



AMEDD Corps History > Medical Specialist > Publication
Professional Services of Physical Therapists, World War II
Colonel Emma E. Vogel, USA (Ret.),
Lieutenant Colonel Mary S. Lawrence, USA (Ret.), and
Major Phyllis R. Strobel, USA (Ret.)
When it was thought that World War II would extend over a long period of time, serious consideration was given to the conservation of manpower to meet a prolonged war. Toward this end, in 1943, the President appointed Mr. Bernard M. Baruch to serve as chairman of a committee [Advisory Unit for War and Postwar Adjustment Policies] to report on "The War and Postwar Physical Rehabilitation and Reconditioning Programs." Serving on this committee were representatives of the medical services in the U.S. Army, U.S. Navy, U.S. Public Health Service, and Veterans` Administration; representatives of the Federal Security Agency and the National Research Council; and several civilian physicians specializing in the field of physical therapy.
Several subcommittees were established to explore the needs in various fields, chief of which was a subcommittee to study the relationship of physical therapy to wartime rehabilitation and peacetime physical fitness preparedness. In this connection, a survey of physical therapy programs in Army general hospitals revealed common problems which included:1
1. The need for basic and clinical research to determine the reaction of normal and abnormal tissues to physical agents.
2. The need for standardization of equipment, particularly electrical apparatus.
3. The lack of standardization of maximal beneficial intensity, duration, and frequency of application of physical agents.
4. The need for more medical officers trained in this specialty.
5. The need for more trained physical therapists.
Obviously, the increasing patient load in Army general hospitals during the war precluded conducting basic research, but the findings of this committee clearly pointed out the vast amount of clinical research and standardization to be accomplished in this field. Limited clinical research subsequently carried on in these hospitals resulted in a reevaluation of the treatment programs for patients with combat injuries and the development of the specialized treatment programs. These programs were widely acclaimed not only in military circles but in civilian fields as well.
1Report, Subcommittee on Rehabilitation, Baruch Committee on Physical Medicine, 1943.
236
Types of Hospitals
There were four types of Army hospitals in the Zone of Interior during World War II; namely, general, regional, station, and convalescent. With the marked increase in the patient load early in 1944, it was decided that general hospitals would care for all patients evacuated from theaters of operations. At this time, some large station hospitals were redesignated as regional hospitals not only to care for patients normally seen in station hospitals but also to serve as general hospitals in the Zone of Interior. By December 1946, all regional hospitals were closed or had reverted to station hospital status.
Generally speaking, the general hospitals were named in honor of deceased military medical personnel and station hospitals were identified by the military reservation on which they were located. At the beginning of the emergency, there were five named general hospitals in the United States. These were markedly expanded by using every available space such as porches and wide corridors for additional beds. After the passage of the Selective Training and Service Act of 1940, plans were immediately implemented for the construction of additional hospitals. Altogether, 60 additional general hospitals were added. Some were of the cantonment type made of wood or brick; some were 2-story brick, tile, or stucco; 6 were in converted hotel buildings, and 5 were in converted civilian buildings not designed primarily as hospitals. Of these, 9 became operational in 1941; 11 in 1942; 24 in 1943; 12 in 1944; and 4 early in 1945.
The only major operational problems in these new hospitals, as far as physical therapy was concerned, were the supply of hot water, the size of the clinic, and the slow procurement of equipment. As originally planned, physical therapy clinics in the new cantonment-type general hospital were entirely too small to accommodate the heavy patient workload and required drastic expansion. Hotels and other buildings in which hospitals were established required considerable alteration to provide adequate space for increased workloads in the physical therapy clinics (fig. 60), especially in those designated as specialized treatment centers.
During the war there were 44 station hospitals in operation in the United States, most of which were of cantonment-type construction. When the troop training program was at its maximum, it was sometimes necessary to have more than one station hospital on a military reservation in order to care for the heavy patient load. All of these hospitals were similarly equipped insofar as the physical therapy clinic was concerned. As the movement of troops overseas was accomplished, the military population at these posts decreased and station hospitals were either closed or redesignated as regional hospitals. Since many of the physical therapists who had served at station hospitals for several
237
238
years were entirely unfamiliar with the specialized treatment programs, every effort was made to reassign them so as to afford them this invaluable experience.
Specialized Treatment Programs
As new Army general hospitals were activated early in 1942, it became obvious that specialists to staff them were limited in number. The solution lay in concentrating related specialties in one hospital and designating it a specialized treatment center. "By the time the peak patient load was reached in June 1945, there were 234 centers for 21 specialties with a total of 132,178 beds in 65 general hospitals in the United States."2
The extent of the specialized treatment programs is indicated by the number of general hospitals designated to provide them; for example, amputations, 7; neurosurgery, 19; orthopedic surgery, 35; thoracic surgery, 5; trenchfoot, 3; and vascular surgery, 3. In many instances, a general hospital was designated to develop more than one specialized treatment program. An example of this was Kennedy General Hospital, Memphis, Tenn., where programs were developed in neurology, neurosurgery, psychiatry, and general, orthopedic, and thoracic surgery.
Concentrating specific groups of patients in this manner was a definite advantage. Current treatment methods were evaluated, and as a result of study and research of a vast amount of clinical material, new programs were developed to insure a more effective therapeutic approach to patients in these groups. Physical therapists assigned to such centers had a most unusual opportunity to participate in these programs and in many instances made outstanding contributions.
Amputations
There were approximately 15,000 patients with major amputations in World War II. Early in 1943, five hospitals were designated as specialized centers for the treatment of amputees: Bushnell General Hospital, Brigham City, Utah; Lawson General Hospital, Atlanta, Ga.; McCloskey General Hospital, Temple, Tex.; Percy Jones General Hospital, Battle Creek, Mich.; and Walter Reed General Hospital, Washington, D.C.3 As the patient load increased, two other general hospitals were added: Thomas M. England General Hospital, Atlantic City, N.J., August 1944 (which became the largest amputation center in the United States), and McGuire General Hospital, Richmond, Va.,January 1945.
Many of the amputees arrived in the Zone of Interior with open wounds resulting from guillotine amputations. Approximately 20 per-
2Smith, Clarence McKittrick: The Medical Department: Hospitalization and Evacuation, Zone of Interior. United States Army in World War II. The Technical Services. Washington: U.S. Government Printing Office, 1956.
3War Department Memorandum No. W40-9-43, 6 Mar. 1943, subject: General Hospitals Designated for Special Surgical Treatment.
239
cent were upper extremity and 80 percent lower extremity losses. Many arrived with advanced necrosis and bone infection. Initially, the management of these patients differed from center to center, but later, procedures were relatively standardized throughout the Army hospitals.
Early in the war, amputation stumps were placed in traction until healed and ready for corrective surgery. Later, when it was determined that early physical therapy procedures hastened the healing process, patients with unhealed stumps were sent to the clinic for treatment. At Walter Reed General Hospital, the treatment of choice was the whirlpool bath, followed by zinc peroxide ionization. The zinc peroxide acted as a stimulant in the formation of granulation tissue. Some centers used localized ultraviolet irradiation to achieve this. The whirlpool bath relieved pain, increased circulation to the part, and cleaned unhealthy areas. Twenty-eight leg whirlpool baths were kept in almost constant use by these patients. The odor of osteomyelitis, which was almost overwhelming, was tempered somewhat by the use of a pine-scented germicide added to the water. With the large number of whirlpool baths in constant use during the day, it was necessary to install a separate hot water heater for the physical therapy clinic in order not to deplete the supply of hot water required for other hospital functions.
The use of stump massage varied from center to center. Some medical officers believed it was necessary to control edema, to free adherent scars, and to increase circulation. Others believed that massage was contraindicated as it softened the stump and irritated nerve endings at the suture line. Consequently, in some hospitals, massage was prescribed routinely in both preprosthetic and postprosthetic phases, whereas in other hospitals, it was not used at all. Bandaging during the prerevision stage was minimal to avoid circulatory constriction.
Following surgical revision, the amputee started a new physical therapy program designed to strengthen weak muscles, stretch contractures, and to shape the stump. A physical therapist gave each amputee a manual muscle test and worked out a set of therapeutic exercises designed to meet each patient`s individual needs. A vigorous exercise program was stressed (fig. 61). If a contracture was present, it was stretched manually by the physical therapist. Occasionally, when a stubborn contracture persisted, such as a hip flexion contracture of a high-above-knee amputation, weights were strapped to the stump to stretch and correct the alinement. In order to toughen the stump for the use of a prosthesis, tapping, or pounding the stump was sometimes indicated.
Proper bandaging by a physical therapist aided the shrinking and shaping of the stump. An effort was made to teach the amputee how to bandage his stump. Some patients learned to do this, but with others, the end results left much to be desired.
After the amputees received their prostheses, occupational therapists trained the upper extremity amputees in the use of their prostheses, and lower extremity amputees received gait instruction in the physical therapy clinic. Physical therapists working with the patients in amputa-
240
FIGURE 61-Exercise for the amputee. (Top) Wall pulleys. (Bottom) Modified Mennel table.
241
tion centers communicated with them using such words as Symes, Chopart, Gritti-Stokes, end bearing, ischial weight bearing, above knee (A/K), and below knee (B/K).
Because these patients were predominantly young healthy soldiers, with a strong drive to become gainfully employed civilians, they were extremely cooperative with their walking instructors. Walking areas were equipped with parallel bars, posture mirrors, plumblines, ramps, and sets of stairs (fig. 62). For walking instruction, the amputees were classified according to their disability into four groups: unilateral above knee, unilateral below knee, hip disarticulation, and bilateral. The classes were divided according to walking ability as beginning, intermediate, and advanced. The prosthetist brought each new prosthesis to the clinic. The patient was not allowed to take it with him to the ward until the physical therapist decided that he would not damage his stump by prolonged walking or develop an incorrect gait pattern. The men dressed in swim trunks and started on crutches in the beginning class. Balance, normal speed, and fit of the prosthesis were stressed, with the physical therapist constantly checking the stumps for blisters or areas of discomfort. Instructions were given in the hygienic care of the stump and stump socks.
In the intermediate class, the patient changed from the use of crutches to canes, learned the more common walking procedures, and developed uniform stride and rhythm. Those in the advanced class walked without assistance with arms swinging normally. The final objective of this class was to pass an achievement test which included many activities, such as falling and rising from the floor, stepping on and off a curb, hill climbing, and walking on rough terrain. Of prime importance was the ability of the physical therapist to correctly analyze the gait problem. She had to know what caused a patient to limp, whether it was weak musculature, a painful stump, a contracture, or improper fit or alinement. Having determined the reason, she helped him correct the fault so that he could walk as normally as possible.
Physical therapists on duty at amputation centers found this a very pleasant assignment. The convalescent patients were young healthy men, congenial, fun-loving, and active. They often challenged the physical therapists to basketball games and invited them to dancing classes conducted by the American National Red Cross. Occasionally, they needed an understanding person to accompany them on their first apprehensive appearance at a public beach.
Head injuries
Head injuries were direct results of bullets, shell fragments, blows by blunt objects, blast concussion, and other diverse causative agents. Salvage of these patients was high when compared with World War I mortality statistics. The reasons for this were many: chemotherapy, antibiotic therapy, early debridement by neurosurgeons in evacuation
242
243
244
hospitals close to the frontlines, and early physical therapy. Patients arrived in the Zone of Interior with histories of skull fracture, hematoma, meningitis, brain abscess, residual bone fragments, and imbedded foreign bodies. Many were candidates for cranioplasty and other surgical procedures. These patients were a tremendous challenge to all concerned with their eventual rehabilitation. Some were spastic hemiplegics or quadriplegics, some were athetoid and others atactic. Some suffered posttraumatic epilepsy. Visual field disturbances were common. Patients with aphasia were a perplexing problem.
The rehabilitation of the brain injured was a long, slow process, and both the patient and the physical therapist had to be acutely aware of this. Such patients were housed together in wards and treated in the clinic with similarly severely debilitated patients, so that they would not become discouraged by the lack of early recovery. At this time, the main goals of the physical therapy program for the head injured were to help the patient to avoid bad patterns of motion, to help him become cosmetically presentable, and to help guide him through his psychological gloom to a healthier, happier, social and emotional life. Before he started his long-term physical therapy program, the patient received a manual muscle test and his muscle strength was recorded. He was classified in one of three types of disabilities: spastic, atactic, or athetoid. Reeducation exercises differed for each type.
Some hemiplegics presented marked flexion deformities, whereas others had extremities that were almost flail; the spastic muscles were hyperirritable and overactive to stimuli. The patient`s voluntary control over these muscles was very much impaired. First the physical therapist passively exercised the part and then the patient slowly progressed to actively exercising by himself under constant careful supervision.
One of the problems the atactic patient faced was that of loss of kinesthetic sense. He found that he had to watch the extremity which was in motion so that he could determine just where it was in space. A head-down gait pattern was corrected ultimately by the utilization of vision. The patient was trained to focus on his environment. He had to relearn control of balance and coordination. The athetoid patient, distressed by involuntary unwanted overflow motions of the body, received instructions in relaxation and motion from the relaxed position.
The equipment needed for these patients was simple and easily constructed. Broad plywood skis were used to assist the patient with poor balance, thus giving him a wider standing base. A relaxation chair was built for those who could not sit in an ordinary straight chair. This chair, used during treatment periods, could also be wheeled about for socializing on the ward--an excellent morale builder of value in the treatment of severe cases were powdered boards which allowed gliding movements with neither friction nor the resistance of gravity.
In addition to specialized treatment received in physical and occupational therapy clinics, a generalized rehabilitation program was also planned for these patients. Games were organized for both ambulatory
245
and wheelchair patients. Group discussions were held on a variety of subjects, including current events. Self-care was stressed in feeding, dressing, and putting braces on and taking them off. Ambulatory patients policed their own ward areas. Speech therapy was provided when indicated.
Peripheral nerve injuries
The incidence of extremity wounds in battle casualties in World War II was 65 to 70 percent, and 15 percent of these were complicated by injury to one or more major nerve trunks. Peripheral nerve injuries were often combined with fractures, soft tissue loss, and vascular disturbances. By September 1944, treatment of these patients was concentrated in 19 neurosurgical centers.4
On the initial visit to the physical therapy clinic, the patient was usually scheduled for the following tests: manual muscle, sensory, dermometer, and one or more of the electrodiagnostic procedures.
Using her knowledge of anatomy, kinesiology, and the standard test positions, the physical therapist completed a manual muscle test, grading the patient`s response to applied resistance. The approximate level of the lesion was localized by this test and the extent of nerve damage evaluated. Followup tests were performed periodically.
A sensory test determined areas of anesthesia. A wisp of cotton and a pin were used to outline areas lacking superficial touch, sensation, and pain. Since the area of diminished sensitivity was similar to though not identical with that of no perspiration, a sweat test was often given. For this test, the involved extremity was swabbed with quinizarin dye, cobalt chloride, or starch iodide and the patient placed in a hot, dry cabinet bath which caused profuse full body perspiration. Dry areas of anesthesia were drawn on a diagram or the patient was photographed. If a cabinet bath was not available, an injection of pilocarpine nitrate was used or hot tea and aspirin were given to force perspiration.
The dermometer, an instrument for measuring skin resistance, was also used by the physical therapist as a diagnostic measure. High skin resistance was discovered where functioning sweat glands were sparse or absent.
Although the Army pioneered in developing electrodiagnostic procedures during World War I, much was done in the thirties to standardize these tests, both in civilian and military medicine. During World War II, the galvanic and faradic currents were used for the simplest and most common electrical tests. The faradic, a relatively rapid frequency current, excited nerve but not muscle tissue. If, for example, an apparent radial palsy responded to faradic current, the nerve was intact. This test gave valuable assistance in the diagnosis of functional paralysis. Response to the galvanic current was usually described by the physical therapist as brisk or vermicular. It was believed that this test
4Medical Department, United States Army. Surgery in World War II. Neurosurgery. Volume I. Washington: U.S. Government Printing Office, 1958, p. 13.
246
offered some indication as to the extent of nerve degeneration. The progressive sinusoidal current was used briefly for diagnostic purposes, but it was discontinued after the Golseth-Fizzell Constant Current Stimulator was introduced. This machine was known to most physical therapists simply as the EDX. It was developed by the National Research Council, scientists at Northwestern University, Evanston, Ill., and neurosurgeons at Percy Jones General Hospital. Since it was not commercially manufactured, it was reproduced in the occupational therapy department at that hospital and distributed to all neurosurgical centers. This well-calibrated stimulator produced a galvanic square wave which was used for testing the following: rheobase, chronaxy, strength-duration curve, tetanus ratio, and repetitive stimuli. Some form of heat, either the whirlpool bath or infrared irradiation, preceded the electrical testing. Because of the tremendous influx of patients with peripheral nerve disorders, physical therapists became extremely expert in the area of muscle testing and developed an awareness of the problems of all types of neurological dysfunction.
Physical therapy for patients with peripheral nerve injuries was used to increase circulation and nutrition to the part to decelerate the rate of atrophy and fibrosis, to keep joints mobile, and to reeducate weak muscles. The modalities most frequently used were the whirlpool bath, radiant heat, massage, therapeutic exercise, and electrical stimulation.
The whirlpool bath, unless contraindicated, was the modality of choice in treating patients with either upper or lower extremity peripheral nerve injuries. Infrared treatments were also used but had to be closely supervised to prevent burns in areas of anesthesia.
Mild massage was sometimes given to an extremity but not as routinely as in facial paralysis. Friction massage with lanolin for adherent scars was often taught to the patient to impress him with the need for self-help.
Passive exercise was used to maintain joint mobility; contracted tendons and fascia were stretched by the physical therapist. Active and resistive exercise of the uninvolved musculature was stressed. With the beginning of reinnervation of the muscles, a reeducational exercise program was started to assist the patient to recall voluntary function as it existed before injury. The physical therapists repeatedly stressed the responsibility of the patient for gaining good results. In addition to one or two clinic treatments a day, patients were instructed to perform exercises frequently throughout the day. The patients were also instructed in the use and care of their splints or braces.
In the 1940`s there was a flood of literature on electrophysiology and research in electrical stimulation of animal and human subjects. Many attempts were made to prove or disprove the value of this modality in the treatment of nerve injury. Most clinicians believed it to be of value; consequently, it was prescribed almost routinely. Controversy, however, existed relative to the most effective form of electrical current to be used, the duration of the treatments, the most feasible method
247
of application, and the desired strength of the muscle contraction to be elicited. Usually, the treatment was stimulation of individual muscles with manually interrupted galvanic current regulated to the patient`s pain and fatigue tolerance. Electrical stimulation was discontinued when voluntary contractions were noted.
Some patients suffered acute causalgia and were treated with a variety of modalities such as hot or cold whirlpool baths, paraffin baths, and sometimes even fever therapy. Only temporary relief was obtained by these methods.
Spinal cord injuries
The management of patients with spinal cord injuries in World War I and early World War II met with extremely discouraging results. After a series of conferences on the subject of transverse myelitis5 and intensive study of the problem, a new program was developed and put into effect in neurosurgical centers which resulted in one of the most outstanding successes in military medicine.
The purpose of this program was as follows: "A defeatist attitude is intolerable in the care of patients with traumatic transverse myelitis. Rehabilitation can and must establish a wheel-chair life for the majority and walking with the aid of braces or crutches for many. Self-support at a sedentary occupation is the ultimate objective. Maximal rehabilitation is essential for the preservation of morale and human dignity."6
The team approach which was developed combined the skills of all hospital personnel concerned with the patient`s care. This team included the neurosurgeon, orthopedic surgeon, urologist, plastic surgeon, internist, ward officer, physiatrist, nurse, physical therapist, occupational therapist, dietitian, physical reconditioning instructor, and hospital corpsman. When it was deemed appropriate, patients were included during the discussions of their progress.
The management problem was complex because of the many complications which existed with partial or complete transection of the spinal cord: paralysis, loss of bladder and bowel control, decubital ulcers, urinary tract infection, urinary calculi, rectal impaction, malnutrition, mental depression, osteoporosis, causalgia, and massive reflexes in those patients with spastic paralysis.
During the early phase of hospitalization, patients were treated on Stryker frames. They were turned every 2 hours, day after day; many times this was done by the physical therapist during the course of treatment. Radiant heat was administered to these patients primarily to
5Transverse myelitis conferences were held at Newton D. Baker General Hospital, Martinsburg, W. Va., 11-12 May and 20 June 1945; Hammond General Hospital, Modesto, Calif., 24-25 June 1945; Halloran General Hospital, Staten Island, N.Y., and Thomas M. England General Hospital, Atlantic City, N.J., 19-20 Oct. 1945. (Medical Department, United States Army. Surgery in World War II. Neurosurgery. Volume II. Washington: U.S. Government Printing Office, 1959, pp. 6, 127.)
6War Department Technical Bulletin (TB MED) 162, May 1945.
248
reduce muscle spasm. Massage was given to edematous extremities, and joint range of motion was maintained either passively by the physical therapist or actively by the patient as indicated. Since prognosis was difficult for these patients, the physical therapist had to be constantly on the alert for signs of returning function. Thorough muscle tests were performed routinely at 3-week intervals. For some patients, many months had to pass before a decision on irreversible change could be made.
The program was planned for progression from treatment in bed to wheelchair to mat exercises on the floor and ultimately to ambulation with braces and crutches, which was achieved by approximately 70 percent of the patients (fig. 63). The gait taught to most patients was the four point crutch-foot-crutch-foot pattern. This was more acceptable than the speedier swing-through gait which was taught as an alternate pattern for crossing streets and going places hurriedly.
At one center, Thomas M. England General Hospital, patients with decubiti received local ultraviolet treatments followed by applications of sugar and penicillin jelly. Other centers acclaimed a variety of other substances as valuable in treating decubital ulcers: these included castor oil, mineral oil, horse serum, zinc peroxide, gentian violet, tannic acid, petrolatum, and iodoform.
Instead of the few months` life expectance at complete bed rest predicted early in the war, many of these patients after an extremely arduous convalescence were actually driving their own hand-controlled automobiles and were achieving a measure of independence heretofore considered unrealistic for them.
After the cessation of hostilities, five Army general hospitals,7 designated as centers for the specialized treatment of patients with spinal cord injuries, were turned over to the Veterans` Administration. The rehabilitation of approximately 1,500 of these paraplegic patients passed from Army jurisdiction to the Veterans` Administration.
Thoracic injuries
In 1943, five general hospitals were designated as centers for the treatment of thoracic injuries: Brooke General Hospital, Fort Sam Houston, Tex., Fitzsimons General Hospital, Denver, Colo., Hammond General Hospital, Modesto, Calif., Kennedy General Hospital, and Walter Reed General Hospital.8 In August 1944, Baxter General Hospital, Spokane, Wash., was designated to replace the center at Hammond General Hospital. At Fitzsimons General Hospital, which was the largest such center, over 2,000 patients were treated in the thoracic surgery section during 1945. Of this number, 90 percent received physical therapy and many made rapid and even spectacular recoveries.
7Medical Department, United States Army. Surgery in World War II. Neurosurgery. Volume II. Washington: U.S. Government Printing Office, 1959, p. 14.
8Medical Department, United States Army. Surgery in World War II. Thoracic Surgery. Volume I. Washington: U.S. Government Printing Office, 1963, p. 171.
249
250
Patients in these specialized treatment centers represented a wide variety of diagnoses, including intrathoracic injuries from bullets, shell fragments, and blast concussion; chronic infections, such as tuberculosis, empyema, abscess, bronchiectasis; and tumors, benign and malignant. Surgical procedures included pneumothorax, phrenicotomy, pneumolysis, aspiration and drainage, thoracotomy, rib resection, thoracoplasty, lobectomy, and unroofing operations. Whatever the cause of the disability, the effects were much the same--poor posture and poor respiration.
During World War I and before World War II, the classical picture presented by the thoracic surgery patient was that of a chest cripple. A marked scoliosis developed, the weakened shoulder on the affected side dropped and was limited in range of motion, excursion of the rib cage was practically nonexistent, and vital capacity was extremely low. Prolonged bed rest produced general muscular debility, loss of appetite and weight, and low morale.
With the concentration of thoracic specialists in these centers, the physical therapy and surgical services developed an intensive program to rehabilitate patients with thoracic injuries. The treatment program was divided into three phases: preoperative on the ward, early postoperative on the ward, and postoperative in the physical therapy clinic and the physical reconditioning gymnasium. Several days before the
251
patient was scheduled for surgery, the physical therapist contacted him on his ward to explain the results he could expect and what was expected of him following surgery (fig. 64). During these visits, the physical therapist demonstrated all the exercises, answered questions, and used conversation therapy to allay apprehension. The patient performed his exercises each day until he went to surgery.
In the absence of postoperative complications, the patient was ambulating for short periods the first day after surgery. Graduated breathing and posture exercises were also started. Breathing exercises, designed to help gain maximum ventilation rapidly, were of several types: diaphragmatic or abdominal, costal, and focal.9 Deep coughing was stressed so that excessive fluids would be expectorated in a normal manner. Since this was pain producing, the physical therapist often assisted by splinting the patient`s rib cage with a large bath towel held firmly wrapped around the chest.
Postural exercises were performed to insure correct body alinement (fig. 65). Shoulder range-of-motion exercises were included because of stiffness and pain in that arm resulting from positioning during surgery. As a general rule, patients were treated on the wards for 2 weeks following surgery. The exercise program was then continued in the physical therapy clinic at a much more strenuous level. Graduated heavy weight lifting was started as were workouts on the bicycle, the rowing machine, and the shoulder wheel. Patients with prolonged pain or discomfort were given infrared treatments or hot fomentations. In the winter months, general irradiation by the carbon arc lamp was given, and in the summer, exposure to sunlight was used for its tonic effect. This program eliminated the physical characteristics which had previously typified the chest cripple.
The physical therapy staff and students participated in a continuous educational program consisting of lectures, demonstrations, ward rounds, clinical conferences, observation of fluoroscopic examinations, and observation in surgery.
Vascular injuries
Many Army general hospitals admitted patients with vascular conditions; however, by the end of the war, only three hospitals10 were designated as vascular surgery centers: Ashford General Hospital, White Sulphur Springs, W. Va.; DeWitt General Hospital, Auburn, Calif.; and Mayo General Hospital, Galesburg, Ill. Trenchfoot centers11 were
9"The English believed that lungs can be selectively reexpanded by the focal exercises; others take little cognizance of them except as a part of the general exercise program. This is probably an unimportant point over which to argue, since general agreement exists as to the same necessity for concentration of exercise effort to these chest segments as there would be for an intensive exercise program for any other part long disused." Rose, D. L.: High Lights of Physical Medicine at Walter Reed General Hospital, 1941-1946. Arch. Phys. Med. 28: 99-108, February 1947.
10Medical Department, United States Army. Surgery in World War II. Vascular Surgery. Washington: U.S. Government Printing Office, 1955, pp. 2-3.
11Medical Department, United States Army. Cold Injury, Ground Type. Washington: U.S. Government Printing Office, 1958, p. 78.
252
253
located at Brooke General Hospital; Letterman General Hospital, San Francisco, Calif.; Mayo General Hospital; Ashford General Hospital; U.S. Army General Hospital, Camp Butner, N.C.; and U.S. Army General Hospital, Camp Carson, Colo. Except for the excessive trenchfoot patient load, the vascular conditions treated were comparable to those treated in civilian hospitals, although there was a much greater number in the younger age group.
The physical therapy section at Ashford General Hospital reported that the total number of vascular conditions treated during the years 1943, 1944, and 1945 was 1,675.12 The statistical breakdown of this number was as follows:
|
Acrocyanosis and vasospasm |
113 |
|
Arteriosclerosis obliterans |
18 |
|
Arteriovenous fistulas |
93 |
|
Combined bone, soft tissue, and blood vessel injuries |
931 |
|
Ligation of major stems |
91 |
|
Raynaud`s disease |
5 |
|
Thromboangiitis obliterans |
33 |
|
Thrombophlebitis |
58 |
|
Trenchfoot and frostbite |
297 |
|
Varicose ulcers |
11 |
|
Volkmann`s ischemic contracture |
25 |
Despite the great wealth of clinical material in the field of vascular disorders, the specific results of physical therapy were difficult to evaluate. Since the task in wartime was to achieve maximum benefit in the shortest possible time, a combination of modalities was often prescribed, thus ruling out the study of one isolated treatment procedure. Also, many of these patients had only a short period of hospitalization in the Zone of Interior and were discharged from service with no subsequent followup by Army medical officers.
Cold injuries cut a tremendous swath in our fighting strength around the world in campaigns from Attu to the Bulge. Trenchfoot, immersion foot, and frostbite resulted from prolonged exposure to cold and dampness. The soldier pinned to his foxhole by enemy fire often found his cold, wet feet to be swollen, numb, and discolored. The soldier adrift on a sea-drenched liferaft had much the same symptoms. All experienced thermal reactions comparable to those of patients with severe burns. Their feet were often blistered, gangrenous, and lacking normal circulation and nerve supply.
During the acute phase overseas, these men were placed on bed rest with feet elevated at room temperature or chilled with ice packs. By the time they were evacuated to the Zone of Interior, their condition was generally subacute or chronic and they were ready for physical therapy and ambulation. The objectives of physical therapy were to increase circulation to the involved parts, decrease pain and edema,
12Report, Capt. Carl Levenson, MC, Chief, Physical Therapy Section, Ashford General Hospital, White Sulphur Springs, W. Va., to Office of The Surgeon General, 12 Dec. 1945, subject: Addition to Report on Physical Therapy in Vascular and Neurosurgical Conditions.
254
increase joint range of motion and muscle strength, and encourage the patient to walk normally.
A variety of modalities were available to obtain these objectives (fig. 66). Whirlpool baths were of value to these patients, as the temperature and agitation of the water could easily be regulated to accommodate the condition. Diathermy to the lumbar area was prescribed for the reflex circulatory changes it produced in the extremities. Mecholyl (acetyl-B-methylcholine) iontophoresis and suction pressure apparatus were also used to increase vasodilatation. Massage and passive exercises were administered by the physical therapists, and patients were instructed in performing Buerger`s exercises, and were advised to stop smoking, stop worrying, and to take long walks. It was believed that these patients would present no postwar problem, although it was expected that many would continue to experience discomfort upon exposure to cold weather. Physical therapy modalities used in the treatment of patients with other vascular disorders were similar to those administered for cold injuries. The success of these measures rested on early diagnosis, early treatment, and the severity of the disorder.
Although patients with cold injuries did not present any great medical or surgical problem in the Zone of Interior, they did occupy a tremendous number of hospital beds. Numerically, they were an overwhelming drain on hospital facilities. The following quote is from a chapter written 15 years after the end of World War II by a physical therapist who was then stationed at Brooke General Hospital, a trenchfoot center. With vivid recall she stated, "I can remember classifying patients [with trenchfoot] who had no open lesions into a group that shared the Hubbard tank. We placed two large boards across the tank that would serve as benches and every 20 minutes 10 patients would share a whirlpool treatment."13
Other programs
There were many specialized treatment centers in the Zone of Interior; the professional activities of physical therapists in all of them cannot be described in detail. Some programs made unique or outstanding contributions. Army and Navy General Hospital, Hot Springs, Ark., offered spa therapy for patients with arthritis and poliomyelitis. It was the only center designated for the treatment of poliomyelitis. Both the main hospital and Eastman Annex (formerly a resort hotel) provided thermal mineral baths. Included was a hydrotherapeutic pool equipped with exercise tables. Most of the poliomyelitis patients were in the subacute or convalescent phase, having been transferred to Army and Navy General Hospital from points all over the world. Reports from this hospital describe the treatment as a modified Kenny method
13Personal correspondence by the author with Georgiana Windham Johnson, formerly 1st Lieutenant, MDPT, AUS.
255
256
which included moist hot packs, baths, and underwater and reeducational exercise. Prevention of contractures and fatigue was emphasized. The physical therapists worked in close harmony with the orthopedic surgeons. Braces, splints, tendon transplants, and joint fusions were provided when indicated.14
Army and Navy General Hospital was designated the Army arthritis center in December 1943. Approximately 65 percent of the arthritic patients admitted were diagnosed as having either rheumatoid arthritis, fibrositis, or osteoarthritis. These patients were considered candidates for physical therapy procedures. Since most types of arthritis were progressive and of unknown etiology, no cure could be offered. Relief of pain and maintenance of normal joint range of motion were the treatment goals. Even though gout was primarily a dietetic problem and psychogenic arthritis a psychiatric problem, all received some form of hydrotherapy. Educational programs, including lectures and films, were provided for all patients. Some of the subjects presented were: "The Meaning of Rheumatism and Arthritis," "Fads, Fancies and False Concepts of Rheumatism," and "Home Physical Therapy."
At Gardiner General Hospital, Chicago, Ill., one of the orthopedic surgery centers, Capt. Thomas L. DeLorme, MC, developed an intensive exercise program in an attempt to shorten the hospitalization period for orthopedic patients. He had observed that, in the development of powerful muscles, amateur and professional weight lifters exercised with extremely heavy weight loads. Theorizing that heavy resistance with a low number of repetitions would produce muscular hypertrophy and power, he incorporated this concept in his exercise program. This was a complete reversal of the belief that low resistance with many repetitions (for example, bicycle, wall pulleys) was the treatment of choice for weak, atrophied muscles. He believed that the repetitive low resistance exercise produced endurance and should be used only after power was attained. The results of his study were so impressive that the DeLorme progressive resistance exercise program was immediately incorporated in physical therapy clinics throughout the Army (fig. 67).
Equipment
Physical therapy clinics in the Zone of Interior were normally adequately equipped with the standard items listed in the Army Service Forces Supply Catalog.15 Early in the war, many items could not be immediately obtained from the manufacturers. This situation was gradually eliminated as production capability increased. In the early forties, there seemed to have been undue enthusiasm for the electric
14A report on the progress made by poliomyelitis patients treated at Army and Navy General Hospital is contained in the following article: Torp, M. J.: Poliomyelitis: Functional Progress Report of Fifty Cases Approximately Five Years Post-Onset. Phys. Therapy Rev. 33: 351-358, July 1953.
15Army Service Forces Supply Catalog 10-2, May 1945.
257
258
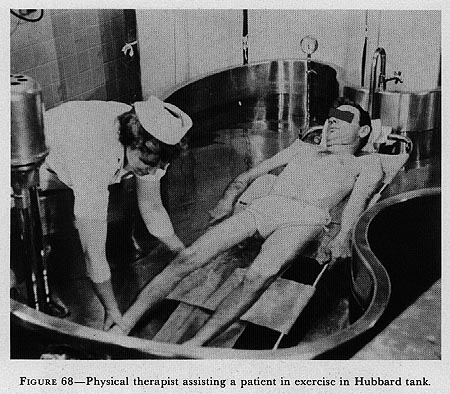
FIGURE 68-Physical therapist assisting a patient in exercise in Hubbard tank.
{kind=link}
cabinet bath. Even if space were available for this large piece of equipment, its use was seldom prescribed, and eventually this item was deleted from the supply catalog.
From time to time, new and additional items of equipment were tested in Army hospitals, and if acceptable, such items were standardized and listed in the catalog. Among such items tested were an invalid walker with attachments; head and shoulder slings; various pieces of exercise equipment, plinths, therapeutic lamps, Hubbard tank (fig. 68); and a galvanic stimulator. With the widespread use of physical therapy equipment, an unusual opportunity was afforded to evaluate such items. If it was found that a piece of equipment did not meet the specifications or did not hold up under heavy usage, it was recommended the item be deleted from the supply table.
Types of Hospitals
Hospitals in oversea theaters of operations were set up in any available building which afforded adequate space, such as schools, warehouses,
16Unless otherwise indicated, the source of information utilized in the preparation of this section is from accounts of physical therapy activities extracted from hospital annual reports and narrative reports of chief physical therapists.
259
apartment houses, hotels, military barracks, museums, churches, and even converted stables. In addition, some were in newly constructed cantonment-type buildings, some were in civilian and military hospitals requisitioned by the U.S. Army, and some were in tents or nissen huts. In the tropical areas of the Pacific and Asia, native construction materials such as bamboo and grass were utilized and many thatch-roofed hospitals operated as efficiently as did those of conventional design (fig. 69).
Operational Problems
The fundamental aims of physical therapy programs remained essentially the same in oversea units as in permanent installations in the United States. In a hospital overseas, however, the modalities were often limited and treatments frequently reduced to the barest essentials. Location of hospitals (front or rear echelon) and military campaigns determined the types of cases and the workload. With chameleon rapididity, some units changed from station to general hospitals and from evacuation hospitals to holding units. Reports show that sometimes the hospital bed occupancy dropped from 800 to 0 in 2 days, or increased from 800 to 1,600 in 12 days.
Since oversea physical therapy clinics were as varied in space and arrangement as the hospitals of which they were a part, no general descriptive statements can be made. Those operating in temporary cantonment-type buildings possessed no characteristics which distinguished them from hospitals of a similar type in the Zone of Interior. On the other hand, descriptions of some of the other clinics point out the problems faced by physical therapists in a wide variety of situations. Though scattered from Ireland to India, they encountered many identical problems. The degree of ingenuity demanded of a physical therapist in setting up an oversea clinic depended largely on the type of housing to which the unit was assigned.
Some of the oversea hospitals were housed in permanent buildings which had not originally been designed for hospital use. For example, in 1944, in the Mediterranean (formerly North African) Theater of Operations, U.S. Army, a former Italian Police School which had been extensively damaged by shellfire was chosen as the site of a station hospital. The physical therapists were dismayed to find that the space allotted for their clinic was littered with debris. Much digging uncovered a beautiful red and black tile floor in excellent condition. Much scrubbing revealed beautiful wall paintings which added to the colorful and even festive appearance of the clinic.
The report of a physical therapist in a general hospital in France, early in 1945, included a description of a physical therapy clinic operated under tentage. Two ward tents pitched side by side on a concrete base provided a large treatment room and smaller rooms for the whirlpool baths and gymnasium. Four wooden arches raised the sloping tent walls
260
261
FIGURE 69-Continued. C. Physical therapy building, India. D. Physical therapy clinic, Iran.
262
263
FIGURE 69-Continued. G. Physical therapy, Mediterranean Theater of Operations.
to provide adequate overhead space. The sides of the tent were winterized and heat was provided by standard Army stoves.
The physical therapist assigned to the 27th Station Hospital, New Caledonia, opened her clinic in March 1943 in a pyramidal tent, where no running water was available. As the number of patients grew, the clinic moved to a ward tent. One year later, the tent was replaced by a wooden building with modern equipment.
At the 8th General Hospital, New Caledonia, the physical therapy clinic at first was located in the main clinic building shared with the dental and eye, ear, nose, and throat clinics. Because of the lack of space, two of the three physical therapists confined their work to the wards. Bakers or lamps had to be carried to each ward where there were only two wall plugs, located at opposite ends of the ward. No extension cords were available. In addition, the beds were not of a suitable height on which to comfortably administer massage. It was 10 months after the 20th General Hospital opened in Ledo, India, before an adequate physical therapy clinic was constructed of concrete with a tin roof overlayed with leaf thatching. The staff, meanwhile, plodded through muddy paths from one ward to another to administer massage and moist heat.
264
While keeping warm posed a problem in some of the hospitals in the European Theater of Operations, U.S. Army, and in the Mediterranean theater, the reverse was true in some of the areas in the Pacific. A physical therapist on duty in a hospital in Saipan reported that the regulation of the temperature inside the tent which housed the physical therapy clinic posed a serious problem in that hot, humid climate. With the sun beating down all day on the black-topped tent, and with heat generated by bakers and infrared lamps, it was often impossible to remain in the tent for any length of time. This problem was solved by making a false ceiling of bed sheets which measurably decreased the temperature inside the tent.
The 7th Station Hospital was the first unit in the Mediterranean theater with physical therapy facilities. Two weeks after the landing of U.S. and British troops, on 7 November 1942, the hospital was established in Oran, Algeria, in buildings which were part of a French civil hospital area. The sections for officer and enlisted patients were in different locations in the city which necessitated more physical therapy personnel than would have been necessary for a single centralized unit.
Frequently, convoys of battle casualties were received in the hospital only a short time after the arrival of medical service personnel and equipment. In such situations, all hospital personnel, regardless of their official designation, expended every effort to prepare the hospital for the immediate reception and care of these patients. Since the services of carpenters, plumbers, and electricians were required in the hurried preparation of operating rooms, kitchens, and wards, the preparation of the physical therapy clinic was understandably delayed. Physical therapists were not idle, however, and served wherever they were needed, assisting in the preparation of dressings, the application of plaster casts, and the supervision of food trays for ward patients.
When physical therapy clinics were housed in permanent-hospital-type buildings, no major problems were encountered. When the hospitals occupied buildings not originally designed for hospital use, it was necessary to accomplish extensive alterations and repairs. In such cases, the physical therapist usually made the plans for necessary changes and executed them with the assistance of enlisted personnel assigned to the clinic. In fact, many physical therapists temporarily assumed the role of painter, plumber, carpenter, or electrician. Since equipment needed for repair and construction was always in short supply, the number of hammers, saws, pliers, nails, and paint brushes were never sufficient to meet the demand. Surprisingly, some physical therapists had the foresight to include complete tool kits in their personal luggage.
Treatment tables and plinths were immediate requirements in all clinics. If the physical therapist was fortunate enough to acquire the necessary lumber for such construction, the plinths were jealously guarded. In one hospital, the physical therapist reported that the plinths had been dismantled, packed, moved, and reassembled four tlmes. When lumber was not available for the construction of plinths, mess
265
tables were sometimes pressed into service and pads were made by placing folded blankets in a mattress cover. Hospital beds with boards placed under the mattresses were also used.
In spite of the fact that furniture was difficult to obtain, physical therapy clinics were usually cheerful and attractive. Physical therapists made an effort to brighten their clinics by placing small plants and flowers around, and by decorating otherwise drab and uninteresting linen hampers, receptacles, and other pieces of furniture. By these added touches, they hoped to improve the morale and attitude of the patient.
The type and availability of electrical current was always a matter of prime consideration. In several oversea areas, it was necessary to use transformers to rectify the 220-volt local supply in order to use the standard 110-volt electrical equipment manufactured in the United States. Because of extensive damage to power plants and lines during the war, the electrical current in some areas was so undependable as to be almost useless. In these cases, electrical power was supplied by hospital generators. Often the hospital power plant could not generate electricity sufficient for all sections to use their equipment simultaneously, and a schedule had to be worked out.
Another problem commonly encountered was the lack of an adequate supply of hot water for operating the whirlpool baths. It was a rare instance when the available supply of hot water was constant and adequate. In some hospitals, water was heated on field ranges or on improvised stoves (fig. 70) and carried to the physical therapy clinic in large containers.
Water supply in many areas was inadequate. The 137th Station Hospital on Guadalcanal reported this was a constant problem. Many, many times the hospital was without water except what could be hauled in one 250-gallon tractor. In some units, water pressure was often so low that it took hours to fill the whirlpool tubs.
One physical therapist who worked in a tent clinic on Saipan wrote: "With a despairingly inadequate water supply, policing a clinic in that part of the world was indeed a puzzle--not that it was expected to sparkle or shine (only the sun shone there!), but some semblance of cleanliness was hoped for. The floor had either a covering of dust which had blown in or one of mud which had been tracked in. Large slimy snails, which crawled in at night leaving grayish white trails in every conceivable place, were a constant source of annoyance."17
In the preparation of the clinic and the execution of the many necessary improvisations, the physical therapist received invaluable assistance from the enlisted personnel assigned to the clinic. The cooperation, ingenuity, and inventive genius of these men were often referred to in the hospital reports. Physical therapists and enlisted personnel alike were proud of their achievements.
17Report, 1st Lt. Barbara M. Robertson, MDPT [February 1946], Physical Therapy in Saipan, p. 8.
266
FIGURE 70-Improvised water heater, China-Burma-India. (Courtesy of National Library of Medicine.)
Equipment
The equipment in physical therapy clinics in oversea hospitals consisted of three types: standard apparatus, which was shipped from the United States; equipment procured locally; and that which was improvised. Because of changing shipment priority and availability, the supply list for oversea physical therapy clinics was revised several times during the war.
267
Distribution of these items was not always made in accordance with bed capacities, and frequently, both small station and large general hospitals received the same number of items. On the whole, the number of issued items was considered adequate and consistent with local conditions. A report from U.S. Forces, India-Burma Theater, states that the "results of the program validated the War Department policy of providing hospitals with but the major items of physical therapy equipment, since American ingenuity could be counted on to complete the paraphernalia required for the program."18 The ingenious American physical therapists and enlisted personnel improvised equipment (fig. 71). They used bamboo, scrap lumber, salvage pipe, and salvage parts from aircraft and vehicles. Many of the weights for resistance exercises were made of tin cans filled with cement, rocks, or sand. Tools and specialized labor were frequently provided by the U.S. Army Ordnance Department and the U.S. Army Signal Corps.
No gymnasium equipment was shipped overseas nor were diathermy machines because the current interfered with radio reception and transmission. A few hospitals in Australia and Hawaii used locally acquired long- and short-wave diathermy apparatus. The Signal Corps recommended that these units be used only in electrically shielded rooms.
Whirlpool baths were generally available in all theaters. After inspecting equipment in the Mediterranean theater, one medical officer reported that he saw no adequate reason for transporting this bulky equipment overseas. He recommended that ordinary bath tubs, large basins, or galvanized iron cans be filled with hot water and used instead.19
Posture mirrors proved very difficult to acquire. At one clinic, numerous small mirrors were diligently pieced together. A physical therapist in New Caledonia, "after much finagling," procured a half-length sheet of metal with a polished reflecting surface.20 It was placed on an easel so that it could be tipped down for gait instruction and up for reeducation exercises in facial palsy. She also devised an ankle exerciser made from jeep cushion springs supplied by the motor pool.
A most unusual heat modality was that used by the physical therapist interned at Santo Tomas Internment Camp, Manila, Philippine Islands. "In back conditions, the iron was usually more effective. The part to be treated was covered with a sheet and two layers of blanket. The process was similar to ironing, except that it was necessary to withhold some of the weight of the iron.21
At the 31st Station Hospital, New Caledonia, an ingenious quadriceps exerciser was made by building tracks on which a chair mounted on wheels could be pushed back and forth. Resistance was provided by
18Stone, James H.: History of the Army Nurses, Physical Therapists, and Hospital Dietitians in India and Burma, October 1945, p. 74. [Official record.]
19Essential Technical Medical Data, Mediterranean Theater of Operations, U.S. Army, for March 1945, dated 29 Apr. 1945.
20Lindberg, Geraldine D.: History of the Medical Department Dietitians and Physical Therapists, 29th General Hospital, Experiences of a Physical Therapist in New Caledonia and Korea, p. 3. [Official record.]
21P.T. Department, The Army Nurse 2: 10-11, June 1945.
268
269
weights attached to a pulley system. The patient sitting in the chair extended his legs by pushing back against the weights. The 21st Station Hospital supplemented their exercise apparatus with weights strung on two pairs of sturdy pulleys obtained from one of the scuttled ships in the harbor of Massaua, Eritrea.
In the early days of the Italian campaign, two physical therapists were told on 24 hours` notice to set up a clinic. No standard equipment was available. They succeeded in obtaining 2 examining tables, 6 blankets, 25 bath towels, and 6 buckets. Hot water was heated on a pot-bellied stove. Fifteen candles were melted in two tin cans and the paraffin was
270
FIGURE 71-Continued. E. Baker. F. Rowing machine and shoulder wheel, India.
271
272
applied by a piece of gauze wrapped around the end of a stick. Histologic paraffin was used in some instances. In Khorramshahr, Iran, paraffin was secured from a nearby oil refinery.
Climate
Women accustomed to the temperate climate in the Zone of Interior learned to adjust to the tropical climate. Adjustment to this environment and professional efficiency were found to be related. A survey made in the India-Burma Theater, in 1945, revealed that a tropical environment did not necessarily result in overwhelming physical and mental devastation in women.22
Climatic conditions definitely affected the administration of treatment. High environmental temperature and humidity had to be considered in the type, degree, and frequency of treatments. To avoid excessive fluid and electrolyte loss, precautions had to be used in administering heat, massage, and in the degree of exercise given.
A physical therapist assigned to the 31st Station Hospital, a tent hospital, reported: "Technique in treatment was changed a bit because of local conditions. We had been taught never to remove our hands from a patient during massage, but the author of that idea must never have worked in a mosquito-ridden swamp land. We learned to massage with one hand and swat with the other any mosquito threatening to lunch on either patient or operator."23
Workday
Often it was necessary to operate oversea clinics 9 or 10 hours a day for 7 days a week. In spite of the long days, much work such as recordkeeping and muscle tests was done in the evenings. Most clinics were understaffed and patient loads were heavy. Welcomed assistants were nurses, enlisted personnel, civilian nationals, convalescent patients, and even prisoners of war. As an outgrowth of the personnel shortage, an economical system of grouping patients evolved; for example, two or three to a single heat lamp or whirlpool bath. Group exercise was a common practice.
Physical therapists in the Communications Zone treated not only U.S. military personnel, but also allied military personnel, prisoners of war, and civilians in areas without adequate medical facilities. The language barrier was a deterrent in some physical therapy programs. Since administrative and professional procedures in the various theaters and areas followed much the same pattern, only the physical therapy programs in the European theater will be described.
European Theater of Operations
Normally, hospital personnel were transported to the European theater as integral units by water transportation. This gave opportunity
22See footnote 18, p. 267.
23See footnote 20, p. 267.
273
for members of the hospital unit to become acquainted with one another personally as well as professionally. Later, under combat conditions, this relationship was most important in the successful development of many timesaving devices and procedures. In the European theater, as in other theaters and areas, the medical officer in charge of the physical therapy clinic was usually designated from within the surgical service and most frequently from the orthopedic section. A mutual understanding between the medical officer in charge of physical therapy and the physical therapists concerning the most effective treatment procedures under the circumstances at hand lessened demands upon the medical officer and released him from clinic activities during periods of increased military operations at which time the primary responsibility of all medical officers was the emergency care of the wounded. The physical therapists functioned as liaison officers between the medical officer in charge of physical therapy and the ward officers, some of whom had had only limited knowledge of physical therapy. As in other theaters and areas, enlisted personnel trained to assist in administering physical therapy were an invaluable asset in the treatment program.
With expanding patient loads, the need for specific physical therapy measures was repeatedly reevaluated. The application of massage and various forms of heat succumbed oftentimes to emphasis on exercise. On occasion, exercise consisted of an instruction period only, given before transfer of the patient to another hospital in the chain of evacuation. The value of group exercises was learned early in the European theater. As workloads assumed staggering proportions, classes were formed for exercise instruction of patients with similar disabilities.24 It was soon realized that a powerful psychological stimulus for recovery was at work in patients engaged cooperatively and competitively in a treatment program for their common conditions. The experiences of physical therapists at the 5th General Hospital shortly after arriving in Ireland, in May 1942, served as a springboard from which to convert an overwhelming individual patient load into a dynamic program of group exercise.25
Concurrently, the need was observed for a general exercise program designed to maintain total body health to the extent possible while the specific injury was undergoing treatment. At the 5th General Hospital, where the first program of this type was developed, aspects of the British Army rehabilitation plan were adopted. Late in 1942, Miss (later 1st Lt.) Edna Blumenthal, with the encouragement and assistance of the medical staff, introduced general exercise classes for patients in all stages of recovery, some of whom progressed to complete convalescence. (Later in England, patients were transferred to other centers for final convalescence.) In the development of this program, she was assisted by British Army medical officers who contributed generously of their time,
24Group exercises for patients wcre first used in World War I. See chapter III, p. 43.
25Lawrence, Mary: History of Physical Therapy in the European Theater of Operations, U.S. Army, World War II. p. 42. [Official record.]
274
knowledge, and experience. This general exercise program was later incorporated into the total rehabilitation program. (See Appendix H, p 607.)
At times, when both general and station hospitals assumed the functions of evacuation units, physical therapists performed tests to evaluate the extent of nerve injuries, instructed patients in positioning and exercise, and assisted in the application of casts and splints.
The support of British physical therapists extended individually and through The Chartered Society of Physiotherapy was a source of inspiration and assistance to U.S. Army physical therapists in England. Through the efforts of Miss Olive Sands, a member of that society, arrangements were made for the first meeting with Army physical therapists stationed in England. This meeting was held in the headquarters of that organization in London. Here discussions and demonstrations were focused on postural drainage and the physical therapy management of patients with asthma and postsurgical chest conditions.
Later, speaking of this meeting, Miss Sands said, "Surely the need for a world confederation became apparent at these meetings and there is little doubt that the seed which grew into the World Confederation of Physical Therapy was planted at this time."26
The advent of drugs such as the sulfonamides and penicillin, new surgical procedures,27 and the desirability of early mobilization brought mounting opportunities for the use of physical therapy in the preservation and restoration of body function. With the new methods of wound closure and long bone immobilization, the value of early physical therapy was dramatically demonstrated during World War II.
Burns
The growing awareness of the value of early treatment in the restoration of function resulted in a reevaluation of the treatment of patients with severe burns.28 Body temperature saline baths, used for removal of dressings, afforded excellent opportunities for active underwater exercises necessary to prevent joint contractures during the period prior to skin grafting. Passive and assistive movements were given to enable the patient to obtain as full a range of motion as possible under the soothing effects of the saline bath. At times, ultraviolet irradiation was given to stimulate healing. After skin grafting, in the absence of complications, assisted active and passive motion was usually begun on approximately the third or fourth postoperative day. With complete healing of the grafted areas, gentle massage with sterile lanolin and graduated exercises were initiated. Early ambulation followed a pattern similar to that for other injuries.
26Letter, Miss Olive Sands, St. Anselm`s Vicarage, Kensington Cross, S.E. 11 London, England, to Maj. Mary S. Lawrence, 19 May 1960.
27(1) Circular Letter No. 131, Office of the Chief Surgeon, Headquarters, European Theater of Operations, U.S. Army, 8 Nov. 1944. (2) Circular Letter No. 23, Office of the Chief Surgeon, Headquarters, European Theater of Operations, U.S. Army, 17 Mar. 1945.
28Bricker, E. M.: Burns. M. Bull. European Theat. Op. 11: 11-16, 1943.
275
Cold injuries
The cold, wet winter of 1944-45 exacted a staggering toll of U.S. fighting forces in their headlong rush to the Rhine, often accounting for more victims than enemy action.29 The tissue damage inflicted by chilling, damp, or dry cold required specific treatment.30 In the acute state of active hyperemia, maintenance of minimal tissue metabolism precluded active physical therapy. The graduated vascular exercises of Buerger were usually begun during the period of bed rest as hyperemia and edema subsided. Early movement of ankle and toes was encouraged. One group of patients treated by this method was completing 10-mile hikes 1 month after injury.31 In severe cases where muscle and nerve damage was present, producing pes cavus and clawfoot deformities, specific exercises to prevent complete fibrosis of tissue and to strengthen intrinsic foot muscles were necessary. Instruction in walking and graduated marches assisted in the restoration of normal function.
Hand injuries
The recognition of the importance of specialized treatment for patients with hand injuries, carried out at designated centers, was a long step forward in preserving and restoring useful function of this vital member. As in other war injuries, accumulating experience pointed to the necessity for early wound closure or plastic repair and emphasized the value of exercise supervised by physical therapists from the beginning and pursued during the entire period of hospitalization.32 Immobilization was reduced to a minimum, and in fractures of the hand, improved methods of skeletal traction were also conceived to provide some degree of continuing motion during its use. At one of the hand centers, an ingenious exerciser,33 used in conjunction with physical therapy, incorporated resilient wires in a frame to which the digits were attached by slings in such a way that a constant stimulus for exercise was provided (fig. 72). Graduated exercise under supervision was usually begun the first few days following surgery. The whirlpool bath was extensively employed preoperatively and postoperatively, and cross-contamination of open wounds was rarely encountered. One hospital, after a number of experiments, used sodium hypochlorite in the whirlpool bath to reduce the danger of contamination. (See Appendix I, p. 609.) Other equipment in general use for hand and finger exercises included rubber balls, marbles, syringe bulbs, pieces of broomstick, Plasticine, and assorted improvised devices. The need for the patient to assume responsibility for his own exercises was always emphasized.
29See footnote 11, p. 251.
30Circular Letter No. 126, Office of the Chief Surgeon, Headquarters, European Theater of Operations, U.S. Army, 18 Oct. 1944.
31See footnote 11, p. 251.
32Medical Department, United States Army. Surgery in World War II. Hand Surgery. Washington: U.S. Government Printing Office, 1955, p. 182.
33Rommel, C. H.: An Improvised Hand Exerciser. M. Bull. European Theat. Op. 32: 25-26, July-August 1945.
276
277
Nerve, brain, and spinal cord injuries
Evaluation of extent of nerve damage and treatment of peripheral nerve injuries by physical therapy measures constituted an important part of the management of these patients. The commonly used galvanic-faradic testing currents furnished information on nerve degeneration. Manual muscle, skin sensory, and resistance tests, developed in various hospitals, were also used in the evaluation of peripheral nerve injuries. The effectiveness of physical therapy was made possible not only because the patient was received relatively soon after wounding and surgery but also because practices in evaluation, treatment, and immobilization were being modified as a result of research and clinical studies.
The physical therapy management of patients with peripheral nerve injuries was similar to the program previously described for these patients in Zone of Interior hospitals. The program was often modified because of lack of personnel, equipment, time, and space. When time permitted, treatment was on an individual basis. When this was not feasible, carefully supervised and graduated reeducational exercises were performed in groups. A routine procedure, however, was to instruct the patient in the self-application of massage and to demonstrate the reeducational exercises which he was to perform at stated intervals during the day. Nonrigid elastic splinting was a common clinical practice.34 Splints were devised to encourage active motion, and patients were instructed in their use.
By volume, the treatment of patients with brain and spinal cord injuries was considerably less than that of peripheral nerve injuries as high evacuation priorities facilitated the early return of the former group to the United States. In the chain of evacuation, when it was necessary to hold these severely wounded patients in a hospital, physical therapy was often given at an earlier date than previously used. Bedside treatment usually consisted of passive exercise to preserve full range of joint motion and reeducational exercises which were sometimes supplemented by heat and massage. If patients remained, coordination and strengthening exercises were added, and if possible, ambulation was begun.
Orthopedic injuries
Wounds of the extremities, including bones and joints, constituted "approximately two-thirds of the 381,350 wounded and injured in action in Europe."35 Before D-day, noncombat training injuries comprised acute and chronic strains, sprains, and fractures. Following D-day, the majority of soft tissue injuries were from penetrating or lacerating wounds of the extremities, complicated many times by fracture and
34Seddon, H. J.: The Early Management of Peripheral Nerve Injuries. Practitioner 152: 101-107, February 1944.
35Medical Department, United States Army. Surgery in World War II. Orthopedic Surgery in the European Theater of Operations. Washington: U.S. Government Printing Office, 1956, p. VII.
278
injury to peripheral nerves, blood vessels, and soft tissue structures. With the subsequent sudden increase in the physical therapy patient load, the already structured rehabilitation program became invaluable in the care of the wounded.
When patients could go to the physical therapy clinic for treatment, whirlpool baths, if available, were frequently used for treatment of partially healed wounds of the extremities. A cleansing effect on septic wounds was noted, and joint stiffness, pain, and contractures were also relieved. In addition, patients found that the buoyancy of the water greatly facilitated the performance of exercises. Ultraviolet irradiation, if available, was also used to stimulate healing of wounds. A treatment sequence was sometimes employed in which the wound was dried by infrared irradiation following the whirlpool bath after which a stimulating dose of ultraviolet irradiation was given. When wounds were completely healed, patients were often instructed in self-application of friction massage to adherent scars. Ordinarily, in damage of muscles and tendons, and in the absence of nerve injuries, return of function was effected largely through graduated voluntary exercise.
Acute and chronic strains of back and feet accounted for a large percentage of disability of troops in combat as well as in training. Patients with acutely painful backs were frequently first treated on the orthopedic wards where some form of dry heat was applied. Later, as pain subsided, exercises were begun. Strains of the knee, as of other joints, received graduated exercises soon after injury. At the initial physical therapy appointment, patients were instructed in muscle setting exercises to be performed hourly. As the patients progressed, they were transferred to classified remedial exercise groups (fig. 73).
It was not possible to provide a complete physical therapy program for patients with major fractures due to the early evacuation of these patients. Those with long bone fractures were usually retained until after skeletal traction was completed. This permitted early use of static muscle contractions in the immobilized segment and active assistive motion of adjacent joints. Simple fractures of metatarsals and phalanges were not immobilized for prolonged periods, and many with little or no displacement were best treated by nonweight-bearing exercise.
Since amputation of an extremity precluded return to combat, evacuation of these patients to amputation centers in the United States was carried out as quickly as possible. When possible, instruction was given in muscle setting procedures and proper positioning of the stump to prevent contractures while enroute.
Patients with combined bone injury and nerve lesions required physical therapy to maintain and restore function. Patients in traction36 received electrical stimulation of denervated muscles and exercise to the adjacent joints. Windows cut in casts permitted stimulation during the period of rigid immobilization (fig. 74).
36Spurling, R. G.: Early Treatment of Combined Bone and Nerve Lesions. Bull. U.S. Army M. Dept. 4: 444-446, October 1945.
279
FIGURE 73-Physical therapist supervising group exercise, Italy.
Thoracic injuries
Early physical therapy, emphasizing breathing and postural exercises, and ambulation, provided as spectacular an impetus in the recovery of patients with thoracic injuries as did the early treatment of injured extremities.37 The pioneer work of the British in the treatment of patients with these injuries at the Brompton Hospital for Chest Diseases in London was interpreted to many Army physical therapists by Miss J. M. W. Reed, a member of The Chartered Society of Physiotherapy. Patients became ambulatory as soon as respiratory and cardiovascular functions permitted, often on the first postoperative day. Localized breathing and graduated exercises, usually begun as soon as the patient entered the hospital, often resulted in return of normal function in 4 to 6 weeks and eradicated the fixed thoracic cage and progressive structural deformities of the chest.
It should be apparent that many conditions other than those discussed here were treated in hospitals in the European theater. An attempt, however, had been made to focus brief attention on the more urgent needs and to point out the vital role of the physical therapist on the hospital team in the treatment of combat injuries.
Rehabilitation program
The general exercise program at the 5th General Hospital later
37Dykins, D.: Thoracic Injuries and Physical Therapy. The Army Nurse 2: 12, May 1945.
280
FIGURE 74-Electrical stimulation while immobilized in cast. (U.S. Army photograph.)
281
became part of the overall European theater rehabilitation program. Under the impact of combat, this program was evolved with the primary mission of returning the injured soldier to duty in the shortest possible time.38 To fulfill this mission, emphasis was placed on maintaining him during his hospital stay in the best possible condition of physical fitness while preserving his interest in the war effort and stimulating in him a desire to return to his outfit. Using the pilot program developed at the 5th General Hospital as a guide, similar programs were developed in other general hospitals, though none were as well recorded.
With the increase in battle casualties and the shortage of physical therapists, the rehabilitation program was delegated to the convalescent centers. There can be no doubt, however, that the success of the program developed at the 5th General Hospital played a most important role in The Surgeon General`s decision to establish what later came to be known as physical reconditioning.
The Philippine Amputation and Prosthetic Unit (9940th Technical Service Unit, Surgeon General`s Office) was appointed in February 1946, by direction of the Secretary of War, with the mission to establish an amputation center and prosthetic shop in the Philippine Islands. The unit consisted of 4 Army officers, 16 enlisted men, and 2 Medical Department civilian occupational therapists.39 Four Philippine Army nurses joined the group for on-the-job training in physical therapy procedures. Supplies and equipment were sent with the unit. A Philippine unit which had been trained in U.S. amputation centers assisted and ultimately took over the center.
Before the two physical therapy clinics, one for exercise and one for gait instruction, were completed the patients were treated at the 155th Station Hospital and the 1st Philippine General Hospital in Manila. The physical therapist was kept busy treating patients and providing training for the Philippine nurses. On Saturday mornings, the nurses received detailed instructions in bandaging, exercise, gait instruction, and clinic administration.
At the end of the 6-month period, 192 patients had been treated in the physical therapy clinic. These patients demonstrated a wide variety of upper and lower extremity amputations. Most amputation stumps were poorly shaped and many required surgical revision. Occasionally, a revision would be refused, forcing the prosthetist into evolving the best adaptation possible with the equipment on hand.
The prostheses were made of aluminum. Despite the damp tropical
38Circular Letter No. 146, Office of the Chief Surgeon, Headquarters, European Theater of Operations, U.S. Army, 27 Sept. 1943.
39Capt. Edward S. Brown, MC, surgeon; Capt. John J. Keys, CAC, prosthesis and brace maker; 1st Lt. Carol Stange, physical therapist; Lt. Roger Noden, CAV, amputee; Miss Mary K. Berteling and Miss Elizabeth Nachod, occupational therapists.
282
climate, the patients preferred to wear the wool stump socks. The physical therapy treatment provided these patients was essentially the same as that conducted in any amputee specialized treatment center in the Zone of Interior. In prosthetic training, walking on rough terrain was emphasized since few communities boasted of paved walks.
A small percentage of the patients arrived at the center with homemade prostheses. One man with an ankle disarticulation fitted his stump with a hollowed out piece of bamboo over which he wore a high-top shoe. Another was using a padded beer can. One bilateral below-knee amputee had put pads on his stumps and walked on his knees. The patients were well motivated and most appreciative. In October 1946, the center was turned over to the Philippine Army and the U.S. Army contingent departed.
The value of Army professional conferences for physical therapists was clearly demonstrated during World War II. The first conference was conducted at Percy Jones General Hospital in May 1945. In attendance were 10 medical officers specializing in physical medicine and orthopedic surgery and 19 chief physical therapists from Army general hospitals conducting physical therapy training programs and specialized treatment programs for amputees and patients with peripheral nerve injuries. While this conference was planned primarily to discuss the physical therapy management of these patients, training and personnel problems also received attention. Percy Jones General Hospital was selected as the site of this first conference because of the abundance of clinical material available for demonstration. The discussion focused on the evaluation of current treatment procedures and the new electrodiagnostic procedures being tested at this hospital.
Upon the conclusion of this conference, the group proceeded to Gardiner General Hospital to observe and discuss the therapeutic value of the weight resistance exercise program developed at that hospital by Captain DeLorme.
After the new procedures for treatment of patients with peripheral nerve injuries had been tested for several months and were considered acceptable, selected medical officers and physical therapists from the neurosurgical centers were invited to Percy Jones General Hospital for orientation courses in the procedures. Three 2-week courses were given in September and October 1945. Following these, the new procedures were instituted in each neurosurgical center.
In September 1945, at the suggestion of Col. Leonard T. Peterson, MC, orthopedic consultant, Surgeon General`s Office, representative medical officers and physical therapists from Army amputation centers conferred at the Army Medical Center (later Walter Reed Army Medical Center), Washington, D.C. Their mission was to analyze the treatment program for lower extremity amputees in respect to exercise
283
and walking instruction and to formulate a standardized program embracing the new concepts which were demonstrated and discussed. Once the program was formalized and accepted, those in attendance were instructed to return to their respective hospitals to initiate the revised program insofar as it was possible to do so without a specific directive.
1st Lt. Paige L. Weaver, a physical therapist on duty at Walter Reed General Hospital, was subsequently designated by the Surgeon General`s Office to visit all general hospitals specializing in the treatment of lower extremity amputees and to evaluate the functional results of the revised treatment program to ascertain if further revision of the program was indicated. Later, this revised program for lower extremity amputees was published by the War Department40 and previous directives relating to this group of patients were rescinded. This new directive filled an acute need in Army general hospitals and was enthusiastically received by officers and patients alike. It was agreed that the interchange of professional concepts was most valuable and contributed immeasurably to expediting the introduction of improved treatment procedures.
In keeping with the War Department`s policy regarding the maximum use and development of visual instructional aids, films were produced which depicted the physical therapy program for various groups of patients with combat injuries. With the approval of The Surgeon General, this program was started late in 1943. An officer assigned to the Army Medical Museum (now Armed Forces Institute of Pathology), Washington, D.C., directed the photography at selected Army general hospitals designated as specialized treatment centers. The Physical Therapy Branch, Surgeon General`s Office, was responsible for research, preparation of the script, and final editing of the film. Capt. (later Maj.) Mary S. Lawrence of the Physical Therapy Branch was assigned to the project as technical adviser.
It was envisioned that these films had a three-fold purpose: To produce an historical record of the professional advancement made in the management of patients with combat injuries, to instruct physical therapy personnel and orient medical officers on the treatment programs, and to orient the patient as to his role in his rehabilitation and stimulate interest in his recovery. At this time, there existed no similar instructional films which had been prepared by civilian agencies. These films were enthusiastically received both in the Army and in civilian groups. Several copies of each film were made and forwarded to service command surgeons for distribution to Army hospitals. Because of the keen interest shown by civilian professional groups, the War Department approved a policy by which such organizations were able to borrow the films on a nonprofit basis. As a result of this policy, these films were widely used.
The films covered the use of physical therapy in the treatment of
40War Department Technical Manual (TM) 8-293, June 1946.
284
amputees and in peripheral nerve injuries, techniques and practices in therapeutic exercise and specific therapeutic exercises for orthopedic conditions, thoracic injuries, and tendon transplants.
The Physical Therapy Branch also played a major role in the production of two films, "Swinging Into Step" and "Toward Independence," which were widely used both in Army and civilian institutions. While not primarily developed for instructional purposes, the treatment program was clearly unfolded in narrative form. "Swinging Into Step" portrayed an amputee wounded on the battlefield, his early treatment in an evacuation hospital overseas, his return to the mainland by hospital ship, the attendant morale and physical problems, and his eventual rehabilitation and complete adjustment to this condition. "Toward Independence" was the portrayal of a factory employee who, later as a combat soldier, incurred a spinal cord injury on the battlefield and depicted his rehabilitation in detail and his eventual return to his former occupation. "Toward Independence" received the annual award of the Academy of Motion Picture Arts and Sciences as being the
285
best documentary film of the year (fig. 75). These films are an invaluable pictorial adjunct to the history of the professional services of Army physical therapists in World War II.
To assure standardization of physical therapy techniques and procedures in massage and in the treatment of amputees, two War Department bulletins and a technical manual were prepared by the Physical Therapy Branch.41 Special directives prepared in the Surgeon General`s Office for the guidance of Army medical personnel in the treatment of patients with poliomyelitis, amputations, and spinal cord injuries42 were coordinated with the Branch to insure incorporation of current physical therapy doctrine and treatment procedures.
A comparison of the physical therapy programs conducted during World Wars I and II clearly points out a definite change in emphasis. In World War I, the emphasis was on treatment administered to injured extremities, while in World War II, attention was shifted to treatment of the patient as a whole in addition to his injured extremity and his participation in his recovery. This change in concept, developed over a period of years, reached its maximum development during World War II when its effectiveness was so dramatically demonstrated.
41(1) War Department Technical Bulletin (TB MED) 122, December 1944. (2) War Department Technical Bulletin (TB MED) 173, August 1945. (3) See footnote 40, p. 283.
42(1) War Department Technical Bulletin (TB MED) 10, 11 Feb. 1944. (2) See footnote 6, p. 247. (3) War Department Technical Bulletin (TB MED) 193, 31 Aug. 1945. (4) Army Service Forces Circular No. 440, 10 Dec. 1945.
![]()