



AMEDD Corps History > Medical Specialist > Publication
Part II
THE CONSTITUENT GROUPS IN WORLD WAR II
CHAPTER V
Wartime Organization and Administration
Colonel Emma E. Vogel, USA (Ret.),
Colonel Katharine E. Manchester, AMSC, USA,
Major Helen B. Gearin, USA (Ret.), and
Major Wilma L. West, AMSC, USAR
The expansion of the Army hospitalization program was concurrent with the period of mobilization, 1940-42. Of the 66 Army general hospitals in the United States in use during World War II, 21 were opened during 1941 and 1942.1 The mobilization program brought into acute focus the problems inherent in the civilian status of dietitians, physical therapists, and occupational therapists in the Medical Department. Those who had been with the Medical Department in the thirties could vividly recall the insecurity generated by the drastic reductions in their personnel and the cutbacks and elimination of professional programs following passage of the National Economy Act of 1933.
As civilian employees of the War Department, they had lived in the same quarters, if available, as those occupied by members of the Army Nurse Corps. They conformed to the same social rules. There were some privileges accorded them as civilians throughout the peacetime years, by nature of their professional status, which could not always be continued during wartime when large numbers of civilians in many diversified categories were employed in Army hospitals. Since dietitians, physical therapists, and occupational therapists were on a subprofessional status under civil service classification, no privileges could be granted to them if the other subprofessional employees could not participate. As the war progressed, government quarters were not often available and they had to obtain housing off the military reservation. With the implementation of gas rationing, this often proved to be a serious problem.
Except in acute emergencies, hospitalization and dental care were not available. Also, transportation to the first assignment was not paid by the government. The disadvantage of civilian status was increasingly evident to the dietitians. Even though their duties in military hospitals were essentially the same as those in civilian institutions, Army dietitians usually did not have control over mess personnel.
In December 1942, the dietitians and physical therapists were authorized relative rank in the Medical Department for the duration of the
1Smith, Clarence McKittrick: The Medical Department: Hospitalization and Evacuation, Zone of Interior. United States Army in World War II. The Technical Services. Washington: U.S. Government Printing Office, 1956, pp. 304-313.
102
war and 6 months thereafter.2 The military occupational specialty designation 3420 was given to the dietitians and 3418 to the physical therapists. Army serial numbers were assigned with an "R" preceding those of the dietitians and an "M" those of the physical therapists. Their civil service classification was terminated on 31 March 1943. In June 1944, they were granted full commissioned rank in the Army of the United States. (See Chapter I, pp. 8-10.) Although there were many efforts made by physicians and national and state occupational therapy associations to include occupational therapists in these legislative acts, The Surgeon General did not seek commissions for them since he had decided they would not serve overseas during World War II and thus would not need the protection under international law which military status provided.
Early in 1944, because of the increased difficulty of procuring occupational therapists under civilian status, it was proposed by The Surgeon General that occupational therapists be commissioned in the Women`s Army Corps and assigned to duty with the Medical Department.3 This proposal was not accepted by the occupational therapists. They wanted commissions, but only in a medically affiliated pattern similar to that authorized for dietitians and physical therapists. The proposal was not approved by the War Department.
Between World Wars I and II, there was no dietitian, physical therapist, or occupational therapist assigned to the Surgeon General`s Office. For many years, Miss (later Lt. Col.) Helen C. Burns,4 chief dietitian, and Miss (later Col.) Emma E. Vogel, chief physical therapist (fig. 25), at Walter Reed General Hospital, Washington, D.C., had served in an advisory capacity to the Surgeon General`s Office on matters pertinent to the training programs which they conducted and the assignment of their specialized personnel. A training program in occupational therapy had not been given since 1933.
Dietitians and Physical Therapists
Early in January 1942, Miss Vogel was assigned to the Civilian Personnel Division, Surgeon General`s Office, on a part-time basis to develop and coordinate the physical therapy program. By February 1942, when problems concerning procurement of dietitians for affiliated reserve units became more numerous and urgent, Miss Burns was also assigned.
In these positions, neither had an opportunity to visit other hospitals to coordinate and standardize programs because they had to
2Public Law 828, 77th Congress, 2d Session, 22 Dec. 1942.
3Memorandum, Lt. Col. Robert J. Carpenter, MC, Executive Officer, Office of The Surgeon General, for War Department, Chief of Staff, 8 Apr. 1944, subject: Commissions in the Women`s Army Corps for Occupational Therapists for Assignment to Duty With Medical Department Installations.
4Later Maj. Helen B. Gearin, WMSC.
 103
103
FIGURE 25. Miss Emma E. Vogel, chief physical therapist, and Miss Helen C. Burns, chief dietitian, Walter Reed General Hospital, 1942.
alternate their services every other day between Walter Reed General Hospital and the Surgeon General`s Office. This situation was alleviated on 24 August 1942 when both were appointed superintendents of their respective groups on a full-time basis. Miss Burns and Miss Vogel not only made field trips to Army hospitals to assist in establishing and maintaining adequate standards and procedures in their departments but they also were responsible for training activities, personnel actions, preparation of pertinent manuals and directives, and many other administrative and professional matters which concerned their specific professional group.
In January 1943, authorized by Public Law 77-828, the Secretary of War designated Miss Burns as director of dietitians and Miss Vogel as director of physical therapy aides. Commissioned in the grade of major, each was the first in her profession to be commissioned under this law. They were transferred to the Military Personnel Division where subsequently they established a Hospital Dietitian Branch and a Physical Therapy Branch. Their duties in these two branches continued to be essentially the same as when they were directors in civilian status.
Although a number of dietitians were assigned to duty in the Dietitian Branch from 1943 to 1947, only four were assigned on
104
other than temporary duty: Capt. (later Maj.) Helen A. Dautrich, Capt. (later Lt. Col.) Katharine E. Manchester, Capt. (later Lt. Col.) Eleanor L. Mitchell, and Capt. (later Lt. Col.) Ruby Z. Winslow. During this same period, the following officers were assigned to the Physical Therapy Branch: Capt. Jean Beatty, Capt. (later Lt. Col.) Olena Cole, Capt. (later Lt. Col.) Mary Lawrence, Capt. (later Col.) Harriet S. Lee, 1st Lt. Martha Norris, and Capt. (later Lt. Col.) Agnes P. Snyder.
Occupational Therapists
At the request of The Surgeon General of the Navy, the National Research Council`s Division of Medical Sciences formed a Conference on Occupational Therapy to advise on the proper organization of occupational therapy in the armed services. The first meeting was held on 15 May 1942. Dr. Winfred Overholser, Superintendent, St. Elizabeths Hospital, Washington, D.C., was chairman5 and Mrs. Winifred C. Kahmann, Director of Occupational and Physical Therapy, Indiana University Medical Center, Indianapolis, Ind., and Chairman of the Education and War Service Committees, American Occupational Therapy Association, was secretary.
Recommendations from this conference, which were forwarded to the Surgeons General of the Army and Navy, included two that had primary bearing on the organization of occupational therapy: "1. Each Army, Navy, and Veterans Bureau, General or Special Hospital, if practical, should have Occupational Therapy Service for reasons of morale and physical improvement. 2. Occupational Therapy Service should be under direct medical supervision in coordination with Physical Therapy."6
There was no central organization in the Army to plan and direct occupational therapy activities for hospital clinics, nor was there information on hand by which to judge requirements for personnel, equipment, and supplies. The Medical Department had "taken no steps to determine the kind and amount of such equipment required in event of emergency" and had suggested that perhaps the American National Red Cross could obtain this "as well as providing the personnel to supervise its use."7 The need for information with which to implement organization was evident to the conferees.
Two subcommittees were appointed by the President, American Occupational Therapy Association, one to investigate the procurement
5(1) Members included representatives of the Surgeons General of the Army, Navy, and U.S. Public Health Service, Veterans` Administration, civilian physicians representing the fields of psychiatry, orthopedics, tuberculosis, and general medicine, three occupational therapists, and the president of the American Occupational Therapy Association. (2) Doctor Overholser was also Chairman of the National Research Council`s Committee on Neuropsychiatry which worked to secure military status for occupational therapists.
6Minutes, First Meeting, Conference on Occupational Therapy, National Research Council, Division of Medical Sciences, 15 May 1942.
7Letter, The Surgeon General, to Norman H. Davis, Chairman, American National Red Cross, 6 Mar. 1939, undated memorandum attached, subject: Assistance To Be Requested From the American Red Cross Upon Mobilization.
105
and classification of personnel,8 the other to investigate supplies, equipment, and staff organization.9 In a combined progress report10 to the conference, on 20 January 1943, the committees proposed that-
1. A field director be appointed to direct organization of departments and maintain standards.
2. A short indoctrination course be given for occupational therapists.
3. All treatment be under the direction of a medical officer and that Red Cross volunteers working with patients in recreational and diversional activities be under the direction of an occupational therapist.
4. There be two occupational therapy units, neuropsychiatric and orthopedic.
5. There be five major types of treatment programs: physical injuries, neuropsychiatric conditions, tuberculosis, general medicine, and blindness.
At a fourth and apparently final meeting of the conference, on 2 June 1943, emphasis was placed on the need for the Civil Service Commission to reclassify occupational therapists from the trades and industries section to the medical section.11
Reports of the conference subcommittees12 reveal an abundance of information which was assembled for guidance and direction in establishing occupational therapy programs in military hospitals. That the work of the conference and its subcommittees was of tremendous value is evidenced by the later implementation of many of the proposals.
It was not until April 1943 that a central organization was established for occupational therapy in the Surgeon General`s Office. The impetus for this came directly from Col. Roy D. Halloran, MC, Director, Neuropsychiatry Branch, Medical Practice Division, Surgeon General`s Office, and indirectly from Maj. (later Lt. Col.) Walter E. Barton, MC (fig. 26).
While serving as Chief, Neuropsychiatric Service, Valley Forge General Hospital, Phoenixville, Pa., Major Barton had occasion to prepare recommendations concerning the requirements for treatment of psy-
8Chairman: Mrs. John A. Greene, Director, Boston School of Occupational Therapy, Boston, Mass. Members: Miss Helen S. Willard, Director, Philadelphia School of Occupational Therapy, Philadelphia, Pa., Miss Marjorie Fish, Director, Occupational Therapy Course, Columbia University, New York, N.Y.
9Chairman: Mrs. Winifred C. Kahmann. Members: Miss Charlotte Briggs, Director, Occupational Therapy, Niagara Tuberculosis Sanatorium, Lockport, N.Y.; Miss H. Elizabeth Messick, District of Columbia Health Department, Washington, D.C.; Miss Margaret S. Rood, Chief Occupational Therapist, Cerebral Palsy Clinic, Indiana University Medical Center, Indianapolis, Ind.; Miss Virginia Scullin. Chief, Occupational Therapy, Pilgram State Hospital, Brentwood, N.Y.
10Progress Report, Subcommittees of the Occupational Therapy Conference, National Research Council, 20 Jan. 1943.
11Minutes, Fourth Meeting, Conference on Occupational Therapy, National Research Council, 2 June 1943.
12(1) Report, Subcommittee on Supplies, Equipment, and Staff Organization. Occupational Therapy Conference, National Research Council, 8 Oct. 1942. (2) Report, Subcommittee on Procurement and Classification of Personnel, Occupational Therapy Conference, National Research Council, 9 Oct. 1942.
 106
106
FIGURE 26. Lt. Col. Walter E. Barton, MC.
chiatric patients in an Army hospital for Col. Henry Beeuwkes, MC, the Commanding Officer. In his recommendations, Major Barton placed considerable emphasis on the need for developing a satisfactory program of occupational therapy. Colonel Beeuwkes forwarded the recommendations to the Surgeon General`s Office where they were referred to Colonel Halloran, a strong advocate of occupational therapy. At Colonel Halloran`s request, Major Barton was transferred from Valley Forge General Hospital to the Neuropsychiatry Branch, on 22 April 1943, to organize the occupational therapy service.13
Two of Major Barton`s early achievements were the civil service reclassification of occupational therapists from the trades and industries section to the medical section and the restriction of appointments in the Army program either to graduates of accredited schools of occu-
13Memorandum, Lt. Col. Walter E. Barton, MC, to Director, Neuropsychiatric Consultants Division, 2 Nov. 1945, subject: Development of the Reconditioning Program Within the Activities of the Neuropsychiatric Consultants Division.
107
pational therapy or to those registered with the American Occupational Therapy Association.14
A Reconditioning Division, Surgeon General`s Office, was established in July 1943, to direct an Army-wide program for reconditioning convalescent soldiers.15 Major Barton was named director, on 19 August 1943, and the supervision of convalescent patient activities, including occupational therapy, was transferred from the Neuropsychiatry Branch to the new Reconditioning Division.
Continued development of the central organization initiated by Major Barton was assured by the appointment, on 18 November 1943, of Mrs. Kahmann (fig. 27) as chief of the newly established Occupational Therapy Branch, Reconditioning Division. She was extremely active in professional affairs on local and national levels and had contributed immeasurably to the development of Army occupational therapy. Mrs. Kahmann`s duties were similar to those outlined previously for the directors of dietitians and physical therapists. To facilitate administration of the program, the Surgeon General`s Office authorized the establishment of two positions in the Occupational Therapy Branch. Mrs. Kahmann`s two assistants, Miss (later Capt.) Wilma L. West and Miss H. Elizabeth Messick, arrived on 6 June and 27 August 1944, respectively (fig. 28). When Mrs. Kahmann returned to Indiana in November 1945, Miss Messick was appointed chief and served in that position until August 1948.
Organizational Problems
The need for personnel was a problem common to the three professional groups. Their national organizations, like other professional organizations, gave the fullest cooperation and support to the Surgeon General`s Office in the interest of obtaining qualified personnel, maintaining high professional work standards, and establishing training programs which would meet their criteria for accreditation or approval.
Because few, if any, of the newly appointed members of the specialist groups had previous experience with military organization or procedure, planning for orientation programs was necessary. Through these, a more immediate personal effectiveness and understanding in the work situations and relationships could be achieved.
Space was an acute problem in the physical and occupational therapy clinics. Because The Surgeon General at first did not have complete supervisory control over hospital construction in the Zone of Interior, many of the physical therapy clinics in new hospitals were entirely too small and required expansion almost as soon as they were operational. Physical therapy clinics were expanded in several of the old general
14The appointment provision precluded appointment of personnel considered by the Civil Service Commission to be qualified solely on the basis of experience and successful completion of the occupational therapy course offered to hospital attendants in a neuropsychiatric hospital of the Veterans` Administration. (U.S. Civil Service Examination, No. 11 (Unassembled)).
15Medical Department, United States Army. Organization and Administration in World War II. Washington: U.S. Government Printing Office, 1963, p. 213.
 108
108
FIGURE 27. Mrs. Winifred C. Kahmann, OTR. (Photograph by Paul Schmick for the American Magazine.)
and station hospitals. At Letterman General Hospital, San Francisco, Calif., a new building was constructed to house the gymnasium and electrotherapy sections. The new Fitzsimons General Hospital, Denver, Colo., opened on 16 December 1941, included a spacious and excellently equipped physical therapy clinic for clinical and teaching purposes.
The expansion program of medical facilities originally made no provision for space for occupational therapy. By 12 August 1943, when authorization for the program was effected,16 space requirements had been estimated and clinic floor plans were available for use in new hospitals being constructed or in modification of existing space.17
A problem which was apparent early in occupational therapy was the function of the volunteer Red Cross worker as it related to the use of handicraft activity with convalescent patients. Even though the
16Circular Letter No. 149, Office of The Surgeon General, 12 Aug. 1943. This circular letter also listed the types of patients for which occupational therapy was indicated, stated the qualifications for appointment, indicated sources of equipment and supplies, specified departmental organization and administration, and prescribed general rules for occupational therapists.
17Clinic plans were prepared by Major Barton and the Hospital Construction Division, Surgeon General`s Office, with the assistance of Mrs. Kahmann and Mrs. John A. Greene.
 109
109
FIGURE 28. Assistants in the Occupational Therapy Branch, Reconditioning Division, Surgeon General`s Office. (Left) Miss Wilma L. West, OTR. (Right) Miss H. Elizabeth Messick, OTR.
program was medically approved, it was not medically supervised. In 1944, the Surgeon General`s Office determined that volunteer arts and crafts programs would be supervised by the department of occupational therapy wherever such a department existed.
This arrangement was most successful for it allowed expansion of occupational therapy in hospitals in the Zone of Interior and freed professional personnel for therapeutic work. The Red Cross Arts and Skills Corps programs were conducted in the majority of Zone of Interior hospitals during the war. While the strength of the corps grew almost tenfold from 1943 to 1946, 715 to 6,700 volunteers, the number of volunteer hours contributed was even more impressive, 39,233 to 681,888.18
Dietitians and Physical Therapists
The earliest requirements listed for dietitians and physical therapists overseas were contained in two 1940 tables of organization, No. 8-507,
18Annual Reports, Arts and Skills Corps, American National Red Cross, 1943-44, 1945-46.
110
General Hospital, and No. 8-508, Station Hospital. A single dietitian was listed as a requirement in T/O 8-232, Evacuation Hospital.19 The ratio used was one qualified specialist to each 125 beds. Early in 1942, because of the shortage of personnel, the tables of organization were amended to authorize three dietitians and three physical therapists for each 500- to 1,000-bed station or general hospital.20
In 1943, the ratios for assignment purposes in the Zone of Interior varied from 1 each for every 150 to 250 patients. Additional personnel, however, were authorized for those hospitals conducting training courses for dietitians and physical therapists.21 Later in 1944, because of the critical shortages of these specialists, it was necessary to reduce the ratio to three dietitians and two physical therapists for a 1,000-bed general hospital; two dietitians and one physical therapist for a 750-bed station hospital; and one each for a 500-bed station hospital. Because of the expanded treatment program generated by the establishment of convalescent hospitals in 1944, physical therapists were assigned to these programs in greater numbers than were the dietitians; for example, the ratio was 5 to 1 in a 1,500-bed hospital, 8 to 2 in a 4,000-bed hospital, and 12 to 3 in a 6,000-bed convalescent hospital.
Occupational Therapists
The estimated need for occupational therapists, as established by the Surgeon General`s Office in 1941, was one for each 1,000-bed hospital. That this ratio was unrealistic was evidenced by a statement from the National Research Council`s Subcommittee on Physical Therapy, on 6 September 1941, in which it was recommended that personnel quotas include "four to six occupational therapy aides in each thousand-bed Army general hospital."22
Surveys pertinent to occupational therapy were conducted by the Surgeon General`s Office in August 1942,23 and by the American Medical Association in early 1943.24 The Surgeon General`s Office survey, investigating the need for establishing occupational therapy sections in hospitals caring for neuropsychiatric patients, showed that
19These three tables of organization were superseded by T/O`s 8-550, 1 Apr. 1942; 8-560, 22 July 1942; and 8-580, 2 July 1942.
20Letter, The Surgeon General to Commanding Officers, All Theater Hospital Units, 23 Mar. 1942, subject: Civilians for Theater Hospital Units.
21(1) War Department Circular No. 99, 10 Apr. 1943. (2) War Department Circular No. 306, 22 Nov. 1943. In addition to other provisions, this circular authorized for each of the training courses one captain (unless a captain was already assigned), and one first and one second lieutenant. (3) For more detailed information, see: Medical Department, United States Army. Personnel in World War II. Washington: U.S. Government Printing Office, 1963.
22Minutes, Third Meeting, Subcommittee on Physical Therapy, Committee on Surgery, Division of Medical Sciences, National Research Council, 6 Sept. 1941, p. 58.
23Letter, Col. John A. Rogers, MC, Executive Officer, Office of The Surgeon General, to Commanding Generals, All Service Commands, 11 Aug. 1942, subject: Establishment of Occupational Therapy Sections in Hospitals Caring for Neuropsychiatric Patients.
24Letter, M. G. Westmoreland, M.D., Council on Medical Education and Hospitals, American Medical Association, to Maj. Walter E. Barton, MC, Office of The Surgeon General, 18 Aug. 1943.
111
such facilities then existed in 5 Army hospitals and were recommended for 50 additional hospitals by the commanding generals of the service commands. The American Medical Association survey, investigating the civilian need for occupational therapists, indicated a range "from approximately 400 occupational therapists this year to 660 or more."25
When occupational therapy programs were established in Army hospitals in 1943, there were insufficient personnel on which to base recommendations for strength authorizations. By June 1945, it was possible to set a strength ratio of one occupational therapist per 250 authorized beds.26
PROFESSIONAL QUALIFICATIONS FOR APPOINTMENT
Dietitians
Initially, the qualifications for dietitians remained the same as during the peacetime period; namely, completion of a 4-year course leading to a bachelor`s degree from a college or university of recognized standing with major study in dietetics and, in addition, the successful completion of a training course for dietitians approved by The Surgeon General.
In September 1942, because of the increased need for dietitians, the experience requirements were broadened. In lieu of completion of an approved training course for dietitians, an applicant could substitute for each 6 months of training, 1 year of successful experience (within the past 10 years) as a dietitian in a hospital of at least a 200-bed capacity. This experience had to include diet therapy, planning of nutritionally adequate menus, supervision of employees, food preparation and service, ordering of food supplies and equipment, and food cost control. This change met the requirements for membership in the American Dietetic Association. When dietitians were given military status in 1943, the length of experience qualification was changed to 2 years.
Physical Therapists
The professional qualifications for the physical therapists were essentially the same for both civilian and military status. Required of the applicants was completion of not less than 2 years (60 semester hours) in an approved college with emphasis on physical education or biological sciences or graduation from an accredited course in nursing (table 5) and, in addition, completion of a physical therapy training course approved by The Surgeon General. Waivers for age and education were granted in the case of a few outstanding physical therapists whose appointments were recommended by The Surgeon General.
25The survey was based on requests for occupational therapists which had been received in a 1-year period, 1 April 1942 to 1 April 1943, by schools of occupational therapy.
26See footnote 13, p. 106.
112
TABLE 5. Tabulation of age and educational background of physical therapists, 31 October 1945
Occupational Therapists
Qualifications for the occupational therapists required that they be graduates of a school of occupational therapy approved by the American Medical Association or occupational therapists registered by the American Occupational Therapy Association. To be appointed a senior occupational therapist, one or more years of experience, following graduation, in the administration of occupational therapy under medical supervision was required.
Having had no military status in the regular Military Establishment, there were no Reserve dietitians, physical therapists, or occupational therapists who could be called to active duty. The needed professional personnel had to be attracted from their civilian positions. They were penalized if they accepted appointments in the Army on a nonmilitary basis as they could not secure military leaves of absence.
The increase in numbers of civilian dietitians from 45 in 1938 to approximately 800 by March 1943 and the increase in physical therapists for the same period from 35 to 354 resulted from a combination of procurement and publicity activities by Major Burns, Major Vogel, the Red Cross, the National Research Council,27 the national professional organizations, and the Civil Service Commission.
These agencies also assisted Major Barton in his procurement drive for occupational therapists, but the results were less spectacular. Forty-three occupational therapists were on duty in Army general hospitals when Mrs. Kahmann was appointed in November 1943. The need was estimated at 300. In her first 2 months, because of her Irish persuasiveness and personal acquaintance with occupational therapists, she was able almost to double the number of occupational therapists on
27The Subcommittee on Physical Therapy, Committee on Surgery, Division of Medical Sciences, National Research Council, was formed in 1940.
113
duty. In the next 6 months, the number was again doubled, thus increasing the total on duty to 180.28
American National Red Cross
In April 1939, the Red Cross, upon the request of The Surgeon General, began an enrollment program to build up a reserve listing of medical technologists who would be available for military service in the event of mobilization.29 The dietetic, physical therapy, and occupational therapy national organizations encouraged their members to enroll with the Red Cross.
The American Occupational Therapy Association requested that the educational qualification for enrollment be changed because it stipulated graduation from a 25 calendar-month training course. Although this conformed with the new educational standards established by the American Medical Association in 1936, the first students to graduate from the program did not do so until 1939; thus, enrollment with the Red Cross was limited to barely 50 of the 1,200 occupational therapists then on the Occupational Therapy Association`s membership rolls.30 The Association suggested, therefore, that the qualification be changed to read: "Graduates from an accredited school of Occupational Therapy, Registered Occupational Therapists, and those eligible for registration in the American Occupational Therapy Association." The Surgeon General, however, did not deem it advisable to change the requirements. His reasons were, as follows:31
The number of these people who will be required by the Army is not very great and their services will probably not be required immediately on mobilization. By allowing the requirements to stand as they are we will be in conformity with the American Medical Association and be in a position to obtain the services of the best trained people in this group.
During the pre- and early-World War II period, some members and 8 of the 19 affiliated groups of the American Occupational Therapy Association formally protested not only the enrollment program, "until the status of the occupational therapist has been cleared up," but also the exclusion of occupational therapists from legislation proposed to grant commissioned status to the dietitians and physical therapists.32
The August 1940 report of the Red Cross enrollment program showed that less than 3 percent enrollment had been effected from
28Annual Report, Reconditioning Division, Office of The Surgeon General, 1943-44, Occupational Therapy Section, pp. 4, 8.
29See footnote 7, p. 104.
30Memorandum, Board of Managers, American Occupational Therapy Association, for The Surgeon General, 19 Mar. 1940, subject: Enrollment by the Red Cross for Occupational Therapists.
31Letter, Col. Albert G. Love, MC, Office of The Surgeon General, to Mr. H. B. Atkinson, Director, Enrollment of Medical Technologists, American Red Cross, 2 Apr. 1940.
32(1) Correspondence files, "Military Procurement for Occupational Therapy, 1940-43." Archives of American Occupational Therapy Association, New York, N.Y. (2) Affiliated groups who filed protests were the District of Columbia, Hawaii, Illinois, Massachusetts, Michigan, Missouri, New Jersey, and New York Occupational Therapy Associations.
114
5,704 mail announcements to the three groups: 90 dietitians, 32 physical therapists, and 8 occupational therapists.33
Civil Service Commission
In December 1940, in order to expedite appointments, authority to procure and assign civilian personnel was decentralized to the civil service districts. Operational control of civilian personnel was also decentralized to the commanding generals of the service commands. Even though the professional qualifications for appointment as a dietitian, physical therapist, or occupational therapist were clearly stated by the Civil Service Commission, those standards were often not observed by the appointing agency. Procurement and assignment were sometimes made by persons who had no knowledge of the professional background and duties of the three specialty groups. This produced a situation which invited much criticism and adversely affected the procurement of qualified personnel.
Pending the establishment of a register of qualified dietitians, many who were not qualified were appointed on a temporary basis. They had no training in the planning of therapeutic diets and management of hospital kitchens, so they willingly performed the work of cooks and mess attendants to the detriment of the professional standards of the group as a whole.
Even though the registers compiled by the Civil Service Commission were used as a source of qualified physical therapists, individuals were appointed and assigned who did not meet the educational standards established by the Surgeon General`s Office. The Civil Service Commission believed that, since a sufficient number of qualified physical therapists were not available, the Medical Department should be willing to employ whoever was available. Another area of difficulty arose from the assignment of experienced physical therapists to positions where they were under the supervision of less experienced physical therapists. This resulted in unhappiness and discontent. By October 1942, The Surgeon General was again given centralized authority to procure, assign, and train dietitians and physical therapists.34
The Surgeon General assisted in the procurement of occupational therapists through the Civil Service Commission by forwarding names of eligible qualified therapists available for appointment of the commanding generals of the service commands. If a service commander desired to make a direct appointment of an occupational therapist whose name had not been submitted, concurrence was obtained from The Surgeon General.35 That this procedure was not always followed is evidenced by a restatement of this policy in an April 1944 directive.36
33Report, Enrollment of Medical Technologists, American Red Cross, 31 Aug. 1940.
34Memorandum, The Adjutant General, for Commanding Generals, All Service Commands, 24 Oct. 1942, subject: Dietetic and Physical Therapy Personnel in Army Hospitals.
35See footnote 16, p. 108.
36Army Service Forces Circular No. 118, 28 Apr. 1944.
115
Officer Procurement Service
In June 1943, recruitment of dietitians and physical therapists was assumed by the Officer Procurement Service, Army Service Forces. Since this organization was designated by the War Department as the procuring agency for other officers and had district offices established in many large cities, the procurement of these groups entailed only a few additional responsibilities.
The resulting increase in dietitian appointments was encouraging. By December 1943, 330 additional dietitians had been commissioned. Because of the limited number of physical therapists available from civilian sources, the number appointed through the efforts of the Officer Procurement Service during the war period was only 256.
In 1944, the number of appointments decreased because most of those who were interested had been appointed. The organization had, however, performed an outstanding service through its well-organized publicity program. People in the United States had been made aware of the terms "dietitian" and "physical therapist" and the acute need for these qualified specialists in the Army. This publicity was especially beneficial as training programs were expanded in an effort to meet the mounting requirements for personnel.
In September 1944, the ceiling for dietitians was 1,500 and for physical therapists, 1,000. By 30 May 1945, although requirements had been calculated as 2,303 for dietitians and 1,770 for physical therapists, only 2,150 dietitians and 1,700 physical therapists were authorized by the War Department.37
Training Programs
The national shortage of qualified personnel necessitated expansion of the dietitian and physical therapist training programs and the establishment of a program for training occupational therapists. (See Chapter VI, pp. 137-182.) With the exception of five enlisted members of the Women`s Army Corps who had participated in the apprentice dietitian program, all of the dietitian and occupational therapy trainees were procured through civil service appointment. The physical therapy trainees were either civil service appointees or enlisted members of the Women`s Army Corps.
APPOINTMENT, PROMOTION, AND CLASSIFICATION
Dietitians and Physical Therapists
Under the act of December 1942 (Public Law 77-828), all initial appointments, with the exception of those of the director of dietitians and the director of physical therapists, were made in the grade of second lieutenant, regardless of the amount of civilian or military
37See footnote 21 (3), p. 110.
116
experience. By May 1943, promotion boards had been appointed in the Surgeon General`s Office to act on all recommendations for promotion of dietitians and physical therapists in accordance with the number of spaces available.
To be eligible for promotion to the grade of first lieutenant required 18 months of satisfactory service with the Medical Department and recommendation by the individual`s commanding officer. Eligibility for promotion to captain also required a recommendation from the commanding officer and 8 years of experience as a dietitian or physical therapist. Five of those years had to be spent in Army service with two of them in an administrative capacity.
Since the number of captain spaces was so limited, the chief dietitians and physical therapists in Army hospitals conducting training programs were given priority in promotion. Originally, the percentage of spaces established by the Surgeon General`s Office, in January 1943, limited captain spaces to 1 percent and first lieutenants to 15 percent of the total number appointed. By May 1944, appointments of first lieutenants exceeded the limitation by 7 percent, and by December 1944, appointments in the grade of captain were in excess of the limitation by less than 0.5 percent.38
Originally, all promotions, except those made overseas, were approved by The Surgeon General upon the recommendation of the promotion boards. After full military status in the Army of the United States was authorized in June 1944, promotions were made in the service commands as they were for all other officers. After June 1946, when Army Service Forces was abolished, promotion boards were again established in the Surgeon General`s Office and final approval on promotions given by that office.
Promotions overseas were accomplished in the same manner as in the Zone of Interior, except for the provision pertaining to length of service in grade. In determining time in grade for this purpose, service outside the continental limits of the United States or in Alaska was counted as time and a half. Promotion overseas to the grade of first lieutenant should have been more rapid than in the Zone of Interior. Exceptions, however, sometimes occurred. For instance, few received promotions during the period of deployment. It was also true that some were not promoted because frequent transfers sometimes precluded the 3-month assignment period required to establish eligibility for promotion. This same frequency of move was experienced by commanding officers, and some, since they had no opportunity to become familiar with the capability of the individual, did not recommend promotion.
The appointment in the grade of second lieutenant and the promotion on length of military service failed to give some individuals credit for their experience in civilian hospitals. Early in the war, many young dietitians and physical therapists volunteered for service and were soon
38See footnote 21 (3), p. 110.
117
promoted to positions of responsibility in Army hospitals. For those older and more experienced persons who entered the service later in the war, promotions to the higher grades were not possible. Terminal promotions to the grades of first lieutenant and captain were authorized at separation centers for officers who had completed the specified length of service for the grade at the time of separation.
Occupational Therapists
Army occupational therapists appointed in the 1941-45 period were given civil service ratings of SP-5, staff occupational therapist, and SP-6, senior occupational therapist. Yearly salaries for these positions were $1,800 and $2,000, respectively. The subprofessional classification had been assigned in 1938 when professional training was not a requirement for the civil service occupational therapist. Since the Medical Department had included professional education and training in its qualifications for occupational therapists in 1943 to conform to current standards of practice, the necessity for a change in classification from subprofessional to professional was apparent.
This action was particularly important in view of the proposal of the Civil Service Commission that experience be substituted for education as a requirement for appointment of graduate and student occupational therapists. This proposal was occasioned by a provision of the Veterans` Preference Act of 1944:39
* * * No minimum educational requirement will be prescribed in any civil-service examination except for such scientific, technical, or professional positions the duties of which the Civil Service Commission decides cannot be performed by a person who does not have such education.
The burden to prove that occupational therapists should have professional classification fell on the Surgeon General`s Office. Achievement of the classification would preclude the selection and appointment of persons who did not meet professional education requirements.
Accordingly, an analysis of the duties and responsibilities of occupational therapists was made at the Thomas M. England General Hospital, Atlantic City, N.J., by representatives of the Secretary of War (Civilian Personnel Division) and The Surgeon General. These representatives then proposed the following changes in classification:40 Occupational therapist, P-1, $2,320 yearly (staff assistant); occupational therapist, P-2, $2,980 yearly (unit supervisor and/or assistant to head occupational therapist in general or convalescent hospital); occupational therapist, P-3, $3,640 yearly (chief occupational therapist in general or convalescent hospital center); occupational therapy consultant, P-4, $4,300 yearly (service command headquarters).
39Public Law 359, 78th Congress, 2d Session, 27 June 1944, also known as the Starnes-Schrugham Act.
40Letter, Col. Robert J. Carpenter, MC, Executive Officer, Office of The Surgeon General, to Office, Secretary of War, Civilian Personnel Division, attention: Salary and Wage Administrative Branch, 28 June 1945, subject: Classification of Occupational Therapist Positions.
118
On 2 July 1945, the Secretary of War approved publication of the new standards as official guides for the allocation of occupational therapist positions. He also said, "The Surgeon General`s Office is to be commended for this valuable contribution to the War Department classification program and is to be encouraged in the continuation of this work."41 One month later, The Surgeon General distributed the new standards to the commanding generals of the nine service commands and requested that all positions be reclassified on or before 1 Septemher 1945.42
Of the 800 dietitian and 354 physical therapist civilian employees on duty in Army hospitals before 31 March 1943, 565 dietitians and 279 physical therapists accepted appointments in military status.43 Peak strength was reached in mid-1945 when the dietitians numbered 1,580 and the physical therapists, 1,300.44
The distribution of World War II assignments for the dietitians and physical therapists is best illustrated by the record of the physical therapists. On V-J Day, physical therapists in the United States were on duty in 66 general, 54 regional, 66 station, and 23 convalescent hospitals.45 By early 1947, this number had been reduced to 14 general and 54 station hospitals. The oversea units to which physical therapists were assigned were 219 general, 101 station, and 4 convalescent hospitals, and 1 field hospital. By 1 August 1946, oversea assignments were reduced to 14 general and 28 station hospitals.
The peak strength, 899, for the occupational therapists was not reached until 1945. This number included 452 apprentices who were in clinical training and 447 graduate therapists. Of this number, only 200 had volunteered their services to the Army. The remainder were graduates of the War Emergency Course. By V-J Day, occupational therapists were assigned in 76 general and convalescent hospitals.46
In the early forties, the position of civilian physical therapist was available to both men and women.47 In accordance with Public Law 77-828, the position of civilian physical therapist was terminated on 31 March 1943.48 At that time, there were a few male physical
41Letter, Vernon G. Mickelson, Civilian Personnel Division, Office of the Secretary of War, to The Commanding General, Army Service Forces, 2 July 1945, subject: Classification of Occupational Therapist Positions.
42Letter, The Surgeon General, to Commanding Generals, All Service Commands, 2 Aug. 1945, subject: Standards for the Allocation of Graded Positions.
43(1) Manchester, Katharine E.: History of the Army Dietitian. [Official record.] (2) Vogel, Emma E.: Physical Therapists of the Medical Department, United States Army. [Official record.]
44See footnote 21 (3), p. 110.
45See footnotes 1, p. 101 and 43 (2), p. above.
46West, W. L.: The Future of Occupational Therapy in the Army. Am. J. Occup. Therapy 1: 89-91, March-April 1947.
47Circular Letter No. 8, Office of The Surgeon General, 10 Feb. 1941.
48Medical Department requirements for continuous service of dietitians and physical therapists from 22 December 1942 to 31 March 1943 precluded the granting of annual leave accrued prior to their acceptance of commissions under Public Law 77-828. It was first thought that these individuals would be protected under the Act of 1 August 1941 which provided that civilian Federal employees entering the military service would receive pay for all leave accumulated to them while in the civilian status.
The Comptroller General, however, ruled (B33305-1943) that, inasmuch as the position of civilian dietitian and physical therapist was terminated by Public Law 77-828, there existed no provision of law by which the compensation for accrued leave could be accomplished. Loss of this compensation constituted a hardship in many cases. A bill to authorize the payment of such leave was later introduced in the 79th Congress and was passed as Public Law 500 on 11 July 1946.
119
therapists employed in Army hospitals in the Zone of Interior. Since they did not come under the provisions of this law, which pertained only to female officers, they were assigned as enlisted men.
Because of their civilian status, only those dietitians and physical therapists who volunteered could be sent overseas. This was true even before the war for those who had been assigned to Tripler General Hospital, T.H., Schofield Barracks Station Hospital, T.H., and Sternberg General Hospital, Manila, Philippine Islands. The affiliated hospital units organized early in the war by civilian hospitals and medical schools often recruited their volunteers from among the dietitians and physical therapists on their staffs. In order that there would be no delay in activating affiliated units, The Surgeon General had the authority to make direct appointment of such individuals provided they met all qualifications and initiated applications for civil service appointment as soon as practicable.
Occasionally, vacancies occurred in hospital units when they were called to active duty. These were filled, if possible, by The Surgeon General before the unit departed for overseas. Some of the last-minute requests were filled by personnel on duty in the training pools which had been established for both the dietitians and physical therapists in several general hospitals.49
Another source of dietitians for oversea assignment was the enrollment program of the Red Cross. The Civil Service Commission granted authority for The Surgeon General to appoint dietitians who were enrolled to fill the vacancies in the oversea hospital units.
In June 1942, additional dietitians were classified as eligible for assignment to hospital units. These were qualified dietitians from other governmental agencies or those who had passed an appropriate civil service examination and who volunteered for oversea duty as an initial appointment.50
The remainder of the vacancies for dietitians in hospital units were filled from the oversea volunteer list maintained in the Surgeon General`s Office. Later, many civilian-trained dietitians volunteered after they had gained experience in the Army.
In 1942 and 1943, some oversea hospitals left the United States lacking physical therapists. In such instances, a limited physical therapy program was temporarily carried on by nurses and enlisted personnel.
49Circular Letter No. 34, Office of The Surgeon General, 16 Apr. 1942.
50See footnote 43 (1), p. 118.
120
In 1944, after physical therapists became available in greater numbers, they were sent overseas in groups to be assigned to hospitals which had embarked without them and to hospitals which had suffered losses due to attrition.
In some instances, physical therapists were employed locally to supplement the Army physical therapy staff. Three were so employed in Hawaii, seven in Australia, and an unknown number in England. There is no information available as to the total number of local physical therapists employed, but they contributed materially to fill the gap until more Army physical therapists arrived.
One oversea assignment problem was that frequently rush calls were put through for dietitians and physical therapists to join oversea units supposedly ready to embark. Weeks or months later, the unit concerned might still be in the staging area. These ill-timed assignments sometimes resulted in time spent in field training when a fixed installation nearby could have utilized them to their greatest professional advantage.
During the war, dietitians and physical therapists were assigned in every theater or area of operations. With the cessation of hostilities, hospital activities reverted to a peacetime status and the oversea requirement for dietitians and physical therapists was markedly reduced. On V-E Day, there were approximately 780 dietitians and 570 physical therapists on duty in all oversea theaters; 1 year later, these numbers had dropped to 125 dietitians and 70 physical therapists.51
In April 1943, at the time of the changeover from civilian to military status, three dietitians, Miss (later 1st Lt.) Ruby F. Motley, Mrs. (later 1st Lt.) Anna Bonner Pardew, and Mrs. (later 1st Lt.) Vivian G. Weissblatt, and one physical therapist, Miss (later Maj.) Brunetta A. Kuehlthau, were Japanese prisoners of war interned at Santo Tomas Internment Camp, Manila, Philippine Islands.52 Misses Motley and Kuehlthau had been assigned to Sternberg General Hospital since early 1940. Mrs. Weissblatt, wife of a United Press correspondent, and Mrs. Pardew, a former Army dietitian, who were living in Manila, had been employed immediately after the bombing of Pearl Harbor to assist in the care of the increased number of casualties.
Since civilian status had been terminated as of 31 March 1943 under the provisions of Public Law 77-828, Maj. Gen. Jay L. Benedict, President of the War Department Dependency Board, recommended that these internees be tendered military appointments. It was, however,
51(1) Monthly strength record maintained by Dietitian Branch, Surgeon General`s Office, May 1943-July 1948. (2) See footnote 43 (2), p. 118.
52Miss Mary McMillan, first physical therapist appointed in the Army in World War I, was in Manila early in December 1941 and was also interned at Santo Tomas. She did volunteer work in the prison camp until she was repatriated in September 1943.
 121
121
FIGURE 29. USAHS Acadia. (U.S. Army photograph.)
the opinion of the Judge Advocate General`s Office, on 17 May 1943, that "The War Department would not be justified in appointing these employees under revised regulations in the A.U.S. [Army of the United States] and necessarily without their knowledge and consent."53 One year later, The Surgeon General was authorized to tender appointments as second lieutenants to the four internees. As the letters of appointment could not be forwarded to these individuals for security reasons, they were retained in the Surgeon General`s Office. All four accepted their appointments upon liberation, on 3 February 1945, and were subsequently promoted to the grade of first lieutenant.
During World War II, 27 hospital ships were in operation for the evacuation of U.S. Army casualties. The Navy Department operated 3 and the War Department operated 24. The first ship to be operated as a hospital ship was the newly converted USAHS Acadia (fig. 29); one dietitian and two physical therapists were assigned on her maiden voyage, on 5 June 1943, to North African ports. Inasmuch as military status had been achieved by that time, authorizations were filled through normal assignment procedures and the necessity to use volunteers was obviated. The USAHS Seminole was the only other ship on which a physical therapist was assigned.
When the Acadia returned to the United States with her first complement of war casualties, it was learned that the physical therapists` activities had been exceedingly limited because of lack of space and
53See footnote 43 (1), p. 118.
122
equipment and that excessive motion of the ship made bedside treatment difficult. In view of the acute shortage of physical therapists, it was The Surgeon General`s opinion that their services could be better utilized in Zone of Interior hospitals. The Acadia had already departed for her second trip when this decision was announced, but on her return, the physical therapists were reassigned and their positions were deleted from the tables of organization for hospital ships.
There were only two hospital ships in which dietitians did not serve, the USAHS John L. Clem and the USAHS Ernest Hinds. During the course of the war, 42 dietitians were assigned to hospital ships; the greatest number assigned at one time was 27. Eleven dietitians had tours in two or more hospital ships. A second lieutenant was authorized for ships carrying 400 to 700 patients, a first lieutenant for those carrying 800 to 1,000 patients, and a first and a second lieutenant for those carrying 1,500 patients.
Hospital ships were not authorized spaces for occupational therapists nor supplies and equipment for such a program. By June 1944, it was recognized that, although the arts and crafts materials selected for use with regular troops were "suitable for the ordinary patients," ships` chaplains reported that psychiatric patients needed specialized equipment.54 The Army Service Forces, Special Services Division, therefore, suggested to The Surgeon General that a special kit be prepared for use by ships` chaplains "when mental cases are present." In view of his previously established policy that occupational therapy (personnel, supplies, and equipment) would be authorized only for Zone of Interior programs, and that arts and crafts activities on hospital ships and in oversea hospitals were the responsibility of the Red Cross, The Surgeon General advised the Special Services Division that the Red Cross would furnish special supplies.
As programs expanded, it became evident that adequate field supervision could not be exercised from the Surgeon General`s Office. Both in headquarters of service commands and in oversea theaters, there was a need for consultants to recommend assignment of qualified personnel so that they could be utilized most efficiently, to facilitate promotions and transfers, to maintain high professional standards, to interpret policy, and to accomplish better coordination with other professional services.
Service command consultants were authorized for occupational therapy in March 1944,55 and by November 1944, appointments had been made as follows: Second Service Command, Miss Elizabeth Smedes;
54Letter, Lt. Col. Frederick M. Warburg, AGD, Chief, Athletic and Recreation Branch, Special Services Division, Headquarters, Army Service Forces, to Col. Augustus Thorndike, Office of The Surgeon General, 12 June 1944, subject: Occupational Therapy Kits for Transports, with 1st indorsement thereto, 13 July 1944.
55Army Service Forces Circular No. 73, 11 Mar. 1944.
123
Third Service Command, Miss Rhoda D. Lester; Fourth Service Command, Miss Mary Reilly; Eighth Service Command, Miss Jane E. Mayers; and Ninth Service Command, Miss Hulda A. Steinmesch. One of the most critical problems facing these consultants was coordination of the apprentice training programs to be given in 40 Army hospitals. In November and December, 100 students were assigned to complete the clinical phase of their training and additional students were to follow in subsequent months. Although training outlines were available, coordination through the consultants was essential if uniform and comprehensive programs were to be conducted.
Although Major Burns and Major Vogel had requested that dietitian and physical therapist consultants be assigned to service command headquarters in 1944, these requests were not approved until June 1945.56 Letters recommending consideration of the establishment of these positions were sent to each service command headquarters. This was not a mandate; Headquarters, Army Service Forces, did not dictate that these positions be established, but left the authorization to each service command. Subsequently, Capt. (later Col., USAF) Miriam E. Perry, dietitian, and Capt. Lois Ransom, physical therapist, were assigned to Headquarters, First Service Command, and Capt. Mary Rose Conway, dietitian, and Capt. (later Maj.) Felie Clark, physical therapist, were assigned to Headquarters, Second Service Command. In some service commands, supervision of physical therapy activities was satisfactorily accomplished by orthopedic consultants and assignment of a physical therapist was not considered necessary.
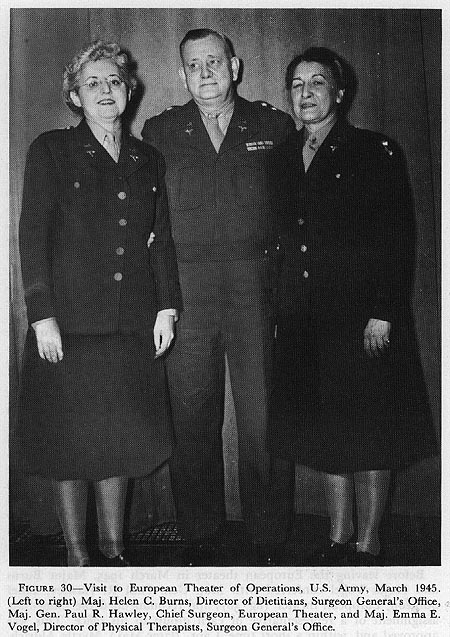
Early in 1945, when Major Burns and Major Vogel made a 3-month visit to more than 70 hospitals in the European and Mediterranean (formerly North African) Theaters of Operations, U.S. Army, they acquired firsthand knowledge of the difficulties which their personnel encountered. One of the major problems they found was that their personnel were assigned by officers who were familiar with neither the capabilities of the individuals nor with the requirements of the two specialized fields involved. Another problem frequently encountered was the lack of opportunity for dietitians and physical therapists to communicate with others in the same field. Many of these specialists were assigned singly in hospitals and the distances and workloads precluded any exchange of ideas or information.
Before leaving the European theater in March 1945, Major Burns and Major Vogel conferred with Maj. Gen. Paul R. Hawley, Chief Surgeon, European theater (fig. 30), and recommended the immediate assignment of a representative of each group to his office. This was approved and, within a short time, Capt. (later Maj.) Myrtle Aldrich, dietitian, and Captain Beatty, physical therapist, were assigned. Because of the decrease in military activity in the Mediterranean theater, there was no need for consultants at that time.
56(1) Quarterly History of Medical Department Dietitians, 1 June-30 Sept. 1945, pp. 2-3. (2) See footnote 43 (2), p. 118.
124
{kind=link}
Authority was given in May 1945 to provide one dietitian and one physical therapy consultant in the grades of captain to Headquarters, U.S. Army Forces in the Pacific.57 To provide these spaces, the bulk
57(1} Quarterly History of Medical Department Dietitians, 1 Apr.-31 May 1945, p. 3. (2) See footnote 43 (2), p. 118.
125
overhead allotment for nurses was reduced. In November 1945, Captain Mitchell, dietitian, and Capt. (later Lt. Col.) Edna Lura, physical therapist, were assigned to the Office of the Surgeon, Far East Command, and 1st Lt. Rosemary Rajkowski, dietitian, and Capt. (later Maj.) Emma T. Harr, physical therapist, were assigned to a similar office in the Middle Pacific Command. These officers were very helpful in solving the many problems associated with the inactivation of hospitals and reassignment and separation of their personnel.
After V-E Day, many problems arose in the European and Mediterranean theaters regarding redeployment of Medical Department personnel. Some hospital units were to be shipped directly to the Pacific areas, some were to return to the United States for inactivation or restaffing and subsequent reshipment to the Pacific, and others were to remain in support of the army of occupation. At the same time, it was essential to return those dietitians and physical therapists who could be spared to general hospitals in the Zone of Interior to assist in the care of casualties being returned from all theaters and areas.
Much of the planning for personnel actions was based on the adjusted service rating score.58 This score was computed (on a weighted point system) for all military personnel on the basis of previous service. In determining this score for dietitians and physical therapists, the Judge Advocate General stated that only commissioned service under the provisions of Public Laws 77-828 and 78-350 could be so credited.
The efficiency of the redeployment program as applied to dietitians and physical therapists was demonstrated in both major oversea theaters. In May 1945, there were 464 dietitians and 358 physical therapists on duty in the European theater; by May 1946, only 48 and 25 of the respective groups remained. In the combined Pacific areas, for the same periods, the dietitians decreased from 200 to 60 and the physical therapists from 147 to 42.59
Armies of Occupation
With the cessation of hostilities in both the European theater and in the Pacific areas, hospital activities reverted to a peacetime basis. Emphasis in patient care in the armies of occupation shifted from treatment of combat injuries to the illness and injuries incidental to normal activities of a military population. As a result, requirements for dietitians and physical therapists were markedly reduced. This reduction is borne out by the redeployment figures given previously.
The army of occupation hospitals were generally located in former military or civilian hospitals. When these were not available, other
58See footnote 21 (3), p. 110.
59See footnotes 43 (2), p. 118; and 51 (1), p. 120.
126
civilian or military facilities were converted for hospital use. In both areas, the hospitals which were taken over were usually permanent installations, well equipped, and well constructed. The military facilities in Germany which were converted to hospital use were barracks-type with no elevators, no hot water on the wards, and no connecting ramps or tunnels between the buildings. These posed a problem to dietitians when the central dishwashing and food cart washing rooms were located in the messhall area, usually a block or two away from the wards.
For army of occupation personnel in Europe, the year following V-E Day was a period of continual adjustment to the situation brought about by deployment. Many troops left the theater during the first 6 months which resulted in the closing or moving of hospitals. The hospitals which were not closed had a constant shifting of personnel during the last 6 months. The movement of hospital units to the Pacific areas also created a shifting of personnel as it made possible the rotation to the United States of those with long months of oversea service.
Demobilization
The problems concerned with the demobilization of an expanded military force were numerous and involved.60 When relieving officers from active duty, it was the desire of the War Department to give every possible consideration to the wishes of the officer concerned and to utilize to the maximum the services of officers who desired to continue on active duty. The separation of Medical Department personnel involved problems, however, which were not pertinent to other military personnel. Hospitals could not summarily close their doors and send their patients home. Since consideration had to be given to the continued care of patients, the need for specialists did not lessen as quickly as did the need for combat-trained soldiers.
Just as standards were established for eligibility to enter the military service, so standards were established to determine eligibility to leave the service. Separation criteria established for the dietitian and physical therapist were based primarily on five factors: (1) Age, (2) the adjusted service rating score, (3) marital status, (4) dependent children under 14 years of age, and (5) the officer`s efficiency index. These criteria were adjusted at different times during the demobilization period to either retard or accelerate separation (table 6) as indicated by the overall fluctuating needs. At the same time, all officers were given an opportunity to state their willingness to continue on extended active duty. This was done by their signing various types of commitments established by the War Department.61 In addition, there
60(1) For detailed information on Army-wide demobilization, see: Sparrow, John C.: History of Personnel Demobilization in the United States Army. Washington: U.S. Government Printing Office, 1952. (DA Pamphlet 20-210.) (2) See footnote 21 (3), p. 110.
61War Department Circular No. 366, 7 Dec. 1945.
127
were other criteria which governed the separation of officers; that is, surplus to the needs of the service; essential to national health, safety, or interest; undue hardship; and age.
In September 1946, an Army Nurse Corps officer was assigned to each of the 22 separation centers in the United States to act as counselor for Medical Department female officers. This assignment filled an urgent need as there had been numerous complaints that female officers returning from overseas were "sort of pushed around," as one officer stated, and given very little information relative to their rights or privileges under the GI bill of rights.
Many of the female officers who had married during the war desired to leave the service to establish their homes. Others were anxious to return to civilian life, not entirely because of a dislike of the service but rather because of the uncertainty of a future career in the military. Those returning from overseas were particularly aware of the need for permanent military status to assure a career with professional satisfaction. Also, the services of some who arrived overseas late in the war were never fully utilized because of cessation of hostilities in the particular area where they were assigned, and, for this reason, they assumed that their services were no longer needed.
Many experienced administrative dietitians had become disillusioned about their professional work in the military service when they found themselves working under untrained mess officers who did not permit them to apply their knowledge and training to the maximum extent in the management of the dietetic department. Many felt that this affected the dietetic treatment of the patient. On the other hand, some with little administrative training felt they had gained much administrative experience from the multiskilled mess officer. Without these mess officers, many dietitians would have found the oversea supply and equipment problems insurmountable.
There was no demobilization program, as such, for the occupational therapists. As Army hospitals were deactivated or as personnel ceilings were lowered, occupational therapists were released at regular intervals.
128
Procurement Following Demobilization
Demobilization caused a shortage of dietitians and necessitated a program for recall to active duty for those who requested it. In April 1946, a quota of 50 was set and dietitians who so requested were granted extension of active duty for an unlimited time (category 1) or active duty until 30 June 1947 (category 2) . All applicants for recall were carefully screened to assure that they met established criteria.
By October 1946, it was found that the number of dietitians eligible for separation greatly exceeded those who were surplus and available for reassignment. A procurement objective for 50 dietitians was authorized. This number was in addition to the number authorized for recall and all appointments were to be accomplished before 30 June 1947.
By June 1947, only 25 dietitians had been obtained through the recall program and 5 through the recruitment program for new officers. Although the recall program continued in effect, it brought only 15 additional dietitians back to duty by January 1948.
Uniform allowances were not provided the civilian dietitians, physical therapists, or occupational therapists, so each was required to purchase the uniform recommended for her particular group. Of particular interest to the dietitians was the change in style of their white hospital uniform in February 1941. This was the first official change in 18 years. Earlier, the uniform had been a straight one-piece dress of white poplin or percale which was slipped on over the head. It had long sleeves with tailored turned back cuffs. Because of the difficulty in purchasing the designated uniform, different styles were sometimes worn. The new uniform, also in white, could be either long or short sleeved and had a side opening which was closed by either zipper or snaps. A detachable stiff collar continued to be used.
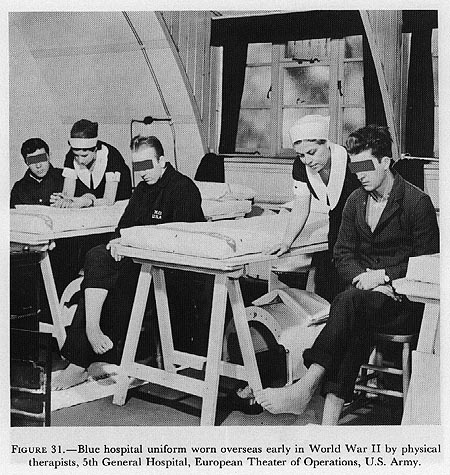
Early in the war period, physical therapists continued to wear the dark blue cotton hospital uniform (fig. 31) which had been authorized in the twenties. The dietitians and physical therapists going overseas early in 1942 joined their units wearing civilian clothes which they found not easily adaptable for wear with canteens, musette bags, gas masks, or life belts. Some hospital commanders issued them the blue street uniform then authorized for members of the Army Nurse Corps; however, they could not wear the official buttons or U.S. insignia.
In June 1942, summer and winter street uniforms were authorized for dietitians and physical therapists.62 They were compulsory items of wear for those going overseas and optional for those in the Zone of Interior. The uniforms were medium blue and several kinds of
62(1) Circular Letter No. 51, Office of The Surgeon General, 3 June 1942. (2) Early in 1941, Miss Helen C. Burns, chief dietitian, and Miss Emma E. Vogel, chief physical therapist, Walter Reed General Hospital, Washington, D.C., on their own initiative designed an attractive street uniform to be worn by their respective groups in the event of a national emergency. These uniforms are described in Circular Letter No. 51.
129
{kind=link}
material were available for summer or winter wear. The uniform also consisted of a blue overcoat, blue felt hat, tan or white shirt, dark red tie, and the "HD" or "PTA" insignia which were worn in the lapels. These uniform items were purchased by each individual.
Even though this uniform was approved, difficulties were encountered in obtaining priorities for the material. Few were able to procure complete uniforms and accessories. They felt fortunate to have even a partial uniform to combine with civilian clothing to wear overseas.
After military status was authorized in December 1942, the letters "HD" or "PTA" were also worn on the left of the hospital uniform collar with the rank insignia on the right. The use of these insignia was discontinued as soon as the caduceus with letters "HD" or "PT" superimposed was available.63
63(1) Army Regulations No. 600-35, 6 Mar. 1943. (2) For insignia of all Medical Department personnel in World War II, see: Medical Department, United States Army. Personnel in World War II. Washington: U.S. Government Printing Office, 1963, frontispiece.
130
{kind=link}
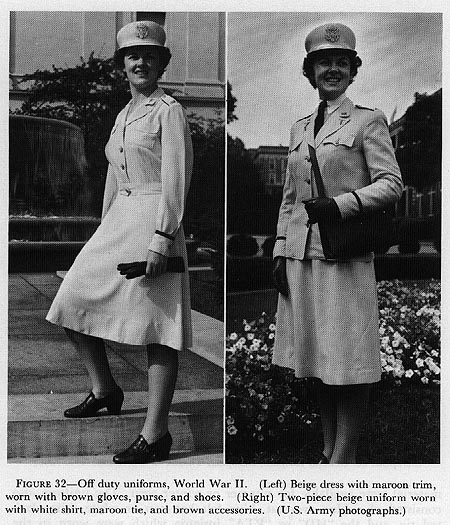
These uniforms were worn until the spring of 1943 when dietitians and physical therapists were authorized the hospital uniform, two-tone blue street uniform, and the off duty dress and suit (fig. 32), worn by members of the Army Nurse Corps. In 1944, when full military status in the Army of the United States was authorized for dietitians and physical therapists, they wore the olive-drab uniform and accessories which were authorized for all women in the Army.
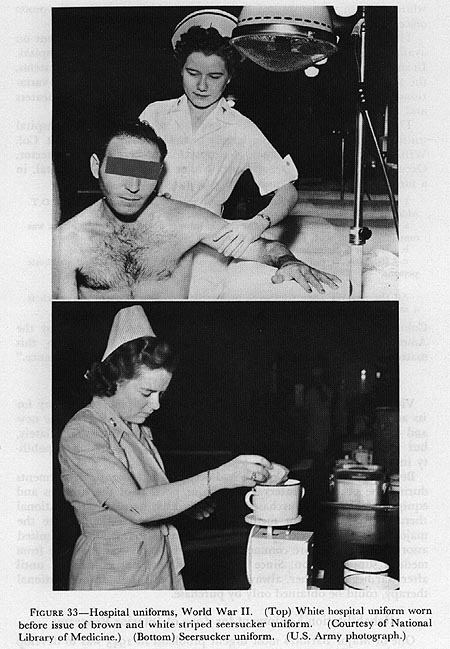
For a short time, dietitians and physical therapists in the United States wore a white hospital uniform until the supply of seersucker hospital uniforms was sufficient to meet the needs overseas and in the United States (fig. 33). It was anticipated that the use of the seersucker garment would be discontinued after the war and that the traditional
131
{kind=link}
132
white uniform with appropriate insignia would be worn by all women officers on duty in Army hospitals.
The uniform worn in oversea hospitals was somewhat dependent on availability of items and on the type of service rendered by the hospital. In spite of Army regulations pertaining to the wearing of uniform items, the supply was sometimes limited and, consequently, there were variations of both the street and hospital uniforms in the different theaters and areas and sometimes even within an area.
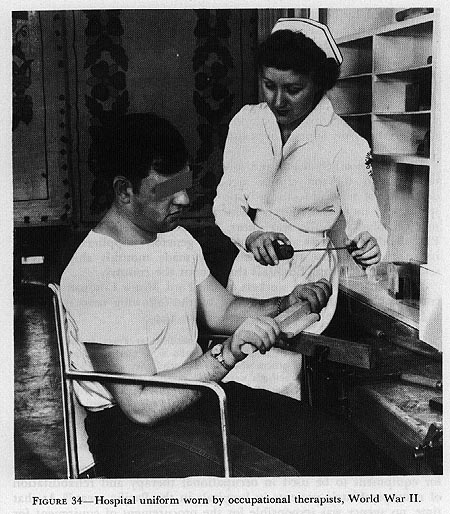
That occupational therapists wore an attractive white hospital uniform (fig. 34) may be due largely to the remarks made by Lt. Col. William C. Porter, MC, Chief, Neuropsychiatric Service, and Director, Occupational Therapy Department, Walter Reed General Hospital, in a memorandum to the Commanding Officer in April 1942:64
I earnestly recommend that the uniform prescribed for and worn by O.T. Aides at this hospital since 1918 be changed because:
a. It is clumsy, unflattering to the female form and suggests that its origin was contemporaneous with Florence Nightingale.
b. It is in 6 pieces and is a laundry nightmare.
c. Its color (a purplish blue) is depressing alike to normal and psychotic persons.
All the remarks made relative to present skirt apply to present cap which is a shapeless mass fabricated from organdy.
Colonel Porter urged adoption of the uniform recommended by the American Occupational Therapy Association and noted: "In this matter, the undersigned has received technical female assistance."
Vital to any program are the supplies and equipment necessary for its accomplishment. Early in the war, many items needed for the new and expanding hospital programs could not be obtained immediately, but this situation was gradually eliminated as production capability increased.
Because so few Army hospitals had occupational therapy departments during the peacetime interval, the major portion of the supplies and equipment had been purchased locally by each hospital. Occupational therapy items were not medical supply items of issue as were the majority of food service and physical therapy items. Only a limited assortment of the more commonly used hand tools was available from medical supply section. Since brace shops were not established until after war began, leather, always a basic item of supply in occupational therapy, could be obtained only by purchase.
Rehabilitation Equipment for Zone of Interior Programs
One of Major Barton`s most urgent problems in 1943 was to develop
64Memorandum, Lt. Col. William G. Porter, MC, Director, Occupational Therapy Department, Walter Reed General Hospital, to Commanding Officer, Walter Reed General Hospital, 29 Apr. 1942.
133
FIGURE 34-Hospital uniform worn by occupational therapists, World War II.
{kind=link}
a supply table of items necessary to open a clinic and sufficient to maintain the program. A list of activities and the necessary supplies had been prepared in 1942 by the National Research Council. To insure an adequate and up-to-date listing, additional lists of estimated requirements based on an experience factor were obtained from four Army general hospitals.65
The Medical Department occupational therapy equipment and supplies list was published in September 1943.66 It contained 378 items authorized for issue to all Army named general hospitals in the Zone of Interior. An annual cash allowance, ranging from $1,000 to $2,500
65Lawson General Hospital, Atlanta, Ga.; Letterman General Hospital, San Francisco. Calif.; Lovell General Hospital, Ayer, Mass.; and Walter Reed General Hospital, Washington, D.C.
66Medical Department Equipment List 9N464, 22 Sept. 1943.
134
(determined by hospital bed capacity), was also authorized for local purchase of items not included in the list.67
Program expansion soon made the original supply list inadequate, and, in July 1944, when cash allowances for supplemental purchases were discontinued to protect supplies and material intended for the civilian economy, the need for a new list became mandatory.68 The revised list, completed in August, included nearly 1,000 items69 and was supplemented by photographic equipment and supplies available through the Army Signal Corps and the authorization for local purchase of lumber.
There were other means and sources of supply through which many occupational therapy clinics met their needs. Among these were donations of new and salvage supplies from community groups, local stores, and industrial concerns which became interested in supporting medical phases of the war effort. The Rohm and Haas Company, Philadelphia, Pa., was among the most generous suppliers; beginning in 1944, in response to requests, they made monthly shipments of scrap plastic to Army hospitals throughout the country.
The management and workers of the Ford Motor Company showed considerable interest, as is witnessed by the following news item from a Detroit paper published in September 1944:
Parts for a complete machine shop to be installed at Percy Jones General Hospital for the benefit of disabled veterans who were mechanics before they entered the service and for others who wish to spend their convalescent period in studying machine shop methods were made possible by workers of Detroit`s Tool and Die Unit of Ford Local UAW-CIO [United Automobile Workers-Congress of Industrial Organizations]. A fine selection of tools to be used in the shop was donated by the Ford Motor Company.
Rehabilitation Equipment for Oversea Programs
Late in 1944, requests were received by the Surgeon General`s Office for equipment to be used in occupational therapy and rehabilitation of neuropsychiatric patients in hospitals in the Pacific areas.70 At that time, no agency was responsible for the procurement of equipment for rehabilitation and reconditioning programs in these oversea hospitals. Although the Special Services Division and the Red Cross had supplied much equipment which had been used in programs for mental patients overseas, neither could be held responsible for procuring equipment for a rehabilitation program since they were not authorized to engage in remedial treatment.
Two groups of patients were involved, those who could be returned
67Letter, Col. S. B. Hays, MC, Director, Distribution and Requirements Division, Office of The Surgeon General, to Commanding Officers and Medical Supply Officers, Supply Depots, 2 Oct. 1943, subject: Occupational Therapy Equipment.
68War Department Circular No. 310, 20 July 1944.
69Army Service Forces Catalog MED 10-23, 11 Jan. 1945.
70Memorandum, Maj. Ira H. Degenhardt, MC, to Chief, Operations Service, Office of The Surgeon General, 21 Dec. 1944, subject: Occupational Therapy and Rehabilitation of Patients Overseas.
135
to duty within the 120-day hospitalization limit and those to be evacuated to the United States. For the latter, inadequate airlift facilities had created a "huge backlog in some theaters" and it seemed advisable to "assure provision of minimal equipment for therapy for this group, pending their return, before they are beyond all salvage."
The Surgeon General recognized the benefit which would be derived from such a program, and, upon his recommendation, the Medical Department was given the responsibility of providing the needed supplies and equipment.71 By this action, The Surgeon General did not reverse his policy restricting occupational therapy to the Zone of Interior. Extensive occupational therapy equipment was not to be provided nor were additional personnel to be made available. A special catalog listing items for diversional therapy was prepared so that equipment could be requisitioned as convalescent aids.72 Through arrangement with Special Services Division, handicraft kits were made immediately available to oversea hospitals to serve as interim measures until the other equipment could be obtained.73
In order to provide a more efficient and coordinated management of the rehabilitation of patients in Army hospitals, on 4 April 1946, The Surgeon General placed the Physical Therapy Branch, the Occupational Therapy Branch, and the Physical Reconditioning Branch under the direction of the Director, Physical Medicine Consultants Division.74 This reorganization resulted in very few changes in the duties of the directors of physical and occupational therapy and their staff officers. Administrative procedures concerning physical and occupational therapists continued to be processed by the Military and Civilian Personnel Divisions, respectively. Under this reorganization, all professional matters were coordinated with the Director, Physical Medicine Consultants Division.
The establishment of physical medicine services in general hospitals was effected as soon as qualified medical officers were available in sufficient numbers to direct such services. The reorganization at the general hospital level vitally affected the status of many of the chief physical and occupational therapists. With frequent changes in medical direction and the many added activities during the war years, they had become more and more responsible for the administration of their clinics. In those instances where the directors of the new physical medicine services recognized and utilized the abilities of these chiefs, the readjustment to the reorganization presented few problems. Unfortunately, there were some situations in which the chiefs were
71Memorandum, Brig. Gen. R. W. Bliss, Chief, Operations Service, Office of The Surgeon General, for Commanding General, Army Service Forces, attention: Director, Planning Division, 5 Jan. 1945, subject: Reconditioning Overseas, with 1st indorsement thereto, 25 Jan. 1945.
72Army Service Forces Catalog MED 10-23, April 1945.
73Loughlin, Richard L.: History of Physical Medicine, p. 154. [Official record.]
74Office Order No. 111, Office of The Surgeon General, U.S. Army, 4 Apr. 1946.
136
relieved of their administrative functions and certain of their professional responsibilities, producing a situation not conducive to good morale or efficient operations.
By far, the most drastic change occurred in the relationship of the chief physical therapist to the chiefs of the other hospital services. Formerly, she had been considered a staff member and, as such, attended hospital staff conferences and had direct contacts with the chiefs of services on matters pertaining to patient care. Under the reorganization, she was relieved of these duties, thereby markedly decreasing her professional status in the hospital organization. This influenced some outstanding physical therapists in their decision not to make application for commission in the Regular Army in 1947.
The organization in general hospitals provided for an administrative officer, usually a member of the Medical Administrative Corps (later the Medical Service Corps). Many of these officers were inexperienced in matters which were routine for the physical and occupational therapists. Where there was proper orientation concerning this reorganization, the administrative officer relieved the chief therapists of many time-consuming duties pertaining to property, supplies, and custodial service, thus permitting them to devote more time to professional matters. Although this was an advantage in many respects, it was also a disadvantage. Newly appointed physical or occupational therapists in general hospitals had no opportunity to gain experience in administrative functions which they would be expected to assume when they were assigned to station hospitals in this country and to hospitals overseas where physical medicine services did not exist.
![]()