant operate the foot-engine.
88Memo, Dir, Dental Div, SGO, for Oprs Sprv,SGO, 3 Sep 43, sub: Proposed plan for dental service in an Armored Division.SG: 703.1.
183
found that modern warfare required electric current in a surprisingnumber of locations, even in the field. In March 1944 the Dental Divisiontherefore reversed its policy and recommended development of a motor whichcould be attached to the foot-engine.89 Issue of a conversionunit for use on existing foot-engines was authorized in November 1944.90
Addition of Operating Lamp. Dentists in the field usually badto work under cover, often in dark buildings or tents. Natural light undersuch circumstances was completely inadequate for dental operations. InFebruary 1944 the Dental Division requested development of a dental operatinglight which could be packed in M. D. Chest No. 60,91 and issueof this item was authorized in June 1945.92
Reduction in Weight of M. D. Chest No. 60. Chest 60, weighingsomething over 167 pounds, was too heavy to be hand-carried long distancesin rough terrain or in jungles. In November 1944 a project was startedto divide the contents of the field chest between two smaller containersweighing about 100 pounds each.93 Plans were being made at thesame time to pack other medical Department outfits in smaller chests, andprogress on the dental equipment was held up pending development of a basiccontainer, so that little had been accomplished on this development atthe end of the war.94
Reduction in Weight of the Dental Field Chair. An aluminum fieldchair had originally been authorized for the dental field chest, but whenquantity production was started the critical shortage of that metal forcedthe substitution of steel.95 As a, result the chair suppliedduring most of the period of hostilities was too heavy for convenient usein a portable outfit. Aluminum did not become available again until nearthe end of the war, and since the chair could not be placed in productionin time to be of much use in the current conflict it was decided to redesignthe entire item before resuming manufacture.96 This projectwas commenced in October 1944, but had not been completed at the end ofthe war.
Minor Changes in Contents of M. D. Chest No. 60. During the wara number of minor changes were made in the contents of Chest 60. In May1941 the old glass syringe designed for use with a fresh anesthetic solutionmade from tablets was replaced with a cartridge-type syringe using preparedcar-
89Memo, Dir, Dental Div, SGO, for Oprs Serv,SGO, 15 Mar 44. SG:700.2.
90Medical Supply Catalog, ASF, C 2, Med 6, November 1944. Washington,Government Printing Office, 1944 (cited hereafter as Medical Supply Catalog).
91Memo, Col Rex McK. McDowell for Inspections Br, Oprs Serv,SGO, 29 Feb 44. SG: 350.05-1.
92Medical Supply Catalog, C 5, Med 6, June 1945.
93Ltr, Brig Gen R. W. Bliss to Dir, Medical Department EquipmentLaboratory, 7 Nov 44, sub: Item 9502500-Chest M. D. No. 60, Complete. SG:428 (Carlisle Barracks) N.
94Monthly Status Report on Medical Department Research and DevelopmentProjects for Period 1-31 May 1945. HD: 700.2.
95The Corps Area Dental Surgeons' Conference. The Dental Bulletin.13: 254, October 1942.
96Ltr, Brig Gen R. W. Bliss to CG, ASF, 6 Oct 44, sub: Chair,dental, field, folding--development project on. SG : 444.4-1.
184
pules of solution,97 making it much easier to maintain sterilityof anesthetic solutions in the field. Early in 1945 the alcohol burnerfor the sterilizer, for which it had been difficult to obtain fuel, wasreplaced with a gasoline burner.98 A bone-file, rongeur forceps,and m-o-d matrix retainer were added at about the same time.99
Army Air Forces Operating Chest
In May 1944 the Army Air Force approved a special dental field chestfor use by its units. Complete, this chest weighed only 2 pounds more thanthe empty M. D. Chest No. 60. Reduction in weight was accomplishedpartly by using lighter materials, and partly by omitting certain heavyitems, particularly the dental field chair, for which a headrest attachableto an ordinary chair was substituted. The foot-engine was replaced withan electric dental engine. Only 50 of these chests were produced sincelater modifications in the regular Chest 60 made it better adapted to AirForce needs, and nonessential modifications of standard items were discouragedin the interests of maximum output.100
Prosthetic Field Chests
At the start of the First World War dental replacements were authorizedonly for teeth lost traumatically in line of duty. Some laboratory equipmentwas issued to base installations, but no field outfit was provided, andeven at Zone of Interior camps the dental surgeon had to draw teeth orgold for each individual case. In March 1918 this policy was liberalizedsomewhat to authorize the replacement, in time of war, of any teeth neededfor mastication, and thereafter a dental field laboratory set, weighingover 200 pounds, packed in a single chest, was issued to each division.101World War I prosthetic service was supplied on a relatively small scale,however, and nearly three times as many cases were completed overseas inthe single month of October 1944 (35,657)102 as were completedin France during the entire period of hostilities in the First World War(13,000).103
The World War II field laboratory set consisted of 2 chests (M. D. ChestsNos. 61 and 62, figs. 7 and 8), which occupied 10 cubic feet of space witha combined weight of 332 pounds. The cost of the complete outfit was about$600. This equipment included a casting machine, a hand-operated lathe,an assortment of teeth, and all the supplies needed for fabricating orrepairing
97SG Ltr 47, 22 May 41.
98New items of dental equipment. Army Medical Bulletin, No.88, May 1945.
99Ltr, Brig Gen R. W. Bliss to CG, ASF, 24 May 45, sub: StockNo. 9502500, Chest M. D. No. 60, Complete; Stock No. 9502600, Chest M.D. No. 61, Complete. SG: 444.4-1.
100Memo, Col George R. Kennebeck for Plans and Services Div,Office of the Air Surgeon, 3 Jul 46. SG: 428.
101See footnote 84, p. 180.
102See footnote 67 for fiscal 1945. HD: 319.1-2.
103History of the Army Dental Corps, 1941-43, Equipment andSupply Section, p. 15. HD: 314.7-2.
185

Figure 7. Contents of dental field laboratory, M.D. Chest No. 61.
the ordinary types of bridges or full or partial dentures.104 It could be set up well forward in the combat zone where it helped dental officers reduce emergency evacuations for prosthetic treatment, but was not adequate for routine quantity production because such conveniences as good lights, electric lathes, handy benches, and well-arranged plaster bins could not be furnished in such an outfit. The limited amount of expendable supplies included was also insufficient to maintain continued high output.
The Chests 61 and 62 were at first supplied to field hospitals, evacuationhospitals, surgical hospitals, the prosthetic teams of auxiliary surgicalgroups, convalescent hospitals, general and aviation dispensaries, andto the medical battalions of divisions. The later withdrawal of laboratoryequipment from most of these units, and its results, are discussed in thechapter on the operation of the Dental Service overseas. The most importantchange in the Chests 61 and 62 was the substitution, in February 1945,of a motor-driven lathe for the hand-driven type which required two men,working in relays, to operate. Since it had become apparent that electricitywould be available in most locations where dental laboratories could function,the wisdom of this move was obvious.
See footnote 75, p. 178.
186
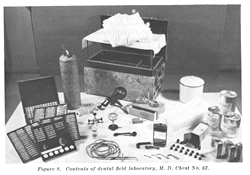
Figure 8. Contents of dental field laboratory, M. D. Chest No. 62.
Dental Pack Chests "A" and "B"
The dental pack chests contained operating equipment to meet the needsof mounted units. The 2 chests, which occupied 6 cubic feet and weighedless than 100 pounds, made a convenient load for 1 animal. They containeda little over 100 items, compared with 160 items in the M. D. Chest No.60, but with a folding chair, foot-engine, sterilizer, and routine instrumentsthey could be used to perform the most common operations.105No significant changes were made in them during the war, but in a mechanizedArmy their use obviously became more and more limited.
Dental Officer's and Assistant's Kits
The dental officer of each tactical unit was supplied 1 large shoulderpouch, and his assistant carried 2 smaller pouches, containing instrumentsfor emergency use in combat when M. D. Chest No. 60 was not available.The 3 pouches were supplementary to each other, and together included itemsrequired for the relief of pain, simple extractions, emergency treatmentof maxillofacial injuries, and temporary fillings. These kits were alsouseful during the movement of large units, when regular equipment was crated,and for that reason were frequently issued to general hospitals and otherinstallations having base dental outfits. They were also used by dentalofficers serving with ski troops or paratroops. The only important changein them was the
105See footnote 75, p. 178.
187
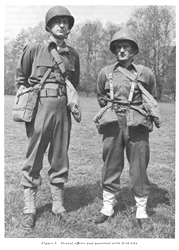
Figure 9. Dental officer and assistant with field kits.
188
replacement, in May 1941, of the glass-barrelled anesthetic syringeswith cartridge-type syringes. Contents of kits could be augmented or changedat will to meet the individual ideas of dental officers. It was reportedthat very little dental work was attempted in combat, and that dental officersoften carried kits of medical supplies in addition to, or in place of,the dental sets (figs. 9, 10, and 11).106
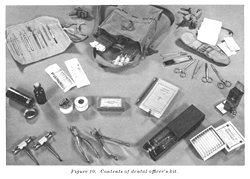
Figure 10. Contents of dental officer's kit.
Maxillofacial Kit
The maxillofacial kit which provided the highly specialized instrumentsneeded for the care of wounds of the oral structures was designed for useby the dental member of a maxillofacial team.107 It containedforceps, elevators, rongeurs, chisels, hemostats, lances, wire ligatures,and anesthetic syringes. The principal change in this set during the warwas the introduction of the cartridge-type anesthetic syringe (fig. 12).
The Mobile Dental Laboratory
(The complete story of the development of this important item is toldin a monograph by Lieutenants John B. Johnson and Graves H. Wilson.108Much
106History of the Dental Division, Headquarters,ETOU SA, 1 Sep-31 Dec 44. HD : 319.1-2.
107See footnote 75, p. 178.
108Johnson, J. B., and Wilson, G. H.: History of wartime researchand development of medical field equipment. HD: 314.7-2.
189
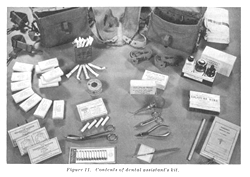
Figure 11. Contents of dental assistant's kit.
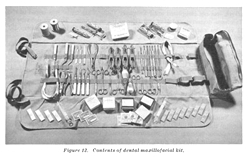
Figure 12. Contents of dental maxillofacial kit.
190
of the material presented here has been taken from that monograph, andits extensive documentation is not repeated.)
The need for improved dental laboratory facilities was based on a numberof considerations, some of which are discussed in greater detail in thechapter on the operation of the Dental Service overseas. In brief, it wasgenerally agreed that prosthetic equipment had to be taken to the soldierwhenever possible, to prevent his evacuation to a rear area for the constructionof dental replacements. For tactical units this meant that laboratory servicehad to be provided well forward in the combat zone, where frequent moveswere necessary. The laboratory with such a, unit had to be highly portable,it had to be put in operation quickly after a move, and it had to turnout a maximum of work in a short time when the opportunity was presented.M. D. Chests Nos. 61 and 62 were portable, but they failed to meet theother two requirements; it took considerable time to find shelter and setthem up in a new location, and with no source of water, fuel, power, orlight the only equipment which could be used was wasteful of manpower anddid not encourage the most accurate work. Further, the two small chestscould not contain enough supplies for prolonged operation in an emergency.The Dental Division therefore recommended, as early as May 1939, that developmentof a more satisfactory, truck mounted outfit be initiated.109
For reasons which are not clear this project proceeded very slowly.Approval was not granted until December 1941, and a pilot model, constructedwith the aid of $18,000 contributed by the manufacturers of precious metalalloys, was not completed until February 1943. This model was tested inthe Tennessee maneuvers of May and June of the same year. The first deliveryof 11 vehicles was made in March 1944, and distribution in foreign theatersdid not begin until near the end of 1944.
As finally adopted, the mobile dental laboratory (figs. 13 and 14) wasmounted on a 6-wheel drive, 21/2-ton chassis, capable of maneuvering inall but the roughest terrain. It carried a 1 1/2-KW generator, 50-gallonwater tank, electrically heated boiling-out and curing apparatus, acetylenetanks, a folding dental chair, a dental engine, an electric lathe, a fullassortment of teeth and all other equipment and supplies for completingor repairing ordinary dentures or bridges. A small trailer was later suppliedfor carrying the generator and other bulky equipment. It was operated by1 officer and 3 dental technicians, one of whom was also the driver.
Numerous improvised mobile laboratories had been placed in operationin foreign theaters while the standard truck was being developed. Constructedon vehicles ranging from captured German trailers to 30-passenger buses,these units had already given valuable service, so it was no surprise thatthe new trucks were highly commended from the start. A typical report wasthat
109Memo, Brig Gen Leigh C. Fairbank for SG,11 Sep 41, sub: Field dental laboratory. SG: 322.15-16.
191

Figure 13. Mobile dental laboratory.

Figure 14. Interior, mobile dental laboratory.
192
from a division which saw combat in both North Africa and Italy, statingthat "The mobile laboratory has proved to be the only answer to thedivision's prosthetic problem."110 Minor defects were reported,however, as follows:
1. While the mobile laboratory provided shelter for the operators inpoor weather it was badly crowded when the chair was set up inside fortaking impressions. In practice the chair was usually set up in an adjoiningbuilding or tent, and when time and circumstances permitted some of thelaboratory equipment was removed as well.
2. In bad weather, some provision had to be made for waiting patients.
3. The laboratory was tied to its vehicle, so that no transportationwas available for picking up supplies and mail, or for carrying water forthe storage tank.
4. When the truck required repairs it was necessary to close the laboratory.
5. The 11/2-KW generator proved inadequate, and a 21/2-KW model hadto be substituted.
6. The single dental lathe was not sufficient, and another had to beauthorized.
7. The small tanks of acetylene were quickly exhausted, and larger oneshad to be provided.
8. Trouble was experienced in obtaining "white gas" (i. e.without a leaded additive) for the burners.
The most fundamental defects were those noted in "3" and "4."These might have been eliminated by placing the laboratory in a trailer,pulled by a truck which could also be used for other transportation. Thispossibility was considered, but it was rejected because:
1. Maneuverability of a truck and trailer would be considerably reducedin unfavorable terrain.
2. It was feared that the truck might be commandeered in an emergency,making it necessary to abandon the entire laboratory.111
The mechanical defects noted were quickly corrected, and the mobilelaboratory was an important aid in bringing effective laboratory serviceto the forward areas.
A total of 107 laboratory trucks were ordered, and the last was deliveredin October 1945. It cannot be determined at this time just how many ofthese units were shipped overseas, though the distribution authorized inDecember 1944 was as follows:
European Theater of Operations | 30 |
Southwest Pacific Area | 15 |
Pacific Ocean Area | 5 |
China-Burma-India theater | 4 |
South Pacific Base Command | 4 |
North African theater | 2 |
110Dental Service with a Division in the Army.J. Am. Dent. A. 32: 1475-1476, Nov-Dec 45.
111Statement of Col Rex McK. McDowell to the author, May 1946.
193
It has already been noted that many theaters had improvised large numbersof mobile laboratories in addition to those standard trucks authorizedby the War Department, and it is probable that the number of these unofficialunits considerably exceeded the number shipped from the Zone of Interior.
The Dental Operating Truck
(The history of the development of the dental operating truck has beentold in a monograph by Lieutenants John B. Johnson and Graves H. Wilson,to which the reader is referred for greater detail and documentation thanwill be given here.)112
Dental operating trucks, which were not made available until near theend of World War II, had been used to a limited extent in the First WorldWar. In the summer of 1917 the Cleveland Chapter of the Preparedness Leagueof American Dentists suggested a project for the construction of "dentalambulances" which would be presented to the Army in the name of theRed Cross. Plans drawn up by the League were approved by The Surgeon General,and the first two units presented in October 1917.113 Otherchapters of the League cooperated until contracts had been let for a totalof 13 trucks, at a unit cost of about $4,000. These dental ambulances wereconstructed on a standard ambulance chassis, and contained a chair, 6-voltelectric engine operated by storage batteries, cuspidor, air compressorand tank, bracket table, sterilizer, and cabinet. Running water was suppliedfrom a storage tank to a small washbasin. The sides of the ambulance openedout and canvas flies were available to cover additional operating spaceadjoining the vehicle. Four dentists and 1 or 2 assistants could thus operatefrom each ambulance. Folding chairs and field equipment were provided forthe three officers who worked outside the unit.114 The WorldWar I dental operating truck was therefore a compromise which providedefficient equipment and utilities for 1 dentist and transported the regularequipment of 3 others.
Unfortunately, the dental ambulances constructed in the United Statesin the First World War never saw service in France. A shortage of transportationheld them at an American port of embarkation in spite of urgent requestsfor their delivery by the dental surgeon of the AEF.115 Two,dental ambulances were presented in France, however, and they were assignedto duty with motor transport troops and with the Air Service, where theyrendered very satisfactory service. The chief surgeon of the AEF commentedupon these units as follows:116
The need for dental ambulances-mobile dental offices-hasbeen indicated many
112See footnote 108, p. 188.
113Weaver, S. M. : Standardized motor dental car and equipment.J. Am. Dent. A. 5: 3-19, Jan 1918.
114Ibid. See also Dental ambulances and Christmas rollcall. J. Am. Dent. A. 5: 1283-1284, Dec 1918.
115See footnote 59, p. 174.
116See footnote 84, p. 180.
194
times during the campaign....The use of dental ambulanceswith outlying commands or detachments within divisional training areas,in the rear of combat sectors, or with the Air Service, would have provenof great value inasmuch as these mobile units could proceed to the variouslocalities with little loss of time, either in actual transport or in theunpacking and repacking of equipment ordinarily required of dental officerson itinerary dental service.
So far as is known, no effort was made to develop a standard dentaloperating truck in the period between World Wars I and II. When the DentalDivision requested such a project in May 1939 it was rejected within theOffice of The Surgeon General, and later numerous requests for a mobiledental unit from overseas theaters did not affect this decision. The AirForce particularly desired such equipment, and in December 1943 it finallyundertook development of a dental unit on its own initiative. Johnson andWilson imply that this action precipitated a sudden change of opinion inthe Surgeon General's Office. In any event the Dental Division resubmittedits recommendations; they were approved by the SGO, submitted to the CommandingGeneral, ASF, and accepted as a research project by the end of the month.When the Air Force asked for equipment for 50 dental trucks on 30 December1943 it was told that a standard model was already being developed, andits model was dropped.117 The Medical Department Equipment Laboratorycompleted a pilot model which was tested and accepted as a standard itemby 16 March 1944. Contracts were immediately let for 35 trucks, the firstof which was delivered in October 1944.
The mobile dental clinic (figs. 15 and 16) was mounted on a 6-wheeldrive, 21/2-ton chassis, similar to the one used for the mobile laboratory.In a space 13 x 7 feet were installed a unit, chair, cabinet, sink, sterilizer,50-gallon water tank, hot-water heater, and an operating light. Equipmentincluded all items needed for extractions, operative procedures, and fortaking impressions for dentures. A 2 1/2-KW generator supplied electriccurrent. No x-ray machine was provided. One hundred and thirty-eight operatingtrucks were purchased, at a unit cost of about $9,000, including equipment.It is not known how many trucks were actually shipped overseas, but theallotment authorized in December 1944 was:
European Theater of Operations | 33 |
North African theater | 18 |
China-Burma-India theater | 18 |
Southwest Pacific Area | 15 |
Pacific Ocean Area | 5 |
South Pacific Base Command | 4 |
The standard operating truck was not available soon enough to receiveextensive testing under combat conditions and estimates of its performanceare based
117Ltr, Col Gustave E. Ledfors, Chief of SupplyDiv, Air Surgeon's Office, to SG, 30 Dec 43, sub: Requirements of equipmentto be installed on mobile dental units. SG 444.4-1. See also 1stand 2d inds to above, 30 Dec 43 and 11 Jan 44.
195

Figure 15. Mobile dental clinic.
mainly on reports on similar improvised units which had been used in almost every theater since early in the war. There was little doubt, however, that this item met an important need. The Director of the Dental Division stated in 1945 that "The success of the mobile operating units in the several theaters, especially in Italy, warrants the conclusion that such units are essential to modern warfare." On the other hand, he did not consider that the final word had been written on the subject. He especially recommended that further thought be given to a. possible combination of a light trailer and truck.118 A German trailer of this type had been towed by a United States unit from the Rhine to Pilsen in Czechoslovakia, behind no more powerful a vehicle than a weapons carrier. If practical, a trailer clinic would not tie up transportation needed to carry supplies and would not have to be closed down when the truck needed repairs or maintenance. It would also be unnecessary for the dental operating team to drive a 2 1/2-ton truck to pick up mail or supplies. The objections to the use of a trailer are the same as those enumerated for the laboratory truck; decreased maneuverability and the danger of losing the prime mover in an emergency if it were detachable from the operating equipment.
118See footnote 21, p. 167.
196
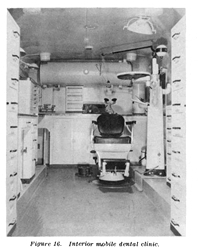
Figure 16. Interior mobile dental clinic.
In spite of the fact that it was not accepted for production, the operating truck developed by the Air Force was believed by officers of that organization to have certain features which should be considered in designing new models. Some of these features were:
1. Provision of a few laboratory items for simple acrylic repairs.
2. Use of a pressure-type water tank located under the body, where itwas easily accessible, rather than the gravity-type tank which had to bemounted on the roof.
3. Installation of the unit at floor level instead of about 6 inchesabove the general floor level, as was necessary in the 21/,-ton truck body.
4. More window space, better natural lighting.
Nonstandard Impression Chests
Units equipped only with the dental field chest had no supplies fortaking impressions for prosthetic appliances. Normally, prosthetic patientscould be transferred to nearby hospitals for this service, but in somecircumstances such a procedure meant the loss of a man to his organizationfor extended periods. To meet this situation the dental surgeon of theEuropean theater assembled chests
197
containing materials and equipment for taking impressions and pouringmodels which could in turn be sent to a central dental laboratory. A chestwould be loaned to an organization for a week or two at a time, and whenall prosthetic cases had been cleaned up the chest was returned to a depotfor replacement of missing or damaged items and for issue to another unit.Later in the war the mobile laboratory units were often able to bring prostheticservice to these isolated organizations, and the improvised impressionchests never became a standard item of issue. At the time they were devised,however, they filled a definite need.
THE DENTAL WARD CART
In hospital practice it was often necessary to provide dental care atthe bedside of patients. Personnel who were bedridden for considerableperiods of time frequently required definitive treatment which could notbe provided with a few instruments carried in a tray, and dentists improvisedcarts to carry the more essential equipment from patient to patient andfrom ward to ward. Some of the more elaborate outfits carried a dentalengine, operating lamp, sterilizer, aircompressor and spray bottles, anddrawers of instruments and supplies for most operative and oral surgicalprocedures. These improvised carts proved so efficient that a project fortheir development as a standard item was authorized in May 1945.119 Thisproject was of course not completed before the end of hostilities, butthe standard ward cart promised to add to the comfort of patients and theconvenience of operators as soon as it should become available.
SUMMARY
Experience in dental supply problems during World War II emphasizedthe following points:
1. In an emergency calling for the mobilization of many millions ofmen and thousands of dentists, requirements for dental equipment and supplieswill far exceed normal peacetime needs. At the same time production willbe hampered by shortages of manpower and materials, and imports are likelyto be cut off. Adequate production of such essential items as burs shouldbe insured in advance, and some control of distribution established toprevent such irresponsible buying, by both civilians and the military,as increased the demand for burs from 33 million a year before the warto nearly 100 million in 1943. To insure that minimum needs of the populationwill be met, plans to stop the production of any item, such as operatingunits, as nonessential, should be considered carefully and cautiously beforebeing adopted; in many cases it will actually be necessary to increaseproduction to meet new military requirements. It is possible of course,that new types
119See footnote 94, p. 183.
198
of warfare will eliminate mass mobilizations, and hence reduce militaryneeds; it is also possible that the manufacture of dental supplies couldbecome one of the casualties of a war for survival. It must be noted, however,that treatment received by the American public in peacetime is far fromadequate, and any further reduction, even in time of war, would have seriousresults which should be weighed carefully before deciding to cut the productionof items used by dentists.
2. Availability of supplies and equipment may well prove to be the factorwhich will determine the rate of mobilization of dental facilities in anemergency. Nothing will be gained by taking dentists on active duty tostand idle at their camps because they have no handpieces or chairs. Theprocurement of dental supplies in sufficient quantities will thereforebe one of the first responsibilities of officials directing the establishmentof an emergency Dental Service.
3. A considerable amount of dental equipment in the hands of civiliandentists will become idle when they are taken into the Armed Forces ina mobilization. It is possible that such equipment will have to be purchasedor leased for the military. The individual purchase of thousands of outfits,of widely varying types and degrees of serviceability, is in itself nosmall problem, however, and the cost of using secondhand equipment willgenerally exceed the cost of purchasing new items. It should not be assumedthat large quantities of dental supplies will be available from civiliansources until test projects have shown that such is actually the case.
4. Close cooperation between the Dental Service and procurement agenciesis essential, and such cooperation will probably be best obtained by assigningqualified dental officers to major supply installations.
5. Convenient and complete dental equipment should be supplied as farforward in the theater of operations as is consistent with the operationalsituation. Mobile operating and laboratory units will make it possibleto provide efficient equipment within easy reach of the fighting men.
6. In major moves dentists should not be separated from their equipmentif their outfits can possibly be forwarded as personal or unit baggage.Too many dentists spent from 1 to 4 months in idleness after their arrivaloverseas in World War II because their field chests had been shipped ondifferent vessels or in different convoys.