



The Fight for the Hürtgen Forest
EXTRACTED FROM
UNITED STATES ARMY IN WORLD WAR II
THE TECHNICAL SERVICES
THE MEDICAL DEPARTMENT:
MEDICAL SERVICE IN THE EUROPEAN THEATER OF OPERATIONS
by Graham A. Cosmas
and
Albert E. Cowdrey
U.S. Army Center of Military History
Washington, DC: 1992
CHAPTER XI
Hard Fighting at the West Wall
During the autumn and early winter of 1944 the Allied armies reorganized and drove forward all along a front that now extended from the Channel to the Swiss border. They collided with a revived and reinforced Wehrmacht in what became at many points a bitter, costly battle of attrition. In this battle the European Theater field army medical service, taking the strain of a continuous high casualty rate, reached full development in organization and technique.
By mid-September the U.S. 12th and 6th Army Groups formed respectively the center and right of the Allied line. They included twenty-seven of the forty-nine divisions then at the disposal of SHAEF on the Continent. Americans in the army groups and their supporting air and service forces made up about half of the 2 million men under Eisenhower`s command. The American army groups paused at the West Wall and the Moselle, to build up their attenuated supply system and to reorganize for the new offensive. When these troop rearrangements were completed late in October, the 12th Army Group had three armies on line from left to right, the Ninth, First, and Third. To the right of the 12th Army Group General Devers` 6th Army Group, which came under
SHAEF`s operational control on 15 September, placed the two corps of the French First Army on its right wing and the U.S. Seventh Army, composed only of the three-division VI Corps, on its left. SHAEF, late in September, reinforced the Seventh Army with the rightmost corps of the Third Army and also with new divisions shipped directly from America to southern France.1
The American and French armies, and the British and Canadian elements of Montgomery`s 21 Army Group on the Allied left, launched their new attacks between 8 and 16
November. SHAEF, still reflecting some of the optimism of the summer, when hopes for an early German collapse had run high, set ambitious objectives for this drive: reaching the Rhine, destroying the German armies west of that river, and perhaps securing bridgeheads across it. At the minimum, a continued fall-winter offensive would deny the enemy leisure to rebuild his armies, strengthen his for-
355
tifications, and introduce new weapons. The Germans, however, had used all too well what breathing space the September and October pause in Allied attacks had given them. By the time the new offensive started, their desperate late-summer mobilization had produced enough troops to contain the Allied advance while accumulating a 25-division reserve for Hitler`s projected grand counterattack.
Gone were the days of swift breakthroughs and hell-for-leather armor exploitation. The battle became one of attrition, as British, French, and American divisions crawled forward against tenacious resistance. The Germans drew upon the hard-learned defensive experience of five years of war and made lavish, effective use mines and artillery; they exacted fearful price in men and time for every town, village, ridgeline, river crossing, and pillbox. The rain, snow, and freezing temperatures of one of the earliest and severest winters on record in that part of Europe reduced Allied mobility and air support and added to the misery of the combatants on both sides.
Nevertheless, through hard pounding and steady pressure the Allies made limited territorial gains. On their left wing the British Second and Canadian First Armies conquered the German forces blocking the seaward approaches to Antwerp, thus opening that great port to shorten Allied supply lines; then they liberated most of southern Holland. The U.S. Ninth and First Armies, attacking side by side, forced their way well inside the German frontier and drove almost to the Roer River, the last major water barrier between them and the Rhine.
On the southern flank of this attack the First Army fought possibly the bitterest battle of the campaign for the Huertgen Forest, a gloomy roadless tangle of fir trees, hills, and ravines. Although the Americans cleared the woodlands in the end, combat for the infantrymen of five divisions who battled there was a nightmare of endless minefields, treetop shellbursts, hidden pillboxes and machine-gun nests, and fierce German counterattacks. A rifle company in the Huertgen Forest could lose 100-200 percent of its original strength in a week`s fighting; battalion and company officers and NCOs were killed and wounded or broke down in near-disastrous proportions. A 4th Division soldier summed it up:
You can`t get all of the dead because you can`t find them, and they stay there to remind the guys advancing as to what might hit them. You can`t get protection. You can`t see. You can`t get fields of fire. The trees are slashed like a scythe by artillery. Everything is tangled. You can scarcely walk. Everybody is cold and wet, and the mixture of cold rain and sleet keeps falling. Then they jump off again and soon there is only a handful of the old men left.2
South of the Ardennes the enemy defended with similar tenacity, but American troops gained more ground. Patton`s Third Army crossed the rain-swollen Moselle in force; took Metz on 22 November; and a month later, after liberating 5,000 square miles of Lorraine, reached the
German border at the Saar River. On the right of the Third Army the 6th
356
Army Group cleared the west bank of the Rhine from the Swiss border to Strasbourg, except for a German-held bridgehead around Colmar. While the French First Army battered at this pocket, the U.S. Seventh Army in early December pushed northeastward though the old Maginot Line
fortifications and prepared to assault the West Wall. The American armies thus captured significant territory, though less than their commanders had hoped to secure. In addition, they inflicted tens of thousands of German casualties, destroyed large quantities of equipment, and took almost 200,000 prisoners.3
The four American armies paid a high price for this ground and the wearing down of German forces. Between them, they suffered over 140,000 battle casualties, more than 85 percent of them in the infantry rifle companies. Among the approximately 100,000 wounded, the pattern
of cause and location of injury resembled that in earlier phases of the campaign. About 65 percent fell victim to shell, bomb, and grenade fragments, and a similar proportion were hit in
the arms and legs. Besides combat casualties, army hospitals during November and December admitted another 150,000 cases of injury, sickness, and combat fatigue. The cold damp weather increased the incidence of respiratory ailments. An epidemic of trenchfoot crowded clearing stations and evacuation hospitals with crippled soldiers, many permanently incapacitated for combat duty, and further diminished the already casualty-thinned ranks of the infantry.4
Organizing for the Offensive
Redeployments and exchange of medical units accompanied the reorganization of the American armies for the November offensive. New ground force medical formations continued to arrive in the theater, increasing the number of medical personnel in the armies to over 65,000 by mid-December. The 12th and 6th Army Group surgeons, in consultation with those of the armies and with Generals Kenner and Hawley, distributed the new arrivals and reshuffled the forces already on the ground to give each army a medical complement proportional to its strength. 5
The Ninth Army, for example, initially entered the line in the Ardennes with the 64th Medical Group, sup-
357
porting the VIII Corps, as well as several former Third Army field and evacuation hospitals and other units taken over in Brittany. When it moved to Holland and joined the12th Army Group`s left wing, the army relinquished these organizations, except for two field hospitals, to the First Army and assumed command in turn of the 31st Medical Group, which supported the XIX Corps (taken over from the First Army) and three evacuation hospitals. The new army also inherited several evacuation hospitals and field hospital platoons serving American divisions, including the 82d and 101st, which were fighting in Holland under 21 Army Group in the aftermath of
MARKET-GARDEN. Other Ninth Army medical units, arriving from the United States and Great Britain, assembled at concentration areas in France and Belgium and then moved into Holland to support the army`s second corps, the XIII, when it began operations late in November.6
The Seventh Army came ashore on the Riviera with a complement of medical battalions, of ambulance, clearing, and collecting companies, and of field and evacuation hospitals sufficient only for a single corps. As SHAEF added to that army`s combat strength, it also reinforced the medical service-a process involving multilateral consultations among the surgeons of the two army groups, four field armies, and two separate communications zones. During September
the Seventh Army acquired from the Third Army an additional medical battalion headquarters, three collecting companies, a clearing company, and a field hospital, as well as the Third`s XV Corps. SHAEF at the same time directed the European Theater and 12th Army Group to provide the southern army with three additional ambulance companies, three evacuation hospitals, a depot company, and part of an auxiliary surgical group. Both headquarters complied, in part by transferring units already in France to the 6th Army Group and in part by diverting new units then still in the continuing flow of troops across the Atlantic. Late in November, with planning under way to expand Seventh Army to three corps and nine divisions, SHAEF called on the northern forces for still more field medical Units, and they again responded with redeployments, to include, whenever possible, redirecting reinforcements already at sea to the French Mediterranean ports.
Augmentation of the Seventh Army medical service did not go altogether smoothly. Colonel Gorby, the l2th`s surgeon, resisted turning over an auxiliary surgical group, insisting he needed it for his own still expanding army group, but in the end he complied with SHAEF directions. The 6th Army Group surgeon, Col. Oscar S. Reeder, MC, and the Seventh Army surgeon, Colonel Rudolph, at times disagreed in estimating their requirements. Reeder, for example, accepted a medical group headquarters, taken from the Third Army, for which the Seventh Army surgeon had no use, but withdrew a request for a gas treatment battalion that Rudolph wanted. The medical units assigned
358
to the Seventh Army took a while to arrive. Those allocated in September, for instance, joined only in late November. The three evacuation hospitals that arrived immediately after being activated in the United States needed additional training before they could become operational. While the unwanted medical group headquarters, the 67th, waited for a new assignment, the Seventh Army conducted most of the autumn campaign with a shortage of field and evacuation hospitals, only partially alleviated by borrowing from the southern communications zone. These difficulties, however, were only temporary.
By late December the Seventh Army included ten evacuation and four field hospitals, a convalescent hospital, portions of two auxiliary surgical groups, six separate medical battalions with attached collecting and clearing companies, six ambulance companies, a depot company, and assorted laboratory and veterinary units (the latter loaned to the French First Army to care for its pack animals).7
The French First Army, the other major component of the 6th Army Group, possessed its own separate medical service. This army, organized and equipped in North Africa with American assistance, included a full complement of ground forces medical units with American tables of organization and equipment and with French personnel. Its hospitalization and evacuation system closely resembled those of the U.S. field armies. By late 1944 the French had about 7,000 field and evacuation hospital beds in operation for their two corps and seven divisions; up to that point in the campaign they had cared for about 23,000 casualties. They evacuated their long-term patients by rail to fixed hospitals, many of them civilian, in liberated southern France and had their own supporting communications zone organization, Base 901, in the same area. The French relied heavily on American medical supplies, which they delivered to their forward units through their own depot system. General Kenner, after a mid-December inspection, pronounced the French First Army medical situation "quite satisfactory, sufficient medical units are available, and civilian facilities and personnel augment them throughout the area."8
Except in allocating medical units, the army group surgeons-Colonel Gorby of the 12th and Colonel Reeder of the 6th-guided their subordinate army surgeons with a loose rein. The group surgeons confined their activities largely to keeping informed about operations, collecting medical reports and statistics, disseminating and interpreting SHAEF
359
and theater medical directives, and occasionally assisting the army surgeons in dealing with COMZ. However, they encouraged the armies to work directly with the Communications Zone whenever possible on evacuation and supply matters, and most of the time the army surgeons did so. Colonel Reeder`s small (two officers and three enlisted men) medical section was especially limited in functions and influence. It had only one American army to oversee and, until May 1945, was submerged within the group G-4 office instead of constituting a separate special staff section.9
Day-to-day direction of activities both administrative and clinical rested primarily with the army surgeons and their fifty- to sixty-person staffs. The surgeons of all four had satisfactory working relationships with their army commanders, generally paid little attention to the medical service except on the exceedingly rare occasions when something went drastically wrong. Usually located with the forward, or tactical, echelon of army headquarters, the surgeons participated in all stages of operational planning. For practical purposes, they had operational control of nondivisional medical units, although the formal definition of authority varied from army to army. Their medical and surgical consultants supervised patient care and enforced the principles of the ETO Manual of Therapy, as well as apportioning auxiliary surgical teams among army hospitals. Army surgeons spent much effort on communications. In the 12th Army Group they maintained liaison officers at group headquarters, and they had attached to them liaison officers from the Advance Section. Army surgeons kept in touch with their own medical units by telephone and courier. The Third Army surgeon at Nancy, for example, had eleven telephones in his office and nineteen drivers and vehicles at his disposal, all in constant use.10
For the army surgeons, and for those at corps and division levels, planning and coordinating medical support for the November-December offensive was a comparatively straightforward task. The surgeons confronted a problem similar to that in the hedgerow battles: evacuation of a large but steady volume of casualties over relatively short distances from slowly advancing combat units. Until the German Ardennes counterstroke, the Allies held the tactical initiative; hence, surgeons generally could forecast accurately the rates and locations of casualties and the supply and evacuation requirements of each stage of the attack. The absence of major breakthroughs, although disappointing to tactical com-
360
manders, simplified the army medical service`s task by reducing the need to move large installations. Third Army evacuation hospitals, for example, changed position an average of slightly more than once each month during this offensive; in the pursuit they had moved three times as often.
The army medical service, accordingly, readily took the strain of the hard autumn and winter fighting. Army medical people at each link in the evacuation chain elaborated upon the expedients and adaptations of standard procedure introduced earlier in the campaign; they relearned old lessons and occasionally learned new ones. Above all, for army medics at every echelon the November and early December battles meant long hours of hard labor, physical and emotional stress, and for some deadly danger.11
Medics on the Line
Divisional unit detachments and medical battalions at the forward end of the entire evacuation chain collected casualties under fire, stabilized their condition, and started them toward safety and healing in the rear. Increasingly, by late 1944, the latter function--evacuation--was becoming the primary one for all medical personnel forward of the clearing stations. By army policy medics confined treatment to the bare minimum needed to fit casualties for immediate further transportation: controlling bleeding, pain, and infection; immobilizing broken limbs; and administering plasma. 12

MEDICS ON THE LINE
First Aid
Medical treatment of wounded soldiers began even before they reached their battalion aid stations. Casualties received first aid at or near the spot on the battlefield where they were injured, administered either by themselves and their buddies or, much more often, by their company aidmen. Each soldier carried an indi-
361
vidual first aid packet, containing field dressings and sulfa powder and tablets, and was supposed to know how to improvise and apply splints and tourniquets. First aid procedures called for a wounded man, if able, to seek protection from fire, examine his injury and assess its severity, sprinkle it with sulfa powder, apply a dressing, and swallow his sulfa tablets. Then he was to get back to the aid station on his own or call for the aidman.
In practice, a large proportion of the wounded forgot to do, or not do, any number of these things. Of casualties polled in COMZ general hospitals, for example, about one-third did not take their sulfa pills before they reached the aid station, claiming that they lacked water to wash them down; doubted the tablets` usefulness; or were incapacitated by their injuries. Soldiers often did not have their belt first aid packets on their persons when hit. "They`d take them off," an aidman reported, "for example to be more comfortable in a fox hole, and we`ll usually find the belts [and packets] lying close by." Hurt, frightened soldiers yelled frantically for the aidman even when only slightly wounded and capable of leaving the field under their own power. Many, in panic, further injured themselves, at times fatally. A company aidman recalled the actions of a lieutenant. He got hit and just had a little bit of gut hanging out and he sits up and lies down and hollers and thinks he is going to die and we fix him up but he`s still excited and pretty soon air gets in and he dies. That same day there`s a Jerry with all his guts hanging out. He puts his hand down there and holds it in. We get him to the aid station and we hear later that the son-of-a-bitch still lives. He just held it there and didn`t get excited.13
Fortunately, comparatively few wounded men-only one in five, according to one hospital survey-had to give themselves first aid. Most found a company aidman at their sides within less than half an hour of being hit. Besides bandaging, splinting, applying tourniquets, administering sulfa powder and tablets, and injecting morphine, aidmen were supposed to fill out an emergency medical tag (EMT) for each casualty, providing the basic record of his identity and initial treatment. Many divisions in practice transferred this chore to the battalion aid stations, for the company medics, amid the urgency and danger of combat, were hardly in an ideal position to do paper work. Company aidmen had a deserved reputation for bravery but they complained that some of their heroics were unnecessary, the result of panic calls for help by the slightly injured or of poor judgment by line officers in sending out their medics under fire. One medic commented: "If a man is hit, he`s hit, and it may be better to leave him there for a while than to send the aid man to him on a suicide job for example, I`ve seen it done when mortars were pounding the area and every foot was covered with [machine-gun] fire." 14
362

PREPARING AN EMERGENCY MEDICAL TAG
Most demands for courage on the part of aidmen, however, were legitimate and essential to their mission, and the medics responded with dedication and self-sacrifice. During the Third Army fighting along the Moselle, for example, Technician 5th Class Alfred L. Wilson, a company aidman in the 328th Infantry, moved about under heavy shelling treating his unit`s many wounded until badly hurt himself. He refused evacuation and, in great pain and slowly bleeding to death, continued dragging himself from one casualty to the next. Finally too weak to move, he instructed other soldiers in giving first aid until unconsciousness overcame him. His unit credited Wilson, who received a posthumous Medal of Honor, with helping to save the lives of at least ten men. A 4th Division captain reported of another aidman in the Huertgen Forest who similarly stayed on duty after being injured: "This man was perhaps an even greater morale aid than a physical aid" to the hard-pressed riflemen around him.15
363
Not surprisingly, in the light of such performance, aidmen were among the most popular and respected soldiers in their companies. Aidmen and infantry troops alike bitterly resented the War Department refusal-based on the need to maintain the medics` Geneva Convention noncombatant status-to grant eligible enlisted medics the Combat Infantryman Badge and the ten dollars a month extra pay that went with it. In some ETO divisions riflemen collected money from their own wages to give their aidmen the combat bonus. The War Department, however, did not remedy this inequity until barely two months before V-E Day. Medical Department soldiers-mostly aidmen and litter bearers-did collect their share of decorations for valor. Four ETO enlisted medics besides Wilson received Medals of Honor; hundreds of others won Silver or Bronze Stars. 16
In the judgment of doctors farther to the rear, aidmen and front-line troops gave generally competent first aid, although they made a few persistent errors. Soldiers-whether medical or nonmedical-regularly misused tourniquets. They applied them unnecessarily; left them unloosened for too long; and occasionally evacuated patients with tourniquets concealed by blankets or clothing, and hence not discovered until the limb was doomed. Trying to prevent such abuses, the Seventh Army surgeon directed that the "sole indication" for applying a tourniquet should be "active spurting hemorrhage from a major artery" and that medics in the field or at battalion aid stations should note the presence of a tourniquet on a patient`s EMT in capital letters. With the morphine Syrette then in use, aidmen easily could overdose casualties, especially in cold weather when slow blood circulation delayed absorption of the initial shot and the patient received more at an aid or collecting station. To guard against such mistakes, front-line medics who did not fill out EMTs often attached their used morphine Syrettes to soldiers` clothing before evacuating them. In the First Army the surgeon, Colonel Rogers, recommended abandonment of the practice of sprinkling sulfa powder on open fresh wounds as an anti-infection precaution. Combined with the taking of sulfa pills, this treatment resulted in excessive doses, and it also made wounds generally dirtier without reaching the deepest portions most in need of prophylaxis.17
364
Evacuation
From the place on the battlefield where the aidmen treated a casualty and marked his position, ETO divisional medical installations and hence the chain of evacuation stretched rearward over a considerable distance. By late 1944 battalion aid stations typically set up at least a mile behind the engaged infantry and armor elements, to reduce losses from artillery and mortar fire among essential, hard-to-replace doctors and technicians. Collecting stations usually took position about a mile back of the aid stations. Clearing stations remained 3 to as many as 15 miles behind the fighting line, to be free of the patient-disturbing noise and counterbattery fire danger or their own corps and division artillery.18
Mass movement of patients over these distances was possible largely because the divisions, by late1944, in effect had motorized their entire chain of evacuation. Since the Battle of the Hedgerows they had used collecting company ambulances, supplemented by trucks for walking wounded, to evacuate their battalion aid stations. By late autumn they routinely extended motor transport forward of the aid stations as well, whenever possible right to the place where casualties lay on the battlefield. Medics now used jeeps, belonging to battalion aid stations and collecting companies, in preference to litter bearers, for moving wounded in the forward areas. Fitted with brackets for carrying litters, these small sturdy vehicles could go most places men on foot could; they could accommodate two or three litters each, and as many ambulatory patients as ingenious drivers could crowd on board. One 4th Division litter platoon commander claimed to have hauled fourteen walking wounded on a single trip. On more typical runs, he recalled, "there would be . . . two litter cases side by side on the rear half of the jeep, then usually one across the hood, and then I would have sitting beside me a severely wounded man, or a couple of them, who could. . . sit up." 19
When their jeeps bogged down in mud and snow, medics often switched to the M-29 Weasel, a small tracked cargo vehicle that had about the same litter capacity as the jeep. Armored division surgeons used light tanks and tank retrievers to move their wounded over ground impassable to jeeps and regular ambulances. On one occasion the 5th Armored Division picked up casualties on the field in medium tanks when heavy shelling prevented any other approach to them. The Shermans maneuvered astride the wounded men; then the crews drew the casualties up inside the tanks through the escape hatches in the bottoms of the hulls. During the Third Army attack on Metz the 95th Infantry Division temporarily pressed an artillery spotter plane into service to fly wounded directly off the battlefield from a point where minefields and enemy fire blocked evacuation by any other means. The aircraft, with a regimental surgeon riding with the pilot to select cases,
365

LITTERBEARERS MEETING THE CHALLENGE OF THE HUERTGEN FIGHTING
lifted out nine men in the same number of trips. Clearly, machines rather than human muscle now were moving most casualties most of the time. 20
Divisions were insatiable consumers of medical manpower, especially when weather and terrain forced them to rely extensively on litterbearers forward of battalion aid stations. The task of litter-bearing in such circumstances was both dangerous and exhausting, for the distances litterbearers had to traverse-often over rugged, wooded country-ranged from 1,000 yards to 4 miles. In the Huertgen Forest 16th Infantry bearers, according to the regimental surgeon, "would work until they were exhausted and then drop. A twelve hour relief and they`d be off on another seventy-two hour shift." Bearers displayed dedication comparable to that of the aidmen with whom they closely cooperated. A 4th Division enlisted medic made two 1,000-yard hauls after a glancing blow from a shell fragment had fractured his skull. Yet even the bravest and strongest men needed frequent rest, and litterbearers suffered a steady drain of casualties from enemy fire and mines. A few broke down emotionally. Another 4th Division litterbearer, after carry-
366
ing to the rear on his back two men from an infantry company with which he had worked for some time and to which he had grown closely attached, began muttering, "They`re killing my boys; they`re killing my boys." He tried to find a rifle with which to fight back and "had to be evacuated for combat exhaustion." 21
Infantry battalion and collecting company litterbearers (the latter all but supplanted by ambulances for work to the rear of the aid stations) customarily combined forces to remove wounded from the battlefield. They were far too few for the job during intense combat and when weather, terrain, or the tactical situation prevented vehicles from assisting them. The Huertgen fighting, in particular, absorbed bearers at an almost intolerable rate. The 1st Infantry Division, during its time in the forest, used 240 additional litterbearers; the 4th Division employed 140. Under prearranged procedures division surgeons obtained these extra men, and also casualty replacements, from their corps medical battalions and the army medical groups. These units drafted bearers from their own attached organizations and, in emergencies, drew upon any other medical personnel within reach. The 68th Medical Group, for example, which supported the VII Corps, provided infantry divisions in the Huertgen Forest with over 450 reinforcement bearers, including the enlisted personnel of two entire collecting companies. Running out of spare medical troops, the group obtained 190 nonmedical infantry replacements from one of the depots. It issued them Red Cross brassards; sketchily trained them in first aid, evacuation, and Geneva Convention rights and duties; and threw them into the line for several weeks. On another occasion the Advance Section sent the First Army a contingent of litterbearers combed out of staging general hospitals. Even with all this extra help, the rifle companies often had to draft combat soldiers from their own thin ranks to carry wounded at least part of the way to their battalion aid stations. These expedients met the immediate requirements. The necessity for them, however, pointed up the inadequacy of the existing division complement of bearers and also underscored how indispensable, under the prevailing conditions, evacuation by vehicle had become. 22
With so much first aid being performed on the field, battalion aid stations concentrated more on evacuating casualties than on treating them. The aid stations, by the time the November offensive began, had honed and perfected their operational tech-
367

BATTALION AID STATION PERSONNEL READYING CASUALTIES for the next stage of their rearward evacuation
niques. Because the stations, for safety reasons, had to keep their distance from the rifle companies, battalion surgeons often established small advance collecting points nearer the infantry. These typically consisted of an officer (frequently the assistant battalion surgeon), a few litter teams, and a couple of jeep ambulances. They gathered casualties and evacuated them to the main aid stations. The latter almost invariably found shelter under roofs and preferably underground, in solidly constructed cellars or abandoned dugouts, which afforded protection from shelling as well as the elements. To better direct evacuation, battalion surgeons, whenever they could, established telephone or radio contact with the company command posts. At night the telephone wires, and sometimes white tape stretched along the ground, guided the rearward traffic of litterbearers and walking wounded. When casualties reached them, the surgeons and their enlisted technicians checked and replaced dressings, splints, and tourniquets and dispensed additional morphine. They filled out EMTs if company aidmen had not done so. They normally administered the first plasma the wounded received. When casualties came through in large numbers, the aid stations, to get patients out quickly, suspended tagging the wounded and limited transfusion and resuscitation to the minimum re-
368
quired to keep injured men alive during the next stage of their rearward journeys. In the First Army, especially, "the rule was to sacrifice full resuscitation for early evacuation." 23
By the time the autumn battles began, most battalions had Medical Administrative Corps (MAC) officers as assistant surgeons. Usually sent into replace Medical Corps (MC) casualties, the MAC lieutenants, by most accounts, performed creditably. The regimental surgeon of the 16th Infantry, for example, commented: "The doctors could take care of the wounded and the [MAC] lieutenants could keep the evacuation going. . . . They had been well taught in first aid and-were skillful in bandaging and splinting and were able to assist the surgeons in their work." At least one battalion surgeon, in the 3d Infantry Division, proposed replacing all MCs at battalion level with MACs. He argued that little actual need existed in the battalions for the doctors` professional skills and that regimental surgeons, if necessary, could assist their aid stations in diagnosing and treating difficult cases. The armies, nevertheless, retained their MC battalion surgeons.24
Divisional collecting companies worked closely in evacuation with the regimental and battalion detachments, often pooling men and equipment with them, as in litter-bearing forward of the aid stations. A collecting company normally operated continuously with the same infantry regiment. During action the company set up its station as close to the regimental command post as safety and the maintenance of noncombatant status allowed and also tied into the regimental telephone system for direct communications with the battalion surgeons. Many companies found it convenient to divide their ambulances into two groups. One, dispatched by an advance loading post, shuttled between aid stations and the collecting station; the second ambulance element picked up patients at the collecting station for the usually longer run to the clearing company and field hospital platoon. Under this arrangement, drivers in the forward contingent gained familiarity with the frequently tortuous, hazardous routes to the aid stations. Collecting station personnel at the same time gave patients whatever refreshment and stabilizing treatment they needed and grouped them into efficient ambulance loads for the next stage of their journey.25
In especially difficult tactical situations, infantry battalion and collecting company medics resorted to all manner of expedients to keep evacuation going. Such was the case during
369
the disastrous attack of the 28th Infantry Division in the Huertgen Forest early in November. In this operation the 1st and 3d Battalions of the 112th Infantry seized a salient of key high ground around the villages of Schmidt and Kommerscheidt, deep in German-held territory, and then came under heavy infantry, tank, and artillery counterattack from three sides. The battalions` route of supply and evacuation consisted of a narrow trail, muddy from the incessant rain, which wound its way down into the gorge of the Kall River and then up another ridge to the American-held town of Vossenack, some 2 miles northwest of Kommerscheidt. Vossenack itself was under intense German infantry attack, as well as artillery bombardment from high ground to its northeast.
The battalion surgeons, Captains Paschal A. Linguiti, MC, of the 1st and Michael De Marco, MC, of the 3d, faced a difficult evacuation problem. Ambulances from their supporting collecting company-C, 103d Medical Battalion, which had its station near Vossenack-could not negotiate the trail across the Kall. Hence, the battalions had to send casualties back in jeeps and weasels (the division had large numbers of the latter attached for this operation) to an ambulance loading point near the top of the ridge at Vossenack. Linguiti initially set up his 1st Battalion aid station in a basement in Kommerscheidt; De Marco, with his 3d Battalion station, took position about a mile farther to the rear, west of the Kall, sheltered in a cave-like 18-by-12-foot dugout built into the steep hillside that bordered the trail. The station in Kommerscheidt in effect functioned as an advance collecting point; it sent wounded in whatever vehicles were available to the 3d Battalion installation for relay on up the hill to the ambulance loading point.
As the American position at Schmidt and Kommerscheidt deteriorated, so did the evacuation situation. Linguiti and De Marco consolidated their two aid stations in the dugout. Disabled American tanks and other vehicles along the trail and German shelling of the ambulance loading point effectively halted evacuation of all but walking wounded, whom the surgeons sent to the rear in parties led by medical troops. Litter patients, eventually about sixty-five of them, accumulated in and around the dugout. Linguiti and De Marco cared for them as best they could, helped by their MAC assistant surgeons, the battalion chaplains, a dwinding contingent of enlisted medics, and infantry stragglers whom the surgeons disarmed and pressed into service as attendants and litterbearers. The medics had adequate food for their patients and enough medical supplies for what little treatment they were attempting, but they were short of blankets and shelter. The dugout could accommodate only about twenty-five patients. The remainder, wrapped in what coverings were available, lay along the trail in the cold, rain, and snow, protected by soldiers holding Red Cross flags. This protection was needed because, during the final days of the battle, German troops infiltrating behind the 1st and 3d Battalions periodically visited the aid station. However, except for announcing that the medics were captured and making sure that no armed Americans were present, the Germans left the facility
370
unmolested. They allowed American walking wounded from Kommerscheidt to reach the station and at one point offered Linguiti and De Marco food and medicine, which the surgeons declined. Nevertheless, the Germans did confiscate the aid station`s few vehicles.
After the survivors of the 1st and 3d Battalions withdrew from Kommerscheidt on the night of 8-9 November, in the process inundating the aid station with a final stream of walking and litter-borne casualties, Linguiti and De Marco and their staff and patients remained within German lines. The enemy evidently had neither the means nor the inclination to remove the American doctors and wounded. The local German commander agreed to a truce, proposed by the 112th Infantry`s surgeon, Maj. Albert L. Berndt, MC, for removal of both sides` casualties from the Kall valley. Under this arrangement the battalion surgeons, after further adventures with a German unit not party to the truce, eventually managed to assemble a makeshift truck and weasel convoy to carry themselves, the other medical officers and men, the chaplains, and the severely wounded back to American lines. However, they had to surrender the lightly wounded and their nonmedical personnel as prisoners of war. 26
The experience of Captains Linguiti and De Marco, besides illustrating the vicissitudes of forward area evacuation, pointed up another circumstance of the campaign very important to Army medics: the enemy`s continued adherence to the international laws and customs of war affecting wounded and those who cared for them on the battlefield. As had been true since Normandy, German troops, at least until the Ardennes offensive, rarely engaged in aimed fire at aidmen, litterbearers, or Red Cross-marked medical facilities. Infantry of both sides, on many occasions, temporarily ceased fire or made short local truces to allow their medics to clear casualties from the field. During a counterattack in the Huertgen Forest the Germans captured a 22d Infantry, 4th Division, aidman. They put him to work caring for American casualties and then employed him, and a German medical soldier, to carry the wounded GIs to a point near American lines while both sides held their fire. American units provided reciprocal courtesies. During an attack at Frenzerburg Castle on the fringes of the Huertgen Forest, for instance, elements of the 47th Infantry, 9th Division, observed a three-hour truce so that a German ambulance could remove thirty severely wounded enemy defenders. On the other hand, the 47th Infantry took prisoner eight less seriously injured Germans who would have been able to return to combat. 27
371

WORKHORSES OF BATTLEFIELD EVACUATION. Much of the work for transporting casualties fell to the jeep, fitted with brackets for carrying litters [above]. When these sturdy vehicles bogged down in mud and heavy snow, medics switched to the tracked M-29 Weasel [below].

372
In response to repeated claims by German prisoners that they often could not see the Red Cross arm brassard on the battlefield, the army medical service adopted more conspicuous Geneva Convention markings. Late in November the 12th Army Group, at the request of Colonel Shambora, the Ninth Army surgeon, formally authorized medical troops to paint large red crosses in white fields on their helmets, a practice already widespread among aidmen and litterbearers. The 7th Armored Division determined in tests that men so marked stood out from other soldiers at distances of up to 750 yards. Medics in some divisions either carried Red Cross flags with which to signal their identity when moving under fire or wore improvised Red Cross tabards and vests modeled on those of German aidmen. The army medical service also scrupulously guarded its noncombatant status against encroachment by its own side. Division surgeons and other medical officers registered vehement protest against use of Red Cross-marked vehicles for nonmedical purposes and against the placing of artillery, tanks, and combat-related supplies too close to their aid stations. More conspicuous Geneva Convention insignia probably saved the lives of many front-line medics in the mud, snow, and mist of the autumn and winter battlefields, and mutual respect for international usage diminished somewhat the dangers they faced. Hazards, however, remained in plenty. As one medical soldier put it, "Artillery and mortars don`t know the difference between a rifleman and a guy with a red cross brassard on his arm." 28
From Battle Line to Hospitals
To the rear of the divisions the medical organizations of the different armies retained the varying forms they had assumed at the end of the pursuit. The First Army, and the Ninth Army following its example, attached most nondivisional medical units except hospitals to their medical groups; the First Army also attached to its groups the field hospitals working with the division clearing stations. These armies placed one medical group in charge of evacuation and various other support activities for each of their corps, with an area of responsibility extending from the division rear boundaries to that of the army. The Third Army, by contrast, employed all but one of its medical groups strictly for evacuation, attaching only ambulance units to them; one group evacuated the division clearing stations of each corps and an additional group transferred patients among and to the rear of evacuation and convalescent hospitals. The Third Army`s employment of its medical groups seemed to General Hawley and others to be inefficient. Indeed,
373
the commander of one of the army`s groups pointed out that his headquarters, with two medical battalions attached, during most of the campaign controlled only four ambulance companies. The Seventh Army got along without medical groups altogether. Separate medical battalions, often with as many as eight companies attached, evacuated its corps, and the army surgeon directly controlled hospitals and other facilities. Offered a medical group from the Third Army, the Seventh Army surgeon, Colonel Rudolph, refused it. He declared that "no necessity existed for such a unit since the functions of . . . a group could be and were being performed either by the battalion clearing corps or by the Operations Section of the Surgeon`s Office." Whatever their differences and drawbacks, all these systems worked well enough that neither theater nor army group surgeons considered it necessary to interfere with them. 29
Especially in the First and Ninth Armies, medical groups performed a number of miscellaneous but vital functions. They operated dispensaries and prophylactic stations for nondivisional army troops. They deployed collecting and clearing companies to reinforce evacuation hospitals; provided additional litterbearers to the divisions; and collected trucks to move the larger army medical units. Because the groups` role in evacuation required constant liaison with tactical headquarters, these units served as communications centers and intelligence clearinghouses for other army medical service organizations. The commander of the 68th Medical Group in the First Army, for example, opened up his morning staff briefing on the military situation and evacuation plans to all medical unit commanders in his area of operations. Other groups distributed periodical news and information bulletins, one inevitably entitled "Poop from Group." The 69th Medical Group in the Third Army ran a daily courier service, which collected statistical reports from all the hospitals for the army surgeon and distributed his messages and circulars to every medical facility. Similarly, in the Seventh Army the medical battalions also augmented hospitals and reinforced the division medical service, as well as operated a neuropsychiatric treatment facility for each corps.30
Whatever their subsidiary activities, the principal function of the medical groups, and of the battalions that substituted for them in the Seventh Army, was evacuation of the division clearing stations. At the height of the offensive the groups transported wounded in large numbers. During November, for example, the Third Army`s 66th Medical Group handled over 12,000 XX Corps patients; its
374
67th Medical Group, in the same period, evacuated over 19,000 XII Corps casualties. The groups` attached battalions, each of which usually supported one or more divisions, normally placed a platoon of ten ambulances at each active infantry clearing or armored treatment station while holding other vehicles in a reserve pool to meet sudden casualty surges. The battalions set up ambulance control points at key road junctions to direct the flow of patients to particular evacuation hospitals. The 66th tried to avoid detouring ambulances through these points. It established an elaborate system for issuing frequent evacuation plans to its battalions, on the basis of which the battalions could send ambulances directly from clearing stations to their final destinations. This system, however, never achieved full acceptance by army authorities. In December, when the group shifted position to help evacuate Third Army forces in the Ardennes, army headquarters ordered it to establish a standard regulating post.
The groups by late 1944 had learned to control casualty flow with increasing sophistication, seeking to shorten as much as possible each patient`s time on the road while not overloading any evacuation hospitals. Most of the groups distributed wounded primarily on the basis of what they called "surgical lag" or "surgical backlog," which the Seventh Army typically defined as "the time, expressed in hours, required for a hospital to complete the surgery required on all moderately to severely wounded . . . casualties then present." Medical groups found from experience that this figure, although subject to inconsistencies in the estimating methods of individual chiefs of surgical service, indicated more reliably than did the simple number of empty beds the actual remaining capacity of a hospital. Depending on the situation and army directives, medical groups at times sorted casualties by type or severity, for example, sending surgical cases needing early operation to evacuation hospitals nearest the front. As hospitals moved into buildings during the autumn, groups had to take into account such details as the limited capacity of receiving wards no longer expandable by pitching more tents. When they could, groups deferred to the wishes of hospital commanders; some wanted a steady stream of new patients, while others preferred to receive them in periodic batches. Juggling such factors and considerations in constantly changing patterns, the groups kept the evacuation system within the armies operating with few interruptions, even in the face of deteriorating weather and road surfaces. They suffered late in the year from a shortage of ambulances and ambulance companies, but General Hawley remedied this by speeding up the transatlantic flow of machines and units and by stripping ambulances from the Communications Zone for the field armies. 31
Each army established an evacuation policy that governed the movement of casualties from its hospitals to those of the Communications Zone
375
(see Diagram 4). Normally, the armies evacuated all patients who needed more than 10 days, on the average, of hospitalization. But they varied this limit in response to the incidence of casualties and the number of empty beds, with an eye always to keeping as many salvageable men as possible within army boundaries until they returned to duty. Accordingly, during the October lull in combat, the First and Third Armies adopted, respectively, 20- and 21-day evacuation policies. Under these they could retain the increasing number of soldiers who came down with respiratory ailments as the weather turned cold and wet, as well as their lightly wounded, their venereal disease cases, and many neuropsychiatric patients. As casualties increased again in November, the armies reverted to 14-day, 10-day, and even shorter policies. The Ninth Army at one point ordered the daily evacuation of all its transportable patients, to clear beds for fresh wounded from the front. At various times during the offensive the First, Third, and Ninth Armies, their evacuation hospitals rapidly filling to capacity, all resorted to "bypassing." When this policy was in effect, evacuation hospitals stopped performing surgery on all but the most severe and urgent cases. They sent other surgical patients, after brief stabilizing treatment, immediately to COMZ general hospitals close in rear of the armies. By this means the army installations reduced their own surgical backlogs, while low-priority patients actually reached the operating table sooner than they would have in the evacuation hospitals. First Army hospitals, at the height of the offensive, bypassed well over 50 percent of the battle casualties they admitted.32
As the front stabilized, so did the locations at which patients passed from the armies to the Communications Zone. The First and Ninth Armies, during the fall and winter, sent casualties to ADSEC holding units and general hospitals at Liege and to a holding unit at Verviers. The Third Army evacuated through Toul, Etain, Nancy, and, as it approached the German border, Thionville. The Seventh Army, which continued to rely on the separate Southern Line of Communications (SOLOC) for evacuation and long-term hospitalization, evacuated through Luxeuil and Besancon to Marseilles and Naples. Later in the campaign its holding units shifted northward to Bayon and Tantonville, about 10 miles south of Nancy. With SOLOC slow to build up and short of hospital beds, the Seventh Army sent limited numbers of patients by air and rail to northern COMZ general hospitals in Paris, the Oise Base Section, and the United Kingdom. Increasingly, during late 1944, ADSEC and its southern counterpart, Continental Advance Section (CONAD), took over the operation of holding units in rear of the armies and the ambulance evacuation of casualties from army hospitals. Only the Third Army continued to maintain
376
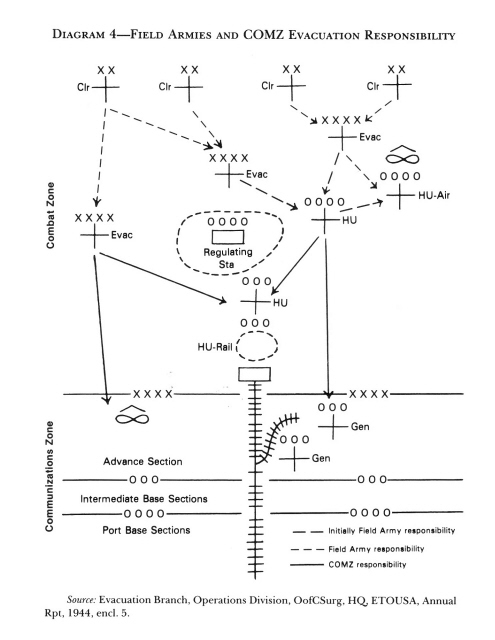
DIAGRAM 4-FIELD ARMIES AND COMZ EVACUATION RESPONSIBILITY
377
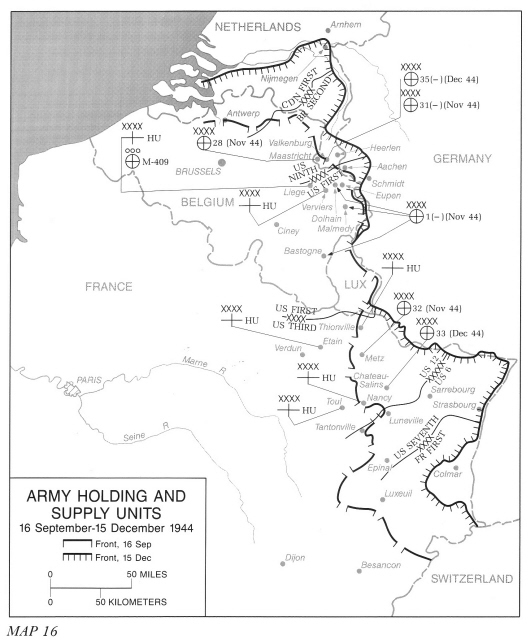
its own air-rail holding unit, and its 69th Medical Group shared with ADSEC the work of transporting patients to the Communications Zone (see Map 16) .
All the armies continued to evacuate their severely wounded by air from forward fields whenever possible. However, as flying weather worsened and rail service steadily expanded, hospital trains carried the greater proportion of patients leaving the army areas. On the whole, the flow of casualties from the armies went smoothly during the November and December battles. Interruptions of evacuation, such as had clogged army facilities at the end of the pursuit, became increasingly rare as ADSEC and CONAD enlarged the quantity and variety of their means of transportation, and as the slow progress of the offensive reduced the need to move forward holding units and extend rail lines. In evacuation, as in other aspects of medical support, bad news for the tactician was, paradoxically, good news Cin terms of operational efficiency C for the logistician.33</p>
Army Hospitals at Work
In each field army, during late 1944, the hospital system reached full development. Field hospital platoons attached to division clearing stations worked on the most urgent emergency surgical cases. Evacuation hospitals handled the transportable severely wounded, the patients with minor injuries, and most of the sick. A convalescent hospital in each army relieved the evacuation hospitals of nearly recovered patients and reconditioned them for return to duty. Improvised special facilities cared for soldiers with contagious or communicable diseases and venereal infections, as well as for neuropsychiatric casualties.
Surgical work in the armies centered in the field and evacuation hospitals. Field hospital surgeons spent most of their time operating on men with massive chest and abdominal injuries, severe compound fractures, and traumatic amputations. Their principal objective was to keep their patients alive and to place them in condition for further evacuation. Postoperative death rates in these installations ran between 12 and 25 percent, higher than in any other type of hospital, and reflected the all but hopeless condition of many of the wounded who arrived on their operating tables. All too common were cases such as the Ninth Army soldier who died twenty-four hours after surgery in the 2d Platoon, 53d Field Hospital: "S[hell] F[ragment] W[ound] multiple with complete amputation right foot; C[ompound]
378
379
F[racture] left fibula, soft tissue wounds [right] thigh and left leg; . . . severe muscle damage both legs. . . ." 34
Evacuation hospital surgeons operated on the great majority of orthopedic patients, who usually were transportable enough to bypass the field hospital platoons. By debridement and the application of plaster casts, the surgeons prepared these casualties for further transportation and laid the groundwork for definitive treatment in COMZ general hospitals. In compound fractures, according to a Third Army surgeon, "what we had to do was create a clean, organizable wound out of an indiscriminately smeared up, messed up situation." Evacuation hospital surgeons, while they handled a large number of minor and moderately severe injuries, also encountered massive wounds, some of which gruesomely illustrated the macabre mischances of modern combat. The same Third Army surgeon recalled:
The French manure pile . . . came into the operating room. An infantryman had hidden next to one when the shell blew up in the pile filling his thigh from knee to buttocks with manure, all tightly packed in as into a sausage, [and] smashing muscle and femur bone. He was in critical condition. . . . I started debriding after the second set of bottles of blood was partly in. . . . After a major debridement, pockets containing manure kept appearing in deeper and deeper layers in all directions until there was not much left of the limb. Reluctantly I had to disarticulate [amputate] the limb at the hip and debride the buttock. This man developed kidney failure and died on the ninth day. . . .35
Field and evacuation hospitals alike depended for surgical reinforcements upon teams from the auxiliary surgical groups; indeed such teams made up the entire operating room staff of the field hospital platoons. The European Theater by late 1944 possessed five complete auxiliary groups, attached to the field armies and army groups, and the equivalent of half of another, assigned to COMZ. Each group included about twenty-five teams of doctors, nurses, and enlisted technicians, the majority organized for general surgery and the rest for neurosurgery, maxillofacial work, X-ray, and dental prosthetics. These teams contained an impressive array of professional talent, and the theater took pains to maintain the quality of their personnel. Accordingly, when the Ninth Army`s 5th Auxiliary Surgical Group arrived in France with a substantial number of young, inexperienced medical officers, -the -army-had no difficulty restaffing it with better qualified men transferred from the Communications Zone and the ground forces. Besides the teams, the auxiliary groups included varying
380
numbers of truck-mounted mobile operating rooms and X-ray facilities, designed for temporary expansion of busy hospitals. The operating trucks proved to be of only limited use, as the hospitals` capacity for surgery was restricted more by shortages of nurses and other postoperative support than by a lack of theater space. The X-ray units, however, effectively reinforced roentgenological departments swamped by sudden floods of patients.
Auxiliary groups normally attached most of their general teams, heavily weighted with thoracic and abdominal specialists, to field hospital platoons. Maxillofacial, neurosurgical, and other specialized teams went to evacuation hospitals, which received most of the type of patients they treated. During heavy fighting a single auxiliary group could not meet an army`s demand for extra surgeons. At such times evacuation hospitals, especially, drew additional temporary teams from staging COMZ units, an arrangement that at once solved the armies` surgical manpower problem and gave useful experience to the fixed hospital personnel. 36
The presence in units of doctors, nurses, and technicians who administratively and in part professionally answered to another organization created problems of command and human relations. This was especially true in field hospital platoons. The commander of the 3d Auxiliary Surgical Group summed up: "Platoon commanders are irked that teams create awkward problems of supply and transportation, that teams do not come under the administrative control of the hospital, and that teams are neither fish nor fowl." On their side, team members "feel that they are always last in line, that they get second-best, and that they are the unwanted children." Permanent unit staff also resented being relegated to routine ward duties, while auxiliary teams did all the surgery and ran the operating theaters. Even in evacuation hospitals, where the auxiliary teams worked under the unit chiefs of surgical service, the reinforcements had an aura of elitism and professional independence that set them apart. An officer in the 109th Evacuation Hospital observed: "The `Aux` teams acted like doctors and nurses doing their job, but in uniform. The Evac teams . . . were more members of a military echelon, hierarchy, order . . . in the lower rank of such an order. . . ." Auxiliary surgical group commanders devoted much effort and diplomacy to smoothing out these undercurrents of conflict. Aided by a shared sense of a common professional mission, they usually succeeded.37
381

EVACUATION HOSPITAL RECEIVING WARD
Field and evacuation hospitals alike arranged their physical plants and streamlined their procedures for rapid reception, sorting, and treatment of a large volume of patients. Most units, whether in tents or buildings, tried to lay out their facilities so that a casualty would move in a more or less straight line from receiving through surgery to postoperative care and evacuation. Many, by converting cots to work stands for litters, were able to keep a patient on the same stretcher from the time he came off the ambulance until he reached the postoperative ward. Hospitals, after initial episodes of confusion, learned to put their most capable officers in charge of reception and triage. These officers quickly examined each arriving casualty and dispatched him to the shock, preoperative, medical, or immediate evacuation wards. In the shock and preoperative wards, doctors, nurses, and enlisted technicians, working with all possible speed, took the necessary resuscitation and stabili-
382
zation measures and moved the patient to and from X-ray. Roentgenology constituted a perennial bottleneck when casualties were coming in rapidly, and hospital technicians taxed their ingenuity to the limit to expedite the taking and development of pictures. One unit, the 107th Evacuation Hospital, sent patients in shock to X-ray before resuscitation, in the belief that a slight delay in starting the latter process would be less harmful to the casualty than a subsequent interruption of it. Using such expedients, hospitals could process masses of casualties. On the night of 16 November, for example, the 111th Evacuation Hospital, located at Heerlen, Holland, behind the Ninth Army, admitted 272 patients in four hours; its people examined, sorted, and placed under shelter more that 1 wounded man each minute.38
Field and evacuation hospitals organized their surgical staffs to operate on the maximum number of cases within the shortest possible time. In field hospital platoons the attached surgical teams, and in evacuation hospitals normally the chiefs of surgical service or the senior surgeons on shift, scheduled patients for operation. While each army set general guidelines for establishing surgical priority, the officers actually managing the traffic applied these rules with great flexibility, their aim being to keep all available surgeons and tables continually busy. Surgeons, nurses, and technicians worked in more or less permanent teams. A field hospital platoon with two attached teams could complete perhaps twenty major operations a day. A 400-bed evacuation hospital could keep eight to ten operating tables in action around the clock; the number of cases they turned out depended on the severity of the casualties then being received. In theory, surgical teams working twelve hours and resting twelve hours could keep up this pace almost indefinitely; in practice, the regimen quickly took its toll. During periods of heavy action the 9th Evacuation Hospital reported that "the staff was nearly always tired and too often lacking in sleep." A surgeon in the 109th Evacuation Hospital recalled: "I began to tire physically and psychologically from the twelve hour operating stretch every day; then, eating after the last surgery, writing letters and going to sleep. . . . I worked on instinct when tired." 39
383

PACKING MEDICAL SUPPLIES IN A 155-MM. HOWITZER SHELL, to be fired to troops cut off by the Germans
Inevitably, with surgery being done under forced draft, errors occurred. Surgeons, especially in hospitals newly placed in operation, debrided wounds improperly or inadequately. They neglected to split casts to allow for swelling and permitted too early evacuation of patients with abdominal wounds or severe vascular damage. The army surgeons and their consultants, who kept close watch on the quality of professional practice in their hospitals, labored continually to reduce the incidence of such mistakes. The First Army temporarily stationed medical officers in ADSEC general hospitals, to check on the condition of patients arriving from the army. On the basis of these officers` reports Colonel Rogers, the army surgeon, among other changes revised his evacuation policies for men with chest and vascular injuries. Hospitals constantly reviewed their own surgical practice, for example, by conducting autopsies whenever possible in cases of postoperative death. In general, the quality of field and evacuation hospital surgery stood the test of review farther to the rear. During October, at a Paris meeting of Allied medical officers to discuss battle casualty treatment, COMZ surgeons, with only minor reservations, pronounced themselves satisfied with the condition of the patients reaching them from the armies. Colonel Cutler, the ETO chief surgical consultant, de-
384
clared that earlier and more effective surgery C combined with widespread use of whole blood and antibiotics and the generally more robust physical condition of the troops C accounted for the higher recovery rate of the wounded in this war as compared to World War I.40
Mobile army hospitals tried to evacuate patients within as short a time as possible after their condition was stabilized, the minor postoperative cases almost as soon as they recovered from the effects of anesthesia. The operating surgeon normally had the final say in determining when his patient was transportable, but he had to take into consideration available beds, how many new casualties were arriving, and army policies. The armies, usually in response to COMZ complaints about evacuating too early, required their hospitals to hold certain postoperative patients C notably chest, abdominal, and neurosurgical cases and men with severe extremity wounds involving vascular damage C for a fixed number of days. Hospitals set up separate wards, with surgeons in charge, for such patients and placed the rest in wards designated for immediate evacuation, usually staffed by officers of their medical services. Evacuation hospitals sent off the majority of their patients within less than ten days; field hospitals, because of the severity and complicated nature of their cases, had to retain theirs for longer periods, a requirement that perennially conflicted with their need for mobility. The Third Army attached thirty-man holding units, drawn from collecting and gas treatment companies, to its field hospital platoons to stay behind with nontransportable patients when the main units moved.41
Getting a patient out of a hospital was itself a complicated task. The commander of the 110th Evacuation Hospital pointed out:
When a patient is said to be ready for evacuation, it is not just a matter of putting him in an ambulance. . . . The patient must be made ready as far as clothing is concerned, then there [are] his valuables, and his x-rays. The problem is increased when you have from one hundred . . . to two hundred patients, spread all over the hospital, ready for evacuation.
Each hospital developed its own system for sending off patients. The 110th, for example, used two enlisted men as evacuation clerks, with four litterbearers to collect evacuees from
385
the wards. When the time came to move patients, the registrar alerted the clerks and bearers and the affected wards and sent the evacuation list to the offices in charge of patient valuables and X-ray files. Those offices packed up the appropriate items for each man for attachment, with his records, to his litter when the bearers brought him to a central point in the hospital. After a Red Cross worker made sure that each soldier had cigarettes, candy, and toilet articles, then litter teams began manhandling their charges into waiting ambulances.42
By late 1944 each army had a full system of specialized medical facilities in operation designed to relieve clearing stations and field and evacuation hospitals of certain categories of nonsurgical patients and to keep as many salvageable soldiers as possible within army boundaries and out of the COMZ replacement system. Convalescent hospitals-T/O 3,000-bed units in the First, Third, and Seventh Armies and a 400-bed facility improvised from a gas treatment company in the Ninth-admitted ambulatory patients transferred from evacuation hospitals. They put these men through usually about ten days of physical therapy and reconditioning before sending them back to line units. Other facilities treated men with specific ailments who came to them directly from division clearing stations. The First Army used two clearing companies as 500-bed treatment centers for soldiers with combat fatigue; its gas treatment battalion operated hospitals for malaria, communicable and contagious disease, and self-inflicted-wound patients. The Third Army established venereal disease and neuropsychiatric sections in its 6th Convalescent Hospital, and the Ninth Army employed its gas treatment battalion to care for these casualties and also malaria cases. In the Seventh Army one clearing company and a platoon of another treated neuropsychiatric patients; another clearing company-reorganized for the purpose before the DRAGOON invasion-operated a 250-bed venereal disease hospital. These facilities, besides caring for many nonbattle casualties, helped- the armies conserve manpower. In four months, for example, Third and Seventh Army convalescent hospitals returned to duty respectively 11,000 and 10,000 veteran troops. 43
All the armies made special efforts to salvage as many as possible of their neuropsychiatric casualties-soldiers who suffered emotional breakdowns, of varying symptoms and severity, under the stress- of battle. The incidence of such casualties fluctuated, as did that of physical wounding, with the intensity and nature of combat. During heavy fighting, such as that of
386
the autumn and winter offensive, neuropsychiatric cases accounted for between 9 and 25 percent of total monthly hospital admissions.
The armies, taking advantage of lessons learned in North Africa and Italy and of the First Army`s early experience in Normandy, treated the emotional casualties of battle as temporarily disabled soldiers rather than mental patients, normally categorizing them with the neutral diagnosis "exhaustion." For the sake of both prevention and cure they attempted to treat such patients as close as possible to the fighting line. Typically, infantry battalion surgeons, trained in this work and supervised by their division psychiatrists, held all but the most severely disturbed men at their aid stations for up to twenty-four hours of rest (often under sedation), hot food, a change of clothing, and rudimentary individual and group therapy. Such treatment sufficed for an unrecorded but very high proportion of men with combat reactions, allowing their immediate return to their units.
Men needing a longer period to rest and more intensive therapy were evacuated to their division clearing stations. There, the division psychiatrist, with a pickup staff and improvised facilities, operated an "exhaustion center" that could hold patients for up to seventy-two hours of treatment. The clearing stations also returned to duty a substantial portion of the men they received. The rest went to the various specialized army facilities mentioned above and, in the Third Army, to the neuropsychiatric wards of regular evacuation hospitals, for periods of up to seven days of therapy and reconditioning, ending in a period of refresher training in a military camp rather than a hospital environment. The Third Army used a section of its convalescent hospital as still another echelon of army-level treatment that could hold patients for as long as two or three weeks. However, the other armies evacuated men still unfit for duty directly from their neuropsychiatric hospitals to the Communications Zone.
In the United Kingdom Base most general and station hospitals maintained fully staffed and equipped psychiatric services. In addition, the 312th Station Hospital (NP) and the 96th General Hospital (NP), specialized psychiatric facilities, received the most severely disturbed soldiers from other installations for prolonged, intensive treatment and rehabilitation. The 96th also selected mental patients for evacuation to the United States. On the Continent the Communications Zone attempted to set up neuropsychiatric hospitals close behind the armies to take patients from their exhaustion centers and to complete their treatment so that they could reenter the replacement system. For this purpose ADSEC in mid-November opened the 1,000-bed 130th General Hospital (NP) at Ciney; Belgium, to serve the First and Ninth Armies. At about the same time CONAD established the 500-bed 51st Station Hospital (NP) at Luneville to support the Third and Seventh Armies. However, given the shortage of forward general hospitals, both units were pressed into service to care for medical and surgical patients during the American offensive and the German December counterattacks. They began functioning primarily as neuropsychiatric facilities only
387
during the last weeks of hostilities. Even without them, the armies and COMZ made an impressive record of success in rehabilitating emotionally damaged soldiers. According to a later estimate, out of every 100 psychiatric casualties in the theater, the armies and the Communications Zone restored 90 to some form of duty. 44
Army hospitals, of whatever type, coped daily with manpower and equipment deficiencies. Ingenuity and improvisation facilitated their overcoming innumerable logistical and operational problems. F ield hospitals made do with standard allowances of people and equipment intended for a very different function from the one they were performing. They had a constant battle to secure transportation for their many moves. The six nurses in each platoon were stretched to the limit of their endurance, caring for as many as sixty-five postoperative patients any of whom, in a civilian institution, would have required the exclusive attention of one or more nurses. The Seventh Army, in an attempt to alleviate these problems, reduced the bed capacity of each of its field hospital platoons to 60 and increased the nurse complement to eight with ANC officers borrowed from the Communications Zone. This army also issued additional trucks, trailers, and weapons carriers to each field hospital, giving the unit enough vehicles to move a platoon without outside help. All the armies -employed collecting and clearing company elements, POWs, and French and Belgian civilians to meet the insatiable requirements of their evacuation hospitals for additional attendants and laborers. By late 1944 the typical 400-bed evacuation hospital had between fifty and eighty prisoners or civilians attached to it. Civilians replaced the German POWs as units neared the borders of the Reich.45
Mud, rain, cold, and snow became major adversaries for army medical installations as the harsh winter closed in. Frequent downpours transformed hospital areas into seas of mud, in spite of the best efforts of engineers and medical troops with gravel and bulldozers. In one Third Army hospital "a plow came in and scraped mud into piles as if it were dealing with snow." As the days and nights grew colder, steam rose from abdominal incisions in unheated surgical tents. One unit resorted for warmth to potbelly stoves placed close to its operating tables. "Probably due to the closed system of anesthesia and good outdoor ventilation," a surgeon recalled, "and adding a
388
factor of luck, there were no ether explosions." With wind and snow came additional tribulations. Work details swept accumulated snow off tents to keep them from collapsing, and they struggled to secure stovepipes and tent pegs against battering gusts. 46
To remove staffs and patients from such hardships, the armies during November and December gave their hospitals and other medical units first claim on requisitioned buildings. Hospitals under roofs-in casernes, schools, hotels, monasteries, and even a former German slave labor camp-encountered new problems. Unlike tents, buildings could not be moved to the most convenient points on the routes of evacuation. Thus field hospital platoons, for the sake of shelter, often perforce set up some distance away from the clearing stations they supported. Hospitals usually had to do extensive cleaning and disinfecting to make their quarters habitable. Enlisted medics of one evacuation hospital jokingly suggested that the letters "SM" (Semimobile) in their unit designation really meant "Scrubbing and Mopping." In nonmedical structures floor plans left much to be desired from the hospital point of view. Dispersal of patients among many small rooms, for example, as in schools, meant harder work for nurses, ward attendants, and litterbearers. Units required additional people and equipment, not included in T/O&Es designed for tented operation, to perform plant maintenance and engineering. With these augmentations, evacuation hospitals, especially, needed still more transportation to move them. 47
As army hospitals acquired campaigning experience, their medics became adept at improvising, and at obtaining-by one means or another-what they needed. Each unit developed its own individual plan for setting up. Colonel Gorby declared: "I don`t think I had a field hospital commander, or an evac hospital commander, that would set [up] his operating pavillion and his ward tents and pre-ops and post-ops and receiving and all that in exactly the same way. . . . We indicated that as long as it was effective it was all right." Foraging, as one hospital report put it, "by now had become instinctive." Medics regularly turned the refuse of war into objects that saved their patients` lives or enhanced their own comfort. In the 59th Field Hospital discarded 5-gallon food tins, cut in half, became operating-room light fixtures, their polished interiors ready-made reflectors. A large box, a 20-gallon gasoline tank, two faucets, a length of pipe, and a galvanized trough, all salvaged, became a surgeon`s scrub sink. Scrap lumber went into back rests for chest-wound pa-
389
tients. Other hospitals built their own suction apparatus, as well as ward desks and tables, folding water towers, and portable showers. They mounted their generators on captured enemy trucks and appropriated whatever other usable German materiel came their way, including in one unit a couple of truckloads of liquor seized in Cherbourg and carried across France. Hospitals followed the campaign philosophy: "Take what you can get and hang onto it; each set-up will be a little different, a little better than the last; make your comfort and your amusements now-who knows when you can again?" 48
Sources of Supply
By the time the offensive began in November, the army supply depots had settled into positions within convenient supporting distance of the front. They gradually edged forward as the attacking divisions gained ground. The Ninth Army brought with it from Brittany a single medical supply unit, the advance section of the 33d Medical Depot Company, temporarily attached from the Third Army. This supply element, which established itself at Valkenburg, Holland, taking over stock of a former First Army dump, distributed supplies to all of the Ninth Army until the last days of December, when the advance section of the 35th Medical Depot Company relieved it. Beginning in late November, another Ninth Army depot company, the 28th, located at Maastricht, assumed the task of receiving supplies from the Communications Zone and forwarding them to the advance element at Valkenburg. Elsewhere in the 12th Army Group, army depots underwent little change. The 1st Medical Depot Company, in the First Army, shifted its base to Dolhain, just west of its former site at Eupen, in order to find suitable buildings. Advance sections of this company operated medical supply points at Malmedy and Bastogne. The Third Army`s 32d and 33d Medical Depot Companies, located respectively at Verdun and Toul when the offensive started, moved eastward, the 32d to Metz in late November and the 33d to Chateau-Salins in mid-December.49
The Seventh Army had its own separate line of medical supply. Its 7th Medical Depot Company followed the army across the Riviera beaches and up the Rhone valley successively to Epinal, Luneville, and Sarrebourg. Throughout the summer and early fall this company bore most of the burden of hauling supplies the entire distance from the Mediterranean coast. During November the Southern Line of Communications finally relieved the 7th Company of that task
390
by setting up an intermediate medical depot at Dijon, which in turn was replenished from a base facility at Marseilles. Materiel to stock these depots came from the Mediterranean Theater during the first sixty days of the southern France campaign and thereafter directly from the United States. The Seventh Army also possessed an independent blood service, provided by the 6703d Blood Transfusion Unit. An advance element of this unit distributed blood, initially flown in from Naples and, after 29 October, drawn from service troops at Marseilles and forwarded, via rail, to field and evacuation hospitals. Late in October, as demand exceeded the capacity of the 6703d, the army also began receiving shipments of ETO blood from Paris. 50
Within the armies, medical supply distribution presented few difficulties beyond those inherent in the conditions of combat. Divisional and corps medical units and detachments drew expendable items on informal requisition from the nearest army supply point, usually an advance section of the depot company or a small dump maintained by the corps. Hospitals, depending on their locations, requisitioned either from the advance points or from the main army depots. Among their liaison functions, the medical groups often assisted hospitals and other nondivisional units in obtaining supplies and resolving logistical difficulties. Divisions employed all types of vehicles and resorted to every conceivable expedient to keep battalion aid stations and front-line medics supplied. They delivered plasma, dressings, and other urgently needed items to temporarily cut-off units by parachute and on a couple of occasions fired materiel to them in specially refilled artillery shells. The 90th Infantry Division, which had several units isolated during its battle for a Saar River bridgehead in December, sent medical supplies to them in remodeled aircraft wing tanks. Fighter-bombers, flying in at treetop level, dropped the tanks accurately into the infantry perimeter.51
When the offensive began, the flow of medical supplies from both communications zones into the army depots was still, from the armies` standpoint, less than satisfactory. In the 12th Army Group medical supply deliveries to the armies regularly fell short of the daily SHAEF tonnage allocations. The army depots constantly reported shortages; those of the First Army at one point had zero balances in over 400 inventory items. The
391
Ninth Army during November had to rely entirely on salvage for spare parts for its medical equipment. In spite of these conditions, all the armies kept their operating units supplied with enough of the things they immediately needed to perform their missions. Army surgeons usually could obtain air shipments to meet emergencies, for example, to remedy the drain of litters and blankets caused by evacuation. They regularly employed their own trucks to haul additional materiel forward from COMZ depots. In the 12th Army Group the army surgeons worked continually with the ADSEC regulating stations and the chief surgeon`s Supply Division to speed up the processing of requisitions and to trace lost or misdirected cargo. The northern and southern communications zones steadily improved rail transportation and built up their advance depot stocks. In the north the opening of the port of Antwerp late in November drastically shortened American supply lines and permitted full use of ADSEC medical depot M-409 at Liege, close behind the First and Ninth Armies. Signaling the end of the long supply famine, SHAEF on 9 December abolished its tonnage allocation system. By that time the army depots, although still short of some items, were well on the way to accumulating their planned fourteen-day reserves. 52
The System in Full Stride
The medical service of the American field armies reached a high level of efficiency and effectiveness during the November-December offensive. The armies had perfected their evacuation systems to the point where most battle casualties arrived at division clearing stations or their attached field hospital platoons within one or at most two hours of being injured. Transportable patients usually reached evacuation hospitals no more than eight hours after they suffered their wounds. Men who entered the army hospitals had an excellent chance of surviving. In all four armies less than 3 percent of the battle casualties admitted to medical facilities died, with the majority of the fatalities occurring in the field hospital platoons. Counting nonbattle as well as combat casualties, the death rate in army clearing stations and hospitals amounted to some 1.5 percent of admissions. The armies evacuated their patients to the Communications Zone in generally good condition. The 28th General Hospital at Liege, for example, reported only 2 deaths among 4,000 surgical patients it received from the First and Ninth Armies and only 1 man with gas gangrene, who recovered. Following one of his many
392
inspections, General Kenner declared flatly: "The medical service in the forward area has been excellent." 53
Thus far in the campaign the field armies possessed the tactical initiative, but in mid-December that condition abruptly changed. Ground force medics were about to undergo what was, for most of them, a new experience: that of retreat before an enemy temporarily and locally superior in numbers and firepower and enjoying the advantage of surprise. The army medical service had proved its ability to support forces engaged in set-piece battles and headlong pursuit. Now its adaptability was to be tested in withdrawal, encirclement, and hastily improvised counterattack.
FOOTNOTES
1. Ninth Army brought the VIII Corps up from Brittany early in October and initially entered the line in the Ardennes. It shifted to the 12th Army Group`s left after relinquishing the corps to the First Army and in turn taking over the latter` left-most corps, the XIX.
2. Interv, T/5 George Morgan, 1st Battalion, 22d Infantry, in 4th Infantry Division Combat Intervs, box 24021, RG 407, NARA [in Interv, Capt. Jennings Frye, Lt. George Kozmetsky, and T/3 Harry I. Fingerroth, 20 Dec 1944].
3. This account is based on MacDonald, Siegfried Line, passim; Cole, Lorraine Campaign, passim; Robert R. Smith and Jeffrey J. Clarke, The Riviera to the Rhine (Washington, D.C.: U.S. Army Center of Military History, 1993), chs. XVI-XXVI; Seventh U.S. Army Report of Operations, France and Germany, 1944-1945, vol. II, pp. 456-94, 505-13, 529.
4. MacDonald, Siegfried Line, p. 617; Cole, Lorraine Campaign, pp. 592-93; Surg, First U.S. Army, Annual Rpt, 1944, pp. 5-6; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 139, 179, 201, 205; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 43-44, 104, 108, ex XXVII; Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 29-32 and 37d-37f; Seventh U.S. Army Report of Operations, 1944-1945, vol. III, p. 1,029; Surg, Ninth U.S. Army, Annual Report, 1944, pp. 20-22; Surg, Ninth U.S. Army, Combat Experience Tables of Casualties, Ninth U.S. Army, October-December 1944 (hereafter cited as Combat Experience Rpt, with month), file HD 319.1-2. For typical casualty distribution among arms, see Surg, XIX Corps, Annual Rpt, 1944, encl. 20.
5. Ground forces medical personnel amounted to about 32-38 percent of the total theater medical strength of over 212,000 in late December. See Personnel Division, OofCSurg, HQ ETOUSA, Annual Rpt, 1944, app. D. MFR, Col B. A. Holtzworth, 8 Jan 45, sub: Notes on Service Troops, Moses Papers, MHI, gives 12th Army Group standards for field army medical troop strength.
6. Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 8-9 and 11-13; Surg, First U.S. Army, Annual Rpt, 1944, p. 48; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, p. 136.
7. Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 11-17, 19-22, 112-14; 12th Army Group Report of Operations, vol. VIII (Medical Section), pp. 57 and 116; Troop Movements and Training Branch, Operations Division, OofCSurg, HQ ETOUSA, Annual Rpt, 1944, pp. 8 and 11; Gorby Interv, 1962, pp. 54-55, CMH; 67th Medical Group Annual Rpt,1944, p. 17. For negotiations on medical reinforcements for the Seventh Army, see correspondence in DRAGOON 1944 file, CMH.
8. Quotation from Medical Division, COSSAC/SHAEF, War Diary, December 1944. See also Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 6-7; MFR, Lt Col J. H. Voegtly, 29 Sep 44, sub: Organization of Sixth Army Group and Medical Services of Sixth Army Group, in Surg, 6th Army Group, Annual Rpt, 1944-1945. For a general account of the formation of the French First Army, see Marcel Vigneras, Rearming the French, United States Army in World War II (Washington, D.C.: Office of the Chief of Military History, Department of the Army, 1957), chs. X and XI.
9. Gorby Interv, 1962, p. 5, CMH; Hartford Interv, 7-8 Oct 80, tape 1, side 2, CMH; Surg, 6th Army Group, Annual Rpt, 1944-1945, pp. 1-3.
10. First U.S. Army Report of Operations, 20 Oct 43-1 Aug 44, bk. 1, pp. 16-17; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 37-38 and 68-70; Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 3 and 6; Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 116 and 129; Hartford Interv, 7-8 Oct 80, tape 1, side 2, CMH; Editorial Advisory Board, 1962, pp. 97-98. In Shambora Papers, MHI, see Surg, Ninth U.S. Army, Daily Journal, 1 Nov 44; Memo, Col W. E. Shambora to ACofS, G-4, Ninth U.S. Army, 12 Jun 45, sub: Organization of the Medical Section, HQ NUSA; Memo, Reinstein to Surg, Ninth U.S. Army, 9 Sep 44, sub: Observation of Medical Service in Operation, TUSA; and Memo, HQ ADSEC, COMZ, to Surg, Ninth U.S. Army, 28 Sep 44, sub: Liaison Officer.
11. Surg, Third U.S. Army, Annual Rpt, 1944, pp. 46 and 91-92, gives hospital movement statistics; for offensive plans and preparations, see p. 38. For an example of corps-level assault medical planning, see VII Corps Medical Plan, pp. 93-95, encl. 1 to Surg, VII Corps, Annual Rpt, 1944.
12. For examples of army policy, see First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 166-67, and Cir Ltr No. 2, Surg, Seventh U.S. Army, 18 Jul 44, sub: Surgery, in Surg, Seventh U.S. Army, Annual Rpt, 1944.
13. Rpt No. E-81, Research Branch, Special Services Division, ETO, September 1944, sub: Opinions of Wounded Combat Veterans on Battlefield First Aid Treatment (hereafter cited as ETO, Battlefield First Aid Rpt, 1944), pp. 2-5, file HD:ETO: 350.07:Battle Experiences. Quotations from app., pp. ii and iii.
14. Quotation from ETO, Battlefield First Aid Rpt, 1944, app., p. ii, file ETO:350.07:Battle Experiences. On EMTs, see Surg, 5th Infantry Division, Annual Rpt, 1944, pp. 34-35, and Rpt No. 368, Army Ground Forces Board, 18 Nov 44, sub: Medical Information, 8th Infantry Division, p. 4.
15. Quotation from Interv, Capt D. Faulkner, in 4th Infantry Division Combat Intervs, box 24021, RG 407, NARA. Wilson`s citation is in U.S. Congress, Senate, Committee on Veterans` Affairs, Medal of Honor Recipients, 1863-1978 (hereafter cited as MOH Recipients), 96th Cong., 1st Sess. (Washington, D.C.: U.S. Government Printing Office, 1979), pp. 715-16. Surg, XIX Corps, Annual Rpt, 1944, an. E, contains a typical tribute to company aidmen.
16. The General Staff, on 1 March 1945, authorized a special combat medical badge and ten dollars extra pay a month for Medical Department personnel "daily sharing with the infantry the hazards and hardships of combat." See McMinn and Levin, Personnel, pp. 337-38. For views of field troops, see Medical Division, COSSAC/SHAEF, War Diary, December 1944, and ETO, Battlefield First Aid Rpt,1944, app., p. v, file HD:ETO:350.07:Battle Experiences. For an example of awards received, see Surg, XII Corps, Annual Rpt, 1944, p. 11.
17. Quotation from Cir Ltr No. 2, Surg, Seventh U.S. Army, 18 Jul 44, sub: Surgery, in Surg, Seventh U.S. Army, Annual Rpt, 1944. See also First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 166-67; ETO, Battlefield First Aid Rpt, 1944, app., p. iii, file HD:ETO:350.07:Battle Experiences; Rpt. No. 368, Army Ground Forces Board, 18 Nov 44, Medical Information, 8th Infantry Division, p. 4.
18. Examples of divisional evacuation systems, see Surg, XIX Corps, Annual Rpt, 1944, ans. C and E; Surg, XX Corps, Annual Rpt, 1944, pp. 18-19; and Surg, 10th Armored Division, Annual Rpt, 1944, pp. 30-32 and encl. 14.
19. Richardson Interv, tape 1, side 2, CMH.
20. Surg, 1st Infantry Division, Annual Rpt, 1944, pp. 22 and 32; Surg, 90th Infantry Division, Annual Rpt, 1944, pp. 20-23; Medical Bulletin, 95th Infantry Division, 1-30 Nov 44, pt. II, in Surg, 95th Infantry Division, Annual Rpt, 1944; Surg, 4th Armored Division, Annual Rpt, 1944, p. 11; Surg, 5th Armored Division, Annual Rpt, 1944, p. 54.
21. Quotation from Tegtmeyer "Diary," pt. II, p. 90. Second and third quotations from Intervs, Assistant Surgeon and Aidmen, 1St Battalion, 22d Infantry, in 4th Infantry Division Combat Intervs, box 24021, RG 407, NARA. See also Richardson Interv, tape 1, sides 1 and 2, CMH.
22. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 130-40 and 144; Surg, V Corps, Annual Rpt, 1944, p. 19; VII Corps Medical Plan, pp. 89-91 and 97-98, encl. 1 to Surg, VII Corps, Annual Rpt, 1944; 68th Medical Group Annual Rpt, 1944, pp. 16, 19-21, 25; 134th Medical Group Annual Rpt, 1944, p. 19; Surg, 1st Infantry Division, Annual Rpt, 1944, pp. 22-23; Surg, 3d Infantry Division, Annual Rpt, 1944, encl. 1; Surg, 4th Infantry Division, Annual Rpt, 1944, p. 3; Surg, 8th Infantry Division, Annual Rpt, 1944, pp. 14-16; Surg, 28th Infantry Division, Annual Rpt, 1944, encl. 5; Intervs, Company G, 22 Infantry, in 4th Infantry Division Combat Intervs, box 24021, RG 407, NARA.
23. Quotation from First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, p. 166; see also p. 164. For examples of aid station operations, see Surg, 3d Infantry Division, Annual Rpt, 1944, encl. 2; AGF Rpt No. 892, War Department Observers Board, ETO, 30 Apr 45, sub: Combat Experiences (hereafter cited as AGF, Combat Experiences Rpt, 1945), pp. 9-10, file HD:ETO:350.07: Battle Experiences; Interv, Assistant Surgeon and Aidmen, 1st Battalion, 22d Infantry, in 4th Infantry Division Combat Intervs, box 24021, RG 407, NARA.
24. Quotation from Tegtmeyer "Diary," pt. II, pp. 90-91. For the recommendation to replace MCs with MACs, see Surg, 3d Infantry Division, Annual Rpt, 1944, encl. 2. Richardson Interv, tape 1, side 2, CMH, describes the role of MACs in evacuation.
25. Surg, 3d Infantry Division, Annual Rpt, 1944, encls. 1 and 2; Surg, 5th Infantry Division, Annual Rpt, 1944, pp. 35-36; AGF, Combat Experiences Rpt, 1945, pp. 9-11, file HD: ETO:350.07: Battle Experiences.
26. This narrative is based on reports of Major Berndt, Captains Linguiti and De Marco, 2d Lt. A. J. Muglia, and 1st Lt. L. C. Johnson, all in 28th Infantry Division Combat Intervs, box 24032, RG 407, NARA. For tactical and logistical details of this battle, see MacDonald, Siegfried Line, ch. XV, and Charles B. MacDonald and Sidney T. Mathews, Three Battles: Arnaville, Altuzzo, and Schmidt, United States Army in World War II (Washington, D.C.: Office of the Chief of Military History, Department of the Army, 1952), pp. 251-418.
27. Intervs, Assistant Surgeon and Aidmen, 1st Battalion, 22d Infantry, in 4th Infantry Division Combat Intervs, box 24021; Intervs, Lt Col Lewis E. Maness and Capt W. L. McWaters, in 9th Infantry Division Combat Intervs, box 24027. For other comments, see also reports of Linguiti and De Marco, in 28th Infantry Division Combat Intervs, box 24032, All in RG 407, NARA.
28. Quotation from ETO, Battlefield First Aid Rpt, 1944, app., p. v, file HD: ETO: 350.07: Battle Experiences. On markings, see Surg, Ninth U.S. Army, Daily Journal, 13, 21 and 25 Nov 44, Shambora Papers, MHI, and Surg, 95th Infantry Division, Annual Rpt, 1944, pp. 11-12. For examples of protests, see Surg, 101st Airborne Division, Annual Rpt, 1944, p. 19, and Memo, Capt P. A. Linguiti to Surg, 112th Infantry, 16 Nov 44sub: Misuse of Aid Station Site, in 28th Infantry Division Combat Intervs, box 24032, RG 407, NARA.
29. Quotation from Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 17, 20-21, 115-16. See also Surg, Third U.S. Army, Annual Rpt, 1944, pp. 7576; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 17; Surg, Ninth U.S. Army, Daily Journal, 1 Nov 44, Shambora Papers, MHI; 1st, 31st, 67th, 68th, 69th, and 134th Medical Groups Annual Rpts, 1944. For additional detail on group functions and organization, see Chapter IX of this volume. Hawley`s concern about the Third Army`s use of groups is in Ltr, Hawley to Col A. L. Gorby, 23 Nov 44, file HD 024 ETO CS (Hawley Chron). Gorby Interv, 1962, pp. 36-37, CMH, expresses general satisfaction with army employment of groups.
30. 1st, 66th, 67th, 68th, 69th, and 134th Medical Groups Annual Rpts, 1944; Surg, Seventh U.S. Army, Annual Rpt, 1944, p. 116.
31. Quotation from Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 126-28. See also ibid., pp. 16 and 116-17; 1st, 66th, 67th, 68th, and 134th Medical Groups Annual Rpts, 1944. On the ambulance shortage, see 12th Army Group Report of Operations, vol. XIII (Medical Section), p. 57, and correspondence in file HD ETO 451.8 (Amb), 1942-44.
32. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 137 and 163-64; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 45 and 79; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 28; Surg, Ninth U.S. Army, Combat Experience Rpt, November 1944, file HD 319.1-2; Memo, Kenner to CofS, SHAEF, 5 Dec 44, sub: Report of Inspection, Medical Service, First and Ninth U.S. Armies, Inclusive Period 20-30 Nov 44, in Medical Division, COSSAC/SHAEF, War Diary, December 1944.
33. Medical Division, COSSAC/SHAEF, War Diary, October-December 1944; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 13637 and 140; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 80-85; Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 12-13; 69th Medical Group Annual Rpt, 1944, pp. 11-12 and 16-17; 134th Medical Group Annual Rpt, 1944, p. 12; 41st Evacuation Hospital Annual Rpt, 1944, pp. 59-60, which gives a hospital view on improving evacuation; HQ SOLOC, History of the Medical Section, Headquarters, Southern Line of Communications, ETO, U.S. Army, 20 November 1944-1 January 1945 (hereafter cited as SOLOC Medical Hist), pp. 20-26; Surg, CONAD, Annual Rpt, 1944, pp. 8-10; MFR, Col J. H. Voegtly, 16 Nov 44, sub: Medical Service, Southern Group of Armies, and Memo, Anon. to Col Peyton, 18 Nov 44, sub: Notes Taken at Conference on Medical Service for Southern Group of Armies, both in DRAGOON 1944 file, CMH. See also appropriate pages in Chapter XIX of Smith and Clarke, Riviera to the Rhine.
34. Quotation from Surg, Ninth U.S. Army, Daily Journal, 9 Nov 44, Shambora Papers, MHI. For other statistics, see Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 118-20; 11th Field Hospital Annual Rpt, 1944, app. B; 13th Field Hospital Annual Rpt, encls. 4-5; 48th Field Hospital Semiannual Rpt, January June 1945, p. 15; 51st Field Hospital Annual Rpt, 1944, p. 13; and Memo, Kenner to CofS, SHAEF, 5 Dec 44, sub: Report of Inspection, Medical Service, First and Ninth U.S. Armies, in Medical Division, COSSAC/SHAEF, War Diary, December 1944.
35. First quotation from Gosman Interv, 24 Mar 82. Second quotation from Joseph A. Gosman, MD, "War without Blood" (1982), p. 150. Both in CMH. For other examples of evacuation hospital work, see 3d Auxiliary Surgical Group Annual Rpt, 1944, pp. 33-35; 5th Evacuation Hospital Annual Rpt, 1944, pp. 12-13; and 41st Evacuation Hospital Annual Rpt, 1944, p. 11.
36. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 168-69; 3d Auxiliary Surgical Group Annual Rpt, 1944, pp. 33, 35-36, 40, 44-46; 4th Auxiliary Surgical Group Annual Rpt, 1944, p. 7; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 99-102; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 28.
37. First and second quotations from 3d Auxiliary Surgical Group Annual Rpt, p. 34. Third quotation from Gosman, "War without Blood," p. 143, CMH. For typical auxiliary team control arrangements, see Medical News No. 1, Ninth U.S. Army, 30 Oct 44, file HD: ETO: 300.41, and Cir Ltr No. 7, Surg, Seventh U.S. Army, 28 Sep 44, sub: SOP for the Use and Control of Surgical and Allied Teams of an Auxiliary Surgical Group, in Surg, Seventh U.S. Army, Annual Rpt, 1944. Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 36-37, and 48th Field Hospital Semiannual Rpt, January-June 1945, p. 17, typify some of the conflicts and complaints.
38. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 161-63, gives a general view of triage and resuscitation in that army. For examples of hospital operations, see 48th Field Hospital Semiannual Rpt, January June 1945, pp. 5, 8, 11-12; 91st Evacuation Hospital Annual Rpt, 1944, pp. 56-57 and 69; 107th Evacuation Hospital Annual Rpt, 1944, pp. 10-12; and 111th Evacuation Hospital Annual Rpt, 1944, pp. 11 and 13-14.
39. First quotation from 9th Evacuation Hospital Annual Rpt, 1944, p. 16. Second quotation from Gosman, "War without Blood," pp. 151-52, CMH. See also Gosman Interv, 24 Mar 82, CMH; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, p. 162; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 102-03; 3d Auxiliary Surgical Group Annual Rpt, 1944, pp. 33-34. For examples of surgical organization and operations, see 47th Field Hospital Annual Rpt, 1944, pp. 9 and 11; 48th Field Hospital Semiannual Rpt, January June 1945, p. 8; 59th Field Hospital Annual Rpt, 1944, pp. 10-11; 11th Evacuation Hospital Annual Rpt, 1944, p. 4; 59th Evacuation Hospital Annual Rpt, 1944, p. 4 and sec. III, p. 8; 91st Evacuation Hospital Annual Rpt, 1944, pp. 59-61; 107th Evacuation Hospital Annual Rpt, 1944, p. 16; 111th Evacuation Hospital Annual Rpt, 1944, pp. 15-16; and 24th Evac Hist, October 1945, p. 93.
40. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 138 and 158; Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 28-32; Surg, Third U.S. Army, Annual Rpt, 1944, p. 41; Ltr, Hawley to Brig Gen J. A. Rogers, 9 Dec 44, file HD 024 ETO CS (Hawley Chron); Memo, Kenner to CofS, SHAEF, 24 Dec 44, sub: Report of Inspection of 3d US Army Medical Service and Supporting CZ Installations . . . , in Medical Division, COSSAC/ SHAEF, War Diary, December 1944. For an example of hospital policy on autopsies, see 48th Field Hospital Semiannual Rpt, January June 1945, pp. 10-11. Cutler`s remarks are in Notes Taken at Press Conference, Paris, 4 Oct 44, . . . by the Chief Surgeon, ETOUSA, in Hawley Papers, MHI.
41. For typical war operations and evacuation policies, see 48th Field Hospital Semiannual Rpt, January-June 1945; 110th Evacuation Hospital Semiannual Rpt, January June 1945; 54th Field and 91st and 111th Evacuation Hospitals Annual Rpts, 1944; and Surg, Ninth U.S. Army, Daily Journal, 31 Dec 44, Shambora Papers, MHI. For army policies, see First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 163-64; Medical News No. 1, Ninth U.S. Army, 30 Oct 44, file HD:ETO:300.41; and Cir Ltr No. 2, Surg, Seventh U.S. Army, 18 Jul 44, sub: Surgery, in Surg, Seventh U.S. Army, Annual Rpt, 1944. On holding units, see Surg, Third U.S. Army, Annual Rpt, 1944, p. 89; 30th and 60th Field Hospitals Annual Rpts, 1944.
42. Quotation from 110th Evacuation Hospital Semiannual Rpt, January June 1945, p. 8. For other examples of evacuation systems, see 91st and 107th Evacuation Hospitals Annual Rpts, 1944.
43. Convalescent hospitals were the 2d (Seventh Army), the 4th (First Army), and the 6th (Third Army). See Surg, First U.S. Army, Annual Rpt, 1944, p. 5; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 134 and 185; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 36, 79-80, 95-97, 111; Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 12-14 and 18; Surg, Ninth U.S. Army, Combat Experience Rpt, November 1944, file HD 319.1-2; Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 18-19, 21, 49, 51, 122-25; 2d, 4th, and 6th Convalescent Hospitals Annual Rpts, 1944; 92d and 95th Medical Gas Treatment Battalions Annual Rpts, 1944.
44. The foregoing discussion is based on Albert J. Glass, ed., [Neuropyschiatry in World War II. Vol. II:] The Overseas Theaters, Medical Department, United States Army in World War II (Washington, D.C.: Office of the Surgeon General, Department of the Army, 1973), chs. VIII and IX; restoration-to-duty estimate is on pp. 273-74. See also Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 32-33. The 130th General Hospital was caught up in the German Ardennes counteroffensive. See Chapter XII of this volume.
45. Surg, Third U.S. Army, Annual Rpt, 1944, pp. 92-93, 101, 124; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 19; Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 43 and - 46; - 68th-- Medical Group Annual Rpt, 1944, p. 21; 134th Medical Group Annual Rpt, 1944, pp. 11-12; Surg, XX Corps, Annual Rpt, 1944, pp. 22-23; 48th Field Hospital Semiannual Rpt, January June 1945; 47th Field Hospital Annual Rpt, 1944; 9th, 11th, 41st, 59th, 91st, 104th, and 111th Evacuation Hospitals Annual Rpts, 1944; Memo, Lt Col A. W. Shiflet to CG, AGF, 11 Nov 44, sub: AGF Report No. 364CMedical Information.
46. Gosman, "War without Blood," pp. 121 and 130, CMH.
47. Quotation from 111th Evacuation Hospital Annual Rpt, 1944, p. 10. For hospital problems from the army viewpoint, see An. 6-Medical Plan, p. 14, to FUSA Plan, 25 Feb 44, file HD 370 ETO; First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 139 and 155; Surg, Third U.S. Army Annual Rpt, 1944, pp. 39, 91, 122, 167; Surg, Seventh U.S. Army, Annual Rpt, 1944, p. 23; and Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 1920 and 23. For examples of unit difficulties, see Surg, XX Corps, Annual Rpt, 1944, p. 23; 48th Field Hospital Semiannual Rpt, January June 1945; 93d Evacuation Hospital Unit Hist, 1944; 110th Evacuation Hospital Semiannual Rpt, January June 1945; and 5th, 51st, and 104th Evacuation Hospitals Annual Rpts, 1944.
48. First quotation from Gorby Interv, 1962, pp. 28-29, CMH. Second quotation from 106th Evacuation Hospital Annual Rpt, 1944, pp. 14-15. Third quotation from 8th Field Hospital Annual Rpt, 1944, p. 4, attributing the words to the 91st Evacuation Hospital. See also 59th Field Hospital Annual Rpt, 1944, p. 10. For other comments on improvisations, see Surg, Third U.S. Army, Annual Rpt, 1944, pp. 126-27; remarks of evacuation hospital commanders in file HD: ETO: 350.07: Battle Experiences; and 91st, 105th, 106th, and 111th Evacuation Hospitals Annual Rpts, 1944. On liquor supply, see Gosman Interv, 24 Mar 82. CMH.
49. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 154-55; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 165 and 168-69; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 12; Surg, XIX Corps, Annual Rpt, 1944, encl. 19; 32d Medical Depot Company Annual Rpt, 1944, pp. 2-3; 33d Medical Depot Company Annual Rpt, 1944, p. 7 and an. 1.
50. Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 7-8, 48-49, 117; Surg, CONAD, Annual Rpt, 1944, pp. 13-14; Surg, Delta Base Section, Annual Rpt, 1944, p. 1; Kendrick, Blood Program, pp. 447-52; Wiltse, Mediterranean, p. 409; Memo, Kenner to CofS, SHAEF, 12 Oct 44, sub: Report of Inspection of Medical Service of 6th US Army Group . . . , in Medical Division, COSSAC/SHAEF, War Diary, October 1944; 7th Medical Depot Company Combat Supply Operations Rpt, [19441, pp. 3-5. For details on the development of SOLOC, see Chapters IX and XIII of this volume.
51. Surg, Third U.S. Army, Annual Rpt, p. 169; Surg, Seventh U.S. Army, Annual Rpt, 1944, pp. 48-49; Surg, Ninth U.S. Army, Annual Rpt, 1944, p. 38; Surg, Ninth U.S. Army, Daily Journal, 1 Nov 44, Shambora Papers, MHI; 7th Medical Depot Company Combat Supply Operations Rpt, [1944], p. 9. For examples of corps supply points, see Surg, XII Corps, Annual Rpt, 1944, p. 6, and Surg, XIX Corps, Annual Rpt, 1944, p, 19. For group supply activities, see 68th Medical Group Annual Rpt, 1944, p. 28. On wing tanks, see Surg, XX Corps, Annual Rpt, 1944, pp. 7-8; Surg, 90th Infantry Division, Annual Rpt,1944, pp 18-19.
52. First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 154-55; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 163-66 and 168-70; Surg, Seventh U.S. Army, Annual Rpt, 1944, p. 118; Surg, Ninth U.S. Army, Annual Rpt, 1944, pp. 3738; Surg, Ninth U.S. Army, Daily Journal, 1, 24, 30 Nov and 22 Dec 44, Shambora Papers, MHI; Surg, Delta Base Section, Annual Rpt, 1944, pp. 1-2; 7th Medical Depot Company Combat Supply Operations Rpt, [1944], pp. 3-4. For armies hauling their own supplies, see 32d Medical Depot Company Annual Rpt, 1944, p. 5. Medical Division, COSSAC/ SHAEF, War Diary, October-December 1944, contains numerous inspection reports illustrating gradual supply improvement. For details on COMZ supply efforts, see Chapters IX and XIII of this volume.
53. Quotation from Memo, Kenner to CofS, SHAEF, 5 Dec 44, sub: Report of Inspection, Medical Service, First and Ninth US Armies . . . , in Medical Division, COSSAC/SHAEF, War Diary, December 1944. This document also gives the 28th General Hospital statistics. On evacuation times, see Kenner memo previously cited and his other reports in ibid., as well as Surg, 4th Armored Division Annual Rpt, 1944, pp. 21-22. On army death rates, see First U.S. Army Report of Operations, 1 Aug 44-22 Feb 45, bk. IV, pp. 199-200 and 204; Surg, Third U.S. Army, Annual Rpt, 1944, pp. 97-99; Surg, Seventh U.S. Army, Annual Rpt, 1944, p. 28; and Surg, Ninth U.S. Army, Combat Experience Rpts, October-December 1944, file HD 319.1-2.
![]()