



AMEDD Corps History > U.S. Army Dental Corps > United States Army Dental Service in World War II
FACILITIES PROVIDED, ZONE OF INTERIOR
General Considerations
From the start of mobilization the Dental Division recommended thatwherever possible dental facilities should be centralized into large, efficient,clinics which would permit specialization and skilled supervision. In July1940 the Director of the Dental Division proposed:1
1. That the plan for the professional service of divisional camps andother new stations include a central dental clinic.
2. That the War Department be asked to include in its building programsuitable housing for such a clinic.
3. That central clinics be located in, or suitably near, the stationhospitals.
Preliminary plans called for 2 types of dental clinics, of 25 and 15chairs, respectively. It was later found necessary to provide smaller unitsfor certain exceptional situations, and by the end of the war the followingtypes had been authorized:
| DC-1 | 25 chairs | DC-4 | 3 chairs |
| DC-2 | 15 chairs | DC-5 | 1 chair |
| DC-3 | 8 chairs | DC-6 | 1 chair |
The DC-1 Clinic
The DC -1 clinic of 25 chairs was authorized for divisional campsor other stations with a strength of approximately 15,000 men.2 Itwas housed in a separate, 2-story, frame building 110 feet long and 30feet wide. The floor plans of the DC-1 are shown in figure 17. This clinic(figs. 18 and 19) was furnished with the most modern base equipment, includinglaboratory (fig. 20), x-ray, prosthetic, and oral surgical facilities.Each operator was supplied a standard chair, unit, cabinet, and operatinglight. DC-2 Clinic
The DC-2 Clinic
The DC-2 clinic consisted of a separate, single-story building withspace for 15 chairs. It was a smaller edition of the DC-1, designed tomeet the needs of camps of about 10,000 men.3 It was also usedas a dental clinic in all station hospitals of 250 beds or more.4In camps of less than 10,000 men, but large enough to have a 250-bed hospital,the hospital DC-2 supplied all dental care
1Memo, Brig Gen Leigh C. Fairbank for SG, 17Jul 40, sub: Definitive dental service in divisional camps and other largeinstallations. AG : 632.
2Dental expansion program. The Dental Bulletin, supp. to theBulletin of the U. S. Army Medical Department (cited hereafter as ArmyMedical Bulletin) 11 : 177, Oct 1940.
3Ibid.
43d ind, TAG to SG, 20 Nov 40, on ltr, SG to TAG, 2 Nov 40,sub: Dental service in cantonment hospitals-dental laboratory service,divisional areas. AG: 632.
258
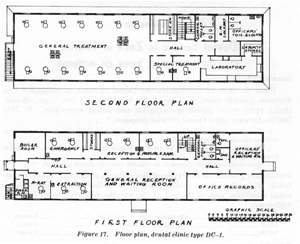
Figure 17. Floor plan, dental clinic type DC-1.
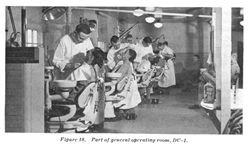
Figure 18. Part of general operating room, DC-1.
259

Figure 19. Oral surgical operating room, DC-1.
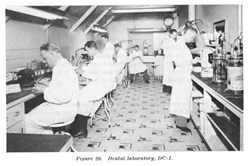
Figure 20. Dental laboratory, DC-1.
260
for the camp. If the installation had a population of more than 10,000men, but less than 15,000, additional facilities were provided in the trooparea. Equipment of the DC-2 was comparable to that of the DC-1. See figure21 for the floor plan of the DC-2 clinic.
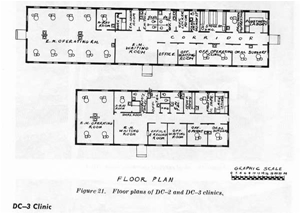
Figure 21. Floor plans of DC-2 and DC-3 clinics.
DC-3 Clinic
The DC-3 clinic, occupying a separate building with space for eightchairs, was developed about the middle of 1941 to meet the needs of postsof intermediate size.5 Policy for its use was not definitelystated, however, until early 1942, when The Adjutant General approved theseinstallations for camps of from 3,000 to 6,000 men. The DC-3 clinic wasalso used in hospitals of from 100 to 200 beds. See figure 21 for the floorplan of the DC-3.
DC-4 Clinic
The DC-4 clinic, with three chairs, was authorized early in 1943, primarilyfor use in small unit dispensaries. No separate building was provided andthe clinic occupied space in the regular dispensary quarters. The DC-4was sup-plied base-type equipment, with an x-ray machine and some laboratorysupplies.6
5The dental clinic number three. The DentalBulletin, supp. to Army Medical Bulletin 12: 249, Jul 1941.
6MD Equipment List No. 95058, 6 Dec 44.
261
DC-5 Clinic
The DC-5 clinic, with 1 chair, was also authorized in 1943 for use inthe smaller dispensaries where the 3 chairs of the DC-4 were not needed.It had no x-ray machine and only the most essential laboratory equipmentwas provided.7 Like the DC-4, it occupied space in a regulardispensary building.
DC-6 Clinic
The DC-6 clinic, which was a simplified version of the DC-5, was intendedfor use in prisoner of war camps. It was authorized a base-type chair butno cabinet. A mobile dental engine was substituted for the operating unit.8
Cost of the Various Clinics
The cost of the aforementioned installations was approximately as follows:9
| Type | Equipment | Building approximate | Total |
DC-1 | $33,684 | $25,000 | $58,684 |
DC-2 | 20,535 | 15,000 | 35,535 |
DC-3 | 11,356 | 10,000 | 21,356 |
DC-4 | 5,717 | (1) | 5,717 |
DC-5 | 2,425 | (1) | 2,425 |
DC-6 | 1,192 | (1) | 1,192 |
1None provided.
By September 1942, 100 DC-1, 150 DC-2, and 138 DC-3 clinics were inoperation or nearing completion.10 11
THE DENTAL SERVICE IN A REPLACEMENT TRAINING CENTER
General Considerations
Major dental rehabilitation for the inductee was not initiated untilarrival at a replacement training center, which was recognized to be themost favorable place in which to concentrate dental facilities. It wasthe first installation in which an inductee spent enough time to permitthe completion of extensive treatment.
The replacement training center was a large, fairly stable establishmentwhere the dental service could be organized for maximum efficiency. Speciallyqualified dental officers could be assigned to the more critical positions
7MD Equipment List No. 95059, 6 Dec 44.
8MD Equipment List No. 95054, 6 Dec 44.
9Cost of equipment listed is taken from the ASF Medical SupplyCatalog of 1 Mar 44, on file in HD. The cost of buildings of course variedgreatly in different locations and at different times. The figures quotedare approximate, obtained from the Fiscal Div, CE, Mr. Jonas Stein. Theywere given the author in a telephone conversation, 7 Mar 47.
10Mills, R. H. : Dentistry in the war. J. Am. Dent. A. 15 Sep42, p. 1754.
11At the time this history was prepared (1947) information wasnot available on the clinics constructed subsequent to 1942.
262
and trained auxiliary personnel and clerical assistants were availableto take over many time-consuming, nonprofessional duties.
Soldiers usually went directly from a replacement training center toduty with operational units and a high percentage were sent overseas withina short time. It was therefore desirable that all possible treatment becompleted during the training period, and absolutely essential that menleaving the center should at least meet minimum dental standards for foreignservice.12 From the start of the war the Director of the DentalDivision, SGO, recommended that replace-ment training center dental clinicsmeet the main burden of dental rehabilitation.
Operation of the Dental Service in a
Replacement Training Center
Time for the treatment of inductees in a replacement training centerwas limited; it was also necessary to avoid as far as possible interruptionof normal activities. The dental service in a replacement training centerwas therefore organized to attain three primary objectives:
1. To examine every man with the least possible delay and start histreatment immediately.
2. To check the progress of his work and make such additional examinationsas were necessary to insure completion of all required treatment beforehis departure from the center.
3. To provide dental treatment at times which would interfere leastwith scheduled training.
No uniform system was prescribed, and each dental surgeon used the methodswhich best conformed to his own ideas and to conditions encountered inhis particular camp. The operation, of a typical training center dentalservice (Fort Knox, Kentucky) has been described as follows:13
Dental surveys were conducted 3 times during each trainingcycle of 17 weeks. The first was made within 48 hours after the arrivalof the trainees from the induction centers. A second was made at the completionof the basic training period, before the start of specialist training.The third or final dental check was conducted during the final week ofthe training cycle, just prior to shipment.
All dental surveys were scheduled by the S-3 officer ofthe center as a part of training and the company commander was responsiblefor the presence of all trainees at every dental check within his unit.Surveys were conducted in the unit area by the dental surgeon and one assistant.Clerks for the examination were supplied by the unit.
The company was requested to furnish duplicate copiesof a current roster for every survey. At the time of examination an individualsurvey form was given to each trainee, who filled in all data on the formexcept the dental classification and infor- mation concerning his dentalcondition. This form was collected by the clerk at the time of examinationand entry made of the dental classification and pertinent informa- tionregarding prosthetic appliances. Forms and rosters were then taken to theoffice
12Memo, Brig Gen R. H. Mills for Exce Off SGO,27 Apr 42. SG:322.0531.
13Incl to Personal Ltr, Dr. H. L. Davidson to Col Walter Love,2 Dec 46. SG: 703.
263
of the dental surgeon where individual classificationswere entered on both copies of the roster and a record of prosthetic appliancesmade on the original copy. This copy was retained by the dental surgeonand the duplicate sent to the company commander for use in filling appointmentsallotted his organization.
From the data on the individual survey forms an MD Form79 [now AG Form 8-116, Register of Dental Patients] was made out for eachtrainee in need of dental care and held in the files of the dental surgeonfor use at such time as the man was ordered in for treatment.
Patients were treated at four widely scattered clinicsbut all orders for trainees to appear for treatment were issued from theoffice of the dental surgeon as an official memorandum over the signatureof the commanding general. The dental surgeon consulted flow charts andtraining schedules so that patients might be called for treatment duringthe least important parts of their training cycle, though dental care heldpreference over all training. A carbon copy of the memorandum directingmen to report for treatment, a list of the trainees requiring care, andthe previously prepared MD Forms 79 were forwarded to the clinic namedin the memorandum.
Patients were ordered for treatment by classificationonly, and the unit commander was charged with the responsibility for selectingmen of the indicated classification from his dental roster, detailing themto the specified clinic. Changes in classification were reported directlyfrom the clinic to the unit of the patient receiving care and to the officeof the dental surgeon. All completed MD Forms 79 were returned daily tothe files of the dental surgeon.
Should the individual clinic chief find it necessary tomake changes in the flow of patients, or should he be confronted by anydelinquency in keeping appointments, he discussed the matter with the dentalsurgeon, who took the necessary steps to correct the situation.
The midtraining survey was necessary because a considerablenumber of trainees were transferred to new companies due to sickness, emergencyfurloughs, etc. These men did not appear on the dental survey rosters oftheir new organizations and were easily lost to the dental service. Itwas therefore deemed advisable to conduct a new survey at the end of basictraining and carry through a second time as the original had been handled,except that new MD Forms 79 were made for new patients only.
The dental check made a few days before completion oftraining gave the dental surgeon a final chance to correct any defectsstill existing among the men about to be shipped out. These patients weregiven the highest priority.
The aim of the dental service of this replacement trainingcenter was to put every man in Class III or IV prior to completion of histraining. This policy was rigidly followed, especially in respect to menbeing sent to Army Ground Forces replacement depots. The dental surgeonhad the authority to request the removal of specific persons from shippingorders for dental reasons.
A check of original dental survey rosters over a periodof 42 months revealed the following average classification of men arrivingin the replacement training center from civilian life:
Class I | 22.5% (35% of these would require prosthetic replacements before completion of treatment.) |
Class I-D | 5.0% |
Class II | 22.5% |
Class III | 1.5% |
Class IV | 48.5% |
264
Treatment Rendered
The personnel of the larger camp dental clinics included specialistsin oral surgery and prosthetics, and the station hospital was able to giveinstitutional care when it was required. As a result, very few dental patientshad to be sent off the post for other than highly specialized treatment.However, when such treatment was necessary for conditions which involvedbadly comminuted or displaced fractures, severe infections, the removalof tumors, or plastic reconstruction, the patient was usually transferredto a general hospital. Dental hygienists provided many soldiers with theirfirst instruction in the individual care of the teeth and the supportingstructures. In general, the centralized clinics of the replacement trainingcenters and other major installations were well designed to provide rapid,efficient treatment of routine conditions and at the same time to givethe more complex defects the extra attention they required.
The "production line" organization of the larger clinics,with all surgical and prosthetic care given by specialists, undoubtedlyincreased output and improved the quality of the treatment rendered. Itwas not without disadvantages, however. In particular, the strain on menin the general operative section was severe. The placing of even routinefillings is meticulous work, hard on the eyes and nervous system, and requiringa tiring posture. In his civilian office the dentist is able to get a "changeof pace" by doing surgical, prosthetic, or laboratory work, but ina large Army clinic, the officer works continuously at the chair "pluggingamalgams," with another patient always waiting to take the place ofthe one just completed. The monotony and physical strain of performingone task over and over for months at a time was a constant cause of complaint.Further, the dentist had no chance to maintain his skill in other branchesof dentistry. The bitterness of young officers toward the "amalgamline" was certainly a factor in their lack of interest in a careerin the Army Dental Corps after the war.
Personnel Problems
In determining the number of dental officers to be assigned replacementtraining centers it was necessary to compromise between what was theoreticallydesirable and what was practical with available resources. The Dental Division,SGO, recommended a ratio of 1 officer for each 300 men in training andthis figure probably represented both the largest number which could bespared and the smallest number which could provide effective treatment.14However, the number of dentists actually provided varied greatly and cannotaccurately be determined, but figures on the overall assignment of dentalofficers in the Zone of Interior give some indication of the working ratio.
On 30 November 1942 there was 1 dentist for each 473 soldiers in theUnited States. This ratio decreased steadily until April 1943 when eachdental officer
14Memo, Chief, Oprs Serv SGO, for CG ASF, 5Jun 44, sub: Requirements for Dental Corps officers. HD: 314.
265
was responsible for 586 men. Thereafter the proportion of dentists againin- creased until in November 194415 it reached a fairly stablelevel of 1 officer for each 350 men. Some Zone of Interior installations(e. g. hospitals) had more than the average ratio; others had less (e.g. air fields); the proportion of 1 dentist for each 350 men is probablynot far from the ratio actually provided replacement training centers in1944.
THE DENTAL SERVICE IN A ZONE
OF INTERIOR REPLACEMENT DEPOT
The function of the dental service in Zone of Interior replacement depotswas to detect and provide treatment,16 within a maximum of 15days, for men who, when reporting for shipment overseas, still failed tomeet minimum dental standards. The details of operating the dental servicein a replacement depot varied in different installations, but two fundamentalrequirements had to be kept in mind: (1) early detection of the men needingtreatment, and (2) a system for insuring that patients were called to thedental clinic without delay and with minimum chance that they would be"lost" administratively. At one replacement depot, Camp Reynolds,Pa., new arrivals were first assigned to a casual battalion where processingwas completed. Men reporting to this battalion were marched directly tothe dental survey office where 2 dental officers and 3 clerks were constantlyon duty. Those in Class I were placed in a separate company and carriedas "unavailable for shipment" until their essential treatmenthad been completed. The dental service notified the Classification andAssignment Section whenever a man was ready for shipment and he was thentaken out of the "dental" company and returned to his unit, orto the regular processing line if he was a Casual.17
Personnel were allotted in about the same proportion as for replacementtraining centers, for though the men were passing through the replacementdepot in a much faster flow they had generally received more or less completedental care at previous stations, so that the average amount of work perindividual was much less than in a replacement training center.
Since only the most essential treatment was rendered at replacementdepots it might have been expected that extractions and dentures wouldhave constituted a high proportion of all operations performed. Apparently,how-
15The proportion of dental officers to totalstrength of the Army was calculated by author from data in Strength ofthe Army, 1 Mar 46.
16This service was also to be rendered at ports of embarkation,redistribution and redeployment stations, but in actual practice theseplayed a minor role in the process; ports of embarkation were primarilyconcerned with the supervision of embarkation, and with the sudden endof the war in Asia the activities of the redistribution and redeploymentstations were curtailed almost before they could reach stable operation.
17Annual Rpt, Surg Cp Reynolds, 1944. HD.
266
ever, these major dental deficiencies had usually been corrected athome stations, and work completed at replacement depots consisted of ahigher proportion of permanent fillings. The following tabulation comparesthe treatment rendered in a replacement depot (Camp Reynolds) in 1944 withthe treatment rendered in the total Army in the same period:18 19
| Operation | Percentage of five principal operations in a replacement depot | Percentage of five principal operations in the Army as a whole |
Permanent fillings | 87.6 | 78.1 |
Extractions | 6.3 | 18.0 |
Dentures | 3.8 | 2.8 |
Denture repairs | 2.2 | 0.9 |
Bridges | 0.1 | 0.2 |
THE DENTAL SERVICE IN A SEPARATION CENTER
Prior to 1944 the problem of providing dental treatment for men beingdischarged from the Army was overshadowed by requirements for the rehabilitationof inductees. A circular letter of 2 September 1943 prohibited the practiceof informing separatees that they could have their dental work completedin Veterans Administration facilities after discharge and also stated that"The status of the soldier with reference to his retention in theservice should be clearly understood before any extensive dental treatmentis started. Every effort will be extended to complete all essential dentaltreatment for a soldier, once begun, prior to his discharge."20While this letter encouraged the completion of work which had already beeninitiated, it also had the probable unintentional effect of discouragingextensive treatment for men due for early discharge. It was not the desireof the Dental Division or The Surgeon General to limit treatment for menleaving the service and on 7 March 1944 the Dental Division recommendedthat care be made available for all Class I patients prior to relief fromactive duty.21 On 31 March 1944 this recommendation was substantiallyrepeated in a memorandum to the Medical Practices Division, SGO, but noformal action resulted. In a Physical Standards Division conference on27 December 1944 the following points were agreed upon with the concurrenceof the Dental Division:22
1. Soldiers with Class I defects to be offered treatment prior to discharge.
2. Treatment to be optional with the man concerned.
3. Priority for treatment of separatees over other personnel to be givenonly at separation centers.
18See footnote 17, p. 265.
19Data on the Army as a whole taken from Army Medical Bulletin4 : 632, Dec 1945.
20ASF Ltr 156, 2 Sep 43.
21Memo, Act Dir Dental Div for Oprs Serv SGO, 7 Mar 44, sub:Dental treatment for personnel during demobilization. SG: 703.
22Memo for Record, 27 Dec 44, sub: Office policy regarding dentaltreatment at separation centers. HD: 314.
267
In spite of informal agreement on general policies for the operationof separation centers no official directive was issued until 10 September1945. Technical Manual (TM) 8-255, published on that date, provided that:23
Individuals having Class I dental defects which are incapacitatingor likely to interfere with performance of duties in military or civilianlife, or individuals who have lost anterior teeth in line of duty, willbe provided with appropriate treatment and/or prosthetic appliances priorto separation if the individual so desires. Routine dental treatment, suchas for Class II's, etc., may be provided for individuals, providing time,facilities and dental personnel are available, and providing the individualelects to have such treatment.
It was further directed that dental officers would be provided on examiningteams, in accordance with the number of separatees processed daily, asfollows:
| Number of daily examinations | Number of dental officers on teams |
| 75-150 | 1 |
| 200-300 | 2 |
| 400 | 3 |
| 500-600 | 4 |
| 800 | 6 |
| 1,000 | 7 |
| 1,800 | 12 |
These dental officers were concerned only with examinations; treatmentwas given in established clinics. In a memorandum of June 1944 it had alreadybeen recommended that dentists be provided separation centers in the, ratioof 1 officer for each 300 separatees,24 though the number actuallyassigned to each center was determined by the respective service command.
A letter to the service commands, dated 6 September 1945, quoted thetentative provisions of TM 8-255 and elaborated on them as follows:25
Every effort should be made to use existing dental facilitiesto the fullest capacity, and when such facilities are inadequate, additionaldental equipment should be installed in other available quarters to meetthe local demands.
Dental personnel, officers and enlisted men, should beshifted within the Service Command to permit the greatest service.
Under the provisions of AR 40-510, C 1, paragraph 5b(3), 10 September 1942, the procurement of civilian dental laboratory servicemay be authorized by the Commanding Generals of Service Commands whereadequate dental laboratory facilities are not available and when thereis insufficient time to have the cases completed at Central Dental Laboratories.. . .
At many stations the Dental Service operated a double shift.
The Dental Division was not in a position to predict how much work wouldhave to be accomplished at separation centers. The, dental classificationof the Army was known, but this classification was based on the urgencyof the treatment required rather than upon its amount. A man in Class II,for instance,
23TM 8-255, Terminal physical examination onseparation from military service, 10 Sep 45.
24See footnote 14, p. 264.
25Ltr, SG to CG 1st SvC, 6 Sep 45, sub: Dental treatment priorto separation from the Army. HD: 314.
268
might have 1 cavity or 10, so that information on total classificationswas of little value in estimating future needs. Above all, it was impossibleto predict 9 what percentage of men needing treatment would ask for it.Previous experience had indicated that only a small proportion of separateeswould risk delaying their discharge even a few hours, but many factorsinfluenced their decisions. It was found, for instance, that more men appliedfor dental care during the period when 45-day furloughs for recuperationand recreation were being granted than after that privilege was discontinued.26
Since the requirements for separatee dental service might change fromday to day faster than personnel could be shifted, the service commanddental surgeons could only establish the separation center clinics to meetaverage expected demands, thereafter maintaining an even flow of patientsby varying the types of service rendered. When the flow of separationswas slow, all kinds of treatment were offered and every effort made tocomplete routine fillings without delaying the departure of patients fromthe center. When the flow of separations was rapid, treatment had to belimited to the urgent cases specified in TM 8-255.
The organization of the dental service of a separation center offeredpeculiar problems which were solved in different ways on different posts.Separatees were understandably impatient to be released from the Army,even when they had asked to be held for dental care. They wanted furloughsand passes and often failed to return in time for appointments. Keepingin touch with the men under treatment was in itself a major problem, andconstant supervision was needed to insure that service was rendered isspeedily as possible and that patients were released for discharge as soonas their dental work was completed. Men requiring prolonged treatment werewithdrawn from processing, but every effort was made to complete minorcare without delaying departure of the patient, although in many casesonly a few nighttime hours were available for such treatment out of the48 which the separatee spent in the center.
The system in operation at Fort Monmouth was typical of the elaboratemethods used to control the dental patient in a separation center.27The salient points of the Fort Monmouth plan were as follows:
1. Patients were classified into three broad groups according to thetype and amount of treatment needed:
a. Men for whom treatment was urgent, including those requiringreplacement of missing teeth, received first priority and at their ownrequest were withdrawn from processing until treatment was completed. Noman in this group was refused care regardless of the backlog of patients.
26Incl to ltr, Col Arne P. Sorum to DentalDiv SGO, 30 Oct 46, sub: Dental treatment at a separation center. HD: 314.
27Memo, Maj Joseph G. Rosen for CG 1260th SCU, 16 Nov 45, sub:Plan of dental treatment at separation center, Fort Monmouth, N. J. SG:703 (Ft. Monmouth) N. J.
269
b. Men needing extensive but routine dental care were also withdrawnfrom processing at their own request if the backlog of patients was sufficientlysmall to permit starting their work within a reasonable time. But thesewere not accepted unless they could be given appointments within 36 hours.
c. Men needing routine care which could be completed at one sittingwere given appointments during free periods of their processing scheduleif such were available. Because these men were often fully occupied duringthe few daylight hours they passed in the installation, their work wasfrequently done at night. If no free time was available for completingtheir work during the normal processing period they could be voluntarilywithdrawn from the schedule under the same provisions as men in group b.
2. A dental officer was on duty at the Initial Receiving Point (IRP)at all times when separatees were being processed. This officer was notifiedin advance as to how many appointments of each type he might give out duringthe day. The IRP dental officer explained to each group the possibilitiesof getting dental treatment. If ample appointments of all types were availablehe notified the separatees that those requiring extensive care could bewithdrawn from processing for such treatment and that those with minordefects could have their work completed without delaying their departurefrom the separation center. If appointments could not be given during thenormal period of processing, but would be available within 36 hours, itwas explained that all men needing treatment could be given appointmentsbut that it would be necessary to withdraw them from processing until suchtreatment was completed. If the accumulated backlog of patients was suchthat no appointments could be given within 36 hours it was explained thatonly urgent cases would be accepted and that it would be necessary to holdthese from processing. The IRP dentist then examined those separatees whofelt that they qualified for treatment and who volunteered to delay theirdeparture if that was necessary. Those in the first two groups were immediatelysuspended from processing by notification to the IRP officer and givencolored cards which they took to the dental clinic as authority for startingtreatment (blue cards for Class, I's, pink cards for Class II's). Men inthe third group were given white appointment cards to the dental clinicfor a period when they were not required for processing.
3. All separatees were given a chance to request dental care at theTRPI as explained above. Those in Class I were given another opportunityto request treatment when they were given the dental examination duringprocessing. To avoid withdrawing partially-processed men from the line,those who did not require urgent care were not accepted later unless theyhad asked for treatment when given the opportunity at the IRP.
4. On arrival at the dental. clinic men in the first two groups weregiven appointments and their names entered on "suspense logs."The IRP dentist also sent in a list of those placed on suspense duringthe day and this was
270
checked against the clinic suspense log to insure that all men withheldhad actually reported to the dental clinic. This log was checked periodicallyto detect for investigation any patient who had been on suspense for anunusually long period. Any Class II patient who failed to keep an appointmentwas automatically released from suspense. The colored cards which patientsbrought to the dental clinic were clipped to their dental records and,when treatment was completed, were filled in on the reverse side and placedin a box which was emptied every hour. Separation center headquarters wasin turn given, by telephone, an hourly list of men whose cases had beenclosed, and this list was verified in writing at the end of the day. Apatient was thus released to continue his processing within an hour afterhis treatment had been completed. No special check was needed for men givenwhite cards for minor care since they were not withdrawn from the processingschedule. The proportion of separatees needing treatment was only a fractionof the number who had needed care when they entered the service. Of 278,309separatees processed at Fort Dix between 1 March and 30 September 1946only 0.86 percent needed extractions or other urgent treatment, only 1.75percent, replacement of missing teeth, and 10.15 percent, fillings or otherroutine care.28 Of those requiring treatment only a small percentagewere willing to delay their discharge even a few days.
The total number of separatees who received dental treatment at thetime of separation is not known since a report was made only of thosesuspended from processing, and many thousands had minor work completedwhile on the normal separation center schedule. During the demobilizationperiod, from May 1945 through October 1946, about 111,800 persons werewithdrawn from the examining line because they needed urgent oral treatmentrequiring a delay in their separation. Of these, about 104,900 were fordental defects, and about 6,900 for mouth and gum defects. These withdrawalsconstituted 1.6 percent of all personnel processed for separation duringthis period: 1.5 percent for teeth, and 0.1 percent for mouth and gum defects.While the proportion of men withdrawn from the line for dental reasonsmay seem to be relatively small, the number of persons who received suchcare is obviously quite important. In fact, the withdrawals for dentalreasons made up about 36 percent of the withdrawals for all physical reasons.About 2.6 percent of the persons withdrawn for dental reasons requiredinpatient treatment.29
Among the soldiers willing to wait for dental treatment, a high proportionneeded extensive prosthetic replacements. Over 65 percent of the men heldfor treatment at Fort Dix required replacement of missing teeth. Specialprosthetic sections had to be set up in many clinics and civilian laboratoriescalled
28See footnote 26, p. 268.
29Unpublished data, from Medical Statistics Div SGO, based onspecial reports dealing with the processing of military personnel at separationcenters, points, and bases.
271
upon to carry some of the unusual load. At Fort Dix, when 4,500 menwere being discharged daily, 1 officer with a staff car was kept busy deliveringand picking up cases from civilian laboratories.30
As a means of saving money the program for dental treatment of separateeswas not too successful. The Veterans Administration soon provided dentalcare for "service connected" defects of former military personneland the many men who had refused such treatment at a separation centerwere able to have their work completed later at Government expense. Theprogram did give the soldier a last chance to have essential work completedbefore he returned to civilian life, however, and those who took advantageof the offer were generally the most urgently in need of care and the mostdeserving of consideration by the Army.
Summary, Dental Service in Separation Centers
1. After extensive service in the Army the average separatee neededrelatively little dental care.
2. The majority of the men willing to delay their discharge to receivedental treatment required extensive replacements, necessitating specialprosthetic facilities and the use of civilian laboratories.
3. To be effective, the dental service of a separation center must havethe facilities and organization adequate to handle as many patients aspossible during the normal separation period. Very few men will take advantageof the proffered treatment if they must be suspended from processing toreceive it. To reach as many of these as possible it becomes necessaryto operate extensive facilities outside of regular duty hours.
THE DENTAL SERVICE IN ZONE OF
INTERIOR STATION HOSPITALS
Each Zone of Interior post of any importance had its own station hospitalfor the institutional medical care of local personnel. These hospitalswere not expected to render highly specialized treatment but were equippedand staffed to handle all routine medical and surgical conditions. Theyvaried in size from 25 to 1,000 beds or more. In small hospitals of lessthan 100 beds the dental clinic normally occupied a part of the administrationbuilding. Intermediate hospitals of from 100 to 200 beds were authorizeda separate dental clinic of 8 chairs (DC-3), while hospitals of 250 bedsor larger were provided a separate clinic building of 15-chair capacity.31The hospital clinics were
30See footnote 26, p. 268.
31Data on the dental clinics provided the smaller station hospitalsobtained by the author from Mr. James J. Souder, Act Chief Hospital ConstructionBr Hospital Div SGO, on 14 Apr 47. Hospitals of 250 beds or larger wereauthorized DC-2's by 3d ind, TAG, 20 Nov 40, on Ltr, SG to TAG, 2 Nov 40,sub: Dental service in cantonment hospitals-dental laboratory service,divisional areas. AG: 632.
272
authorized base-type chairs, units, cabinets, x-ray machines, and laboratories.Equipment and instruments were adequate for all routine operations.
Unlike overseas station hospitals, the Zone of Interior station hospitalshad no prescribed allotments of personnel. The number of officers and enlistedmen required in each situation was determined within the service commandon the basis of relative strength, the primary activity of the post, andindividual ideas of the staff officers concerned. Late in the war (October1945), ASF published a "guide" for the allotment of officersand men to station hospitals. It suggested that I dental officer and 11/2enlisted men be provided for each 200 hospital beds. Since the hospitaldental clinics on the smaller posts had to furnish all dental care forthe troop areas as well as for hospital patents, it was recommended thatthey be allowed 2 additional dental officers and 3 enlisted men for each1,000 troops.32 This directive was only advisory, however, andnot binding on local commanders.
The station hospital dental clinics fulfilled different functions onposts of different sizes, as follows:
1. On posts of less than 10,000 men the hospital dental clinic normallyfurnished all definitive dental treatment f or the command, including routinecare for outpatients, laboratory service, and any treatment of hospitalpatients which was not of a highly specialized nature. If tactical unitswere present on the post their own dental officers conducted surveys, heldsick call, and rendered emergency care to their men, but all other treatmentwas carried out in the hospital clinic, sometimes with the aid of the tacticaldentists on temporary duty. The hospital clinic constructed prostheticappliances, placed permanent restorations, treated infections about themouth, extracted diseased or impacted teeth, and rendered emergency treatmentto serious facial injuries pending their transfer to a hospital where specializedcare would be given.
2. On posts of more than 10,000 men the hospital dental clinic providedroutine care only for hospital patients. In addition it undertook the moredifficult types of treatment such as the construction of complicated prostheticreplacements or the extraction of impacted teeth. It provided care forinfections or other conditions which could not be treated on a duty statusand rendered emergency treatment for serious facial injuries. Simple fracturesmight be handled in the, hospital dental clinic but more difficult surgicalcases were normally transferred to a general hospital. Routine fillings,prosthetic restorations, and extractions for nonhospitalized personnelwere taken care of in the troop-area clinics.
The maximum number of station hospitals in the United States was reachedat the end of 1943 when 611 hospitals provided bed space for 270,499 patients.33
32ASF Ltr 389, 16 Oct 45.
33Info from files of Medical Statistics Div SGO.
273
THE DENTAL SERVICE IN ZONE OF
INTERIOR GENERAL HOSPITALS
Zone of Interior general hospitals were strategically located to providehighly specialized medical and surgical care which could not be furnishedin the station hospitals. A circular letter of 1 January 1943, stated that:34
General hospitals are established and maintained to affordbetter facilities than ordinarily can be provided in station hospitalsfor the observation, treatment, and disposition of complicated or obscurecases; for the performance of the more formidable surgical operations;and to provide beds for the evacuation of station hospitals. . . .
No hard and fast rules can be laid down, but in generalit will be the policy of the Medical Department to treat as general hospitalcases all patients who require more than 90 days' hospitalization, as wellas all cases requiring specialized treatment which is not available atstation hospitals. . . .
Complicated or severe fractures of the long bones, facialbones, and fractures of the vertebrae should be transferred to a generalhospital as early as possible. . . .
It was soon apparent, however, that not even all of the general hospitalscould provide certain types of treatment. The Adjutant General thereforedirected, in March 1943, that maxillofacial cases would be sent to oneof the following general hospitals:35
Bushnell General Hospital, Brigham, Utah.
O'Reilly General Hospital, Springfield, Mo.
Valley Forge General Hospital, Phoenixville, Pa.
Walter Reed General Hospital, Washington, D. C.
The number of hospitals offering maxillofacial care increased graduallyuntil the following eight installations were designated as maxillofacialhospitals in August 1944:36
Baker General Hospital, Martinsburg, W. Va.
Beaumont General Hospital, El Paso, Tex.
Cushing General Hospital, Framingham, Mass.
Dibble General Hospital, Menlo Park, Calif.
Northington General Hospital, Tuscaloosa, Ala.
O'Reilly General Hospital, Springfield, Mo.
Valley Forge General Hospital, Phoenixville, Pa.
Wakeman General Hospital, Camp Atterbury, Ind.
These installations were given specially trained personnel and everyitem of equipment needed for performing the most exacting operations onthe oral and facial structures. The other general hospitals had qualifiedoral surgeons, prosthodontists and operative personnel, and laboratoryand x-ray equipment, for the treatment of any but the most unusual cases.
As in the case of the station hospitals, allotments of personnel forgeneral hospital dental clinics were determined within the service commands.Pro-
34SG Ltr 1, 1 Jan 43.
35WD AG Memo W40-9-43, 6 Mar 43, sub: General hospitals designatedfor special surgical treatment. AG: 705.
36WD Cir 347, 25 Aug 44.
274
curement was based on the following hypothetical authorization of dentalofficers, but the hospitals concerned were not necessarily provided thenumbers listed:37
| Number of beds | Number of dental officers |
| 1,000 | 7 |
| 1,500 | 8 |
| 1,750 | 9 |
| 2,000 | 12 |
| 2,500 | 14 |
| 3,000 | 16 |
| 3,500 | 19 |
| 4,000 | 21 |
The maximum number of general hospitals in the United States was reachedin 1945 when 65 installations provided bed space for 153,595 patients.38
DENTAL SERVICE ON HOSPITAL SHIPS
Since the primary purpose of hospital ships was transportation ratherthan definitive treatment, the Dental Service operated on a slightly smallerscale than in a hospital of corresponding size. Ships of 400-bed capacityor less had a single exodontist in the grade of captain or lieutenant;with 500 beds an oral surgeon in the grade of major was authorized; with600 to 800 beds 2 officers were allotted, with the senior in the gradeof major; ships with 900 or 1,000 beds had a lieutenant colonel, a major,and a captain or lieutenant; vessels carrying 1,500 beds had a lieutenantcolonel, a major, and 2 captains or lieutenants.39
Hospital ships carried full base dental equipment, including prostheticand x-ray facilities. As mentioned, the smaller vessels were authorizedan exodontist, larger craft an oral surgeon. All types of work were possibleand needs of seriously wounded or ill patients could be met en route.
The Dental Service of hospital ship platoons proved less satisfactory.These auxiliary units were used to provide medical care for patients returningto the Zone of Interior on ordinary transports. Each platoon with a capacityof 100 or more patients was authorized a dental officer.40 Alarge proportion of all patients with maxillofacial injuries were transportedby air, however, and these small contingents had little need for a dentist.Also, much valuable time was wasted in long "layovers" betweentrips. Since specially qualified exodontists or oral surgeons could notbe spared for such minor organizations it was found that the men assignedwere often young and inexperienced.41 In view of these considerationsthe Dental Division decided that it would be in
37WD Cir 209, 26 May 44.
38See footnote 33, p. 272.
39T/O&E 8-537T, 7 Dec 43; T/O&E 8-537, 3 Mar 45.
40T/O&E 8-534, 21 Oct 43.
41History of the Dental Division, Hq ETOUSA, 1 Sep-31 Dec 1944.HD.
275
the best interests of all concerned if the dental officers and theirequipment were removed from hospital ship platoons.
A recommendation to this effect was made to the Operations Service,SGO, 7 March 1944.42 No action being taken, it was repeated7 December 1944.43 The new recommendation was approved by theTechnical Division, to which it was first sent, and forwarded on 20 December1944 to the Hospital Division for comment. The Hospital Division disapprovedthe proposed action because (1) it was felt that the dental officer wouldbe of some use treating patients, (2) dentists were filling administrativepositions which would have to be filled by Medical Administrative Corpsofficers if the dental officers were removed, and (3) it was believed thatthe dentists with the hospital ship platoons would serve as a useful poolof officers from which to draw in case of special need.44 Facedwith this nonconcurrence the Dental Division dropped the matter, thoughit still held that the use of dentists in hospital ship platoons was wastingmanpower needed elsewhere.
DENTAL SERVICE ON ARMY TRANSPORTS
In World War I regular dental service on Army transports, as distinguishedfrom incidental treatment rendered by transient dental officers, was notinaugurated until the latter part of 1919, when most ships on the Atlanticrun were provided dental personnel and equipment. The Surgeon General'sannual report for that year stated that experimental installations hadproved so successful that new transports were being built with space fora dental clinic especially provided.45 In the period of retrenchmentfollowing World War I, however, and with the withdrawal of most troopsfrom overseas areas, this project was neglected. In the period precedingWorld War II the transport surgeon was normally equipped with a few essentialdental instruments, and if no dental officer was on board as a passengerhe took what measures he could to relieve pain until the ship docked. Armyregulations authorized the assignment of dentists "if required,"but did not specify definite conditions under which such assignment wouldbe made.46 So long as transports were small the absence of adental officer was not serious, but when ships capable of carrying 10,000men were taken over at the start of the war adequate dental facilitiesbecame a necessity.
On 26 January 1942 the Dental Division recommended to the Finance andSupply Division, SGO, that a dental field chest be placed on every transport
42Biweekly Dental Service Reports, 1 Jan 1944-30Oct 1945. HD: 024.
43Memo, Dir Dental Div for Dir Technical Div SGO, 7 Dec 44.HD: 314.
44Memo, Col A. H. Schwichtenberg, Dep Chief Hosp Div for ChiefTechnical Div SGO, 23 Jan 45, sub: Dental officers in medical hospitalship platoons. HD: 314.
45Annual Report of The Surgeon General, U. S. Army, 1920, Washington,Government Printing Office, 1920, p. 303.
46AR 30-1150, 16 Sep 42.
276
so that emergency treatment could be rendered, presumably by personneltraveling on the ship.47 No specific action was taken, and inAugust 1942 the Dental Division resubmitted the recommendation, accompaniedby the following extract from a letter received from the European theater:48
One of my greatest headaches, and the source of my greatestcomplaints, is the dental service on board transports en route to thistheater of operations. As previously stated, in many cases there is littleor no dental equipment on board these transports to relieve the urgentdental emergencies. Reports come to me of acute conditions going untreatedduring the entire voyage.
The Chief of the Finance and Supply Division answered that he knew ofno convoys which had not had an adequate number of field chests assignedand suggested that the trouble lay in coordination at the ports.49On 16 September 1942 The Surgeon General directed all port surgeons tomake maximum use of the available dental equipment and officers to insurethat each transport complement was afforded at least emergency dental care.50On 23 November 1942 Col. Thomas C. Daniels, DC, was assigned to the NewYork Port of Embarkation to supervise the transport dental service underthe port surgeon, and to take any action required to provide dental officersand equipment on transports leaving the harbor. These steps were apparentlyeffective, at least so far as the eastern seaboard was concerned, for thedental surgeon of the European theater reported in October 1943 that hehad had no further trouble due to inadequate dental treatment on transportsbound for England.51 Dental field chests were, still not standardcomponents of the medical equipment of transports, however, and on 7 March1944 the Dental Division again recommended to the Operations Division ofthe SGO that M. D. Chest No. 60 be routinely authorized for all ships carryingArmy personnel.52 An equipment list published about a monthlater listed the dental field chest as a regular item for troop ships.53
When used on the larger transports field equipment left much to be desired.The amount of treatment to be rendered might equal that of a small post,and one ship reported that the dental clinic was in constant use from 8a. m. to 9 p. m.54 In addition, the light wooden chair of thefield set proved very unstable at sea and the foot engine was difficultto operate on an undulating platform. On 20 June 1944, after a conferencewith the Director of the Dental Division, the surgeon of the San FranciscoPort of Embarkation
47Memo, Col Don G. Moore for Finance and SupplyDiv SGO, 28 Jan 42. SG: 444.4-1 (BB).
48Memo, Col Rex McDowell for SG, 26 Aug 42. SG: 703.1 (BB).
49Memo, Col F. C. Tyng, Finance and Supply Div SGO, for GenJ. C. Magee, 28 Aug 42. SG: 703.1 (BB).
50Ltr, SG to CGs of all ports of embarkation, 16 Sep 42, sub: Dental attendance of troop transports. SG: 703.-1.
51Ltr, Col William D. White to Maj Gen Robert H. Mills, 22 Oct43. HD: 703 (ETO).
52See footnote 42, p. 275.
53Incl 4, Equipment List No. 9N809, to Ltr, Chief Oprs Servto CofT, 3 Jul 44, sub: Dental equipment for transports. SG : 444.4 (BB).
54Rpt, dental surg of an unnamed transport, 21 Jul 44. HD: 460(Army Transport).
277
asked that permanent outfits be authorized for troop transports operatingout of that base,55 and 4 days later his medical supply officersubmitted a requisition for 50 units, chairs, cabinets, air compressors,and operating lights.56 On the recommendation of the DentalDivision this requisition was approved.
On 28 June 1944 the Dental Division recommended to the Technical Division,SGO, that current equipment lists be amended to authorize base-type dentaloutfits for Army transports.57 For reasons which remained obscure,this recommendation was neither adopted nor disapproved. Its status on14 December 1944 was described in a letter from the Chief of the TechnicalDivision to the Chief of Operations Service, in which it was stated, ineffect, that all efforts to get a decision from the Chief of Transportationhad failed but that under existing instructions port surgeons could getthe necessary equipment when they wished. It was further stated that "Itis informally understood that the Chief of Transportation prefers thisarrangement to. any set requirement, which would necessitate the automaticinstallation of dental equipment on all transports regardless of the circumstancesunder which they operate or the availability of permanent dental personnel."58By 6 February 1945 the Dental Division had apparently given up any hopeof having permanent dental outfits authorized as standard equipment andasked the Technical Division to distribute a list of recommended itemsto assist port surgeons in ordering supplies on their own responsibility.59The Technical Division concurred in this request since it also had manyinquiries from port surgeons concerning appropriate outfits.60The Supply Service, SGO, disapproved, however, for the reason that it wouldbe tantamount to authorizing the issue of items for which no formal procurementauthority existed.61 Meanwhile, port surgeons had been ableto have the desired equipment installed in many transports without theformal approval of either the Chief of Transportation or The Surgeon General.By the end of November 1944, 35 ships had been so equipped62and by March 1945, 63 transports had permanent chairs and units. Sincethe most important needs had been met by these conversions the Dental Divisionnotified the Technical Division on 7 March 1945 that no further effortswould be made to have the base outfits placed on the standard equipmentlist.63
55Ltr, Brig Gen Wallace DeWitt to Col Rex McDowell,20 Jun 44. SG : 444.4-1 (BB).
56Incl 3, ltr, Col F. C. Tyng to Chief of Supply Div SGO, 24Jun 44, sub: Requisition No. D 4424-44, to ltr, Chief Oprs Serv to CofT,3 Jul 44, sub: Dental equipment for transports. SG: 444.4 (BB).
57Incl 1, Memo, Col Rex McDowell for Technical Div SGO, 28 Jun44, to ltr, Chief Oprs Serv to CofT, 3 Jul 44, sub: Dental equipment fortransports. (SG: 444.4 (BB).
58Ltr, Chief Technical Div to Chief Oprs Serv SGO, 14 Dec 44,sub: Dental equipment for Army transports. HD : 314.
59Memo, Dental Div for Chief Technical Div SGO, 6 Feb 45. HD:314.
60Memo, Chief Technical Div for Chief Supply Serv SGO, 21 Feb45, sub: Dental equipment for Army transports. HD: 314.
611st ind, Chief Supply Serv, 26 Feb 45, to memo cited in footnote60 above. HD: 314.
62Memo, Col Rex McDowell for Chief Technical Div SGO, 30 Nov44. HD: 314,
63Ibid.
278
PROSTHETIC FACILITIES IN THE ZONE OF INTERIOR
Prior to World War II, prosthetic facilities were concentrated in centraldental laboratories (figs. 22, 23, and 24). For a peacetime Army, or forsmall stations scattered over a corps area, these well-equipped laboratories,staffed with skilled technicians, could complete dentures or applianceswith enough 7 efficiency and economy to outweigh the disadvantages of transportingthese cases considerable distances. However, with a fully mobilized Army,it was recognized that the facilities of the existing central dental laboratorieswere64 inadequate to meet the demands of the increased prostheticneeds and plans were made to inaugurate laboratory facilities in the largercamps.
From the outset some laboratory space and equipment was provided inall the larger dental clinics. To reinforce these facilities The SurgeonGeneral recommended to The Adjutant General on 2 November 194065that a DC-2 clinic be established in each station or general hospital of250 beds or more. On 20 November 1940 The Adjutant General approved thisaction with additional comment as follows: 66 67
In camps of less than 10,000 strength the building willprovide dental chairs for all camp personnel, including hospital patients,and laboratory space for necessary making of prosthetic appliances. Incamps of over 10,000 strength the building will provide dental chairs forhospital patients only, and laboratory space for making prosthetic appliances.The division of floor space between chairs and laboratory will be madelocally.
Four months later, in March 1941, the Dental Division found it necessaryto ask that laboratory equipment for these station hospitals be increasedslightly, though it was still expected that the hospital laboratories wouldsufficiently reinforce the small prosthetic facilities in the camp dentalclinics.68
By May 1941 the Director of the Dental Division foresaw that largerlaboratories would be required in training camps and other strategic locationsand announced a plan for their construction.69 Responsibilityfor obtaining these installations, however, was left largely to local dentalsurgeons. In fact, Maj. Gen. Robert H. Mills, who became Director of theDental Division early in 1942, subsequently stated that he had at firstattempted to have additional CDL's authorized, and only after this recommendationhad been rejected by The Surgeon General did he definitely decide to establishlaboratories in each
64Final Report for ASF, Logistics in WorldWar II. HD: 319.1-2 (Dental Div).
65Ltr, SG to TAG, 2 Nov 40, sub: Dental service in cantonmenthospitals--dental laboratory service, divisional areas. AG: 632.
663d ind, TAG, 20 Nov 40, to ltr cited in footnote 65.
67The footnote referred to here is found only on a single copyof the basic communication. AG : 632.
68Memo, Brig Gen Leigh C. Fairbank for Finance and Supply DivSGO, 13 Mar 41. SG: 444.4-1.
69Fairbank, L. C.: Prosthetic dental service for the Army inpeace and war. J. Am. Dent. A. 28: 798-802, May 1941.
279
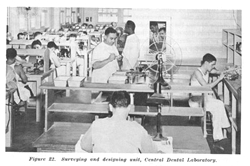
Figure 22. Surveying and designing unit, Central Dental Laboratory.
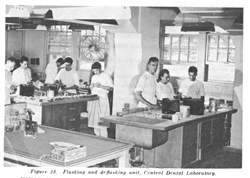
Figure 23. Flasking and deflasking unit, Central Dental Laboratory.
280
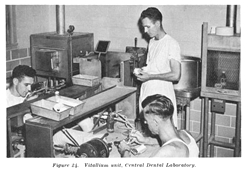
Figure 24. Vitallium unit, Central Dental Laboratory.
camp of 10,000 men or more.70 Standard camp laboratory equipment was prescribed in March 1943. In the annual report of the Dental Service for the fiscal year ending 30 June 1943, it was noted that "An increasing number of the larger camps have been able to institute their own laboratory service, thereby reducing the load on the central dental laboratories."71 From the annual report of the Dental Service for fiscal year 1944 it was noted "The tremendous requirements for dentures made it necessary to expand the laboratory facilities to include those camps of 10,000 or over . . . . "72 It was not until 1946, however, that a War Department circular stated unequivocally that:
All general hospitals, camps and stations with a militarystrength of 10,000 or over will furnish their own laboratory service, withthe provision that each of those stations is authorized to forward casesto the central dental laboratory serving its service command when localfacilities cannot meet the demands, and cases which require special fabricationmethods available only at central dental laboratories.73
Laboratories established in the more important camps were often largerthan the peacetime CDL's. Fort Knox, Ky., for instance, had 2 laboratoriesemploying a total of about 25 men to provide prosthetic service for a strengthof from 15,000 to 20,000 trainees.74
70Memo, Brig Gen R. H. Mills for Supply ServSGO, 15 Feb 43. SG: 322.15-16.
71Annual Rpt, Dental Serv, 1943. HD.
72Annual Rpt, Dental Serv, 1944. HD.
73WD Cir 21, 22 Jan 46.
74Info given to author by Col Walter D. Love, former dentalsurg at Ft. Knox.
281
General approval by the War Department did not in itself insure thatadequate facilities would be provided these camp installations, however.Under the usual system of assigning enlisted men, camp dental surgeonsstill had to obtain allotments of personnel in competition with all otherbranches. Moreover, there was no backlog of trained laboratory men in replacementcenters in 1942 and 1943. Often a large proportion of all enlisted menallotted to the dental clinic had to be put on duty in the laboratory,leaving few assistants for the operating sections. Later, civilian assistantswere hired to replace the technicians so lost, but at first, when demandswere greatest, the activities of many dental clinics were hampered by thenecessity of assigning half or more of their men to the construction ofprosthetic appliances.
The camp laboratories reduced the strain on the CDL's, but prostheticservice still had to be provided for a large number of stations too smallto operate their own establishments. It was therefore necessary to multiplythe facilities of the five existing CDL's, and their increasing outputfrom 1940 through 1944 is shown in the following tabulation:75 7677
| Year | Total cases completed |
| 1940 | 10,658 |
| 1941 | 10,658 |
| 1942 | 48,012 |
| 1943 | 216,358 |
| 1944 | 178,034 |
| 1945 | 153,908 |
But while the total output of the CDL's expanded about 2,000 percentbetween 1940 and 1943, they completed in 1943 only 22 percent of all prosthesesconstructed in the United States, as compared with over 50 percent in 1940.
Operation of the Laboratory Service
There can be no doubt that the prosthetic service was severely hamperedby shortages of personnel and equipment at a period when the demand fordental appliances was increasing many times as rapidly as the strengthof the Army.78 In spite of these difficulties there was surprisinglylittle delay in the processing of cases. In July 1943 the Director of theDental Division stated that the current time interval from impression toinsertion of the finished appliance was as follows: 79
75Data on the annual output of the CDL's in1940 are taken from Annual Report . . . Surgeon General, 1941.
76Figures for 1941-43 are found in Annual Rpt, Dental Serv,1944. HD.
77Figures for 1944 are found in Annual Rpt, Dental Serv, 1945.HD.
78For discussion of personnel and supply difficulties seechapters on "Personnel and Training" and "Equipmentand Supply."
79Memo, Brig Gen R. H. Mills for Chief Prof Serv SGO, 19 Jul43, sub: Construction of dentures. SG: 444.4-1.
282
| Elapsed Time | Percentage of appliances completed |
| 1-7 days | 33 |
| 8-10 days | 21 |
| 11-14 days | 18 |
| 15-21 days | 17 |
| 22-28 days | 6 |
| over 28 days | 5 |
Actual laboratory time (CDL's and station laboratories combined) was:
| Elapsed Time | Percentage of appliances completed |
| 1-7 days | 54 |
| 8-10 days | 18 |
| 11-14 days | 11 |
| 15-21 days | 10 |
| 22-28 days | 5 |
| over 28 days | 2 |
A comparison of the time required for the completion of cases in CDL'sand station laboratories is given in the following tabulation, based on21,156 appliances processed in CDL's and 73,416 in station laboratoriesbetween 1 June and 31 August 1943:80
| Elapsed Time | Percentage completed in camp laboratories | Percentage completed in CDL's |
| 0-6 days | 39.9 | 67.3 |
| 7-10 days | 23.8 | 17.7 |
| 11-14 days | 14.8 | 7.2 |
| 15-21 days | 12.4 | 4.8 |
| 22-28 days | 4.0 | 1.6 |
| over 28 days | 5.1 | 1.4 |
It is evident that CDL's were able to process cases in considerablyless time than the camp laboratories. This advantage was somewhat reduced,of course, by loss of time in the mails for cases sent to the CDL's, and21.8 percent of all cases completed in camp laboratories were actuallyinserted within 6 days after the impression was taken, compared with only15.3 percent of the cases completed in CDL's. But for any laboratory timeover 6 days the greater speed of the CDL more than offset the time requiredfor mailing, so that except for the 21.8 percent of the camp laboratorycases completed in less than 6 days the actual elapsed time between takingof impressions and insertion of the finished denture was less for appliancesmade by the CDL's than for appliances completed at the patient's home station.Actual elapsed time from impressions to insertion of the finished denturesfor cases completed in CDL's and camp laboratories is shown in the followingtabulation:81
80History of the Army Dental Corps, 1941-43,Table 16. HD.
81Ibid.
283
| Elapsed Time | Percentage completed in camp laboratories | Percentage completed in CDL's |
| 0-6 days | 21.8 | 15.3 |
| 7-10 days | 24.8 | 35.8 |
| 11-14 days | 17.6 | 22.8 |
| 15-21 days | 17.8 | 15.6 |
| 22-28 days | 8.6 | 5.7 |
| over 28 days | 9.4 | 4.8 |
Data on the output per technician are limited to the larger laboratoriesbecause of obvious difficulties in determining how much time was actuallydevoted to technical procedures in the smaller units. Figures given forthe large laboratories include all dentures, repairs and bridges, thoughthe latter item constituted a negligible part of the total. On this basiseach technician completed 58.6 cases per month in 1943 and 51.0 cases permonth in 1944.82 83 The decrease in output per technician in1944 was probably due to a slackening in the demand for dental appliances,which had made it necessary to operate with considerable overtime in 1943.
Use of Civilian Laboratories
In some individual centers the situation was more critical than indicatedby the aforementioned figures. In July 1943 Fort Bragg reported that minimumtime required for completion of a prosthetic case was 35 days; averagetime 56 days, while some patients had had to wait 120 days for their appliances.Fort Riley reported an average period of 91 days between impressionand completion of dentures.84 To meet these emergency situationsthe Dental Division was forced to make temporary use of civilian laboratories.In a letter of 26 November 1942 The Surgeon General called the attentionof local commanders to their authority to send cases to civilian installationsand requested that they take necessary action when military facilitieswere inadequate.85 86 The following day a second letter placedsome restrictions on the amounts and types of service to be obtained fromthe civilian laboratories, as follows:87
a. This is an emergency measure to relieve the presentcritical situation in construction of needed prosthetic appliances onlyuntil our dental laboratories are established and equipped to take careof our needs. It is in no manner to be construed as a reason for any delayof effort to establish and place in full operation laboratories adequateto care for all local needs in all large camps. The Central Dental Laboratorieswill then be able to meet the demands made upon them by smaller stations.
82Data for 1943 computed from History of theArmy Dental Corps, 1941-43. HD.
83Data for 1944 computed from Annual Report of the Dental Service,Jan-Dec 1944. HD.
84Memo, Lt Col R. S. Nourse, AG Replacement and School CommandAGF for CG AGF, 13 Jul 43, sub: Eye correction and dental restorations.SG : 444.4-1.
85AR 40-510, C 1, 10 Sep 42.
86Ltr, SG to CG 1st SvC, 26 Nov 42, sub: Prosthetic dental appliances.SG: 703.
87Ltr, SG to CG 1st SvC, 27 Nov 42, sub: Dental appliances constructedby civilian laboratories. SG: 703.
284
b. When laboratories are established as above, exceptin isolated cases, there will be no need for further employment of civilianlaboratories for the construction of dentures.
c. No special appliances, such as all-cast dentures ofgold, ticonium, vitallium, or similar materials, are to be authorized underprovisions of this letter.
d. In approving vouchers for payment care will be takento assure that the prices charged are reasonable and not above those chargedcivilian dentists for similar work in the locality.
After March 1944 payment for civilian laboratory service was made bythe service commands and it is therefore not known how many cases werecompleted under this plan. In 6 months, from March through July 1943, 16,607dentures were constructed by civilian laboratories,88 amountingto 5 percent of the total of 327,838 appliances constructed for Army personnelin the United States in the same period. From April 1943 through January1944 a single medical depot at Los Angeles paid vouchers for dentures constructedfor 8,643 patients, costing $276,271.35, or an average of $31.96 per patient.89At this installation the cost of dentures increased gradually from $23.09per patient at the start of the program to well over $30.00 at the endof the period reported upon. (About 40 percent of these patients received2 appliances.)
Important as the civilian laboratory service was in an emergency, itdid not supply a significant proportion of the total cases completed. BySeptember 1944 the central laboratories were able to handle all cases notcompleted in their home stations and a circular letter announced that astation unable to complete any appliance within 1 week would forward suchappliance to a CDL. It also directed that station laboratories would bediscontinued where diminishing activities warranted this step.90
Coordination of the Activities of
Camp and Unit Dental Officers
Tactical units in training in the United States or awaiting shipmentoverseas were concerned primarily with the instruction of their personnelin the duties they would have to perform in action. They were unable andunwilling to assume responsibility for the routine operation of the permanentstations on which they were temporarily quartered. Nevertheless, many postfunctions had to go on whether the units housed there were in barracksor absent on maneuvers or field exercises. A camp where tactical unitswere quartered was therefore authorized a permanent service detachmentwhich provided the neces-sary utilities and such special facilities asmedical and dental service. Since it was undesirable to change the campadministrative staff with each successive tactical organization, this servicedetachment was put under a post commander and its activities were independentof those of the tactical units.
88Memo, Voucher Audit Br AGO, for Col Rex McDowell,18 May, 3 Jun, 22 Jul, and 11 Aug 43. SG: 703.
89Weekly Civ Lab Rpts, LA Med Depot, 24 Apr 43-8 Feb 44. SO:703.
90SG Ltr 295, 8 Sep 44.
285
During the early period of mobilization the fact that tactical unitdentists were administratively independent of the post dental surgeonsled to some confusion. Unit dental officers had to devote much of theirtime to training activities, and were equipped with field dental chestsonly. They were therefore not expected to meet the routine needs of theirorganizations. However, though post dental officers were expected to assistthe unit dentists, they were not authorized in sufficient numbers to enablethem to provide full dental care for both permanent and temporary personnel.Adequate treatment could be rendered only by using both groups of dentiststo the limit of their availability. Post clinics were planned to provideextra working space for as many tactical unit dentists as could be sparedfrom their units, but some difficulty was encountered in obtaining theirservices when needed. Organization commanders disliked to release theirdental officers for duty in the camp clinic and often gave them nonprofessionalduties to occupy their time when not engaged in training. Unit dental surgeonsalso felt that they should have control of any installation where theirmen were receiving dental treatment and sometimes refused to cooperatewhen told that the camp dental clinic would remain under the directionof the camp dental surgeon.
To clear up any misunderstanding concerning respective responsibilitiesfor dental care on posts having both types of dental personnel, The AdjutantGeneral directed in January 1941 that:91
1. Camp dental clinics would operate under the camp commander.
2. Camp dental facilities would be operated and maintained so that theusing troops would derive the utmost benefits therefrom.
3. Tactical unit dentists would be used in the camp dental clinic wheneverthey were not required for essential duties in their own organizations.
4. The use of tactical unit dentists in camp clinics would be arrangedby mutual agreement between the commanding officers concerned. In caseof failure to come to an agreement the matter would be forwarded to theWar Department for decision.
At the same time it was explained in the Dental Bulletin that:92
... under its provisions [the directive mentioned above]the dental clinics will be activities operated by the personnel assignedor attached to the post, camp, or station complements and not by fieldforce personnel, although the dental clinics may be operated in areas occupiedby the field force. Under this same authority, the permanent personnelof the dental clinics (i. e. those assigned to post, camp, or station complements)has been limited to that necessary for the operation and maintenance ofthe post when all units of the field forces are absent therefrom. Thispersonnel will be augmented by members of units of the field forces onlywhen the field forces are present. When the field forces leave the postfor maneuvers or for any other reason, these men will be relieved fromduty with the dental clinic and will rejoin their units. . . .
91Ltr, TAG to CGs of Armies and Corps Areas,11 Jan 41, sub: Station complement activities and agencies. SG : 320.3-1.
92The control and operation of central dental clinics. The DentalBulletin, supp. to the Army Medical Bulletin 12 : 118, Apr 1941.
286
A second directive of 11 April 1941 provided that:93
a. Dental service at regimental and separate battaliondispensaries and aid stations will consist of emergency service and dentalsurveys in the tactical units to which the dispensaries are attached andwill be provided by dental officers attached to the regimentor separatebattalion.
b. Definitive dental treatment, serious extractions, andtreatment which demands more extensive dental equipment will be providedin camp or hospital dental clinics and will be under the control of theCorps Area Service Command.
c. Dental officers of the tactical units will receivetraining in medical tactics as auxiliary medical officers and in emergencytreatment of jaw casualties in their respective units. Technical instructionin more extensive definitive dental treatment will he provided in the campor hospital dental clinics. . . .
d. Training activities in medical tactics and functionsof the regimental and separate battalions will be under the direction ofthe division or unit surgeon. Technical training in camp or hospital dentalclinics will be under the direction of the camp or station surgeon.
In July 1942 still more specific instructions were issued, as follows:94
1. a. The current shortage of Dental Corps officers requiresthe maximum utilization for professional duties.
b. It is desired that all Dental Corps officers underyour jurisdiction who are now engaged in nonprofessional duties be relievedof those duties and returned to professional work with the Dental Corpsas soon as practicable, and that in the future no dental officers be assignedto nonprofessional duties. You are authorized to make exceptions to theforegoing policy only when the immediate release of such officers willseverely interfere with the functions of the medical service. In theseexceptional cases dental officers will be permitted to continue on nonprofessionalduties only until they can be replaced by qualified Medical AdministrativeCorps officers.
2. a. Instructions are being issued to division and othertactical unit commanders that up to 50 percent of the dental officers assignedto and present for duty with such organizations while they are at campsor stations where dental clinics are in operation are to be made availablefor duty at such clinics at all times.
b. It is desired that in cases of dental officers fromtactical units made available for duty in clinics under your jurisdiction,mutual arrangements be effected locally to insure that although the clinicswill be fully staffed at all times, no individual dental officer from atactical unit will spend more than 50 percent of his time on such dutyand that during the remainder of the time, each officer be returned tohis organization for such training as may be directed by the appropriatetactical commander.
The restriction on the nonprofessional use of dental officers curbedthe tendency of some commanders to use dentists for purely administrativefunctions, and at the same time the provision that 50 percent of the dentistswith tactical units would be on duty in the camp dental clinics whenevertheir organizations were on the post helped the service detachments completeessential dental treatment for these units before they were sent overseas.
93Ltr, TAG to CGs of Armies and Corps Areas,11 Apr 41, sub: Organization, training, and administration of medical units.SG: 320.2.
94Ltr, TAG to CGs all SvCs, 31 Jul 42, sub: Utilization of dentalofficers for professional duties. HD: 314.